
Abstract
Background:
The therapeutic value of bursectomy remains controversial for patients with gastric cancer. Therefore, the purpose of our study was to explore the safety and survival benefits of bursectomy.
Materials and Methods:
A total of 943 patients with gastric adenocarcinoma were included in our study, and all patients were operated on by high-quality gastrointestinal surgeons. The factors associated with overall survival (OS) were determined using the Kaplan–Meier method. In addition, patients in the bursectomy group and nonbursectomy group were matched with 1:1 propensity score matching for sex, age, tumor location, type of operation, tumor size, degree of differentiation, and pathological stage to reduce the possibility of choice bias.
Results:
Among the 943 eligible patients, 188 (19.9%) underwent bursectomy and 755 (80.1%) did not. In all patients, the number of retrieved lymph nodes (P = .0596), blood loss volume (P = .0896), operation time (P = .0747), number of postoperative complications (P = .626), and OS in the bursectomy group were similar to those in the nonbursectomy group. After a stratified analysis of TNM grade and T stage, it was found that bursectomy could lead to survival benefits for patients with stage T4 disease (P = .0398).
Conclusions:
Bursectomy does not increase the amount of blood loss, operation time, or incidence of postoperative complications. This procedure is an extended and safe surgical method for gastric adenocarcinoma. Bursectomy does not improve the survival of all patients, but for patients with stage T4 disease, bursectomy can provide survival benefits.
Introduction
Gastric cancer is one of the most common malignant tumors of the digestive system. In the United States, it is estimated that 27,510 new cases of gastric cancer occurred and 11,140 died in 2019. 1 China is a region with a high incidence of gastric cancer in the world, with morbidity and mortality accounting for 42.6% and 45.0%, respectively. 2
Treatment for gastric cancer includes surgery, chemotherapy (CT), radiation therapy, and other immunotherapies. Although gastric cancer has a high metastatic and recurrent rate, the survival rate after gastrectomy is less than 40%, and surgical resection is still considered the best treatment.3,4
The peritoneal metastasis is one of the important ways of recurrence. 5 Bursectomy was a procedure containing the removal of the anterior membrane of the transverse mesocolon and the peritoneal capsule of the pancreas after total omentectomy. 6 Bursectomy was recommended by the Japanese Gastric Cancer Association (JGCA) 7 for patients with prophylactic or therapeutic peritonectomy over the lesser sac during radical gastrectomy, especially for patients with serosa-involved gastric adenocarcinomas. 8 With adding this kind of omentectomy to D2 gastrectomy, the potential of microscopic tumor deposition in the lesser sac and diseases of the pancreatic head is eliminated. In addition, bursectomy also offers a completely high-risk lymph node resection. 9
However, some surgeons still doubted of its oncologic value. A study conducted in Japan showed that the 5-year overall survival (OS) rate of the bursectomy group was 76.9%, while that of the nonbursectomy group was 72.9%. There was no significant difference in the OS rate between the two groups (hazard ratio, 1.05, 95% confidence interval: 0.81–1.37, P = .65). 10 Terashima et al. also pointed that the 3-year OS was similar between the bursectomy group and nonbursectomy group (86.0% versus 83.3%). 11
The purpose of our study was to explore the safety and clinical benefits of bursectomy based on patients who underwent radical resection of gastric cancer in our hospital.
Materials and Methods
Patients
We retrospectively analyzed patients who underwent gastric cancer resection in the Department of General Surgery, First Affiliated Hospital of Anhui Medical University from January 1, 2012 to December 31, 2013. According to the pathological examination results, all patients were diagnosed with gastric cancer. The clinical diagnosis staging of patients with tumors was determined according to the 2002 American Joint Committee on Cancer/International Cancer Control Tumor, Lymph Node and Metastasis (TNM) staging system. This study was reviewed and approved by the Ethics Committee of Anhui Medical University.
Inclusion criteria for our study were as follows: (1) pathology confirmed as adenocarcinoma of the stomach; (2) no radiotherapy or CT before the operation; and (3) subsequent CT based on the 7th NCCN guideline, unless the physical conditions refused to intolerant.
The exclusion criteria were as follows: (1) preoperative neoadjuvant radiotherapy and CT; (2) multiple primary tumors; and (3) only gastrointestinal bypass surgery.
