
Abstract
Background:
Reports on preoperative progressive pneumoperitoneum (PPP) and botulinum toxin A (BTA) for managing giant inguinoscrotal hernias are limited. Hence, we report our experience with these preoperative techniques in patients with this condition.
Materials and Methods:
Observational study of 8 consecutive patients with giant inguinoscrotal hernias between January 2018 and December 2018. All patients were treated preoperatively with BTA injection to the lateral abdominal wall muscles and PPP for passive abdominal cavity expansion. Length of abdominal wall muscles, volume of inguinal hernia (VIH), volume of the abdominal cavity (VAC), and VIH/VAC ratio were measured before and after PPP and BTA using abdominal computed tomography. All hernias were repaired laparoscopically using transabdominal preperitoneal (TAPP) repair techniques.
Results:
The mean insufflated volume of air for PPP was 5625 ± 845 mL for 15.4 ± 1.6 days. An average reduction of 5.3% of the VIH/VAC ratio after PPP and BTA was obtained (P < .01). The length of lateral abdominal muscles with a mean gain of 3.3 cm/side (P < .01) and complications associated with PPP were 12.5% and with surgical technique, 25%. Laparoscopic TAPP repair was achieved in all cases, with no clinical evidence of postoperative abdominal hypertension. The mean follow-up was 22 months; no hernia recurrences have been reported.
Conclusions:
Combination of PPP and BTA is feasible and useful for surgically managing giant inguinoscrotal hernias, which can avoid abdominal compartment syndrome after laparoscopic TAPP repair of giant inguinoscrotal hernias.
Introduction
Giant inguinoscrotal hernias rarely occur in developed regions because of early intervention; it is often associated with the rural region.1,2 A giant inguinal hernia is characterized by the following: the inguinal hernia extends below the midpoint of the inner thigh of a patient in a standing position, the front and rear diameters exceed 30 cm, the left and right diameters exceed 50 cm, and it is difficult to return it to the abdominal cavity for >10 years.3,4 This condition can hinder patients' daily life activities, such as walking, sitting, and voiding. A so-called loss of domain hernia (LODH) occurs when it persists for a long time and is impossible to be repaired by a simple technique of fascial closure. If preoperative preparation is inadequate, complete reduction of the herniated viscera can be dangerous because the abdominal pressure may suddenly increase, causing respiratory disorders and sometimes, abdominal compartment syndrome (ACS).5,6 Therefore, adequate preparation before surgery is vital.
Preoperative progressive pneumoperitoneum (PPP), which was introduced by Goñi Moreno, 7 can cause passive abdominal cavity expansion, allowing the viscera to reestablish the right domain and improve the respiratory adaptation. Thus, the risk of ACS, which is a major problem in LODH, can be reduced. 8 Pneumoperitoneum also improves diaphragmatic function, 9 diminishes chronic edema of the herniated intestine and mesentery,9,10 and results in lysis of adhesions.9–11
Muscle relaxation with botulinum toxin A (BTA) injection has recently been reported. BTA is a neurotoxin that blocks the acetylcholine receptor at the neuromuscular junction, resulting in temporary flaccid paralysis of the abdominal muscles and facilitating surgical closure and repair.12,13 The combined use of PPP and BTA has been described in the literature for large incisional hernias; successful outcomes were achieved.14,15 However, there have been few related case reports for giant inguinoscrotal hernias.16,17 Furthermore, the cases of giant inguinoscrotal hernia that have been reported in the literature were mostly treated with an open repair, and endoscopic treatment has been rarely reported.3,18
Thus, the purpose of this observational study was to discuss our experience in preparing patients with giant inguinoscrotal hernias for the combined use of PPP and BTA before endoscopic repair.
Materials and Methods
This single-center prospective study included patients with giant inguinoscrotal hernias who underwent PPP and preoperative BTA abdominal wall injections before elective surgical repair of endoscopic hernia from January 2018 to December 2018. Informed consent was obtained from each patient for inclusion in the study.
