
Abstract
Purpose:
To improve the tumor localization during laparoscopic surgery, we describe an innovative technique involving superselective intra-arterial injection of blue dye in tumoral vessels to color the tumor before surgical enucleation.
Materials and Methods:
The dye injection was performed at the same time as superselective embolization, immediately before laparoscopic surgery in a hybrid operating room. We used this new treatment sequence on 50 consecutive patients.
Results:
The selective intra-arterial injection of an emulsion of blue dye and lipiodol was feasible in 46 (92%) cases and well tolerated, followed by superselective embolization of the tumor vessels with glue or coils. The tumor was easily localized during surgery due to the blue coloration. Tumor coloration was not associated with postoperative complication, especially allergic reaction or renal failure. Pathologic analysis of the tumor was not modified by the coloration and all tumors had negative surgical margins.
Conclusions:
The preoperative dye localization is a feasible, safe, and accurate procedure. This combined approach reduces the difficulty of surgery and increases patient safety.
Introduction
Renal cell carcinoma accounts for 2%–3% of cancer worldwide, with an annual increase of ∼2% in the last 2 decades. Based on European association guidelines, nephron sparing surgery (NSS) is recommended for treatment of localized renal cancers. 1 Minimally invasive approaches, such as laparoscopic or robot-assisted surgery, have gained importance recently. However, laparoscopic NSS presents a high risk of surgical complications due to its technical complexity. One of the main limitations of this technique is to localize the renal tumor inside the normal renal parenchyma. Indeed, sometimes the tumor is endophytic, and do not change the relief of the kidney. 2 Moreover, in 30%–40% of cases, the tumor is difficult to localize because of an important adherent perirenal fat (APF), also called “toxic fat.” A recent study suggests that the presence of APF increases operative time and perioperative morbidity, specifically the risk of bleeding and conversion to an open approach. 3 To avoid this problem, laparoscopic surgery needs tools to improve the localization of the tumor. Currently, the intraoperative techniques used to identify renal tumors, such as ultrasonography (US) or fluorescence imaging, have some limitations.
In this study, we describe and evaluate the feasibility of a new technique of renal tumor localization based on selective intra-arterial injection of blue dye during tumor embolization immediately before laparoscopic partial nephrectomy (LPN) in a hybrid operating room.
Materials and Methods
An Ethics Committee approved this prospective clinical study and 50 consecutive patients gave consent to be treated by LPN after selective arterial embolization for a localized T1 renal tumor in a university hospital between February 2016 and June 2017. The procedure was performed in a Discovery IGS 730 (GE Healthcare) operating room, under general anesthesia. A three-dimensional (3D) renal arteriography was performed to identify tumor vascularization. Superselective catheterization of subsegmental arteries feeding the tumor was achieved using a coaxial microcatheter (Progreat hydrophilic coated microcatheter 2,7F, Terumo Europe, Leuven, Belgium) (Figs. 1 and 2). For tumor coloring, we used an emulsion of a blue dye (Patent Blue V) with iodized oil (lipiodol; Guerbet, Paris, France). This emulsion was previously tested in vitro by a pharmacologist and characterized by physicochemical evaluations (average conductivity of 2.59 ± 0.10 mS/cm, globule size of 5 μm in optical microscopy). Blue dye emulsion was prepared at the time of use by the interventional radiologist: using a three-way tap, we performed a “water in oil” emulsion of these two products at a concentration of 2:3. Then, this emulsion was injected slowly into the tumoral arteries under fluoroscopic guidance to avoid reflux in healthy renal arteries. Then, a selective embolization of arteries feeding the tumor was carried out using fibered micro coils (VortX Boston Scientifics) or glue (N-butyl-2-cyanoacrylate Glubran 2, GEM Srl, Viareggio, Italy) diluted 1:5 with lipiodol. A final 3D arteriography was performed to control tumor devascularization and confirm parenchymal preservation (Fig. 3). Subsequently, patients were positioned in a lateral decubitus position to perform the laparoscopic NSS. The surgeon localized the tumor by visual tracking of the blue dye (Figs. 4 and 5).

Selective renal arteriography before embolization showing a hypervascularized tumor (arrow).

Superselective tumoral arteriography with microcatheter.

Selective renal arteriography after embolization showing a limited ischemic area (arrow) related to the superselective embolization.

