
Abstract
Background:
The linear geometry of the meshes undergoes significant changes after the transabdominal preperitoneal (TAPP) inguinal hernia repair, caused not only by the presence or absence of mesh fixation but also by reparative processes occurring in the area of surgical intervention.
Objective:
To assess the position of mesh in the preperitoneal space after the TAPP inguinal hernia repair using ultrasonography in the immediate and late postoperative periods.
Materials and Methods:
A total of 65 patients who underwent inguinal hernia repair with TAPP were examined. In all cases, a lightweight large-pore monofilament polypropylene mesh (size 10 × 15 cm) was used as a prosthesis. Follow-up examinations and ultrasonography of the mesh were carried out on the first postoperative day and at 1, 3, 6, and 12 months of the follow-up period.
Results:
Ultrasonography demonstrated mesh in two distinctly different appearances. Although it was seen as an echogenic structure with mild acoustic shadowing, the shape was either wavy or straight linear depending on the method and time elapsed from surgery. Thus, in patients without mesh fixation, it has a wavy appearance on the first day and at 1 month after TAPP, whereas at 3 months it took the appearance of a straight line, and at 12 months the implant has retained the shape of a straight line. Among patients who underwent mesh fixation in the immediate postoperative period, implant appeared as a straight line, and starting from the third month it began to acquire a wavy outline.
Conclusion:
Geometry of mesh used for TAPP inguinal hernia repair undergoes significantly different changes depending on the method of mesh fixation and time of postoperative period.
Introduction
Transabdominal Preperitoneal (TAPP) repair is one of the most commonly used techniques for surgical treatment of inguinal hernia, which has a proven safety and efficiency data by numerous studies.1–3 Minimal injury, low postoperative pain, and rare recurrences facilitated the widespread use of TAPP in clinical practice. Currently, almost a quarter of patients with inguinal hernias are treated using the TAPP approach. 4 At the same time, despite the success in laparoscopic technologies, the issue of treating inguinal hernias is far from being resolved. In particular, the phenomenon of chronic pain and foreign body sensation, “stiff-man” syndrome, testicular atrophy, and impaired ejaculation due to the implantation of a mesh prosthesis were described.5–9 . The changes in the size of the implant, the so-called “shrinkage” effect, have been shown to develop with time. According to different authors, the mesh size is reduced by 2.5%–48.0% during the first year, and this is one of the reasons for the recurrence of inguinal hernia.10,11 Langer et al. used specially prepared radiopaque heavy or light mesh in 50 patients with various abdominal hernias, who underwent open sublay repair. 11 During 2-year follow-up period, 92% of the patients with a light mesh did not show any changes in the size of the implants, whereas in the group of patients with heavy mesh its dimensions were reduced in 1 patient by 22.2%, in 2 patients by 8%, and in 1 patient by 3%. There were no cases of hernia recurrence. According to Lowham et al., the causes of hernia recurrence after implantation of mesh include, along with insufficient experience of the surgeon and the improper selection of the mesh and its positioning in relation to the hernia orifice, the bending and twisting of the mesh in the postoperative period. 12
The role of mesh material and method of its fixation (or absence of fixation) in the occurrence of chronic pain, contraction, and migration of the mesh is not fully understood. The study of Smith et al. in patients with inguinal hernias who underwent TAPP has demonstrated identical outcomes in groups of patients with or without mesh fixation. 13 The review by Macintyre indicates that there is no evidence of the need for stapling when performing TAPP, and the use of a mesh with dimensions of 10 × 15 cm or more allows to avoid the recurrence of the disease reliably. 14 At the same time, the author does not support an extensive dissection of the parietal peritoneum in TAPP, which contributes to an increase in the rate of retroperitoneal seromas, hematomas, and hernia recurrences. Similar results were presented in the works of Kapiris et al. (2009) 15 and Li et al. 16 According to the guidelines for the treatment of groin hernias by the HerniaSurge Group, the mesh fixation in the TAPP technique should be performed only in case of large direct hernias (M3 by European Hernia Society [EHS] classification, 2014), that is, when hernia neck is >3 cm. 3 It is also preferable to use a less invasive approach, such as fibrin or cyanoacrylate glue, where fixation is required.
This study aimed to assess the position of mesh in the preperitoneal space after TAPP inguinal hernia repair using ultrasonography in the immediate and late postoperative periods.