Before and after the treatment, the volume of the inguinal hernia (VIH) and volume of the abdominal cavity (VAC) as well as the length and thickness of abdominal wall muscles were calculated from noncontrast 64-slice multidetector computed tomography (CT) using a specific software (Fig. 1). A radiologist, who specialized in abdominal wall scanning, calculated the diameters and volumes according to the abdominal CT findings and the modified index of Tanaka. 19 The axial length of muscles was measured along the deep surface of the abdominal muscle complex from the lateral edge of the quadratus lumborum to the medial edge of rectus abdominis muscle on each side at the same spinal level. Meanwhile, the thickness of the muscle was measured along the midaxillary line from the deep surface of the transversus muscle to the superficial surface of the external oblique muscle. All cases were radiologically assessed by the same radiologist. If the VIH/VAC ratio was higher than or equal to 20%, regardless of the size of the hernia defect, he was included in the protocol of preoperative techniques.
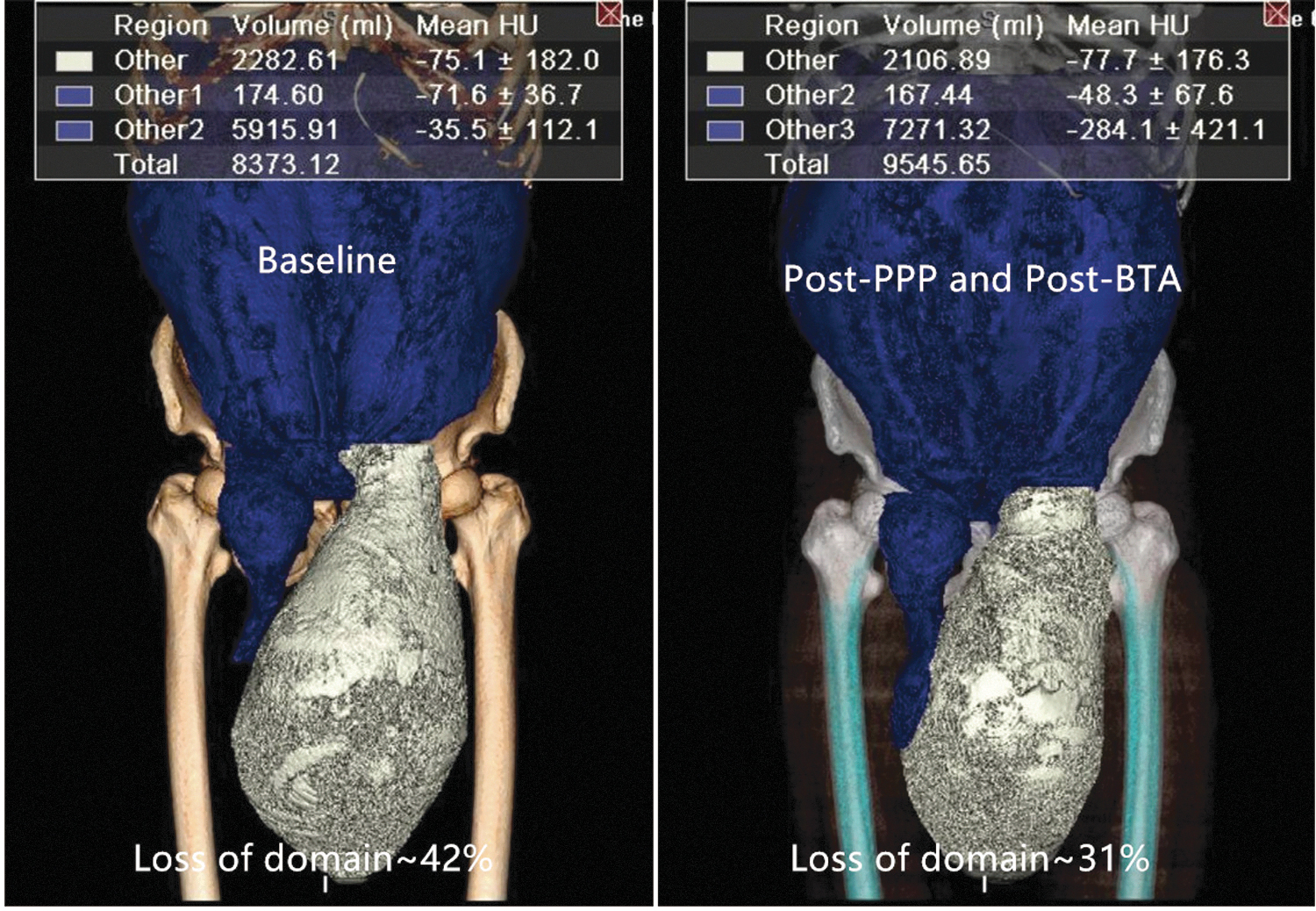
Abdominal volumes (volume of the abdominal cavity and volume of inguinal hernia) were calculated from a 64-slice multidetector CT using a specific software before and after the preoperative techniques. BTA, botulinum toxin A; CT, computed tomography; PPP, preoperative progressive pneumoperitoneum.