According to the above criteria, 943 patients were included in our study. The most common methods of follow-up were routine outpatient visits and supplemented by email and telephone interviews. OS was recorded as the time from the date of surgery to death or the last follow-up. The end point of this study was follow-up until December 31, 2018 or death.
Surgery
The surgeries were all performed by a high qualification gastrointestinal surgeon in our institution (the annual average gastric cancer cases were over 200). All surgical methods were traditional laparotomy. Total bursectomy refers to the complete resection of the anterior and posterior walls of the less omental together with the gastric and peripheral adipose lymphoid tissues, in which the complete resection of the anterior transverse mesocolon and pancreatic capsule is the most important part.
Statistical analysis
Data in our study were all collected and analyzed by SPSS 24.0 (SPSS, Inc., Chicago, IL) and R software. Continuous data were presented as mean ± standard deviation. The classification data were expressed as the frequency (or percentage). Orderly classification variables of the two groups were analyzed with Mann–Whitney U test. Disorderly variables of the two groups were analyzed by Wilcoxon signed rank test. Differences in survival curves between the bursectomy group and nonbursectomy group were computed using a log-rank test. A P value less than .05 is considered statistically significant. In addition, patients in bursectomy group and nonbursectomy were matched with 1:1 propensity score matching (PSM) for sex, age, tumor location, type of operation, tumor size, degree of differentiation, and pathological stage to reduce the possibility of choice bias. The matching precision is set to 0.01.
Result
Patient characteristics
Of the 943 patients in the study, 552 males and 391 females were comprised with a median age of 64.3 years. Seven hundred fifty-five patients received purely omentectomy, while 188 patients received bursectomy added in omentectomy. The clinical characteristics of patients in different groups are shown in Table 1. In the analysis, gender, age, tumor location, type of surgery, tumor size, grade of differentiation, and pathological stages were included as covariates. By PSM, 180 cases were selected from each group (Table 1). After matching, the clinic pathological characteristics of the two groups showed no significant significance (P > .05), which was comparable.
Comparison of Characteristics Before and After Propensity Score Matching
p < 0.05.
Postoperative complications and mortality
Patients who underwent bursectomy did not have a higher incidence of postoperative complication than the nonbursectomy group (P > .05): 23 patients in the bursectomy group versus 20 in the nonbursectomy group. Four patients of the study group suffered from anastomotic leakage, while 3 patients in the control group. In terms of pancreatic fistula, the two groups also showed no significant difference (P > .05). Postoperative abdominal abscess rate was 1.1% versus 0.5%. The same number of cases got bowel obstruction after surgery, as well as pneumonia and incision infection.
There were just 3 patients in the bursectomy group and 2 patients in the nonbursectomy group died during 1 month among total bursectomy. In terms of incision hemorrhage and abdominal hemorrhage, the incidence of both showed no statistical difference (P > .05).
The postoperative mortality of patients with bursectomy was on the brink of those without bursectomy (1.7% versus 1.1%) (Table 2).
Comparison of Postoperative Complications
Fisher's* means statistical method using Fisher's exact probability method.
Short-term efficacy
The performance of bursectomy was not associated with longer operative time (P > .05). With regard to the blood loss, there was no significant difference (P > .05). The number of lymph node dissections in the two groups was similar (19 ± 5.23 versus 18 ± 4.24), which indicated that bursectomy involved group could not provide more lymph node dissections (Table 3).
Results of Short-Term Efficacy
The values are in mean ± standard deviation.
Long-term outcomes
After the 5-year follow-up, we found that the bursectomy did not affect patients' survival, whose rate was 71.3% versus 69.1% (bursectomy versus nonbursectomy) without statistical difference (P = .8948) (Fig. 1). Kaplan–Meier analysis and the log-rank test demonstrated that bursectomy cannot provide a survival benefit for patients in all clinical stages (P > .05) (Fig. 2A–H).
