
Abstract
Purpose:
To present the outcomes of the laparoscopic and robotic treatment of pediatric simple renal cysts with two novel modifications: the indocyanine green (ICG) fluorescence and the perirenal fat tissue wadding technique.
Methods:
Between 2012 and 2019, 13 patients with solitary renal cysts were treated through minimally invasive approach. Preoperative work-up included ultrasonography and computed tomography or magnetic resonance. A cyst deroofing was performed in all cases. In the last 3 cases, the ICG fluorescence technique enabled a clear identification and safe puncture of the cyst dome. Five cysts were filled with perirenal fat tissue after deroofing.
Results:
Thirteen patients (9 boys) were treated through laparoscopic (6 patients), retroperitoneoscopic (3 patients), or robotic approach (4 patients). Median age was 8 years (5–15 years). The median cyst size was 70 mm (42–160 mm). Eight cysts were located in the right kidney. All cysts were progressive and symptomatic. Thirteen cysts (100%) were graded as type II according to the Bosniak classification. No conversion was recorded. The median operative time for laparoscopy was 50 minutes (35–90 minutes) and 85 minutes for robotics (65–120 minutes) including surgical and docking time. No intraoperative complications occurred. The median hospital stay was 2 days (36–96 hours). No residual liquid was detected on follow-up after deroofing and fat tissue wadding technique.
Conclusions:
Cyst deroofing is an effective and durable treatment for symptomatic simple renal cysts. Robotics enables excellent tissue dissection and ergonomics. The perirenal fat tissue wadding of the cyst seems to reduce the recurrence rate. The ICG fluorescence technique allows for better identification of the cyst and safer surgical procedure.
Introduction
Solitary Renal Cysts (SRC) are defined as unilateral and solitary lesions outside the renal parenchyma with no associated systemic illness or disorders and no communication with the renal pelvis. 1 SRC are classified into “simple” or “complex” according to their radiological characteristics and malignancy risk.2–4 As oppose to adult population, the incidence of SRC in children is below 1%5,6 and complex SRC are rarely encountered. The pathophysiology of pediatric SRC formation remains unclear. 3 SRC are usually incidental findings as only 5% present with abdominal pain, hypertension, or renal dysfunction.3,4 Renal cysts may also be the first manifestation of genetic or syndromic conditions.7,8 Although rare, pediatric cystic renal tumors have been described in a small series of complex renal cysts.9,10
There is no current consensus on the appropriate diagnostic work-up, management, or follow-up for SRC in children. 11 Nowadays, the first evaluation of SRC at the time of diagnosis relies on the radiological classification of Bosniak and colleagues, originally described for adults.2,12 According to the radiological findings and malignancy risk, SRC are classified into Stages I–IV. Stages I–II represent 95% of SRC and are considered as simple or benign SRC, 5 whereas Stages III–IV demonstrate high vascularity and are considered as complex or potentially malignant. 12 Regarding the surgical treatment of simple or benign SRC in pediatrics, the current literature is scarce and heterogeneous with less than 40 cases described so far.5,11,13,14 The knowledge in the robotic treatment for pediatric SRC is even more limited. 15
We present herein the laparoscopic and robotic treatment of simple pediatric SRC in our institutions. We contribute two novel technical modifications to the surgical technique: the indocyanine green (ICG) fluorescence and the pedicled perirenal fat tissue wadding of the cyst. We associate a literature overview to offer a proposal of management of this rare condition in children.
Materials and Methods
Patients
Between 2012 and 2019, 13 patients with SRC were treated through minimally invasive approach in our centers. Clinical, radiological, and surgical parameters were retrospectively gathered from medical records. Conservative management based on clinical and ultrasound (US) follow-up was carried out until the patient showed clinical worsening or the SRC was at risk of traumatic rupture secondary to its massive size. Preoperative work-up included a magnetic resonance imaging (MRI) or a computed tomography (CT) (Fig. 1). The imaging was decided upon the radiologist experience and the availability of each center. SRC were classified according to the Bosniak classification upon CT or MRI findings.2,12 The recently revised classification considers SRC bigger than 3 cm automatically as Stage IIF. 12 We considered them as Stage II because Stage IIF has not been clearly defined in pediatrics yet.
