
Abstract
Introduction:
Robotic-assisted surgery (RAS) is increasingly used in adulthood but its application in pediatric population is limited. We report our initial experience in pediatric RAS, focusing on conversions to analyze their causes.
Methods:
All pediatric patients who underwent RAS between June 2015 and April 2019 were included, analyzing demographics, comorbidities, previous surgery, and intraoperative surgical and anesthetic parameters. A three-arms robotic technique was used in all cases. Additional laparoscopic ports were added, when needed. The surgical team did not change during the program, whereas the anesthesiology team varied.
Results:
Thirty-nine patients (23 females, 16 males; mean age ± SD = 9.33 ± 4.73 years [range = 1–16]; mean weight ± SD = 35.2 ± 20.0 kg [range = 9–85]) underwent 40 different procedures (18 gastrointestinal, 15 urogynecological, 5 oncological, and 2 miscellaneous). Three procedures (7.5%) were converted to open surgery for inadequate working space (two marked bowel distension and one insufficient hepatic retraction). Converted patients were of significant lower age (mean ± standard error of mean [SEM] = 2.97 ± 1.03 versus 9.83 ± 0.77 years, P = .01) and lower weight (mean ± SEM = 11.83 ± 1.74 versus 35.47 ± 3.16 kg, P = .03). The two groups did not differ statistically for duration of facial mask ventilation before intubation (mean ± SEM = converted 10.67 ± 2.33 versus completed 10.31 ± 0.91 minutes), neuromuscular block dosage (rocuronium; mean ± SEM = converted 0.46 ± 0.06 mg/kg versus completed 0.62 ± 0.03 mg/kg) and in the type of bowel preparation (mechanical and/or pharmacological).
Discussion:
Conversion rate in initial pediatric RAS program is acceptable. In children, the need for conversion is mainly because of inadequate working space, particularly in smaller children, but it seems not to be influenced by measurable anesthetic factors or different regimen for bowel preparation.
Introduction
Robotic minimally invasive surgery has been rapidly adopted for a wide variety of surgical procedures in adult patients across a broad spectrum of surgical specialties. This has occurred despite the high costs and uncertain benefits of surgical robotics.
The first case of robotic minimally invasive surgery in children was a Nissen fundoplication that was performed in July 2000 and reported in April 2001. 1 Since that time, robotic procedures have been adopted by select pediatric surgical specialists. Pediatric surgical disciplines have been much slower to embrace this new technology. Most children's hospitals do not possess a surgical robot, because of financial reasons, many pediatric units borrow them from the adult programs, with variable scheduled rotation from one to three times a month. 2 With such a limited access of robotic facilities for pediatric surgeons, there is a risk of a longer learning curve and higher conversion and complication rates. In the first comprehensive single-institution paper on pediatric robotic-assisted surgery (RAS), an open conversion rate of 12% was reported for the entire series (12% of abdominal cases and 9% of thoracic case), mainly because of unexpected anatomic difficulties. 3 In the first large pediatric literature review, a total of 2393 robotic-assisted procedures were reported in 1840 children, with a net overall conversion rate of 2.5%. 4 Recently, more consolidated monocentric experience of pioneers of robotic approach in pediatric conditions, reporting a 5% conversion rate in children weighing <15 kg (versus 2% in heavier children) found that with some adjustment in patient position and in trocar placement, robotic surgery is feasible in small children, 5 despite the lack of dedicated smaller instruments.
We aimed to analyze the conversion rate and its reasons in the experience of a pediatric surgical unit with a limited access to scheduled robotic-assisted procedures.
Materials and Methods
Our tertiary care pediatric surgical unit participated in the program of RAS of our General Hospital, which started in the summer of 2015. The hospital acquired the Da Vinci Surgical System Xi in 2016, after using the loaned Si Da Vinci Surgical System for 1 year. The system was shared with different surgical specialties for adults (general, thoracic, gynecology, urology, and ENT surgery). Pediatric elective cases for robotic procedures were scheduled one to two times per month.
Surgeons and the nursing staff underwent a training course before starting. The surgical staff involved in the robotic program had a previous limited experience in advanced minimally invasive procedures. A mentorship from national experts was arranged for the first pediatric robotic cases.