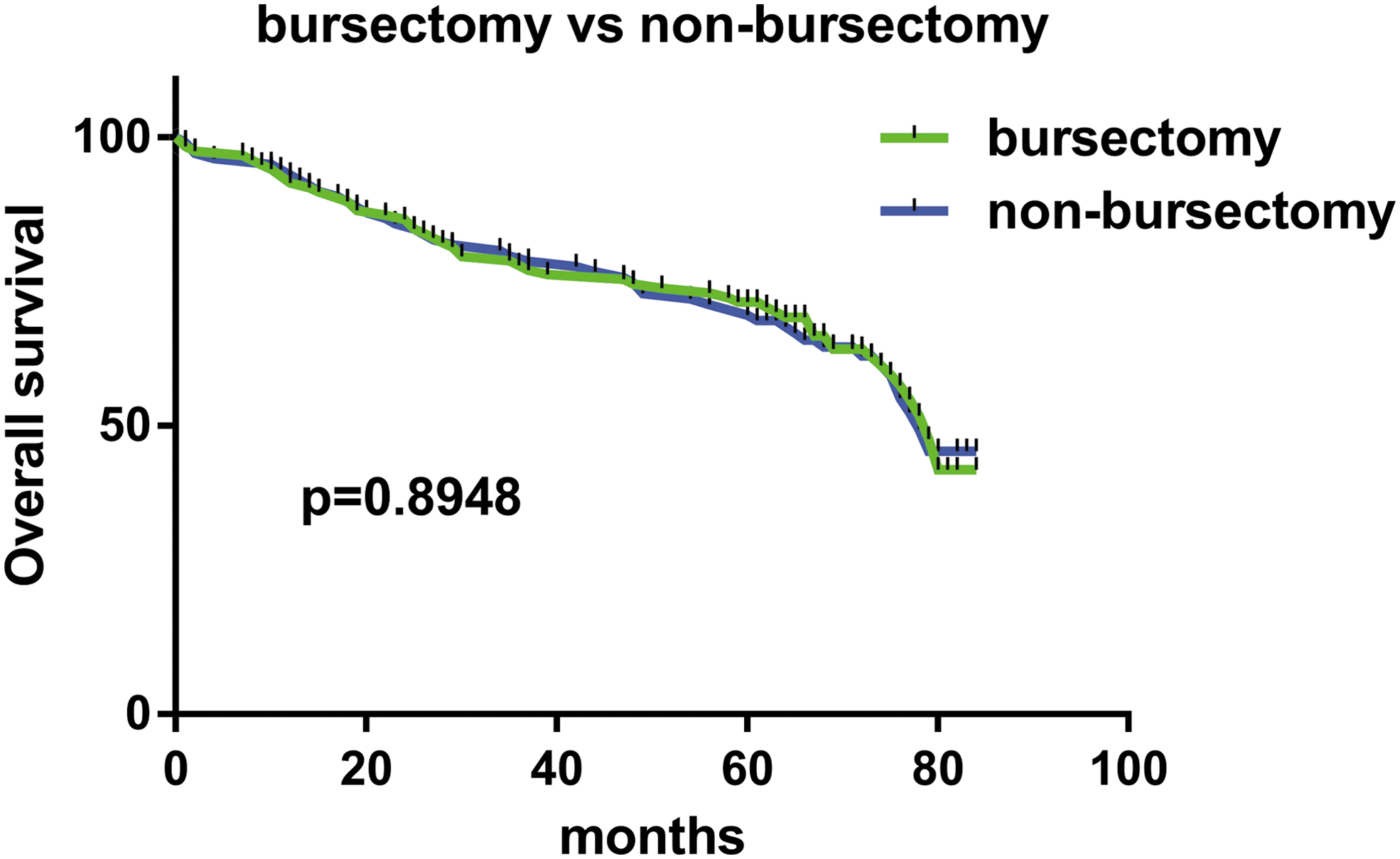
Five-year OS of patients in patients in the bursectomy and the nonbursectomy group. OS, overall survival.