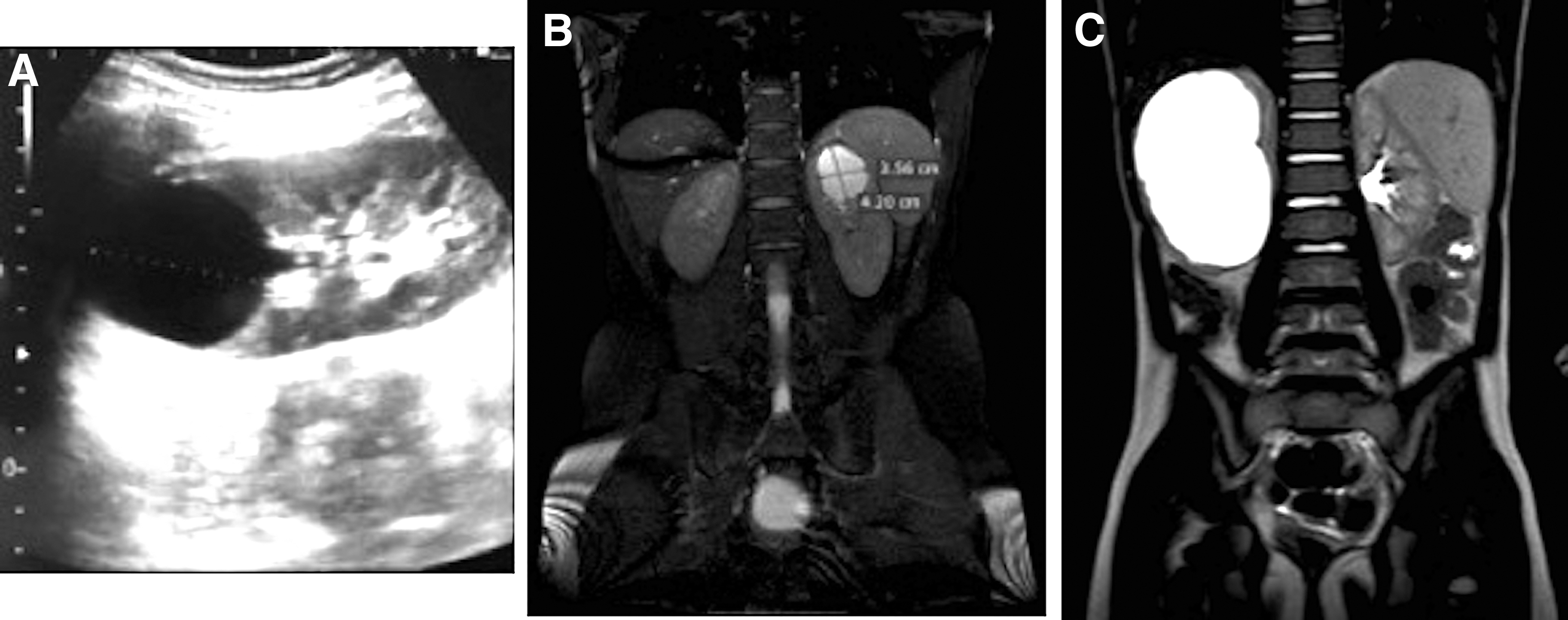
Preoperative assessment of simple renal cysts (from left to right). Thirteen-year-old patient with increasing renal cyst in follow-up and recurrent abdominal pain.