Laparoscopic view: immediately approach to the tumor with blue dye localization after Gerota's fascia incision.
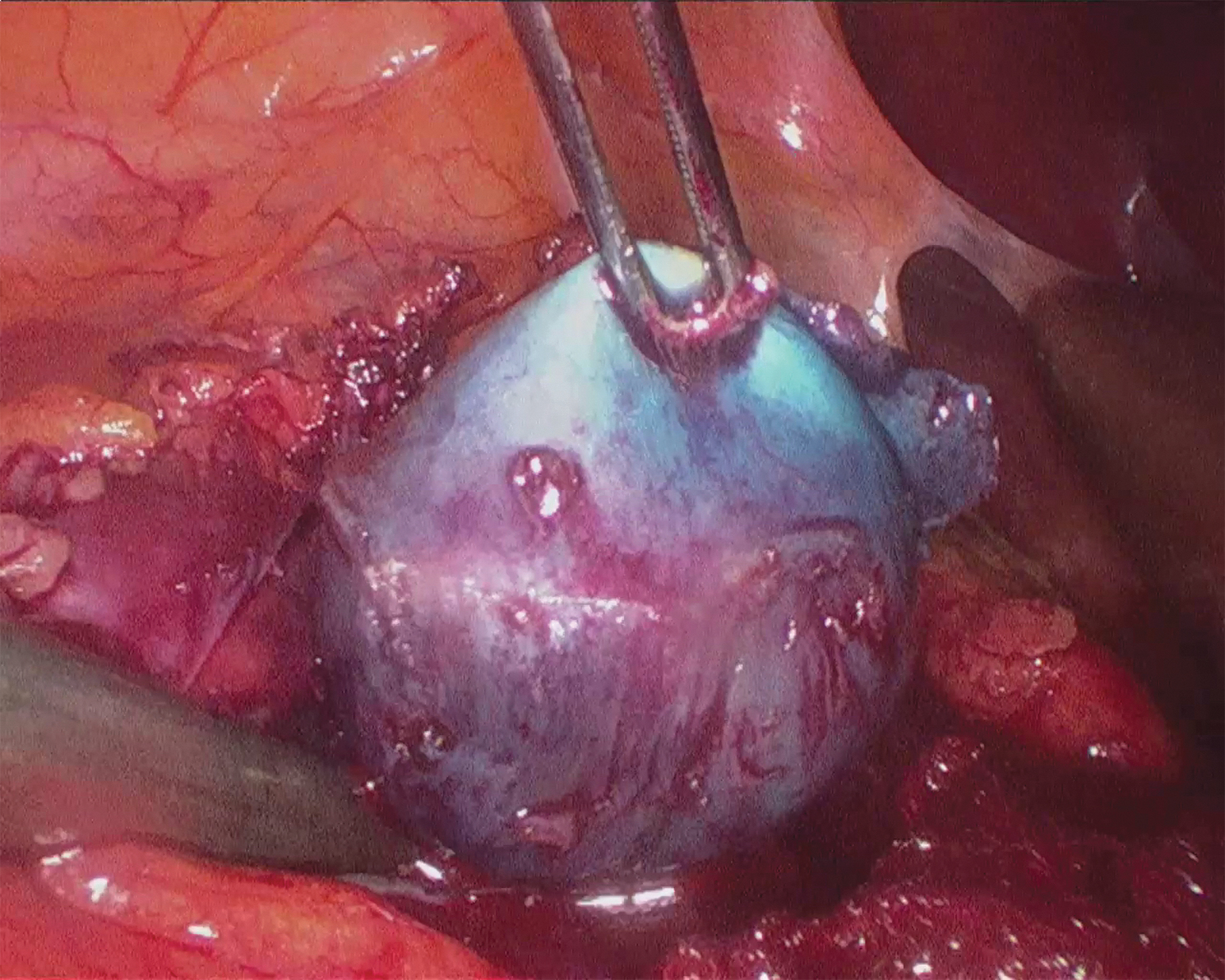
Enucleation of the colored tumor after blue dye localization without arterial bleeding and few venous bleeding.