All patients underwent preanesthetic evaluation and pulmonary function tests. In the preoperative assessment, we emphasized on the importance of smoking abstinence and pulmonary function exercise.
For preoperative preparation of the patients, two consecutive techniques, namely intraperitoneal catheter placement and BTA injection administration, were used 2–3 weeks preoperatively and performed simultaneously under ultrasound guidance. Initially, the patient was administered the abdominal wall BTA (Botulinum Toxin Type for Injection; BOTOX®, Allergan, Ireland) injection as an inpatient procedure. All patients received a total dose of 100 units of BTA, which was diluted to 2 units/mL with 0.9% saline and divided into six equal amounts to obtain a volume of 8 mL in each aliquot. Using ultrasound guidance, we placed the patient in a lateral position and identified three sites on each side of the abdomen, that is, along the anterior axillary line equidistant between the costal margin at the level of the ninth rib and a point anterior to the anterior superior iliac spine, according to the positions identified by Smoot et al. 20 Then, 8 mL of the diluted BTA was injected at the three sites of the three lateral oblique muscles (transversus abdominis, internal oblique, and external oblique) at each of the six points (16 units/8 mL at each injection site), and the patient was returned to a supine position. Pneumoperitoneum was then introduced 2–3 weeks before elective hernia repair. Under ultrasound guidance, we established pneumoperitoneum by introducing a 14-Fr deep venous catheter into the peritoneal space at a location distant from the previous incisions. We initially insufflated 200 mL of air via a syringe and then performed X-ray with the patient in a standing position to check whether the PPP catheter was appropriately placed. Subsequently, 300–400 mL of air was introduced daily according to the patients' tolerance. Catheter placement and initial insufflation were performed as inpatient procedures, and patients were discharged on the following day. During the period of pneumoperitoneum introduction, patients wore an abdominal binder and were encouraged to improve their respiratory function and to walk for at least 2 hours a day. We tried our best to reduce the loss of domain ratio, so that the increase in abdominal volume was greater than that in the inguinal hernia volume before PPP. PPP administration was temporarily terminated when the following instances occurred: (1) intolerable subjective symptoms such as abdominal pain, abdominal distension, and shoulder pain; (2) dyspnea, hypoxemia, or CO2 retention; and (3) serious subcutaneous emphysema.
Elective surgical repair was performed using the transabdominal preperitoneal (TAPP) approach. 21 The patient was placed in a supine position, and an indwelling urinary catheter was routinely inserted after intubation. A 12 mm port was placed 1 cm below the umbilicus for inserting a 10 mm, 30° telescope. Two 5 mm working ports were inserted at a two-finger distance below the umbilicus in both lateral margins of the rectus abdominis under direct vision. After the hernial sac was completely reduced, the defect diameter was measured. The peritoneum was transected 2 cm from the upper margin of the defect and then dissociated from the medial Retzius' space and the lateral Bogros' space. The hernial sac was incised in a “T” shape, and the spermatic cord was then transversely severed and was fully separated up to 6 cm long. The defect of the inner ring was stitched continuously with barbed sutures (2–0) and was weaved into a network structure, avoiding excessive tension and injury to the inferior epigastric vessel. We then inserted a single central venous catheter through an abdominal puncture for drainage and placed the catheter tip in the lowest part of the scrotum through the inner ring. Finally, we introduced a mesh to complete the procedure without using fixation. We routinely used a macroporous polypropylene mesh (BARD® 3DMax™, 10.8 × 16 cm; Davol, Inc.).
In the immediate postoperative period, we routinely assessed the bladder pressure and elevated the scrotum. Patients were asked to locally apply mirabilite to the groin area for 48 hours. Intravenous antibiotics were continued postoperatively for 72 hours. The drainage was removed 48 hours later.
The difference in the length and peritoneal volumes of the lateral abdominal wall before and after the PPP and BTA procedure was analyzed using the SPSS version 24.0 software (IBM Corp., Armonk, NY); P < .05 indicates statistical significance.
