
Abstract
Introduction:
Minimally invasive major hepatic resection (MIMHR) is increasingly being performed in tertiary centers using either hand-assisted laparoscopic surgery (HALS) or totally laparoscopic surgery (TLS). The outcomes data of MIMHR are scarce, especially in comparison to open major hepatic resection (OMHR). Our aim was to compare 90-day outcomes in major hepatic resections when minimally invasive approaches are attempted.
Methods and Procedures:
At our institution, minimally invasive liver resection was formally introduced in January 2007, initially using the HALS approach. Since then, the use of TLS approach has increased. We collected data on all patients who underwent major liver resection between January 2007 and December 2017 at our institution. In an intention to treat fashion, we then compared MIMHR to OMHR.
Results:
From January 2007 to December 2017, 669 patients underwent liver resection. Of these, 203 patients (30%) underwent major hepatic resection and MIMHR and OMHR were performed in 68 (33%) and 135 (67%) patients, respectively. The rate of conversion from minimally invasive to open was 30.9%. Overall, there were no significant differences in 90-day mortality (2.9% versus 1.5%; P = .499) or major complications (14.7% versus 14.8%; P = .985). MIMHR was associated with a shorter average postoperative hospital stay (6.2 days versus 7.9 days; P = .0110) and shorter average ICU stay (0.66 days versus 0.90 days; P = .0299) compared with OMHR.
Conclusions:
The minimally invasive approach to major liver resection is a safe and reasonable alternative to an open approach when performed by a surgeon experienced with the relevant surgical techniques. MIMHR may be associated with similar outcomes and a shorter postoperative hospital stay with no increase in 90-day postoperative complications to OMHR.
Introduction
Laparoscopic hepatic resection was first introduced in the early 1990s. 1 However, due to some inherent challenges of laparoscopic surgery such as decreased tactile sensation, difficulty in handling massive bleedings, and gas embolism among other things, adoption was slow relative to other surgical domains. 2 For these reasons, while laparoscopy for minor hepatic procedures has steadily increased, an open approach has generally been the standard of care for major hepatic resection.
At the first International Consensus Conference on Laparoscopic Liver Resection (ICCLLR), in Louisville in 2008, 2 it was determined that the standard of practice for minor hepatic resection should be a laparoscopic approach when feasible. 3 Since then, with the improvement in technology and equipment, the number of minimally invasive hepatic resections has increased rapidly worldwide, and extended to major hepatic resection (which is defined as resection of more than three liver segments).4,5
At the second ICCLLR in 2014, it was concluded that minimally invasive major hepatic resection (MIMHR) is an innovative procedure but that more information would be needed before it could be declared the standard of practice. 6 With increasing popularity and growing evidence for MIMHR, the European Guidelines Meeting for Laparoscopic Liver Surgery in Southampton in 2018 produced a set of clinical practice guidelines, which advocate that the laparoscopic approach should be considered standard practice for most current liver lesions. 7
At our institution, MIMHR has become a common method of liver resection, however, it remains challenging due to technical difficulty and control of hemorrhage.
A few recent studies demonstrated advantages of MIMHR over conventional open major hepatic resection (OMHR) in terms of blood loss, postoperative hospital stays, complications, and return to a normal diet.8–17 Nevertheless, data remain scarce. In this study, we retrospectively compared the short-term surgical outcomes of patients who underwent OMHR versus MIMHR in the same period.
Methods and Procedures
At our institution, MIS hepatic resection was formally introduced in January 2007, initially using the hand-assisted laparoscopic surgical (HALS) approach. Since then, the use of a totally laparoscopic surgical (TLS) approach has been adopted and increased. Data were retrospectively collected on all patients who underwent major hepatic resection (defined as resection of three or more Couinaud segments) between January 2007 and December 2017 at our institution by five experienced hepatobiliary surgeons (J.A.S., H.J.A., J.B., K.C., and J.N). A prospectively maintained database was used to identify all the patients who had undergone all procedures meeting inclusion criteria during this time period.
No patients in the database were excluded from the study. The demographics of the two groups as well as operative indications were then analyzed in an intent-to-treat fashion. We then did a subgroup analysis between the 21 patients who underwent conversion to an OMHR compared with those who successfully underwent MIMHR.
Surgical and perioperative outcomes were then retrospectively analyzed using a two-sample test. Liver function was evaluated using serum total bilirubin, alanine aminotransferase levels and albumin, platelet count, and prothrombin time. Differences in continuous variables between groups were statistically analyzed using the Student's t-test. The Mann–Whitney U-test was used to compare continuous variables with skewed distributions, and a chi-square was used to compare categorical variables. P values of <.05 were considered statistically significant.