Technique and procedure
The surgical approach was decided upon the SRC location, the surgeon experience, and the availability of robotic console. Retroperitoneal laparoscopic deroofing was performed using a three 5 mm port technique already described in previous publications. 16 Laparoscopic and robotic cases were performed transperitoneally. Three 5 mm trocars were used during laparoscopy. Robotic cases warranted four trocars: three working trocars of 8 mm and one accessory trocar of 5 mm (Fig. 2). After the induction of general anesthesia, the patient was catheterized and positioned in the standard left/right lateral decubitus position. After mobilization of the colon, we divided the Gerota fascia to access the kidney. Pathological adhesions of epiploon to the parietal abdominal wall on the same side of the SRC were found especially in the biggest cases (Fig. 3). To shorten the dissection time and reduce the risk of bleeding, we used sealing devices in laparoscopy and retroperitoneoscopy and monopolar scissors or bipolar Maryland forceps in robotics. Once the cyst was identified and exposed, we punctured it with a transparietal needle. The cyst content was aspirated and analyzed. The roof of the cyst was resected then, with bleeding control, and sent for histological evaluation (Fig. 4). In the last 3 robotic cases, we administered 0.35 mg/kg (maximum allowed 2.5–5 mg/kg) of ICG intravenously intraoperatively. ICG is a fluorescent dye of intravenous administration that is eliminated from the body with a half-life of 3–5 minutes. The fluorescence effect lasts in vivo a few hours. Once injected, in a matter of seconds, the ICG fluorescence technique enabled to identify the nonvascularized cyst dome from the vascularized renal parenchyma (Fig. 5). Thanks to the ICG fluorescence technique, the cyst evacuation and deroofing were safely performed (Fig. 5). In the last 5 cases (4 robotic and 1 laparoscopic), we created a pedicled flap of perirenal fat tissue to wad the cyst cavity. Before filling the cyst with perirenal fat tissue, we sprayed the cystic concavity with a layer of chemical glue (Glubran®2; GEM) to dry the surgical site (Fig. 6) and secure the flap of perirenal fat to the cyst cavity. No sutures were used to fix the flap to the cyst to avoid injuring the underlying renal parenchyma. An aspiration drainage was left in renal loggia for 24 hours as per protocol. Discharge criteria were complete oral feeds, clear diuresis, and pain control without opioids. Clinical follow-up was carried out on postoperative days 7, 30, 180, and then every year for the first 5 years after the surgery. Ultrasonographic monitoring was performed on postoperative days 30, 180, and then yearly.

Trocar positions for robotic renal cyst deroofing. Standard left/right lateral decubitus position. A four trocars technique was used: three working trocars of 8 mm and one accessory trocar of 5 mm.
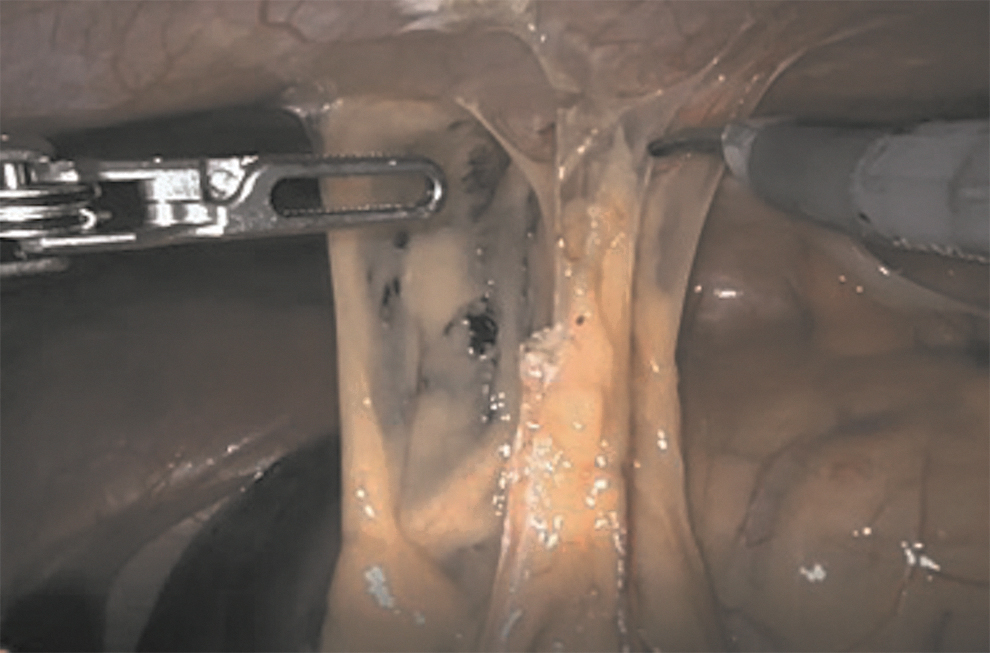
Robotic renal cyst deroofing. Immediate intraoperative finding. Pathological adhesions of epiploon to the abdominal parietal wall in the same side of SRC. They are cautiously taken down using monopolar scissors. SRC, solitary renal cysts.