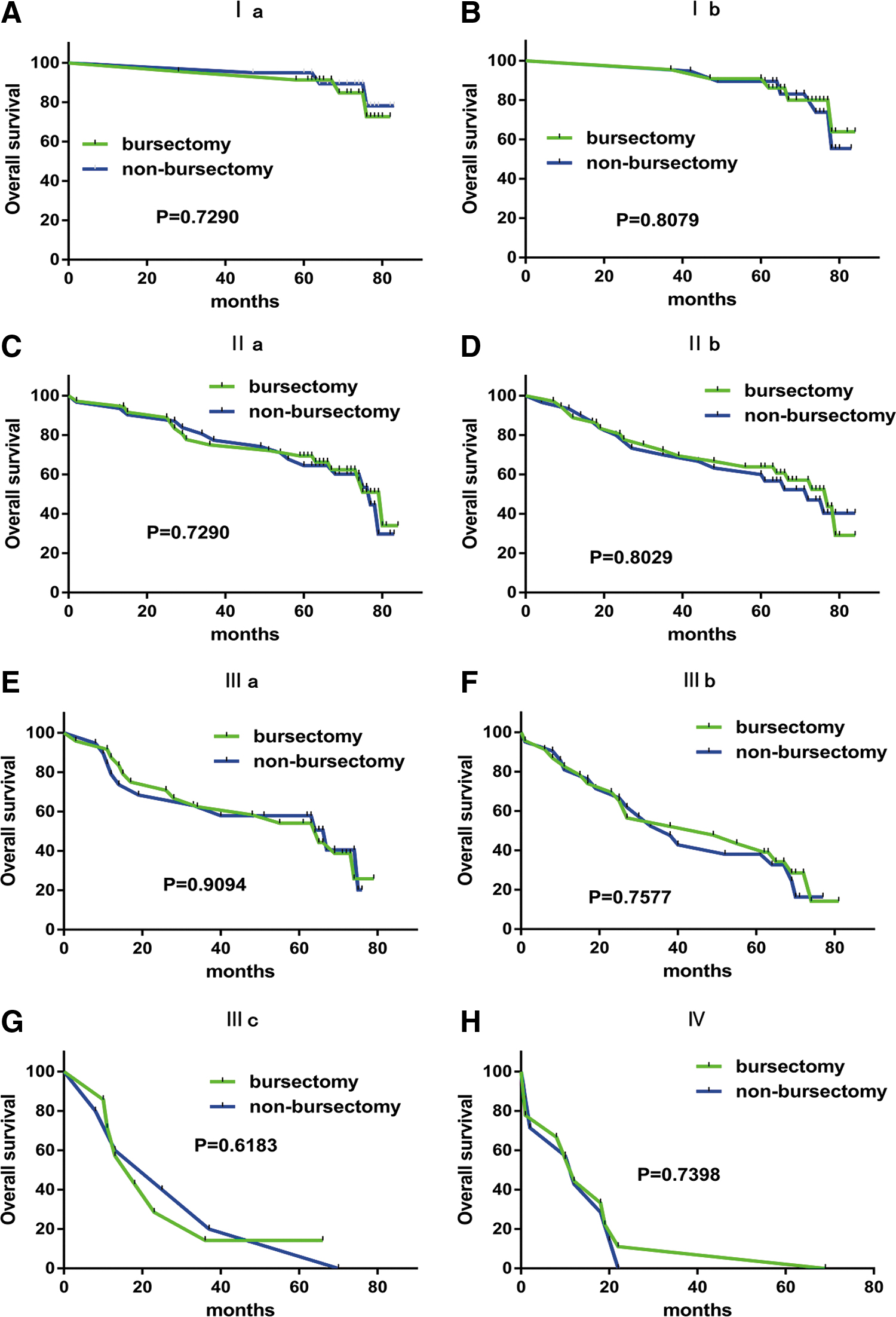
OS in patients with bursectomy and nonbursectomy groups in different stages.
Subgroup analyses were conducted in the pT stages. In the secondary analysis, we found that bursectomy provided survival benefit for patients with stage T4 (P = .037) (Fig. 3B). There were macroscopic survival differences in patients with stage T3, lacking of statistical evidence (Fig. 3A).