Study period and patient selection
The study period lasted from June 2015 to April 2019. No IRB approval was necessary for this observational longitudinal nonprofit study. All pediatric robot-assisted procedures performed under the care of a senior pediatric surgeon (P.L.C.) were recorded in a standardized prospective database, analyzing preoperative, intraoperative, postoperative medical, surgical, and anesthetics details. Procedures were divided into gastrointestinal, urological, oncological, and other categories. Case selection was based on surgeon's preference; the choice was not randomized but based on the surgeon's attitude. Only elective patients were included, after obtaining appropriate informed written consent from parents or caregivers. The duration of surgery, possibility of conversion and potential complications were explained. Previous medical history, surgery, and scarring, comorbidity and risk factors were recorded for each patient.
All patients underwent bowel preparation before surgery, either mechanical (saline enemas) or pharmacological (oral Picoprep™: sodium picosulfate, magnesium oxide, citric acid), depending on patients' age and neurological status. The mechanical preparation was used for younger and less compliant patients and the pharmacological method for older and better compliant patients.
Anesthetic protocol
Patients older than 1 year received oral premedication 30 minutes before surgery with midazolam (0.5 mg/kg).
Surgery was performed under general anesthesia with endotracheal intubation, controlled ventilation, and muscle relaxation. In smaller children, the induction phase was preferentially with inhalant delivered with a facial mask (sevofluorane+O2) followed by intravenous propofol (3 mg/kg). Neuromuscular blockade was obtained with rocuronium (0.4–0.6 mg/kg). During surgery, patients were routinely monitored for body temperature, respiratory and hemodynamic parameters, electrocardiography, and urine output. The anesthetic teams (physician and nurse) were not consistent during the study period.
Surgical protocol
The correct position for the patient, assistant surgeons, theatre team, and equipment was planned according to the type of the procedure. Special attention was given to the pressure points. Proclive position was used for upper abdominal surgery, Trendelenburg position for gynecological and lower abdominal procedures, and oblique position for renal surgery. The surgical team members did not change during the entire program (same senior surgeon at console and 2 consultants with the patient, simultaneously or individually with trainee). One 12 or 8 mm reusable camera port was placed usually in the umbilical region with an open technique, a CO2 pneumoperitoneum was established with a humidifier insufflator from 0.5 to 3 L/mL CO2 flow rate. Intra-abdominal pressure was set at 10 mmHg. A 30° telescope was the preferred scope for the surgeon. Two 8 mm reusable working ports were placed under endoscopic camera vision. For additional retraction, suction, irrigation, insertion, and cutting of sutures, an additional accessory valve-less port (5 or 12 mm, Airseal trocar; Conmed™) was used. A retractor (Reveel™ or PretzelFlex™) for the liver or colon could be applied through a stab incision, especially for upper gastrointestinal or right kidney surgery procedures. A preliminary gastroscopy or cystoscopy was performed in some cases of Nissen fundoplication and pyeloplasty, respectively, as needed. Solid organs, like adrenal gland and kidney, or neoplasia were recovered from the umbilical incision through a retrieval endo-bag. At the end of the procedure, the wound was closed in layers, first the primary port, then the others.
All patients received postoperative analgesic infusion for 48 hours, continuing with oral analgesia, if necessary. They were discharged when clinically stable and a follow-up was arranged for each child, with or without investigations.
Data collection
Information about robotic procedures were extracted from the datasheet. Data were recorded prospectively for each patient in a digital format. Each patients' demographics (age, sex, and weight at surgery), preexisting conditions, preoperative investigations, surgical details, robotic and laparoscopic instruments, timing (patient in theater, patient positioned, skin incision, docking of robotic system, start of surgery, and end of surgery), and length of robotic procedures (surgeon console time) were noted. All data about conversion were collected. Any intraoperative complications were recorded. Information about preoperative preparation, including bowel preparation, type of anesthesia, and ventilation time during the induction phase, medications used during the procedure, monitoring, and postoperative analgesia were all recorded.
Statistical analysis
Data were reported as percentage for categorical variables and as mean and standard deviation (SD) or mean and standard error of mean (SEM) for the continuous variables. Differences in the frequencies of each categorical variable were evaluated by Fisher's exact test; unpaired t-test was used for continuous variable. A value of P < .05 was considered statistically significant (95% confidence interval [CI]).