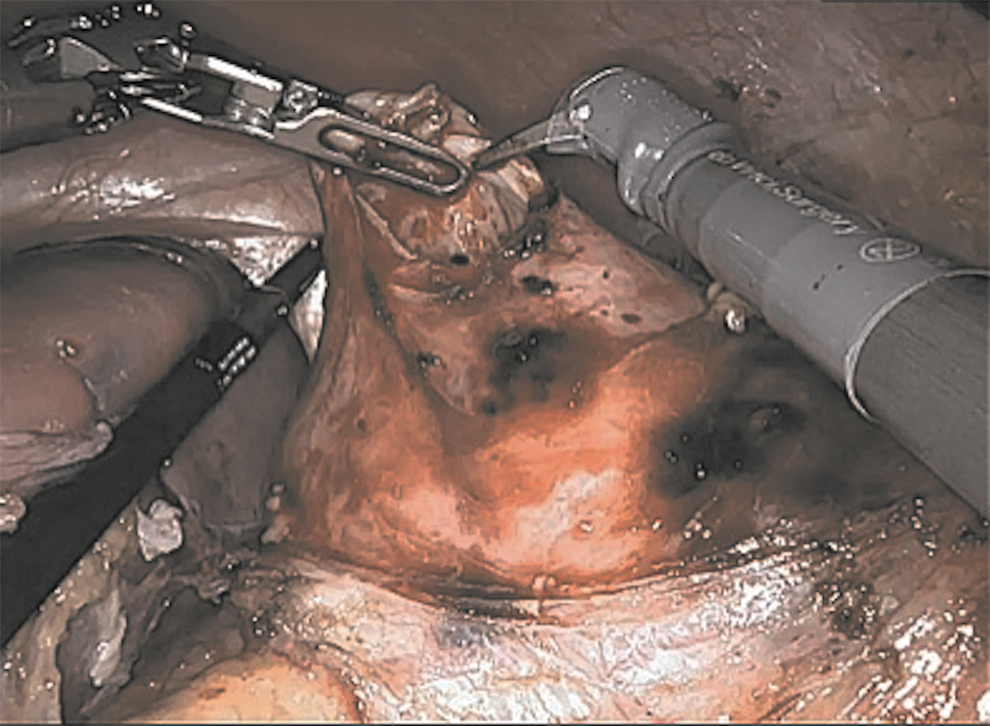
Robotic renal cyst deroofing. Opening and deroofing of the renal cyst with bleeding control using monopolar scissors.
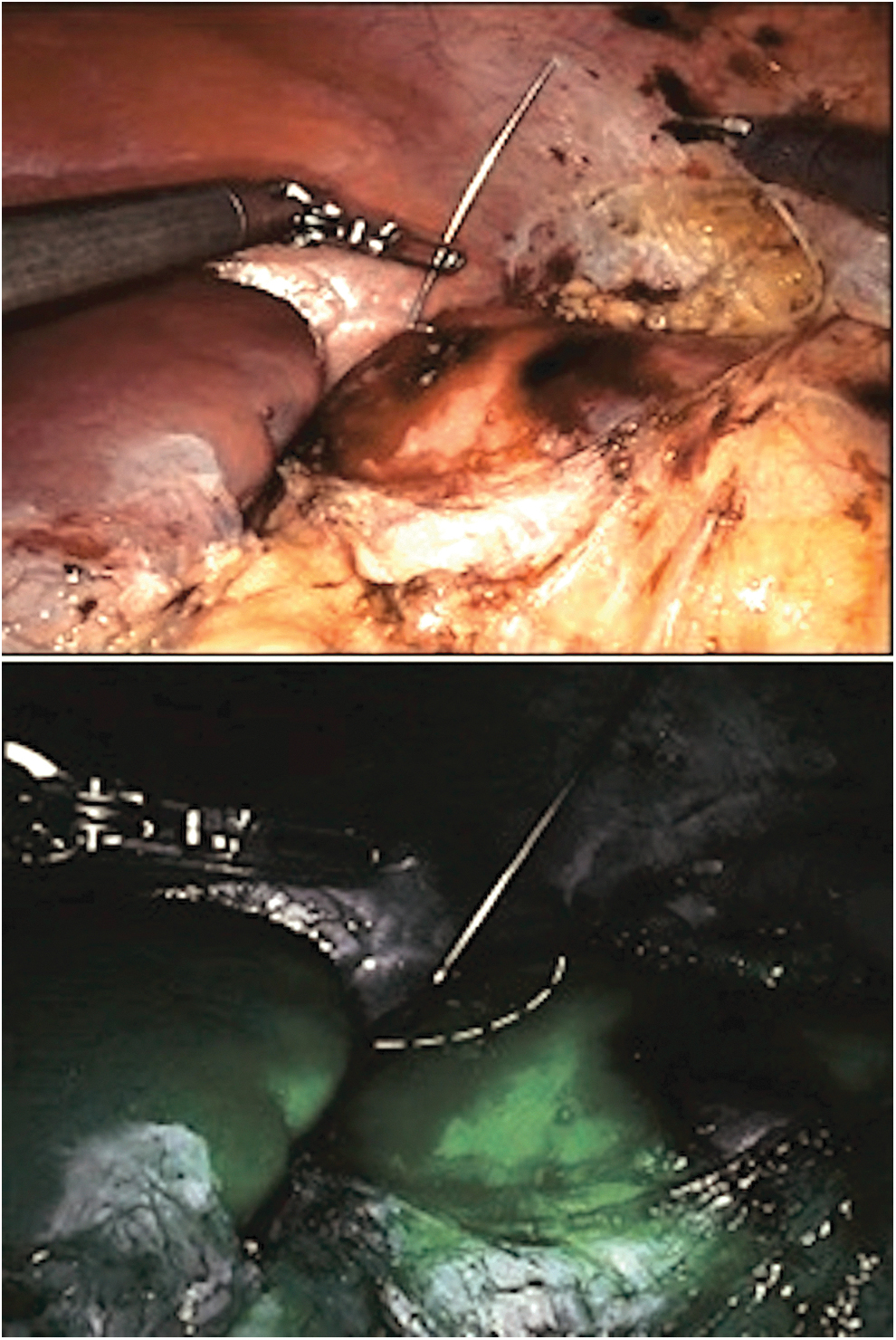
Intraoperative ICG fluorescence during robotic renal cyst deroofing. Top: view of the operative field without ICG fluorescence. The identification of the cyst dome to puncture without damage to the renal parenchyma might be challenging. Bottom: view of the operative field right after the intravenous administration of ICG. Delimitation of the nonvascularized renal cyst from the vascularized renal parenchyma is highlighted with a white dotted line. ICG, indocyanine green.

Robotic renal cyst deroofing. Last step of the surgical procedure. Spraying of the cyst concavity with chemical glue (blue stick) to dry the surgical field. Wadding of the remaining cyst with a pedicled flap of perirenal fat tissue (white arrow).
Results
From 2012 to 2019, 13 patients (9 boys) were surgically treated. Median age at surgery was 8 years, ranging from 5 to 15 years. The median preoperative size was 70 mm, ranging from 42 to 160 mm. Regarding anatomical considerations, 8 SRC (61.5%) were right-sided, 10 (76.9%) located in the upper pole, and 3 (3.1%) interpolar. The 13 cases showed an increase in size of the cyst during ultrasonographic follow-up with worsening of intensity and frequency of the abdominal pain. Hematuria, hypertension, urinary tract infection, or impaired renal function was not registered. No family history of polycystic disease was detected either.
The 13 patients underwent a cyst deroofing through laparoscopic (6 patients), robotic Da Vinci Xi® (4 patients), or retroperitoneoscopic (3 patients) approach. There were no conversions to open surgery. The median operative time was 50 minutes (range 35–90 minutes) for laparoscopic transperitoneal and retroperitoneal deroofing. The median operative time for robotic deroofing was 85 minutes (65–120 minutes) including surgical and docking time. There were no intraoperative complications. The cyst content was clear fluid with no debris. Cytology consistently revealed low cellularity, a few macrophages, and some urothelial cells. The median hospital stay was 2 days (range 36–96 hours). All the patients remained asymptomatic during follow-up (2–42 months). In the first 8 cases, a small amount of liquid in the bottom of the cyst was detected on the US examination. Those cases were managed conservatively due to the absence of symptoms and size stability during follow-up. In the last 5 cases where we performed the fat tissue wadding technique of the cyst, no liquid was detected postoperatively. The histological analysis consistently showed a cyst wall lining of a transitional epithelial type without evidence of malignity, compatible with simple SRC. Macrophages and lymphocytes were also found reflecting a chronic inflammatory status.