Materials and Methods
This prospective cohort study enrolled 65 patients with inguinal hernias (57 men and 8 women, aged 34–70 years, mean age 48.7 ± 5.8). The study was approved by the institution's Human Research Ethics Committee (protocol no. 143.17). All patients underwent treatment at the University Surgical Clinic in 2017. Of them, 37 patients had LI, 8 had LII, 6 had LIII, 6 had MII, and 8 had MIII inguinal hernia according to the 2014 EHS classification. Fifty-one patients presented with indirect hernias, type II; 14 patients had direct hernia type IIIa (L.M. Nyhus, 1993 classification). The size of the indirect inguinal hernia neck was in the range from 1 to 4 cm (mean 2.2 ± 0.7 cm), whereas the direct hernia necks were in the range from 1.5 to 4 cm (mean 2.6 ± 0.8 cm).
Inclusion criteria were the presence of an uncomplicated primary inguinal hernia, the age group from 18 to 80 years, and willingness to participate in the study. Exclusion criteria were the diagnosis of complicated inguinal hernia (irreducibility, incarceration, and phlegmon of hernia sac), disease recurrence, the presence of unavoidable predisposing, and triggering factors for hernia development. Clinical presentations of included patients are displayed in Table 1.
Clinical Characteristics of the Patients (n = 65)
BMI, body mass index; EHS, European Hernia Society; SD, standard deviation.
The standard TAPP technique was employed for treating the patients with the lightweight large pore monofilament polypropylene mesh “Bard® Soft Mesh” (USA) 10 × 15 cm. No slit was cut into the mesh for the spermatic cord exit at the deep inguinal ring. In 14 patients, with L3 and M3 hernias (type II and IIIa hernias, L.M. Nyhus, 1993; inguinal hernia neck—3.5 ± 0.4 cm), mesh implants were fixed with Protack™ Fixation Device (Covidien Surgical, Mansfield, MA). The mesh was not fixed in the rest of the patients. Left-sided TAPP was performed in 39, right-sided in 16, and bilateral in 10 patients accordingly.
Follow-up clinical assessment and ultrasonography of the mesh implant were performed on the next day and at 1, 3, 6, and 12 months after the procedure. The assessment included recording of patients' complaints, visual observation of the site of intervention, and digital examination of the inguinal canal. The study design is outlined in Figure 1.
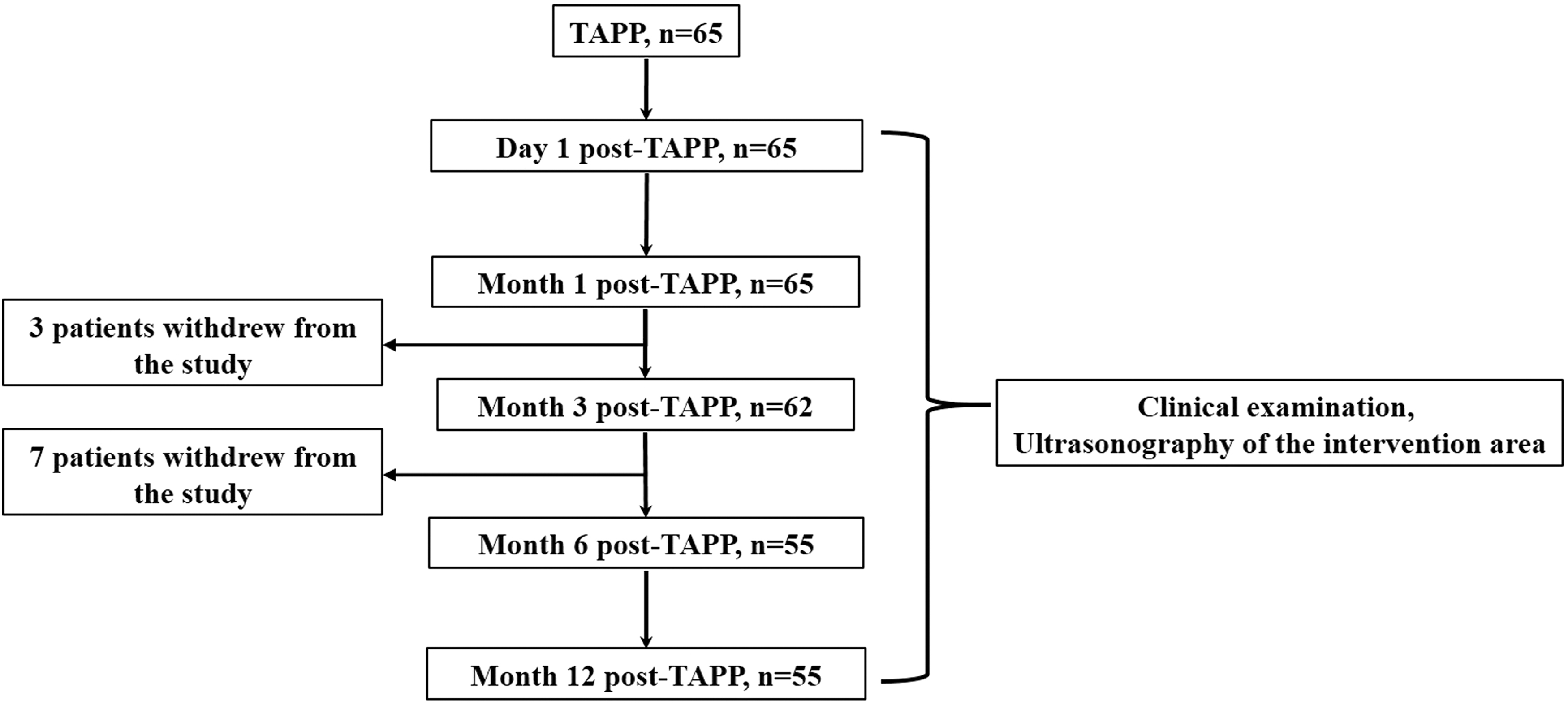
Flowchart of the study design.
