
Abstract
Background:
Inguinal hernia repair is one of the more common procedures performed in the United States. The optimal surgical approach, however, remains controversial. We aimed to compare the postoperative outcomes and costs between laparoscopic and open inpatient inguinal hernia repairs in a national cohort.
Materials and Methods:
We performed a retrospective analysis of the National Inpatient Sample during the period 2009–2015. Adult patients (≥18 years old) undergoing laparoscopic and open inguinal hernia repair were included. Multivariable logistic, generalized logistic, and linear regression were used to assess the effect of the laparoscopic approach on postoperative complications, mortality, length of stay, and hospital charges.
Results:
A total of 41,937 patients undergoing open inguinal hernia repair (N = 36,575) and laparoscopic inguinal hernia repair (N = 5282) were included. Patients undergoing laparoscopic inguinal hernia repair were less likely to have postoperative wound complications (odds ratio [OR]: 0.64, 95% confidence interval [CI]: 0.41–0.98), infection (OR: 0.34, 95% CI: 0.27–0.42), bleeding (OR: 0.72, 95% CI: 0.63–0.82), cardiac failure (OR: 0.72, 95% CI: 0.64–0.82), renal failure (OR: 0.54, 95% CI: 0.47–0.62), respiratory failure (OR: 0.70, 95% CI: 0.58–0.85), and inpatient mortality (OR: 0.27, 95% CI: 0.17–0.40). On average, the laparoscopic approach reduced length of stay by 1.28 days (95% CI: −1.58 to −1.18), and decreased hospital costs by $2400 (95% CI: −$4700 to −$700).
Conclusion:
Laparoscopic hernia repair is associated with significantly lower rates of postoperative morbidity and mortality, shorter length of hospital stays, and lower hospital costs for inpatient repairs. The laparoscopic approach should be encouraged for the management of appropriate patients with inpatient inguinal hernias.
Introduction
Inguinal hernia repair is the most common procedure performed by general surgeons. Nearly 20 million herniorrhaphies are annually done worldwide and over 800,000 are performed in the United States (US) alone. 1 Despite the wide experience in hernia surgery, reported postoperative morbidity remains high,2,3 and thereby, different techniques and surgical approaches are continuously investigated.
Open inguinal hernia repair with mesh reinforcement has been historically considered the “gold standard,” due to its short learning curve and low recurrence rate.4,5 Since its introduction, laparoscopic inguinal hernia repair has also been demonstrated to be safe and efficient.6–8 Multiple previous studies comparing outcomes between laparoscopic and open inguinal repair have shown contradictory results9–13 and there are no specific guidelines to recommend one method over the other.
The appropriate balance between outcomes and costs should be carefully analyzed for the embracement of a different surgical technique. Based on findings from prior inguinal hernia studies,9–13 we hypothesized the postoperative outcomes after inpatient inguinal hernia repair would be similar for both open and laparoscopic methods, while costs would favor a laparoscopic repair. Therefore, we aimed to compare the postoperative outcomes and costs between open and laparoscopic inguinal hernia repairs in a national cohort.
Materials and Methods
The National Inpatient Sample (NIS) database was used to identify a cohort of patients between January 1, 2009, and September 30, 2015. The NIS is the largest publicly available all-payer health care database in the US, and includes over 7 million hospitalizations from 1000 hospitals each year, representing a 20% stratified sample of all hospital discharges in the US. Eligible patients were identified using International Classification of Disease, 9th revision, Clinical Modification (ICD-9-CM) diagnostic and procedural codes.
Patients ≥18 years of age, with a primary diagnosis of inguinal hernia (ICD-9-CM 550.X), who underwent laparoscopic (ICD-9-Procedure 17.1X, 17.2X) or open (ICD-9-Procedure 53.0X, 53.1X) hernia repair, were eligible for inclusion. Elective and nonelective hospital admissions were both included. Patients whose discharge disposition status was unknown or missing were excluded from the analysis.