Results
Eight male patients underwent our protocol using PPP and BTA injections. Their mean age was 65 (58–73) years, and the mean body mass index was 25.4 (21.6–29.3) kg/m2. Four patients had right-sided inguinal hernia, 2 had left-sided inguinoscrotal hernia, and 2 had bilateral inguinoscrotal hernia. The mean time since the occurrence of the inguinal hernia was 119 (72–180) months. The smallest defect size was 4 × 5 cm, whereas the largest size was 6 × 7 cm (Table 1).
Comparison of Peritoneal Volumes Before and After the Preoperative Techniques
Results for the first 8 patients undergoing preoperative PPP and BTA therapy.
BTA, botulinum toxin A; PPP, preoperative progressive pneumoperitoneum; VAC, volume of the abdominal cavity; VIH, volume of the inguinal hernia.
The mean duration of the preoperative techniques was 15.4 ± 1.6 (13–18) days, and the mean volume of insufflated air was 5625 ± 845 (4000–6800) mL. A comparison of the peritoneal volumes before and after the preoperative techniques is shown in Table 1. Before and after PPP, the VIH was 1894 ± 500 (1023–2459) mL and 2020 ± 482 (1191–2617) mL (P < .05), the VAC was 6720 ± 1281 (5054–8793) mL and 8864 ± 1473 (7052–11,250) (P < .01), and the VIH/VAC ratio (LODH ratio) was 28.1% ± 6.0% (20.2%–41.5%) and 22.8% ± 4.5% (15.6%–31.3%) (P < .01), respectively. The LODH ratio was significantly reduced by 5.3% on CT after the combination of PPP and BTA (Fig. 1). As expected, the mean length of lateral abdominal muscles significantly increased, and the mean thickness of lateral abdominal muscles decreased (Fig. 2). A statistically significant increase was found in the length of mean abdominal muscles from 16.8 ± 2.8 (14.2–21.5) cm/side before the combination approach to 20.1 ± 3.4 (16.3–25.5) cm/side after the combination approach (P < .01), indicating a gain in the mean transverse length of the lateral abdominal muscles of 3.3 (1.3–4.1) cm/side. In all cases, the thickness of lateral abdominal wall muscles decreased by a mean of 6.3 (0.4–13.5) mm. Intestinal segments at the level of the femur on CT before and after the preoperative techniques are shown in Figure 3.
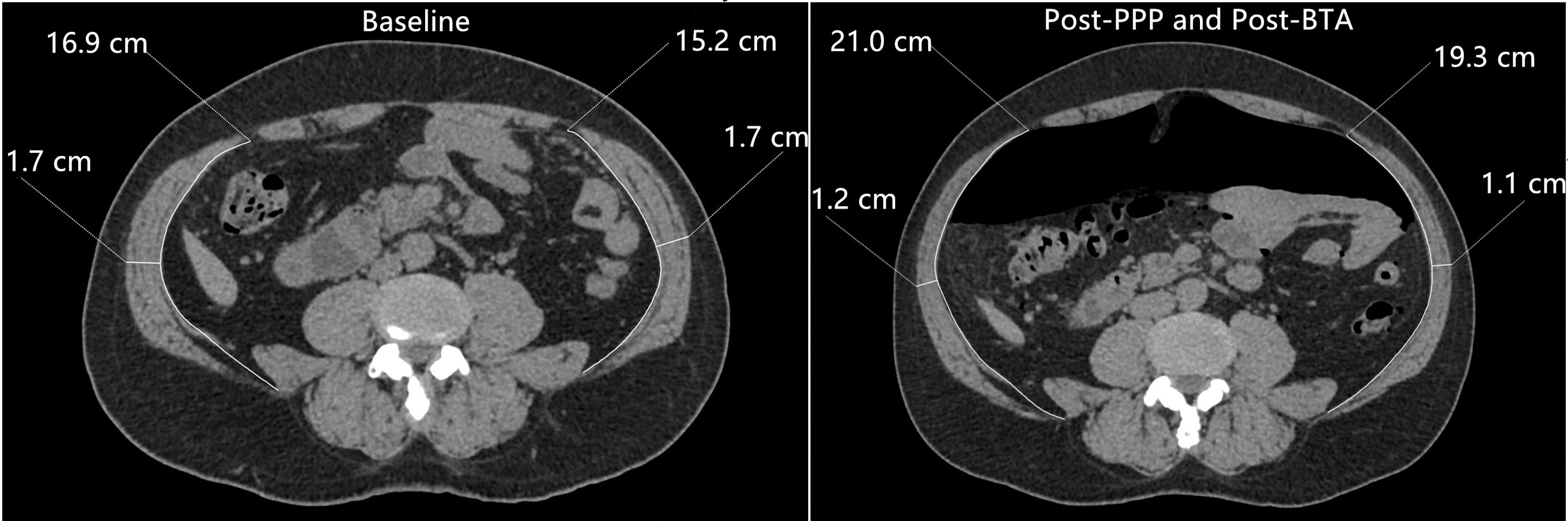
Comparison of preoperative axial CT images before and after the preoperative techniques; significant elongation and thinning of the lateral abdominal oblique muscles were observed (patient 2). BTA, botulinum toxin A; PPP, preoperative progressive pneumoperitoneum.

