
Abstract
Introduction:
The role of robotic surgery in radical nephrectomy is controversial with detractors claiming no benefit over standard or hand-assisted laparoscopic nephrectomy with increased cost. We routinely offered robotic radical nephrectomy (RRN) for all renal masses not amenable to partial nephrectomy regardless of size or complexity and evaluated the success rate for massive tumors (≥15 cm) to assess whether RRN may be justifiable in such cases.
Methods:
We reviewed our prospective database of RRN by an experienced robotic surgeon (R.A.). All patients with massive renal tumors (≥15 cm) were included without exclusions, and no nephrectomy procedures were performed laparoscopically or open approach by the surgeon such that there was no selection bias.
Results:
Fifteen patients had tumors of 15–30 cm (mean 19 cm) and underwent RRN without exclusions. Mean age was 62 years (35–78 years) with mean body mass index of 31 kg/m2 (21–41 kg/m2). One required partial liver resection, one splenectomy and distal pancreatectomy, one had a large caval thrombus, one a large renal vein thrombus, and one invaded psoas muscle, but all were completed robotically without conversions and no transfusions, with mean operative time of 235 minutes (72–337 minutes). Midline extraction incisions were used and no patients required intravenous narcotics. Twelve were discharged on the first postoperative day (80%) with median length of stay of 1 day and no 90-day readmissions. The only complication was temporary renal insufficiency in 1 patient.
Conclusions:
RRN for massive renal tumors (>15 cm) is feasible, and can be safely performed with excellent outcomes even in the setting of locally advanced malignancies.
Introduction
The National Comprehensive Cancer Network (NCCN) guidelines state that radical nephrectomy may be performed with open, laparoscopic, or robotic surgical techniques. 1 Long-term outcomes indicate that open and minimally invasive approaches have equivalent cancer-specific survival. 2 Laparoscopic radical nephrectomy (LRN) with or without hand assistance has demonstrated advantages compared with open radical nephrectomy with regard to estimated blood loss (EBL), postoperative pain, recovery, hospitalization, and convalescence. 3 The laparoscopic approach has been widely adopted and has been extended toward larger tumors, with different groups reporting success with increasing tumor size and number of patients.4–6
Previous studies have examined LRN for large (>7 cm) and very large (>10 cm) renal tumors, but LRN for tumors of 7 cm or even 10 cm is not materially different than for smaller tumors. 7 The role of robotic surgery for radical nephrectomy is controversial as opponents claim no benefit over LRN and no need for robotic technology to perform minimally invasive nephrectomies.8,9 If robotic radical nephrectomy (RRN) has any benefit over LRN, it would be expected to be for more challenging cases due to size or complexity.
We routinely perform RRN for all renal masses not amenable to partial nephrectomy regardless of size or complexity with the hypothesis that robotic technology would enable removal of even the largest or locally advanced tumors. We evaluate the safety, feasibility, and clinical outcomes of patients with massive renal tumors ≥15 cm who underwent RRN and compare with LRN series of large and very large tumors to determine if RRN may be beneficial for tumors rarely managed by LRN in the literature.
Patients and Methods
We reviewed our prospective database of RRN by an experienced robotic surgeon (R.A.). All patients with massive renal tumors (≥15 cm) were included without exclusions, and no nephrectomy procedures were performed laparoscopically or open by the surgeon such that there was no selection bias. Local invasion, including caval thrombus, was not considered a contraindication for RRN. Preoperative variables included age, body mass index (BMI), and medical comorbidities. Operative and postoperative variables included EBL, operative time (OT), transfusions, number of robotic ports used, tumor size, lymph node dissection, final pathological stage, length of stay (LOS), and complications.