Study outcomes were discharge disposition (including inpatient mortality), inflation-adjusted hospital charges, length of stay, and postoperative complications. Postoperative complications were identified by ICD-9 codes and included venous thromboembolism (453.X, V125.1, 415.11), wound complications (998.13, 998.30–998.32, and 998.83), infection (54.91, 86.04, 569.5, 995.9X, 996.64, 998.5, 998.51, 998.59, 999.3X, 567, 567.2, and 567.22), bleeding (99.00–99.09, 998.1, 998.11, and 998.12), cardiac failure (410.X and 428.X), renal failure (38.95, 39.95, 584.X, and V45.11), respiratory failure (31.1, 31.29, 96.04, 96.05, 96.7X, and 799.1), and shock (998.0, 998.00, 998.01, 998.02, and 998.09). In addition, a composite complication variable was created, indicating if any of the above complications was in the discharge record.
Comorbidities considered in adjusted models were identified by ICD-9 codes and included hypertension (401.X and 402.X), diabetes (249.X and 250.X), obesity (278.X), renal insufficiency (585.X), coronary artery disease (414.X), peripheral vascular disease (443.X), chronic obstructive pulmonary disease (491.X and 492.X), sleep apnea (327.23), tobacco abuse (305.1), liver disease/cirrhosis (571.X), anticoagulation use (V58.61), and steroid use (V87.45).
Statistical analysis
Descriptive statistics were calculated for patient and hospital characteristics stratified by surgical procedure. Proportions of postoperative complications and discharge disposition were calculated for each surgical procedure, as were the median length of stay and median hospital charges.
Crude and multivariable analyses of the effect of laparoscopic hernia repair, compared to open hernia repair, on study outcomes were conducted using logistic, generalized logistic, and linear regression models. Multivariable models were adjusted for age, sex, race, insurance, income, comorbidities, hospital size, hospital location/teaching status, and hospital region. Trend analyses were conducted using Poisson regression to analyze how utilization of laparoscopic surgery has changed over time.
All analyses were performed using SAS software version 9.4 (SAS, Inc., Cary, NC), and a P value <.05 was considered significant for all the statistical methods.
Results
A total of 41,937 patients were included, of which 36,575 underwent open inguinal hernia repair and 5282 laparoscopic inguinal hernia repairs. The median age of patients undergoing open and laparoscopic procedures was 69 (interquartile range [IQR]: 55–80) and 66 (IQR: 55–76), respectively (P < .0001). There were no significant differences in gender, race, and presence of comorbidities between patients undergoing open and laparoscopic procedures. Patient and hospital characteristics, stratified by surgical approach, are described in Table 1.
Distribution of Discharge Characteristics Among Adult Patients with Inguinal Hernia, Stratified by Type of Surgical Approach
Median household income quartile based on patient's ZIP code and calendar year.
IQR, interquartile range.
Open procedures, compared to laparoscopic procedures, had a higher incidence of postoperative wound complications (0.8% versus 0.5%, P = .012), infection (6% versus 2%, P ≤ .0001), bleeding (9% versus 6%, P < .0001), cardiac failure (11% versus 7%, P < .0001), renal failure (11% versus 5%, P < .0001), respiratory failure (4% versus 3%, P < .0001), and inpatient mortality (1.8% versus 0.4%, P < .0001). The median length of stay was 3 days (IQR: 2–6) for open procedures and 2 days (IQR: 1–4) for laparoscopic procedures, P < .0001. Incidence of postoperative complications, length of stay, and total hospital charges among adults undergoing open and laparoscopic procedures is shown in Table 2.
Postoperative Complication, Discharge Disposition, Hospital Charges, and Length of Stay Among Patients Undergoing Open and Laparoscopic Hernia Repair
IQR, interquartile range.
After adjusting for patient and hospital characteristics, patients undergoing laparoscopic inguinal hernia repair were less likely to present postoperative wound complications (odds ratio [OR]: 0.64, 95% confidence interval [CI]: 0.41–0.98), infection (OR: 0.34, 95% CI: 0.27–0.42), bleeding (OR: 0.72, 95% CI: 0.63–0.82), cardiac failure (OR: 0.72, 95% CI: 0.64–0.82), renal failure (OR: 0.54, 95% CI: 0.47–0.62), respiratory failure (OR: 0.70, 95% CI: 0.58–0.85), and inpatient mortality (OR: 0.27, 95% CI: 0.17–0.40). On average, the laparoscopic approach reduced length of stay by 1.28 days (95% CI: −1.58 to −1.18), and decreased hospital costs by $2400 (95% CI: −$4700 to −$700) (Table 3).
Crude and Adjusted Effects of Laparoscopic Hernia Repair, Compared to Open Hernia Repair, on Outcomes, Among Adult Patients Presenting with Inguinal Hernia
Adjusted for sex, age, race, insurance, income, hospital region, and hospital.