Intestinal segments at the femur level on CT before and after the preoperative techniques (patient 2). BTA, botulinum toxin A; PPP, preoperative progressive pneumoperitoneum.
Only 1 patient (12.5%) experienced PPP-related complications. This patient experienced shoulder pain, but required no intervention. No bowel perforations or instances of air embolism, peritonitis, or venous thrombosis occurred. Moreover, no complications occurred during BTA administration. All patients had a successful laparoscopic repair of their giant inguinal hernias (Fig. 4). The closure of the inner ring was feasible in all patients. The mean operation time was 93.1 ± 16.2 (70–120) minutes, and the mean duration of postoperative hospitalization was 7.6 ± 0.7 (7–9) days. Postoperatively, seroma developed in 2 patients but was resolved within 1 week after local application of mirabilite. No patient suffered from abdominal hypertension or required prolonged ventilatory support. To date, no hernia recurrences have been reported, and the mean follow-up was 15 (9–20) months.
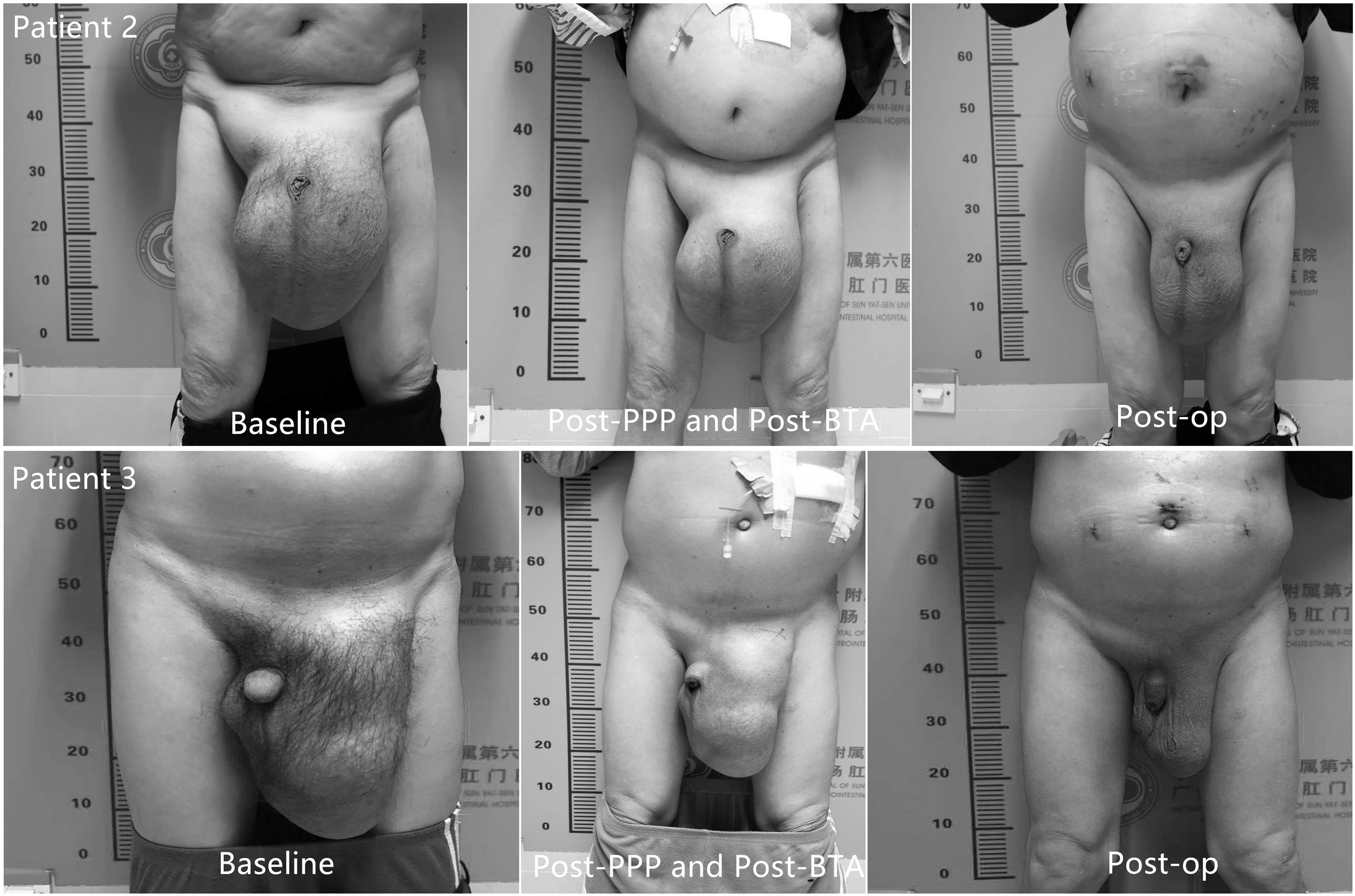
Comparison of before and after the preoperative techniques and day 7 postoperative coronal views with the patient in an active crunching maneuver (patients 2 and 3). BTA, botulinum toxin A; PPP, preoperative progressive pneumoperitoneum.
Discussion
Despite recent advances in surgical techniques and approaches, the repair of giant inguinoscrotal hernias is particularly challenging for surgeons. Considering that the herniated viscera progressively lose their “right of domain” in the peritoneal cavity, this type of hernia cannot be repaired with a simple technique of fascial closure. The forced reduction of the herniated viscera into an unprepared abdomen can increase the postoperative risk of elevated intra-abdominal pressure and its associated ventilatory complications because of an abrupt rise in abdominal pressure.5,6 Hence, adequate preoperative preparation of these patients is crucial.