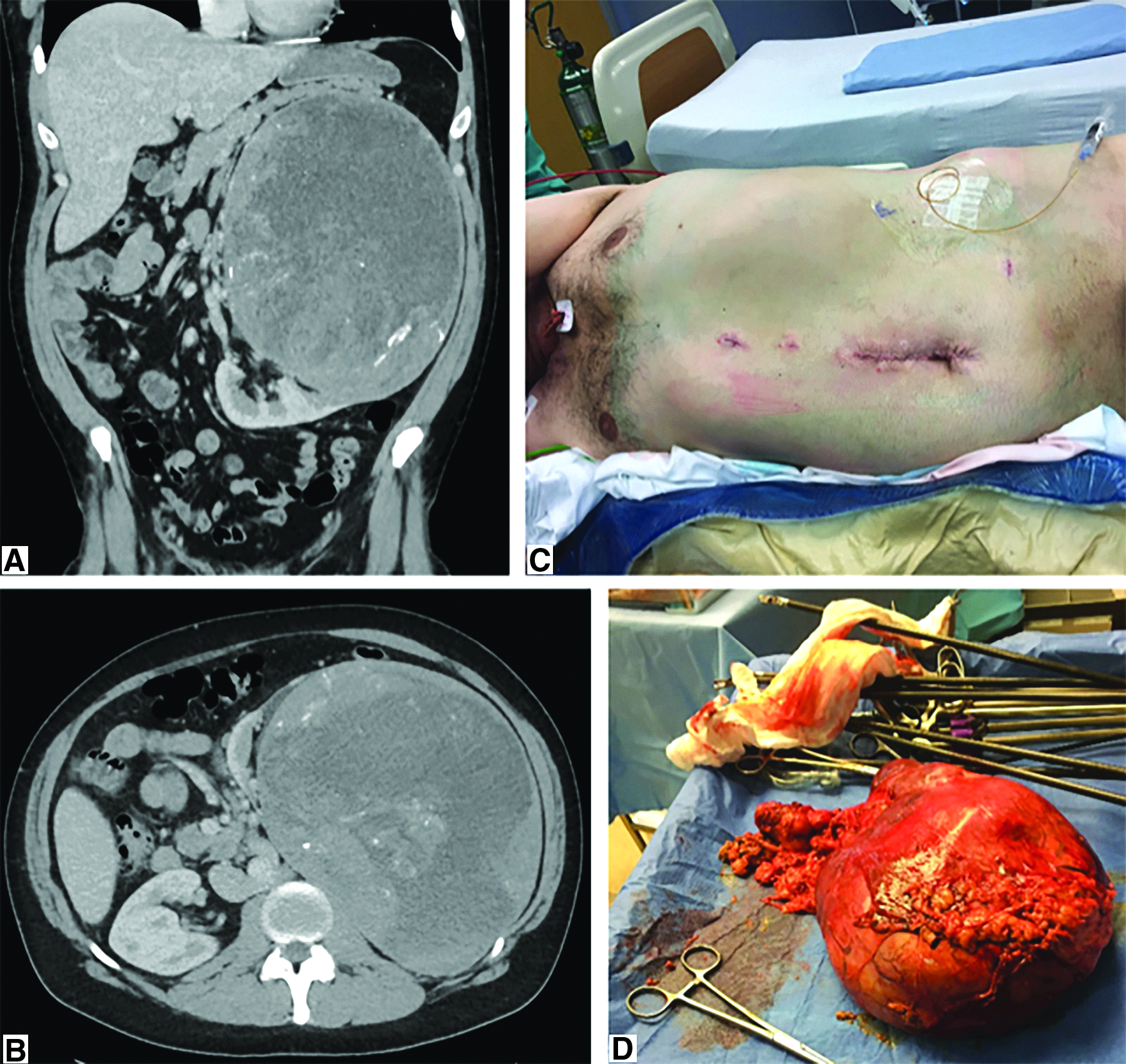
A prospective database captured all cases, and those patients with tumors 15 cm or larger (i.e., massive) were reviewed and compared with the laparoscopic literature for large (>7 cm) and very large (>10 cm) tumors (Fig. 1).
Results
Between May 2008 and November 2017, we identified 15 patients with a renal mass ≥15 cm. All underwent RRN without exclusions for size and without conversions to open surgery in any case. The mean age was 62.4 years (range, 35–78 years), mean BMI was 30.6 kg/m2 (range, 21–41 kg/m2). Distribution by gender was 7 female and 8 male patients (Table 1). Preoperative medical comorbidities included emphysema, myocardial infarction, osteoarthritis, hypertension, diabetes, dyslipidemia, gastroesophageal reflux, and skin cancer.
Descriptive Characteristics of 15 Patients Treated with Robotic Radical Nephrectomy for Renal Tumor ≥15 cm Between May 2008 and November 2017
BMI, body mass index.
Twelve surgeries (80%) were performed using three robotic ports with the remaining three using four robotic ports. In 7 patients (47%) the procedures were performed without using an assistant port. A surgical drain was placed in 1 patient (7%) due to involvement of the pancreas and need for partial pancreatectomy and splenectomy. In addition to this, 1 patient required a partial liver resection for liver invasion, 1 had a large caval thrombus, 1 had a large renal vein thrombus, and 1 tumor invaded and required partial resection of the psoas muscle.
Mean OT was 234.6 minutes (range, 72–337 minutes) and mean EBL was 159.6 mL (range, 10–750 mL). No patients required blood products or blood transfusion. A midline (nonmuscle cutting) extraction incision was made in all cases. No patients required any intravenous narcotics, all managed with non-narcotic analgesia and oral narcotics when needed. Twelve patients (80%) were discharged on the first postoperative day for a median LOS of 1 day with prolonged admission occurring in only 1 patient who had a temporary renal failure that resolved after 7 days without need for dialysis. There were no other complications or readmissions within 90 days of surgery and only one emergency department visit for an issue related to the patient's history of substance abuse. In cytoreductive nephrectomy patients, systemic therapy was begun as early as 2 weeks postoperatively (Table 2).
Operative and Perioperative Outcomes of Radical Nephrectomy for Renal Tumor ≥15 cm Between May 2008 and November 2017
The total specimen weight and pathologic tumor size (maximum length) were 1620 g (range, 660–2400 g) and 18.9 cm (range, 15–30 cm). Pathological analysis reported 12 (80%) renal cell carcinomas (10 clear cell, 1 sarcomatoid, 1 chromophobe). The predominant pathologic stage was T3 (n = 8/12) and Fuhrman grade 4 was the most frequent (n = 7/12). Lymph node dissection was performed in 9 cases with an average of 9.1 nodes and 9 overall positive nodes. No readmissions within the first 90 postoperative days were registered (Table 3).