CI, confidence interval; CIE, change in estimate location, hospital size, and presence of the following comorbidities: hypertension, diabetes mellitus, obesity, renal insufficiency, coronary artery disease, peripheral vascular disease, chronic obstructive pulmonary disease, sleep apnea, tobacco abuse, liver disease, anticoagulant use, and steroid use; OR, odds ratio.
The yearly rate of laparoscopic procedures slightly increased from 12.9% (95% CI: 12.0–13.8) in 2009 to 13.7% (95% CI: 12.6–14.9) in 2015, P = .15 (Fig. 1a). The results from the trend analyses indicate that the trend in the rate of laparoscopic procedures did not significantly differ by hospital rurality and teaching status (P = .15). However, rural and urban non-teaching hospitals did have a lower rate of laparoscopic procedures across the study period (P < .0001 for both, Fig. 1b). Similarly, the trend in the rate of laparoscopic procedures did not significantly differ by the elective status of the procedure (P = .16), but elective procedures had a higher rate of laparoscopic procedures across the study period (P < .0001). Rates of any complication increased from 2009 to 2015 in both the laparoscopic procedure group (P = .0020, Fig. 2a) and the open procedure group (P < .0001, Fig. 2b).

Trend in percent of inguinal hernia surgical procedures that were laparoscopic 2009–2015,
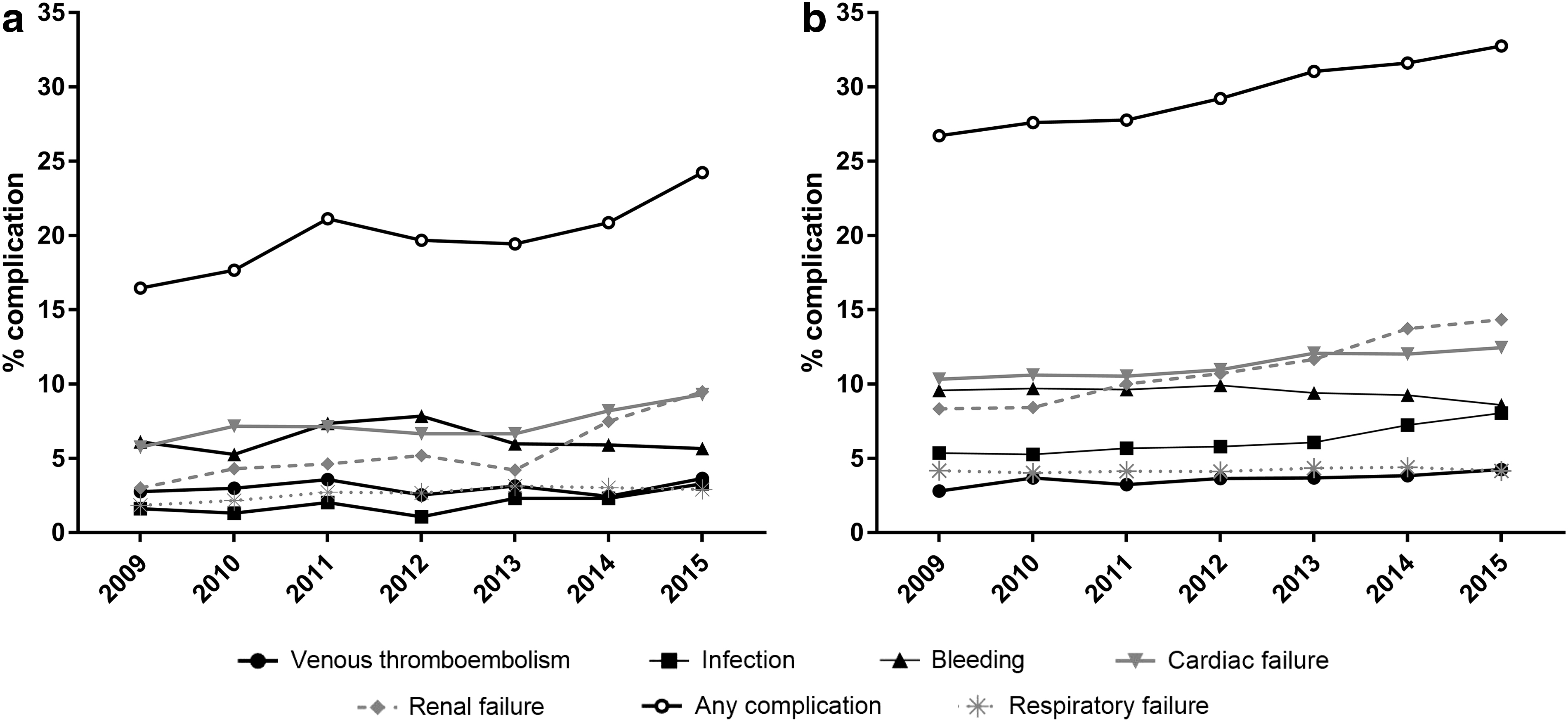
Proportion of procedures resulting in complications, by surgical approach,
Discussion
This large retrospective study using data from the Nationwide Inpatient Sample (NIS) from 2009 to 2015, demonstrated that laparoscopic inguinal hernia repair has favorable outcomes when compared to open inguinal hernia repair in a varied demographic, representative of the US population. Despite the superior outcomes with laparoscopy throughout our study period, the rate of all complications increased, whether the inguinal hernia was repaired open or laparoscopic. In addition, open inguinal hernia repair was more commonly utilized than the laparoscopic method. However, when laparoscopy was utilized, it was more commonly being performed in urban teaching hospitals.
After adjusting for patient factors and hospital characteristics, patients undergoing laparoscopic repair were less likely to develop postoperative wound complications, infections, cardiac failure, renal failure, and bleeding complications. Patients repaired with the laparoscopic method had a shorter length of stay, lower hospital charges, and a higher likelihood of routine discharge to home (in contrast to rehab, nursing facility, or home with home health care) compared to those patients repaired with the open method. Both the European Hernia Society (EHS) guidelines for inguinal hernia repair of 2009 and the more recently published 2018 International guidelines for groin hernia management tout multiple benefits of laparoscopic inguinal hernia repair, while still deferring to a surgeon's experience and expertise when choosing the optimal method of inguinal hernia repair.14,15 Our data demonstrated reduced complications, shorter hospital stays and lower hospital costs with the utilization of laparoscopic inguinal hernia repair. The lower complication rate is in line with findings from Schmedt et al.'s meta-analysis of randomized controlled trials in which laparoscopic repair demonstrated a lower incidence of wound infection and reduced hematoma formation. 16 It must be considered that our data analysis is for all comers, including bilateral hernias, recurrent hernias, primarily repaired open hernias, and female patients.
In a more specific analysis, the HerniaSurge group's comparison of laparoscopic (totally extraperitoneal [TEP] and transabdominal preperitoneal [TAPP]) versus open (Lichtenstein) from randomized control trials in primary unilateral inguinal hernias repaired in male patients demonstrated no difference in intraoperative and postoperative complications. 15 The reduced length of hospital stay is both statistically and clinically significant with over one less hospital day.
Similarly, multiple other studies, including The SCUR Hernia Repair Study, which compared 613 patients randomized to open suture repair, open preperitoneal mesh repair, and laparoscopic TAPP repair, 17 Payne et al.'s prospective trial of 100 patients randomized to laparoscopic TAPP or open tension-free repairs using a polypropylene mesh, 18 and further citations within the EHS and International guidelines14,15 support the laparoscopic advantage of quicker recovery and thus shorter hospital stays. The quicker recovery and the reduced complications in turn reduce the total hospital costs for laparoscopic inguinal hernia repair when compared to open.
Trend analysis demonstrated a gradual increase in complication rates for both laparoscopic and open inguinal hernia repairs (Fig. 2a, b). This may be due to an aging US population with an increased life expectancy 19 and an increased trend in inguinal hernia repair as an outpatient procedure, leaving a sicker and more comorbid population requiring an inpatient hospital stay, which is captured by NIS data. Multiple guidelines14,15 have recommended and multiples studies20–22 have shown an increased trend toward outpatient inguinal hernia repair. Despite the slight increased complications, laparoscopic repairs demonstrated a continued lower complication rate when compared to open inguinal hernia repairs.