Statistical analysis was performed with the GraphPad Prism version 7.0 (GraphPad Software, San Diego, CA).
Results
A total of 39 pediatric patients (16 male and 23 female) underwent 40 different types of robotic procedures during the study period. Mean ± SD age at surgery was 9.33 ± 4.73 years (range = 1–16 years), mean ± SD weight was 35.2 ± 20.0 kg (range = 9–85 kg). Patient demographic data and outcomes (overall operative time, console time, and length of hospital stay) for each group (gastrointestinal, urogynecological, oncological, and miscellaneous) are given in Table 1.
Demographic Data, Operative Times, and Length of Hospital Stay Divided According to Type of Procedures (Gastrointestinal, Urogynecological, Oncological, and Miscellaneous)
ANOVA, analysis of variance; GI, gastrointestinal; O, oncology; M, miscellaneous; SD, standard deviation; UG, urogynecology.
Eleven of 39 patients (28.2%) had preexisting significant medical comorbidities, such as neurological impairment (8), epilepsy (1), congenital heart malformation (1), and food disorder+depression (1). Nine of 39 patients (23%) had previous surgery and abdominal scarring, such as Nissen fundoplication (3), pyeloplasty for controlateral hydronephrosis (1), splenic cyst marsupialization (1), esophageal atresia repair (1), adhesiolisis for hydronephrosis (1), Soave procedure for Hirschsprung disease (1), and contralateral surgery for renal duplex system (1).
We performed a predominance of gastrointestinal (45%) and urogynecological (37.5%) procedures, but we performed also oncological procedures (12.5%; Table 1).
A total of 18 gastrointestinal procedures were performed, including Nissen fundoplication (13; 3 of which were redo after a failed open procedure), Heller–Dor myotomy (1), gastric cyst enucleation (1), 6 partial splenectomy for recurrent splenic cyst (1 case, previous laparoscopic marsupialization), a combined splenectomy and cholecystectomy for hereditary spherocytosis for symptomatic gallbladder stones (1).
A total of 15 urogynecological procedures were performed, including Anderson–Hynes pyeloplasty (8; of which 1 was a redo procedure), vascular hitch for hydronephrosis (1), parapielic adhesiolisis for extrinsic pelvi-ureteric junction obstruction (2), nephroureterectomy for hydronephrosis and nonfunctioning kidney (1), pyelogenic cyst marsupialization (1), hemi-nephroureterectomy for nonfunctioning upper pole duplex system (1), ovarian functional cyst enucleation (1), and salpingectomy for hydrosalpinx secondary to previous pelvic surgery for Hirschsprung's disease.
A total of five oncological procedures were performed, including enucleation or tumorectomy of solid mass (four; namely pheocromocytoma, solid pseudopapillary tumor of the pancreas [Frantz's tumor], and two ovarian dermoid cysts), and adrenalectomy for another pheocromocytoma (1).
Two other procedures were performed with robotic surgical assistance in the study period: a median arcuate ligament release, for a median arcuate ligament syndrome (also known as Dunbar syndrome) and the excision of a subdiaphragmatic pulmonary sequestration.
The mean ± SD operative time for the entire series was 262.6 ± 117.9 minutes (range = 90–560) and the mean ± SD console time was 223.7 ± 101.6 minutes (range = 30–445). The mean ± SD hospital stay was 8.25 ± 5.797 days (range = 2–24).
For calculation of timing we excluded converted cases.
Conversions
There were three conversions, resulting in an overall conversion rate of 7.5%. No conversion was the result of intraoperative complications or robotic malfunction.
The first conversion was in a 4-year-old male neurologically impaired patient, with gastroesophageal reflux, because of a hugely distended intestine that did not allow an optimal visualization. The second conversion was during a Nissen fundoplication in a 2-year-old female neurologically impaired patient with West's syndrome. The procedure was converted owing to suboptimal visualization because of inadequate liver retraction. The third conversion was a 1-year-old female patient with a subdiaphragmatic extralobar sequestration. The conversion was because hugely distended bowel loops obstructed the view. All conversions were in the early operative phase of the procedure. Because of the lack of adequate working space, we did not consider conversion to the laparoscopic approach.