Ultrasonography of the mesh implant
It was performed in the supine position using the Voluson E8 ultrasound system (GE, USA) equipped with the 3.5–5 MHz linear transducer.
“Bard Soft Mesh” cannot be visualized with X-ray or computed tomography due to its nonradiopaque material. Therefore, the ultrasonography was the only noninvasive test allowing assessment of the status of the mesh after the TAPP.
The full length of the implant was examined with ultrasound in the longitudinal and transverse projections. A sonologist visualized the mesh implant, its position relative to the muscles of the anterior abdominal wall, pubic bone, and the internal (deep) ring of the inguinal canal. During the ultrasound study, the mesh was identified as a hyperechoic linear structure of various thicknesses with mild acoustic shadowing. It was located in the projection of the inguinal gap between the muscles of the anterior abdominal wall and abdominal organs throughout the full length of the inguinal gap, overlapping the internal ring of the inguinal canal (Fig. 2).
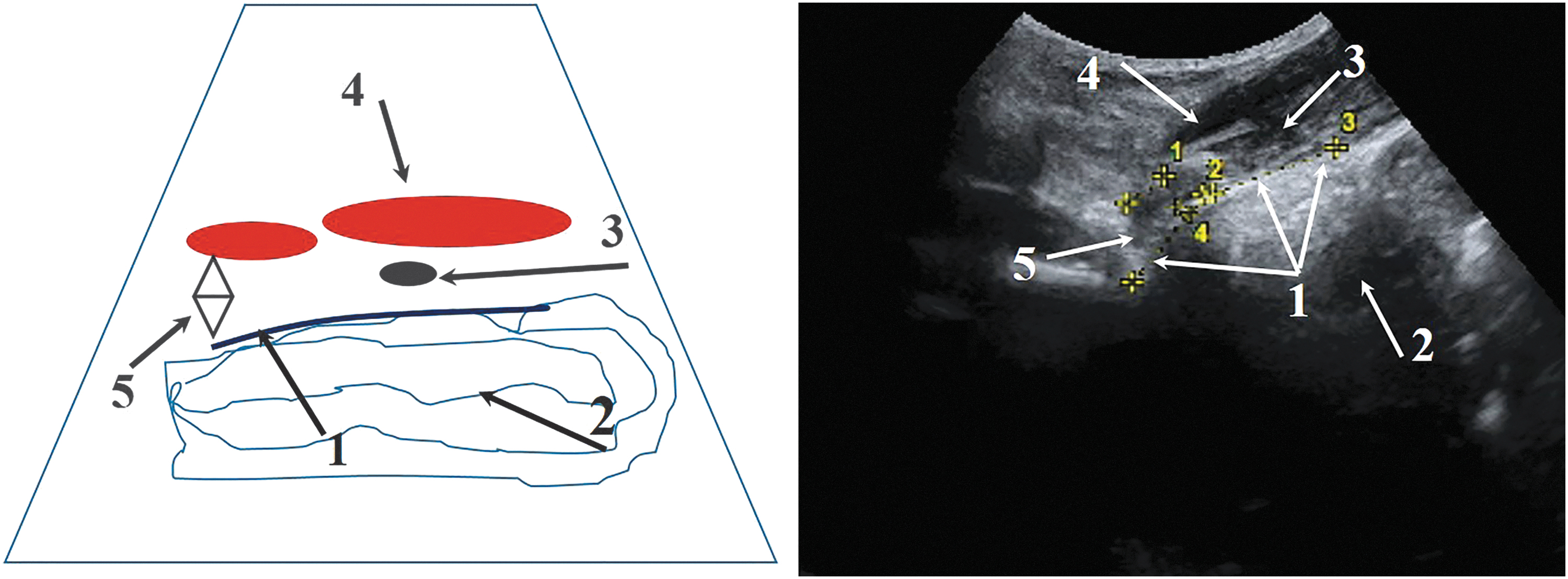
Diagram and ultrasound image of prosthesis position and elements of the abdominal wall after right-sided TAPP. 1: mesh; 2: intestinal loops; 3: internal (deep) ring of the inguinal canal; 4: muscles of the anterior abdominal wall; 5: pubic bone. TAPP, transabdominal preperitoneal.