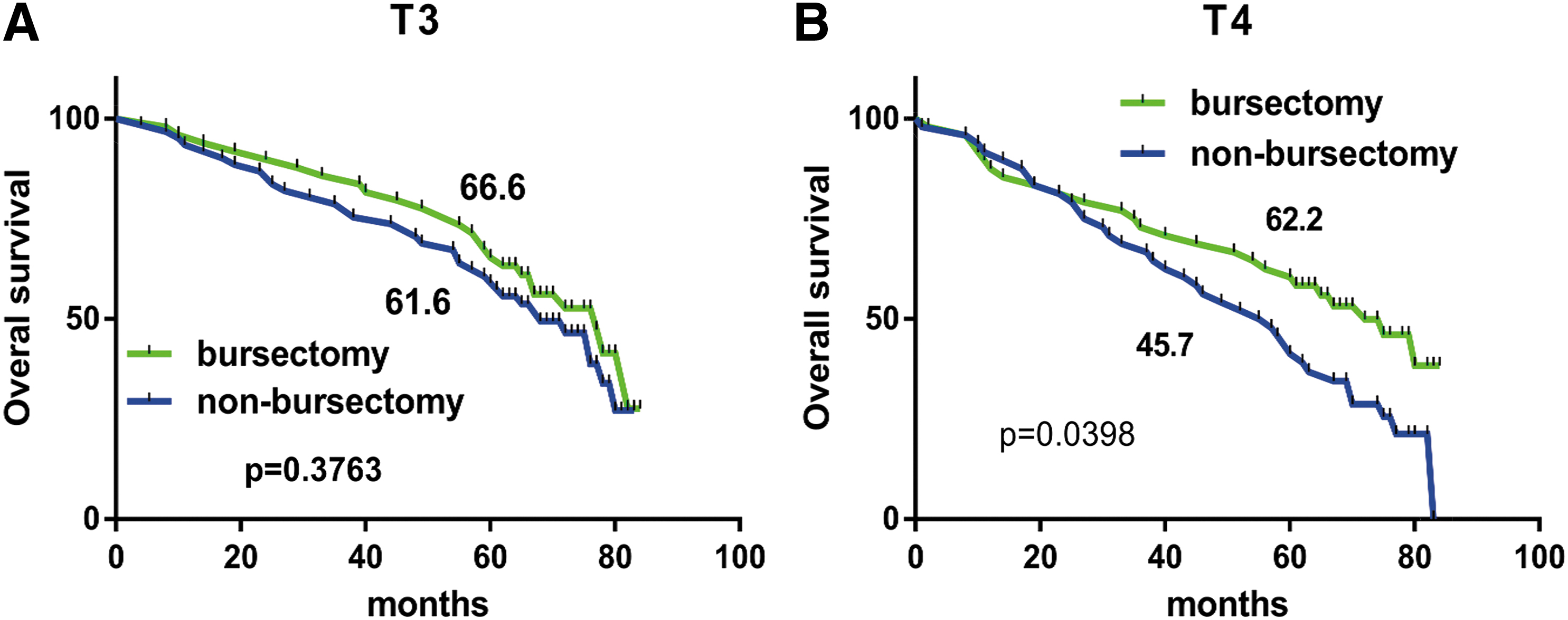
OS in patients with pT3 tumors
Discussion
Of the 360 eligible patients after the PSM analysis, 180 underwent bursectomy and 180 had no bursectomy. In those patients, the amount of bleeding, operative time, postoperative complications, and OS in the bursectomy group was similar to those in the nonbursectomy group. A stratified analysis of TNM and T-levels revealed that bursectomy can provide a survival benefit in patients with stage T4.