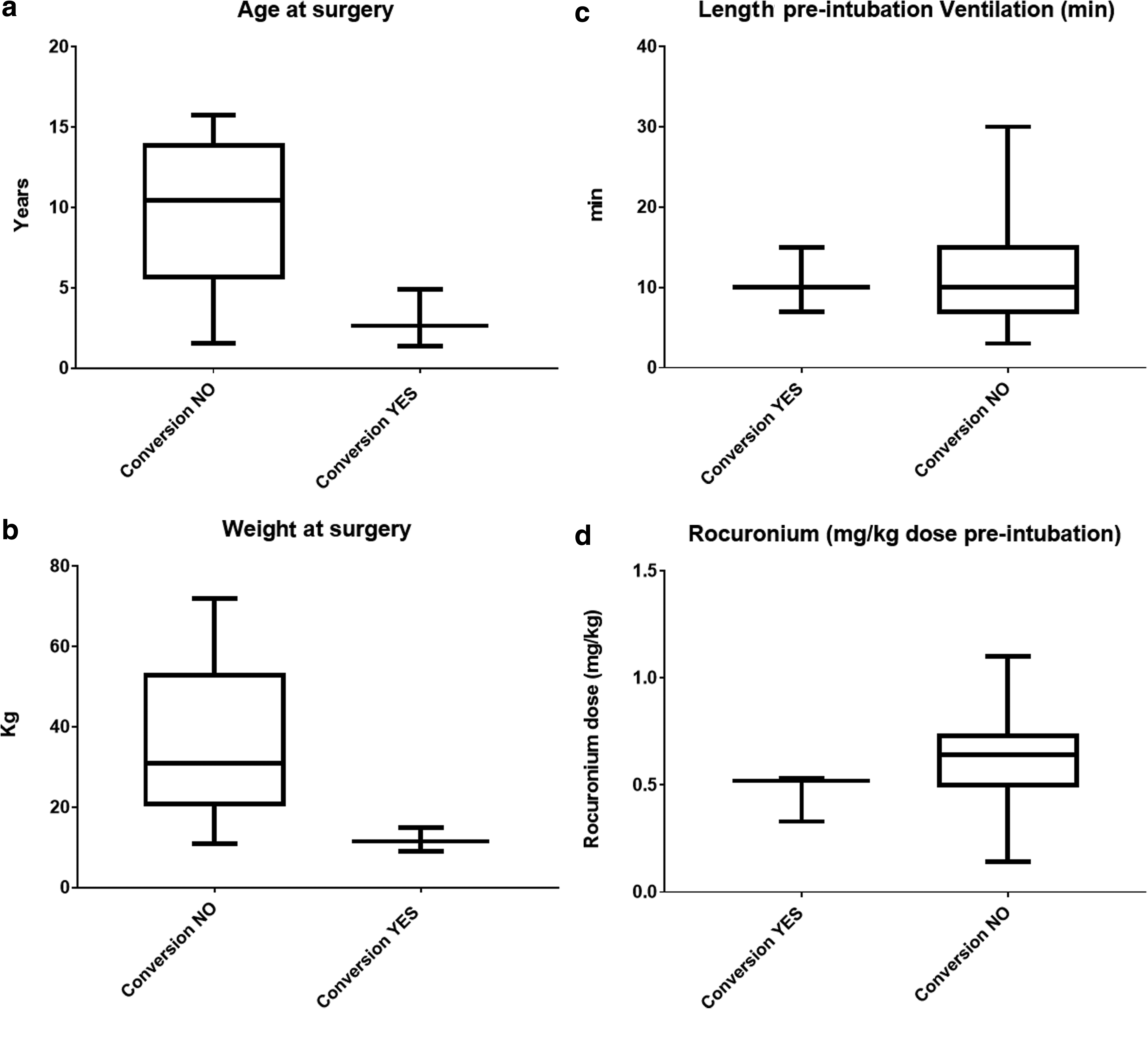
The mean ± SEM age of converted patient group was 2.97 ± 1.03 years, significantly younger than the nonconverted patient group (9.83 ± 0.77 years; P = .01; differences between mean values = −6867 ± 2627, 95% CI = −12.2 to −1.534) (Fig. 1a). The mean weight ± SEM of converted patient's group was 11.83 ± 1.74 kg, significantly lower that mean ± SEM weight of nonconverted cases (35.47 ± 3.16 kg; P = .03; differences between mean values = −23.63 ± 10.33, 95% CI = −45.24 to −2.027) (Fig. 1b).