Discussion
We presented herein the laparoscopic and robotic management of 13 pediatric cases of symptomatic simple SRC, one of the largest surgical series published in the literature to the best of our knowledge.9,11,14 Only 1 case of robotic treatment of a pediatric SRC has been published so far. 15 We contributed two novel modifications to the surgical technique that have not been described in pediatric series yet: the ICG fluorescence technique to guide the procedure and the fat tissue wadding of the cyst to reduce the recurrence rate after deroofing.
The patients' characteristics were consistent with prior epidemiological studies. SRC affected predominantly males,11,17 aged around 8 years,5,9,13 and were mostly located in the upper renal pole.6,18 The 13 cases presented with abdominal or flank pain. 95% of SRC have a silent course though. 13 This observation could be explained by the fact that we only studied symptomatic and, hence, surgically treated cases. Hematuria, hypertension, recurrent urinary infection, urinary tract obstruction, palpable mass, or impaired renal function was not detected in our series as they are infrequent manifestations of SRC.4,5,13 No case was related to familiar or syndromic conditions such as autosomal dominant polycystic kidney disease or tuberous sclerosis complex.7,8 Every SRC increased in size during follow-up in our series. The high rate of progression did not match with prior reports, where SRC mostly remained stable.5,6,11,13 This observation is the result of a surgical series, not of an epidemiological one. The indications in the literature for treatment of simple SRC in children include abdominal pain and/or SRC-related complications such as hemorrhage, infection, rupture, or arterial/vein compression. 5 No SRC-related complications were detected in our series as they are unusual (0%–4%).4,13 Conservative management based on clinical and US follow-up was carried out until the patient showed clinical worsening or the SRC was at risk of traumatic rupture secondary to its massive size. A CT or an MRI, depending on the radiologist experience and availability, was then performed to reassess Bosniak's category and to plan a surgical strategy. Our choice of management and assessment of Stages I–II SRC was supported by the previous literature. The modified Bosniak classification has been widely accepted to assess SRC in children based on US, 5 CT, 9 or MRI4,19 findings. All pediatric malignant cystic tumors described in the literature were initially classified as Stage III or more,5,9,10 and there is no evidence of malignant transformation so far. 9 Stages I–II SRC can therefore be managed conservatively if asymptomatic and stable. If treatment is needed, the evacuation of SRC and relief of symptoms are the therapeutic target not the excision.
Even though percutaneous techniques have already been used in pediatrics to treat simple SRC, we managed all our cases through minimally invasive approach when treatment was needed. This choice was endorsed by previous literature. US- or CT-guided percutaneous aspiration of SRC showed 90% recurrence rate due to the secretory epithelium lining the cystic wall. 20 The use of sclerosant agents such as tetracycline, 99% ethanol hypertonic saline, or doxycycline 14 as adjunct therapy has lowered the recurrence rate to 43%.20–22 However, serious adverse effects secondary to the use of ethanol have been described, such as systemic absorption, calcification, or pain. However, the laparoscopic deroofing of SRC has shown lower recurrence rate (19%), minimal invasiveness, lower morbidity, and earlier recuperation compared with percutaneous therapy in adults. 23 Pediatric cases of SRC deroofing have already been reported through either transperitoneal or retroperitoneal approach11,14 with encouraging outcomes.