For preventing life-threatening ACS after the repair of a large hernia, PPP has been suggested as a preparatory procedure.7,11 PPP increases VAC, results in a pneumatic lysis of intestinal adhesions, facilitates visceral reintroduction during surgery, and minimizes the involvement of respiratory function. 22 Hence, PPP is also recommended for the repair of giant inguinoscrotal hernias.17,23,24 Meanwhile, in 2009, Ibarra-Hurtado et al. 12 first reported the benefits of BTA injection in patients with abdominal wall hernias after an open abdomen management. Since then, the number of reports regarding BTA being used preoperatively to facilitate surgical reconstruction of abdominal wall hernia has been limited because of its effect on lengthening and relaxing the laterally retracted abdominal muscles and decreasing lateral traction.25–28 Furthermore, the advantages of preoperative BTA therapy in conjunction with PPP, which facilitates primary closure of large complex ventral hernia, have been described.14,15,29
The scrotum is not covered by muscles; most of the insufflated gas can spread into the hernial sac, leading to an insufficient increase in abdominal volume. 30 Hence, preoperative BTA injections were also administered as an adjunct procedure to PPP for expanding the abdominal space. In our series, the VIH increased by 126 mL after PPP (P < .05). The VAC increased by 2144 mL (P < .01) and was slightly greater than that in the inguinal hernia volume (1894 mL), and roughly equal to the mean volume (2020 cc) of the VIH after PPP. However, this degree of increase in abdominal volume basically ensures safety of the operation. Furthermore, only 1 patient had a specific complication that required intervention. During BTA administration, no complications occurred. Combined with PPP, this approach allowed us to obtain reduction in the LODH rate in all patients. Such reductions are important for reconstruction in patients with LODH. Other common methods to enlarge the abdominal space include component separation technique 31 and transversus abdominis muscle release. 32 However, these methods increase the rate of surgical wound morbidity, and recurrence rates remain high. Another approach is to reduce the contents of the abdominal cavity by resecting the bowel, omentum, ovary, or spleen.33,34 This approach, however, is associated with the risks of intraperitoneal infection, partial loss of physical function, and infection of the mesh grafts.