Conversion to open surgery was more common in neurologically impaired children (2 of 8) compared with neurologically normal patients (1 of 31). However, the difference did not reach statistical significance (Fisher's exact test).
Bowel preparation was mechanical with enema in 21 patients (3 of which underwent conversion), pharmacological in 16 patients, undetermined in the remaining 2 cases. The type of bowel preparation between the two groups (converted versus not converted) proved not to be statistically significant (Fisher's exact test).
To evaluate the role of anesthetic aspects in the pathogenesis of inadequate working space, we compared the converted and nonconverted groups for variables such as the duration of facial mask ventilation at the induction phase (for bowel dilatation; mean ± SEM = 10.67 ± 2.33 versus 10.31 ± 0.91 minutes, respectively; P = ns; differences between mean values = −0.3524 ± 3.193, 95% CI = −6828 to 6123) (Fig. 1c) and rocuronium dose (for abdominal muscle relaxation; mean ± SEM = 0.46 ± 0.06 versus 0.62 ± 0.03 mg/kg, respectively, P = ns; differences between mean values = 0.1597 ± 0.1089, 95% CI = −0.06115 to 0.3806) (Fig. 1d).We did not find a statistically significant difference between converted and nonconverted patients.
Comparing the trend of conversions during the entire study period, we could not observe any statistically significant difference between the different years of the study period (0 of 5 in 2015, 1 of 12 in 2016, 1 of 11 in 2017, 1 of 10 in 2018, 0 of 2 in 2019, chi-squared test).
Discussion
Robotic surgery is an established approach in adult practice, especially in urology and gynecology.
The use of the Da Vinci® Surgical System in clinical practice for children's surgery is not widespread. Since the first case of robotic-assisted laparoscopic Nissen fundoplication in a child, robotic procedures have been slowly adopted by select pediatric surgeons. In the last few years, the number of centers establishing a robotic program in children is growing. The number of publications about the safety and effectiveness of this technology are also increasing.
Conversions owing to mechanical and electronic malfunctions or any other issues related to the technology would raise immediate safety concern. 7 Alemzadeh et al. recently reviewed the adverse robotic adult surgery events reported in the U.S. Food and Drug Administration (FDA) database from 2000 to 2013. They reported that procedures conversion or interruption was because of device malfunctions in 75.9% cases, in 13.1% cases it was because of patient injuries, and in 1.4% cases because of patient death; the incidence of conversion was higher in more complex surgeries, such as cardiothoracic and head and neck. 8 Although a single-center experience from our study cannot possibly be compared with a 13-year FDA database, the data from our series show the reliability of the robot in children's surgery.
Previous large pediatric laparoscopy series described a one-to-one-relation between conversions and complications.9,10 In our series, conversions were not related to the intraoperative complications and none of them was related to robotic technology.
Meta-analyses comparing outcomes between robot-assisted and conventional laparoscopic fundoplication and pyeloplasty procedures in children have found no significant differences in conversion rates.11,12
Overall conversion rates of pediatric RAS published in literature range from 1.3% to 13.5%.3,13–15 Our overall conversion rate of 7.5% (3 of 40 procedures) is comparable with these data.
Our sample of patients showed that smaller children undergoing robotic surgery have a higher risk to be converted to open surgery during the procedure and it is probably because of the smaller working space. We found that an inadequate working space is the main cause of conversion. The converted cases were owing to failure to progress with the minimally access approach because of dilated bowel in two cases and a suboptimal liver retraction in another case, with a lack of safe operative space and poor vision.
Gaseous distension of the gastrointestinal tract is a problem in robotic surgery, especially in small children and neonates where the operating space is limited and currently available robotic instruments are relatively large. The bowel dilatation, as a reason for conversion, has been reported by other authors. 16 A suboptimal anesthetic technique, including poor muscle relaxation, could possibly explain this lack of adequate working space for the surgeon. In our series we analyzed possible measurable factors influencing bowel dilatation, such as the type of bowel preparation (mechanical or pharmacological), the length of facial mask ventilation in the induction phase before intubation (for bowel dilatation), and rocuronium dose (for abdominal muscle relaxation), but we did not find a statistically significant difference between converted and nonconverted patients.