Posthepatectomy liver failure (PHLF), posthepatectomy bile leak, and posthepatectomy hemorrhage were graded according to the International Study Group of Liver Surgery definitions.18–20 Major complication rates were defined using the Clavien/Dindo classification system. 21 Major complications were defined as Clavien grade 3 and above, which includes PHLF grade B and C.
Results
From January 2007 to December 2017, 669 patients underwent hepatic resection. Of these, 203 patients (30%) underwent major hepatic resection. MIMHR was attempted in 68 patients. In 38 patients, a TLS was attempted, however, 2 were converted to HALS. One of these patients was then converted to an open procedure. In the other 30 patients who underwent a minimally invasive approach, a HALS was initially attempted but 15 of these patients were converted to an open procedure for either bleeding or failure to advance the procedure. Patients were analyzed on an intention-to-treat basis. There were 135 patients who underwent OMHR during this same time period.
Four of the OMHR patients underwent a second OMHR as part of a staged procedure, however, the second procedure's short-term outcomes were excluded from the analysis due to the confounding effect that recovery from the first resection may have had on the outcomes of the second procedure.
Patient baseline characteristics in the MIMHR and OMHR groups are summarized in Table 1. There were no statistically significant differences in terms of sex, age, or comorbidities, including hypertension, diabetes, cardiac disease, or pulmonary disease. There was a higher percentage of patients in the OMHR with chronic kidney disease (16.8%) compared with the minimally invasive group (4.4%), P = .012. There was also a higher percentage of patients in the OMHR group with chronic hepatic disease (29.5%) compared with the MIMHR group (4.4%), P ≤ .001.
Patient Demographic Data and Outcomes
Bold indicates p ≤ 0.05.
ASA, American society of Anesthesiologists; CKD, chronic kidney disease; ECOG, Eastern Cooperative Oncology Group Performance Score; MIMHR, minimally invasive major hepatic resection; OMHR, open major hepatic resection.
Pathological indications for resection in the MIMHR and OMHR groups are summarized in Table 2. There were no statistically significant differences.
Patient Pathological Indications for Surgery
MIMHR, minimally invasive major hepatic resection; OMHR, open major hepatic resection.
Operative details in the MIMHR and OMHR groups are summarized in Table 3. There were significantly higher rates of right hepatectomy in the MIMHR group (57.4%) than in the OMHR group (27.4%), P ≤ .001. There were no statistically significant differences in transfusion rates, estimated blood loss (EBL), or operative time between the two groups. The median EBL for OMHR and MIMHR was 300 and 400 mL respectively.
Operative Details
Bold indicates p ≤ 0.05.
EBL, estimated blood loss; HALS, hand-assisted laparoscopic surgery; pRBC, packed red blood cells; MIMHR, minimally invasive major hepatic resection; OMHR, open major hepatic resection.