During open repair of giant inguinoscrotal hernias, a long surgical incision close to the scrotum skin is performed; thus, incisional infection or even mesh infection can most likely occur. To benefit from the advantages of minimally invasive surgery, researchers suggest a laparoscopic approach with TAPP repair. 35 In our study, all patients were treated by the TAPP approach. We found no significant increase in the operation time, postoperative hospital stay, chronic pain incidence, or recurrence compared with that with open repair. Endoscopic TAPP repair has its advantages. First, the hernial contents can be easily observed from the abdominal cavity, and the blood supply and adhesion of the hernia contents can be completely and comprehensively evaluated. Second, under the combined action of general anesthesia and pneumoperitoneum, the hernial contents can be easily returned to the abdominal cavity and the operation time can be reduced. Third, the mesh can completely cover the myopectineal orifice and reduce the chance of recurrence. Finally, TAPP repair can lessen incision and mesh infection incidences.
Piskin et al. 17 reported 2 patients with giant inguinal hernias who were prepared for hernia repair with PPP therapy. In the first patient, the volume of insufflated air for PPP was 7400 mL over 18 days. The intra-abdominal pressure increased over time, but the waist circumference at the umbilical level stayed at 11 cm at that time and on day 4. Thus, they insufflated their second patient with 3000 mL of gas for 4 days, and the expansion length of the waist circumference at the umbilical level was 11 cm on day 4. These 2 patients underwent successful hernia repair without recurrence, indicating that abdominal expansion correlated with the inflated volume and pressure during the first 4 days of PPP. More recently, a case report on the combination of PPP and preoperative BTA injection for repairing LODH in the inguinal area has been documented. 16 This patient received BTA injection in the abdominal wall. Four weeks after BTA administration, the hernia had shrunk markedly. Then, the surgeons continued with a PPP technique, insufflated 1 L of ambient air per day into the peritoneal cavity for 2 weeks, and performed the Lichtenstein technique. Two years after the surgery, this patient is doing well without hernia recurrence.
The giant inguinoscrotal hernia recurrence rate can be as high as 30%. 4 To prevent hernia recurrence, surgeons should ensure that the mesh covers the entire myopectineal orifice and at least 3 cm over the edge. In our study, the defect of the inner ring orifice was closed horizontally with a barbed suture to weave a loose “net,” providing support for the mesh and reducing hernia recurrence. However, the inner ring orifice should not be closed forcibly to prevent postoperative pain due to excessive tension. At the same time, a loose network structure is conducive for draining of the fluid in the scrotum. To reduce postoperative seroma incidence, surgeons incised the hernial sac in a “T” shape and then transversely severed. Savoie et al. 36 also concluded that leaving the distal hernial sac in the scrotum can limit the occurrence of complications in patients after repair of giant inguinoscrotal hernias. The patient should also elevate the scrotum and apply mirabilite to the groin area to reduce the formation of scrotal effusion.
The present study has some limitations. First, the sample size is relatively small (n = 8), although it is one of the longest series previously reported in the literature. Second, the mean follow-up duration is limited. Further inclusion of more patients in this study and long-term follow-up of these cases are required to more convincingly demonstrate the advantages of this method.
In conclusion, the combined use of PPP and preoperative BTA is a safe and easy method for preventing ACS after laparoscopic TAPP repair of giant inguinoscrotal hernias. In our limited experience, we observed that the combination approach induces an insignificant increase in VAC and in the length of lateral abdominal muscles before surgery, thereby eliminating the need for expanding the abdominal space with a surgical technique and allowing total reintegration of the bowel into the abdomen.
Footnotes
Acknowledgments
We thank all the participants included in this study. We acknowledge the kind assistance of Z.Z., MD, in designing the study and J.-B.X., MD, and N.M., MD, PhD, in editing the article. Furthermore, we acknowledge Prof. T.-C.Z. and Prof. S.C. for their critical reading of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was funded by the Science and Technology Planning Project of Guangdong Province (Grant No. 2017A020215036), the National Natural Science Foundation of China (Grant No. 81860433), and the Natural Science Youth Foundation of Jiangxi Province (Grant No. 20192BAB215036).