Preprocedural clinical data were collected and anonymized via a National Renal Cancer Database (Uro-CCR). 4 They included: age, sex, body mass index (BMI), tumor size, results of a potential preoperative biopsy, renal function according to the modification of the diet in renal disease (MDRD) criteria, 5 and renal tumor complexity according to the R.E.N.A.L. score. 2 Presence of APF was visually determined by the surgeon during the laparoscopic procedure. Tumors were classified according to the TNM 2009 classification, 6 and histological subtypes were recorded according to the 2015 WHO classification of kidney tumors. 7 Fuhrman grade for clear cell renal cell carcinomas 8 and surgical margins were systematically analyzed. We evaluated perioperative data, postoperative complications, surgical margin status, and modifications of renal function immediately and at 1 month after surgery. Clavien-Dindo scale 9 was used during follow-up to record complications. Our primary endpoint was the tumor's blue color seen by the surgeon during laparoscopy. The secondary endpoint was the presence of postoperative complications related to dye injection. Statistical analysis was performed with SPSS 15.0 software. Preoperative, postoperative, and at follow-up MDRD glomerular filtration rate (GFR) rates were compared using a paired Student's t-test.
Results
Population
Subjects and tumors characteristics are reported in Table 1. They were 29 men and 21 women. The average age was 62.5 years (range, 33–84). The average BMI was 28.1 kg/m2 (range, 19.2–46.4). The average size of the tumors was 3.4 cm (range, 1.5–7.5) with a low R.E.N.A.L. complexity score for 23 (46%) patients, moderate complexity for 23 (46%) patients, and 4 (8%) high-complexity score. A partially (>50%) endophytic tumor was present in 20 (40%) patients, 7 (14%) patients had an entirely endophytic tumor, and 13 (26%) patients had APF.
Patients and Tumors Characteristics
Radiological procedure
Radiological and surgical data are reported in Table 2. The radiological operative time, including dye injection and embolization, was 43 minutes (range, 16–90). The injection of blue dye was feasible in 46 patients (92%). In four cases dye injection was not possible, because of insufficient tumoral arterial flow (hypovascularized tumor) and risk of dye reflux (n = 3) and because of an arterial spasm that did not allow dye injection (n = 1). Embolization of tumor vessels after injection of blue dye was successful in 100%, with glue (n = 46) and/or micro coils (n = 10). No postembolization complication and no allergic reaction occurred.
Radiological and Surgical Data
Surgical procedure
NSS was performed with average bleeding of 215.4 mL (range, 10–1300). One patient had a bulky posterior upper pole tumor (moderate R.E.N.A.L. complexity score of 8) difficult to access and presented a venous operative bleeding of 1300 mL. The average surgical procedure time was 85.4 minutes (range, 32–150).
Primary endpoint: tumor coloration
The tumor coloration was observed by the surgeon during the laparoscopy in 92% of patients (46/50 patients).
Secondary endpoint: postoperative complication
Nine complications were reported: five were of Clavien-Dindo grade I (isolated fever), four were of grade II (three sepsis treated by antibiotics and one transfusion). No allergic reaction occurred, and no complication was directly related to dye injection.
Postoperative data
Average hospital stays of 3.7 days (range, 2–8). No patient had postoperative renal failure. The mean estimated MDRD GFR preoperative was 87 mL/min (range, 31–121.3) and mean MDRD GFR at 1 month was 81.2 mL/min (range, 29–120), with a significant variation of 5.4% (P < .001).
Pathological results
The patent blue V dye did not interfere with pathologic diagnosis, which revealed benign tumor in 13 patients and malignant tumor in 37 patients. The pathological analysis confirmed negative surgical margins for all tumors.
Discussion
Performing a superselective arterial embolization before laparoscopic NSS presents the advantage of performing a zero ischemia partial nephrectomy without the clamping of the renal pedicle. 10 Surgery is facilitated by avoiding dissection of the renal pedicle and by a low bleeding. Furthermore, performing the renal embolization at the same time and in the same place as laparoscopic NSS reduces the occurrence of postembolization perilesional edema, which is described in cases of delayed surgery and which makes the surgical excision difficult. 11 Despite preoperative selective renal embolization, the surgeons still had difficulties to localize the tumor during the laparoscopic NSS, especially in case of endophytic tumor or perirenal adherent fat.