Bursectomy is a highly technical procedure that should be performed by experienced surgeons and postoperative managers. Although bursectomy is an extended radical gastrectomy, there is no evidence that additional surgery may increase the risk of postoperative complications. In our study, we found similar blood loss (120 ± 22.3 mL and 100 ± 19.7 mL, P > .05) and operation time (2.45 ± 0.39 hours and 2.32 ± 0.25 hours, P > .05) in the bursectomy group and the nonbursectomy group, which was similar to the reported median blood loss by Blouhos et al. 12
After providing a specialized mesocolon and pancreas, capsulotomy could aggravate abdominal organ adhesion and cause intestinal obstruction when the visceral adhesion is severe. In addition, we performed postoperative follow-up of all patients (Table 2). We found that 23 patients and 20 patients had postoperative complications in the bursectomy group and the nonbursectomy group. There was no significant difference in postoperative complications between the two groups (P > .05). The number of cases of anastomotic leakage, pancreatic fistula, abdominal abscess, incision hemorrhage, abdominal hemorrhage, bowel obstruction, pneumonia, and incision infection were 4, 2, 2, 3, 2, 3, 4, and 3 in the bursectomy group, while 3, 1, 1, 2, 3, 3, 4, and 3 in the nonbursectomy group. It is reported that about 10% of patients may develop pancreatic fistula by removing the pancreatic capsule.13,14 Recently, a meta-analysis showed that the incidence of pancreatic fistula was comparable whether synovectomy was performed or not. 15 In our study, the incidence of bursectomy was 0.01, which was almost the same as that of the nonbursectomy group (P > .05). In terms of safety, our study involved anastomotic leakage, abdominal abscess, bleeding, pneumonia, and wound infection, so there was no difference in synovectomy during surgery. In this study, the incidence of postoperative complications was 12.8% in the synovectomy group and 11.1% in the nonbursectomy group. We can speculate that the safety of bursectomy can be guaranteed with the support of skilled surgeons.
Dose bursectomy means a significant improvement in patients' survival outcomes? Yoshikawa et al. counted the T3–T4 patients who underwent radical bursectomy and radical D2 total gastrectomy and found that there was no significant difference in survival benefit between the two groups. 16 Kochi analyzed the effects of the two surgical methods on the survival of T2 patients and found that there was no significant difference between the two groups. 14 In contrast, one study in Osaka doubted about the conclusion. 17 Our study rematches patients by PSM analysis and involved patients from different clinical stages (from I to IV), which found no survival benefit. From further analysis performed, we found that bursectomy can not improve survival outcomes of patients from stage I to IV without exception. But when the tumor invasion depth was thought only, we found the statistically significant prognostic difference for patients with stage T4 between the bursectomy group and nonbursectomy group. Another finding was that patients with stage T3 which underwent the bursectomy group had a better survival outcome than the nonbursectomy group, regardless of the fact that these differences were not statistically significant. Depending on our study, patients under penetration of the serosa could receive a survival enhancement through bursectomy.
Theoretically, bursectomy provides a more efficient dissection of subpyloric lymph nodes (LNs) theoretically: the subpyloric and peripancreatic lymph nodes (the No. 6 lymph nodes along the right gastroepiploic vein down to the gastrocolic trunk); the capsule covering the pancreatic head (the peritoneal lining of the pancreas and the No. 17 lymph nodes) and the superior mesenteric vein lymph node (the No. 14v lymph nodes) got a complete resection. 9 A retrospective study of a single Chinese institution found a higher number of LNs examined in the bursectomy group. 18 Nevertheless, through analyzing the pathological data of 360 patients, our study found no statistical difference between bursectomy group and nonbursectomy group, the same as the result of Imamura et al. 19 Eom et al. also reached the same conclusion. We concluded that there was no significant difference between the two groups in terms of the LN resection by comparing. According to our study, it could be postulated that bursectomy provides oncologic benefits not from more accurate lymphadenectomy, but from the en bloc removal of free cancer cells or micrometastases contained in the bursa omentalis. 6
There are several limitations in this study. First, it was a retrospective study, thus having clear inherent limitations. Moreover, all patients need to be followed up prospectively, and the sample numbers need to further expand.
Conclusion
In conclusion, bursectomy group has a similar number of retrieved lymph nodes as nonbursectomy group. But it is an extended and safe surgical procedure for gastric adenocarcinoma that does not increase the amount of blood loss, operation time, or incidence of postoperative complications. Although bursectomy does not improve the survival of all patients, bursectomy can result in survival benefits for patients in stage T4.
Ethics approval and consent to participate
This study has been performed by the Declaration of Helsinki. The First Affiliated Hospital approved the research protocol of Anhui Medical University Ethics committee.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Footnotes
Acknowledgments
Y.L. and Z.H. contributed equally to this study. The authors are thankful for the guidance and support from X.M. and B.C.
Authors' Contributions
X.M. conceived and designed the experiments. X.M. and Z.H. collected and analyzed the data. Y.L. and Z.H. wrote the article. B.C. helped to identify the results of the statistical analysis. All authors read and approved the final article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Science Foundation of China (No. 81602425 to B.C.).