Concerning the surgical approach, the use of laparoscopy or robotics relied on SRC location, surgeon's experience, and availability of robot. Previous surgical literature on SRC is scarce and heterogeneous.11,14 Laparoscopic transperitoneal SRC deroofing is probably the easiest surgical strategy. However, posterior SRC may have a better access through retroperitoneoscopy. For those who have access to a surgical robot, robotics enables precise and careful tissue dissection and manipulation, comparable outcomes with laparoscopic approach and optimum ergonomics. One previous case of robotic deroofing 15 and now 4 cases of our series confirm that robotic approach is feasible and safe. If we analyze the surgical time, robotic is faster than laparoscopic approach, but patient preparation, docking time, and removal of robot are still longer than standard laparoscopic preparation. The experience in robotics will shorten this gap.
Pathological adhesions of epiploon to the parietal abdominal wall on the same side of the SRC were found in big bulky cysts. Interestingly, the pathology specimens of cyst wall showed several degrees of chronic inflammation infiltration. We hypothesize that those adhesions may be secondary to previous episodes of cyst inflammation and abdominal pain. This specific finding has never been described so far.
The use of ICG fluorescence technique to guide surgical procedures has recently started in pediatrics.24,25 In this particular case, the ICG fluorescence enabled to identify the nonvascularized SRC from the vascularized renal parenchyma. Consequently, SRC evacuation and deroofing were safely performed without major bleeding or damage to the renal parenchyma. This specific application of the ICG fluorescence is even more useful in giant SRC where renal architecture is distorted. This is the first published series so far.
Small amount of residual fluid was detected in the remaining concavity of the SRC after deroofing in long-term follow-up in the first 8 cases. From previous investigations, we know that the secretory activity of the remaining cyst wall after deroofing may explain the residual liquid and the risk of recurrence by becoming adherent to surrounding tissues. 26 Fulguration of the base of the cyst after deroofing to prevent recurrence is not recommended because of the risk of fistulization with the major renal vessels or collecting system. 27 A randomized trial proved that the insertion of a wad of fat tissue into the base of the cyst reduces the risk of cyst recurrence in adults. 28 Even though the follow-up time is still too short, we hypothesize that both the chemical glue spraying and the fat wadding of the SRC may play a role in preventing recurrence.
Despite the lack of consensus and official guidelines to manage SRC, we can conclude from the literature the following statements. Given the low risk of malignancy (<1%)5,9 and complications (<5%),4,13 conservative management of asymptomatic and simple SRC should be the first-line treatment. Hematuria, hypertension, impaired renal function, and syndromic or genetic conditions should be ruled out. Sonographic follow-up appears to be suitable in children, especially in the first 2 years after diagnosis in young children with SRC >2 cm at diagnosis. 13 The US-modified Bosniak classification is a reliable tool to differentiate between Stages III–IV and Stages I–II SRC. 5 We suggest the follow-up of Stages I–II SRC with serial US, in the absence of any change in the cyst morphology or patient symptoms. CT is warranted in all children with US-indeterminate findings or consistent with a Stage III or Stage IV cyst.9,10 All Stages III–IV or symptomatic Stages I–II SRC should be treated. If surgical intervention is considered, a single-phase, delayed, postcontrast CT scan is suggested to rule out a calyceal diverticulum (potential for either percutaneous or retrograde fulguration) or communication with the urinary tract. In case of symptomatic Stages I–II SRC, minimally invasive cyst deroofing has high successful rate, low morbidity rate, and early recuperation. 23 Percutaneous aspiration with sclerotherapy has lower success rate.20–22 In case of Stages III–IV SRC, complete excision of the lesion is mandatory to rule out histological features of malignancy.
This study has some limitations that need to be highlighted. Only 13 patients have been reviewed, and follow-up is relatively short (range 2–42 months) especially in robotic cases. Even though strong conclusions cannot be drawn from our results, this is a preliminary report with positive outcomes about robotic approach, ICG fluorescence, and fat wadding technique of SRC. We expect that those results will be endorsed by long-term follow-up and new cases in the future.
To conclude, laparoscopic or robotic cyst deroofing is the first-line treatment for symptomatic Stages I–II renal cysts. Robotic approach is safe, feasible, and has proven successful. The ICG fluorescence guides the evacuative puncture and deroofing of the cyst, preventing major bleeding or damage to the renal parenchyma, especially in giant renal cyst where renal architecture is distorted. We suggest the use of a perirenal fat tissue wadding technique stabilized with chemical glue to reduce the recurrence rate after deroofing.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.