Several imaging techniques have been advocated for intraoperative identification of renal tumor. The most widely used technique is intraoperative US. 12 Advantages of US are its wide availability, low costs, and ease of use. However, US add time to the operative procedure13,14 and is not useful for a real-time guidance during resection, especially using a minimally invasive technique, since the probe interferes with the resection. Fluorescence imaging can be used for tumor localization and delineation in real-time imaging before and during resection. However, this requires, at additional cost, a special telescope and a camera to detect fluorescence. In addition, the kidney needs to have the perinephric fat removed to visualize the surface of the renal cortex and entirely endophytic tumors could not be detected with fluorescence imaging, due to overlying fluorescent normal parenchyma. Moreover, in cases of zero ischemia, the fluorescent dye passed through the renal parenchyma and did not assist in the excision of the suspicious renal mass.15–17
Dye localization of renal tumor in laparoscopic NSS is a new concept in the treatment of kidney cancer, which has never been described before. During superselective arterial embolization, a catheterization of subsegmental arteries feeding the tumor is realized. The situation of the microcatheter very close to the tumor allows for injecting a dye directly into the tumor, to obtain an important macroscopical coloration of the tumor, which improves the tumor localization by the surgeon.
Patent blue dye is an isomer of isosulfan blue and is widely used for sentinel lymphatic mapping in breast cancer surgery. 18 It is also used recently for localization of pulmonary nodules in thoracoscopic surgery. 19 The advantages of these methods include cost effectiveness and safety. Allergic reactions to patent blue are rare with a reported incidence of 0.9%. 18 Initially, we used pure patent blue for intra-arterial injection of tumor vessels during preoperative superselective renal embolization, but the dye rapidly diffused into the renal parenchyma. That is why we used an emulsion of patent blue and lipiodol. Lipiodol is an oily contrast medium which is widely used in embolization because of its properties of radio-opacity and tumor seeking. Lipiodol is used in renal tumor embolization, mixed with ethanol for percutaneous ablation, or with glue for tumor vessels embolization. 20 Recently, Hongo et al. describe preoperative lipiodol marking before computed tomography-guided cryoablation for renal tumors. 21 In our study, we used the property of the lipiodol to seek selectively the hypervascular tumor to facilitate fixation of the blue dye in the renal tumors and to limit its intraparenchymal diffusion.
In our study, the injection of the emulsion of blue dye and lipiodol was feasible in 92% and well tolerated in all cases, without specific complication, especially no allergic reaction. The tumors were correctly colored by the blue dye at the time of the laparoscopic NNS and quickly localized by the surgeon. Compared to the literature, laparoscopic surgery duration was reduced by the localization of the tumor with the blue dye, despite the fact that tumor was endophytic or despite the presence of APF. Indeed, average surgical procedure time was 85.4 minutes in our study, while it was 153 minutes in a large literature review on robot-assisted partial nephrectomy, 22 and 123 minutes in a study on LPN after superselective embolization without blue dye injection. 23 The average bleeding was also lower (215.4 mL) in our study compared to the literature (275 mL): this can be explained by the fact that the faster localization of the tumor with the blue dye limit the volume dissection of perirenal fat, in addition with the lower bleeding induced by tumor ischemia due to the embolization of tumor vessels. 22 From a functional point of view, our study showed a small decrease of MDRD GFR at 1 month (5.4%), which is comparable to those found in the literature: Khalifeh et al. 24 and Haber et al. 25 both reported a decrease in MDRD GFR of 7% and 9%, respectively.
Our study is limited by the low number of cases, its monocentric character, and the lack of a control group without blue dye coloration. However, since we began to use this new coloration method, the surgery is easier with a lower time to localize the tumor, and we do not have specific complication.
Blue dye localization is a new effective tool, feasible, safe, and accurate in superselective renal embolization before LPN. The use of this localization method enables surgeon to quickly perform the tumor excision, especially in case of endophytic tumors or perirenal adherent fat, with good surgical margins. Other studies with control group could be necessary to validate the usefulness of this new treatment option.
Footnotes
Acknowledgments
We thank all the patients and the team. The anesthesia team: Dr. A. Ter-Minassian, Dr. E. Rineau; the radiology team: D. Dabli, G. Brehier, D. Lefort, N. Leroy, C. Vrignaud; and the surgical team: P. Grison, T. Culty, P. Panayotopoulos, A. Thibaut.
Disclosure Statement
A.B. and P.B. are consultant for GE Healthcare. All other authors state that they have no conflicts of interest that are directly or indirectly related to the research.
Funding Information
No funding was received for this article.