Short-term surgical outcomes for the MIMHR and OMHR groups are summarized in Table 4. Overall, MIMHR was associated with a similar duration of operation time (314 minutes versus 290 minutes; P = .291), similar blood loss (971 mL versus 935 mL; P = .064), transfusion rate (24% versus 28%; P = .544), and transfusion volume (4.6 U versus 4.2 U; P = .230). As shown in Figure 1, patients who underwent MIMHR had a shorter average postoperative hospital stay (6.2 days versus 7.9 days; P = .0110) and shorter average ICU stay (0.66 days versus 0.90 days; P = .0299) compared with OMHR.
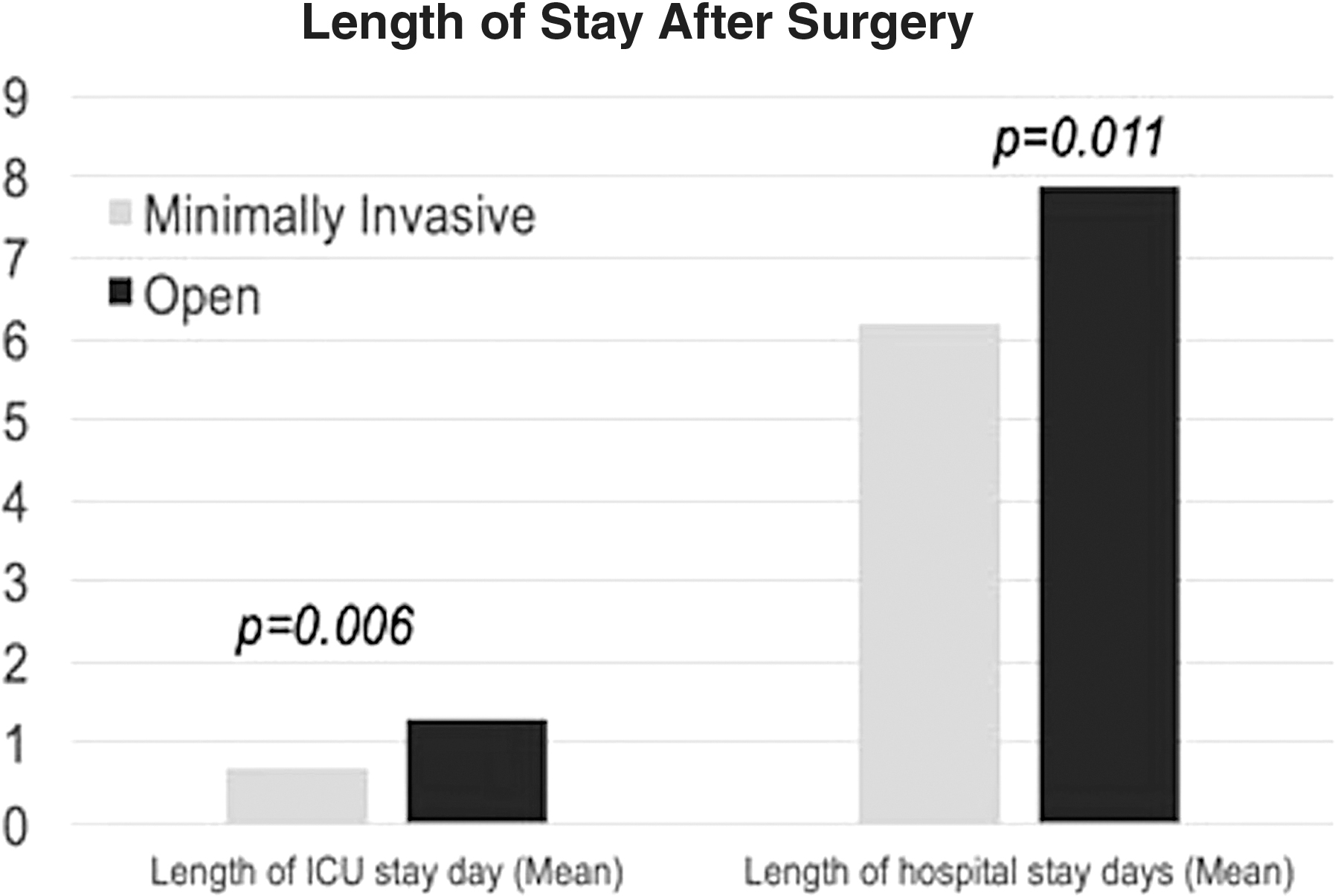
The mean length of ICU stay and overall hospital stay compared between laparoscopic and open major hepatic resection at Mayo Clinic Jacksonville between 2007 and 2017.
Short-Term Surgical Outcomes
Bold indicates p ≤ 0.05.
MIMHR, minimally invasive major hepatic resection; OMHR, open major hepatic resection; pRBC, packed red blood cells; UTI, Urinary tract infection.
Ninety-day mortality and complication rates in the MIMHR and OMHR groups are summarized in Table 4. There were no significant differences in 90-day mortality rates (2.9% versus 1.5%; P = .499) or major complication rates (14.7% versus 14.8%; P = .985).
We compared the subgroups of patients who underwent conversion to an OMHR against those who successfully underwent MIMHR, these results are summarized in Table 5. On average, the EBL was more than double in the conversion group as compared with the not converted group (712 mL versus 1798 mL, P = .007), and subsequently the transfusion requirements through the hospital stay on average were significantly higher in the converted patients compared with the not converted patients (1.5 U versus 4.4 U, P = .0004). Notably, the median EBL was again more similar (300 mL in the nonconverted group and 500 mL in the converted group), as was the median number of blood transfusions given (1 and 2 U for the nonconverted and converted groups, respectively). In the conversion group, there were higher rates of right hepatectomy (71.4% versus 25%, P = .0011) and extended right hepatectomy (25.0% versus 1.9%, P = .0029) than in the nonconversion group. In the conversion group, there were no statistically significant differences in concomitant wedge resections (10.2% versus 12.5%, P = .798) or concomitant organ resections (10.2% versus 25%, P = .138) compared with the nonconversion group. The conversion group had longer operative times but did not reach significance (386 minutes versus 288 minutes, P = .059). The two groups did not have significant differences in average age, body mass index (BMI), or American Society of Anesthesiologists (ASA) class.
Analysis of Converted vs Non-Converted Patients Where Minimally Invasive Major Hepatic Resection was Attempted
Postoperatively, the converted patients were more likely to suffer pulmonary complications (12.5% versus 1.9%, P = .0332), but there were no other significant differences in complication rates between the two groups, including reoperation (1.9% versus 0%, P = .582), bile leak (1.9% versus 0%, P = .582), abscess (1.9% versus 0%, P = .582), or liver failure (1.9% versus 0%, P = .582). The average length of stay was similar between the two groups (6.7 days versus 6.3 days, P = .95), and the length of ICU stay on average similar between the two groups (0.6 versus 0.9, P = .642).