The bowel distension, in our series, was not affected by the length of time of facial mask ventilation during the induction phase nor was it because of the type of bowel preparation. A strategy to decrease the negative effect of bowel dilatation could be to apply a fine-needle aspiration to deflate a distended bowel in infants. This approach has been evaluated by a group from Mexico 17 through a prospective randomized controlled trial in patients older than 6 months, scheduled for laparoscopic Nissen fundoplication, in whom severe colonic distension was observed. The authors found this maneuver simple and efficient to decompress a dilated large-bowel loop during laparoscopic surgery, without clinical complications. However, caution must be exercised before suggesting this decompressive maneuver even in the case of distension of the small intestine, as in our two cases, for the obvious infectious risk connected. Without clear clinical data about safety and effectiveness of this maneuver under these circumstances, we would not recommend bowel puncture.
A poor muscle relaxation did not cause any conversion in our series. Neuromuscular blocker did not influence the abdominal cavity dimension during the establishing of the pneumoperitoneum. A Dutch group has studied a standardized-size and a small-size porcine laparoscopy model for the effects of neuromuscular blockade, using computed tomography to measure volumes and linear dimensions. They found no statistically significant effect of neuromuscular blockade on the working-space dimensions in both models.18,19 The same authors studied the effect of CO2 abdominal wall prestretching to increase the working space and found that a previous insufflation of the abdomen with CO2 up to 15 mmHg significantly increase the working-space volume. They found a 21% increase at a repeat intra-abdominal pressure of 5 mmHg, reducing the negative effects of prolonged high-pressure pneumoperitoneum on the cardiorespiratory system and microcirculation. 20 These studies may suggest that the abdominal wall prestretching is more effective than pharmacological muscles blockade in achieving an effective working space volume.
The role of anesthetic protocols needs to be further investigated, especially for nonmeasurable variables, such as the volume of air introduced into the digestive tract during the induction phase with, for example, the facial mask. It is possible to hypothesize that there may be an effect linked to the interindividual variability in the application of anesthetic procedures, in case of multiple operators, but we have no enough data to analyze this effect.
Other authors have investigated the possible advantages of the smaller (5 mm) robotic instruments. These authors have pointed out that these instruments would not have had any positive effect in the small working space of smaller children, because the 5 mm instruments actually require more space to operate. 5
Our study has some limitations such as a sample size and the retrospective nature of our data collection. Further limitations are because of the patient's selection, with the absence of thoracic robotic procedure in our cases. According to the literature, thoracic procedures have a higher risk of conversion, especially in smaller children 21 or neonatal cases. 5 The urological procedures in our series were for kidneys and none was for infants or for children <18 months of age or weighing <15 kg. In this age group of patients, we consider a small (3 cm) muscle-sparing lombotomic open approach faster than RAS and painless. However, we do not expect that the decision to include urological cases in infants or smaller children would have increased our conversion rate, as already demonstrated in literature that urological procedures are feasible with RAS in this age group with minimal or null risk of conversion.5,22,23 It would be of interest to mention that, unlike other authors with similar degree of experience as us, we have not included in our cohort simple “gateway procedures” such as Palomo for varicocele or cholecystectomy. 24 In addition, we have included benign or locally aggressive oncological conditions in adolescents but, even with these exclusion and inclusion, our overall conversion rate compares favorably with other such publications.
Conclusion
Conversion rate in initial pediatric RAS program is acceptable and is mainly because of inadequate working space, particularly in smaller children. It seems not to be influenced by measurable anesthetic factors or different types for bowel preparation.
Further prospective studies investigating additional reasons of conversion and how anesthetic protocols can affect the robotic performance are necessary. It is mandatory to understand what factors affect the robotic procedures, to assure the best quality of care to our children and to develop a surgical and anesthetic protocol to use with RAS.
Footnotes
Acknowledgments
The authors thank Azad Najmaldin and Naved Alizai from the St. James University Hospital in Leeds, United Kingdom, for their support and precious suggestions during the elaboration of this research project.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.