Laparoscopic inguinal hernia repair is not all too new. It was first introduced by Ger in 1982 using a simple closure of the internal ring with a metal clip. 23 This simple repair method evolved into the two most common laparoscopic methods of inguinal repair used currently: the TAPP approach described by Arregui in 1991 24 and the TEP approach described by Dulucq in 1991. 25 Despite high rates of adoption of laparoscopy in other general surgery procedures, 96% of cholecystectomies 26 and 75% of appendectomies, 27 and moderately long duration in practice, our analysis demonstrates that laparoscopic repair has only had a very small increase in its adoption from 12.9% in 2009 to 13.7% in 2015 (Fig. 1a) for use in inguinal hernias. It has been proposed that this reluctance of adoption is due to lack of training, perceived minimal benefits, and increased resource requirements. 28
Our data show that laparoscopic inguinal hernia repair is more commonly utilized in urban-teaching hospitals, followed by urban nonteaching hospitals, and then rural hospitals. This is fairly in line with Trevisonno's survey of general surgeon practice patterns, in which surgeons in urban nonteaching hospitals (59%) and in university/academic hospitals (57%) were more likely to perform laparoscopic inguinal hernia repair than those in rural hospitals (44%). 28
One would assume, that as more surgical trainees graduate from residency, there would be a corresponding increase in the adoption of laparoscopic inguinal hernia repair. However, despite increased training of senior-level residents in the US now performing more laparoscopic inguinal hernia repairs than open 29 and an 87.% increase in laparoscopic hernia repairs by chief residents from 1999 to 2008, 30 there has been a stagnant, although minimally increased, use of a laparoscopic method of repair for inguinal hernias.
Even with increased residency training exposure to laparoscopic inguinal hernia technique, it may have still been inadequate. It has been proposed that, compared to open repairs, the laparoscopic inguinal hernia repair learning curve required between 50 and 100 procedures to gain proficiency. 14
Based on the most recent change in the Accreditation Council for Graduate Medical Education (ACGME) requirements for the 2017–2018 academic year, general surgery residents must have a minimum of 85 hernia repairs (open or laparoscopic) and a minimum of 75 laparoscopic complex procedures (inguinal herniorrhaphy, incisional herniorrhaphy, antireflux procedures, bariatric procedures, enterolysis, colon procedures, and solid organ surgery). 31 The previous minimum graduating requirement for complex laparoscopic procedures had been 25, which was instituted in 2008, and before that, it had been 0. 32 With these increased training requirements, future analysis may show an even greater increase in the utilization of laparoscopic inguinal hernia repair.
This study does have some limitations, which are inherent to any large retrospective database. In an era where elective inguinal hernia repair has become more commonly performed as an outpatient procedure and emergent and urgent cases for obstructed or strangulated hernias are performed open are more commonly admitted for inpatient monitoring, NIS data are limited to inpatient procedures and this can be a potential for selection bias. Despite the growing use of robotic hernia repairs, the ICD-9 coding for robotic repair is nonspecific and not routinely applied, and was not evaluated in our study. As an administrative database, information from the NIS does have potential for data entry and coding errors.
Data from the NIS are restricted to patient information for each surgery only for the duration of the hospital stay up until discharge. No further follow-up information is available, such that nay events after discharge will not be captures. This can be somewhat problematic, as postoperative complications often occur after discharge in the setting of a short hospital stay. Even more so, laparoscopic patients are discharged sooner than open, decreasing the window in which complications can arise and be accounted.
As a cross-sectional retrospective analysis, preoperative decision making for selecting laparoscopic or open repair methods is unable to be determined. Specific surgical methods and outcomes important to hernia repair, such as laparoscopic totally extraperitoneal versus transabdominal placement of mesh, open Lichtenstein versus Bassini repair, hernia recurrence, postoperative pain, and other patient-reported outcomes are not available for analysis within the NIS data.
This study demonstrates that laparoscopic inguinal hernia repair is associated with a significantly lower rate of postoperative morbidity and mortality, shorter length of hospital stays, and lower hospital expenses for inpatient repairs. It provides additional support demonstrating the benefits and improved outcomes of laparoscopic inguinal hernia repair when compared with an open method even in the inpatient setting. Despite a growing body of evidence to encourage the use of laparoscopy, there is a disproportionate utilization of the open method of inguinal hernia repair. The laparoscopic approach should be encouraged for the management of appropriate patients with inguinal hernias and its continued adoption bears to be seen as surgical trainees' exposure to minimally invasive methods continues to grow.
Footnotes
Acknowledgments
The authors would like to thank Dr. Marco Patti for his support in this project and editing of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.