Discussion
Despite challenging conditions, MIMHR is gaining increasing popularity for patients with various liver diseases. MIMHR has been shown to be safe when done by experienced laparoscopic surgeons.
In this study, the MIMHR and open groups had similar characteristics and similar indications for resection. According to data reported in this series, MIMHR appears to be comparable if not superior to OMHR, especially if the procedure can be completed in a minimally invasive fashion. The MIMHR group demonstrated superior surgical outcomes, such as ileus, wound infection rate, and hospital stay. Other surgical outcomes, such as EBL and operative time, were similar between the two groups.
Short-term outcomes between MIMHR and OMHR have recently been reported.5,9–12,14–17 These studies overall have similar outcomes to ours, showing that MIMHR results in similar morbidity, blood loss, transfusion rates, but with a shorter hospital stay. The first randomized trial (OSLO-COMET) 16 also reported shorter hospital stay and lower morbidity in their minimally invasive resections, however, only short-term outcomes were analyzed since this study concluded in 2017. Long-term outcomes will need to be reassessed for a more thorough comparison of these two techniques.
The major limitation to this study is that it is a retrospective study which does not allow for randomization and therefore is susceptible to selection bias. Other limitations include that there were higher rates of chronic kidney disease and chronic hepatic disease in the OMHR patients than in the MIMHR group. This may have skewed the results of the study outcomes against the OMHR group as those patients would be expected to have a longer recovery from the procedure, especially the chronic hepatic disease patients who may have a more prolonged recovery since they have a less robust liver remnant.
There were some slight differences in the makeup of the baseline surgical risks from a demographics standpoint. For example, there was also a higher percentage of patients with an ASA score of IV who underwent OMHR (18.5%) versus MIMHR patients who had an ASA score of IV (2.9%), P ≤ .001. There was also a higher percentage of patients with a Eastern Cooperative Oncology Group Performance Score (ECOG) score of II who underwent OMHR (20.0%) versus MIMHR patients who had an ECOG score of IV (2.9%), P ≤ .001. Patients who underwent an open resection also had a lower mean BMI (25.3) in comparison to the MIMHR patients (27.0), P = .0403.
A few comparative studies, which were done more similarly to this study, reported the same results between MIMHR and OMHR: Yoon et al. 9 reported lower complications in MIMHR than in OMHR (6.9% versus 22.4%; P = .02), and Cheung et al. 8 reported similar complication rates (6.3% versus 18.8%; P = .184) between the two groups.
Additionally, this series showed a higher-than-expected blood loss for major hepatectomy for both groups. We, however, feel that this is likely due to the relatively small number of cases that were disproportionally affected by several outliers in each arm. The median blood loss in this series was 300 mL in the OMHR and 400 mL in the MIMHR group, which is similar to other reported outcomes in literature.5,8–17,22–27
In this study, we report a conversion rate of 31%. However, a subgroup analysis was done and we did not find a significantly worse major complication rate compared with those who were completed successfully in a minimally invasive fashion. Based on the increased blood loss, these cases were likely more complex operations than those that were not converted. This is due to the nature of hepatic surgery where it can be difficult to accurately preoperatively assess the perihepatic adhesions (e.g., diaphragm attachment) or difficulty of a hilar dissection, especially in the case of previous operations or liver-directed therapies, which were common in this patient cohort. Most of the surgeons performing hepatectomy in this patient series have a low threshold to attempt a minimally invasive approach, which maximizes the number of patients who might benefit from this approach. While this approach may result in an increased conversion rate in this series, this is not a reflection of increased complications for the patients who underwent conversion. The reasons for converting are less likely due to an urgent issue, such as hemorrhage, but was frequently for failure to progress or increased difficulty with dissection. In fact, the conversion rate increased (20% in 2008 to 50% in 2017) due to increasing experience and lower threshold for attempting minimally invasive surgery. When we examine the subgroup analysis of conversion versus nonconversion MIMHR patients, we also see a significantly higher EBL in the conversion patients, however, we again feel this is due to outliers in the group which had very large EBLs because both median EBL (300 in conversion versus 500 in nonconversion) and median transfusion rates (1 versus 2) were much more similar between the two groups.
Overall, the evidence, which supports laparoscopic major hepatectomy, is continuing to accumulate. Expert opinions and consensus guidelines are also advocating more and more for MIMHR.7,28,29 Our data are consistent with the other outcomes data reported and would also suggest that MIMHR is safe in the hands of a surgeon who is proficient and minimally invasive and OMHR.
Conclusion
MIMHR is a feasible and safe alternative to OMHR when performed by a surgeon experienced with the relevant surgical techniques. MIMHR is also associated with a shorter postoperative hospital stay and ICU stay with no compromise in complication rates.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.