Pathological Outcomes
Discussion
Over a 10-year period, 15 patients with massive renal tumors ≥15 cm underwent successful RRN. The mean tumor size was 18.9 cm, yet all patients benefitted from a minimally invasive operation with most going home the next day and without intraoperative or postoperative complications associated with the surgery. To our knowledge, this is the largest series of RRN for large renal tumors described in the literature and the only series specifically studying minimally invasive surgery for massive tumors ≥15 cm.
Since Clayman et al. published the first LRN in 1991, the benefits of minimally invasive surgery have been extended for larger and more complex tumors.10,11 The laparoscopic literature has described LRN for large (≥7 cm) and very large tumors (≥10 cm) (Table 4).3,5,7,12–15 We hypothesized that the benefit of using robotic technology in performing laparoscopic nephrectomy might not be apparent until reaching larger sizes or for more complex tumors with local invasion, for example. In our experience, tumors of 7 cm or even 10 cm are not materially different than nephrectomy for smaller tumors, and in the age of nephron-sparing surgery for increasingly larger tumors, nephrectomy is less often performed for tumors <7 cm. Unlike the previous series rarely including tumors >15 cm and all having mean tumor size of <13 cm,7,5,15 we specifically studied tumors ≥15 cm (mean 18.9 cm) and compared their outcomes after RRN with these series of smaller tumors.
Comparative Studies Evaluating Specimen Size, Conversions, Transfusions, and Intraoperative Complication Rates of Radical Nephrectomies for Large and Very Large Tumors
IVC, inferior vena cava.
Despite our series including larger tumors of up to 30 cm and several locally invasive tumors involving the inferior vena cava (IVC), liver or pancreas, and spleen, we had no intraoperative complications, transfusions, or conversions to open surgery. Although our series is small, the absence of these events in contrast with the previous literature may suggest a benefit to using the improved technology afforded by robotic surgery. We believe that the major challenges in nephrectomy for massive tumors are the limited working space (potentially preventing room for hand assistance), neovascularity requiring extreme care to prevent injury to pathologic and thin-walled veins, and difficult access to the renal hilum due to the tumor drooping over the hilum and often the great vessels themselves. We found that the dexterity of the robotic instruments as well as surgeon control of the scope allowed safe access to the hilum even in massive tumors, where no more than an inch of clearance under the tumor could be obtained because of the inability to lift the tumor any further as confined by the anterior abdominal wall.
In addition, local tumor extension was not an obstacle to completing the surgeries without conversion to an open procedure. The presence of venous tumor thrombus was an exclusion criterion in some LRN studies, and the reason for conversion in others.4,5 We believe that the 3D vision and articulated instruments of robotic surgery that aid in suturing in other procedures, such as prostatectomy and pyeloplasty, can be equally advantageous over laparoscopic surgery in nephrectomy procedures where suturing is required, whether for the IVC, the liver, or the pancreas. 16
Admittedly, robotic nephrectomy has been shown to be costlier than LRN. 17 While selection bias likely impacts this finding such that failing to control for tumor size and complexity might lead to a bias against RRN, given that surgeons might choose LRN for simpler cases and reserve RRN for more complex procedures. Additionally, a surgeon only performing LRN might exclude more complex tumors such as IVC thrombus or locally invasive cases and perform these open. In our experience, RRN can be performed routinely without additional costs in hospitals already owning robotic equipment since in less complex procedures assistant ports can be avoided as well as other disposables like staplers and energy devices. 18
While we did not perform a cost analysis or have a comparison group of LRN procedures, it is possible that RRN might be deemed cost effective if it can reduce complications, transfusions, conversions, and LOS, as well as the need for open surgery. We were able to routinely perform RRN for all patients presenting with renal masses requiring nephrectomy regardless of size or involvement of contiguous organs with excellent outcomes in this small series of massive tumors. Most patients required only an overnight stay, which would not be expected for open surgery, and while only 80% of patients went home on the first postoperative day as compared with our experience with RRN for all tumor sizes (∼94% overnight stay), 19 only 1 patient had a prolonged stay due to renal insufficiency that we believe was a result of losing a kidney and not the surgery. A larger experience with more surgeons will be required to confirm our findings and to suggest whether the results are truly reflective of an advantage with robotic technology or other factors.
Conclusion
RRN for massive renal tumors (≥15 cm) can be safely performed with excellent outcomes even in the setting of locally advanced malignancies. Robotic technology may offer an advantage when considering the laparoscopic literature for large and very large tumors, but a larger and multi-institutional experience is necessary to confirm or refute this.
Footnotes
Acknowledgments
The authors would like to acknowledge Janice Rosenthal, R.N. and Deborah Chervin for database maintenance and the OhioHealth Research Institute.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.