Criteria for the correct position of the implant were its visualization at the level of the pubic bone and the complete overlap of the posterior wall of the inguinal canal, including its internal (deep) ring. Criteria for mesh displacement were the absence of the implant on ultrasound at the level of the pubic bone and the internal (deep) ring of the inguinal canal, the partial overlap of the latter by the mesh, or its displacement into the inguinal canal.
Also, the thickness and length of the mesh were measured by ultrasonography. During the examination, patients were asked to perform the Valsalva maneuver to evaluate changes in the appearance of the implant and to identify its potential displacement relative to the reference points during a short-term increase in the intra-abdominal pressure.
Statistical analysis
Statistical analysis was carried out using the Microsoft Excel and Statistica 6.0 software, as well as the statistical online calculator medstatistic.ru. The arithmetic means (M) with standard deviations (σ) was calculated, and the data were presented as absolute and relative values. A nonparametric statistical test (Fisher's exact test) was used to evaluate the significance of differences in the qualitative and quantitative variables without normal distribution. The differences were considered statistically significant at P value <.05.
Results
A total of 55 patients (49 men and 6 women) completed the study. Four men and 1 woman, who underwent unilateral repair, withdrew from the study due to various reasons. Taking into consideration that bilateral procedure was performed in 10 out of 55 patients who completed the study, we analyzed the position of 65 implants. Thus, the withdrawal of 5 patients with no mesh fixation from the study did not affect the results of the statistical analysis.
Clinical data
There were no complications in the immediate postoperative period. All patients were discharged from the hospital on the first day after the procedure. Follow-up clinical assessment did not reveal any hernia recurrence or chronic pain syndrome on day 1, and after 1, 3, 6, and 12 months. Left-side hydrocele was diagnosed in 1 patient within 1 month after bilateral TAPP and required Winkelmann procedure.
The foreign body sensation and discomfort in the right inguinal region within a 12-month follow-up period were reported by 2 patients aged 34 and 38 years (body mass index <25 kg/m2; with no comorbidities) who underwent right-sided and bilateral TAPP with mesh fixation. These events occurred after 3 and 6 months after the procedure, respectively, they disturbed patients periodically and persisted until the end of the follow-up period. Physical examination revealed no abnormalities (defects or protrusions) of the posterior wall of the inguinal canal at rest and during the cough test. Table 2 presents the results of follow-up clinical examinations at 1, 3, 6, and 12 months after the procedure.
Results of Clinical Examinations During 1-Year Follow-Up Period
Thus, the follow-up observation during the first year demonstrated the persistence of discomfort in the area of intervention in 3% of the patients who had mesh fixation.
Ultrasound data
Ultrasound of the intervention area did not reveal any signs of mesh migration in any patient. The mesh implant was located at the level of the inguinal canal, projected to the level of the pubic bone, and was seen completely overlying the deep inguinal ring and inguinal canal throughout the follow-up period. At the same time, ultrasound has demonstrated significant changes in the appearance (shape and thickness) of mesh at consecutive postoperative scheduled visits, depending on the time elapsed postprocedure. Mesh presented on ultrasound as an echogenic linear or wavy structure in the region of the pubic bone with some posterior acoustic shadowing. Ultrasound appearance depended on the time elapsed after the procedure and the use of fixing elements.
Thus, in patients without mesh fixation, it had an echogenic wavy appearance on the first day and at 1 month after TAPP, and then changed to a straight echogenic line from month 3 and appeared as almost straight line after 12 months (Table 3 and Fig. 3).
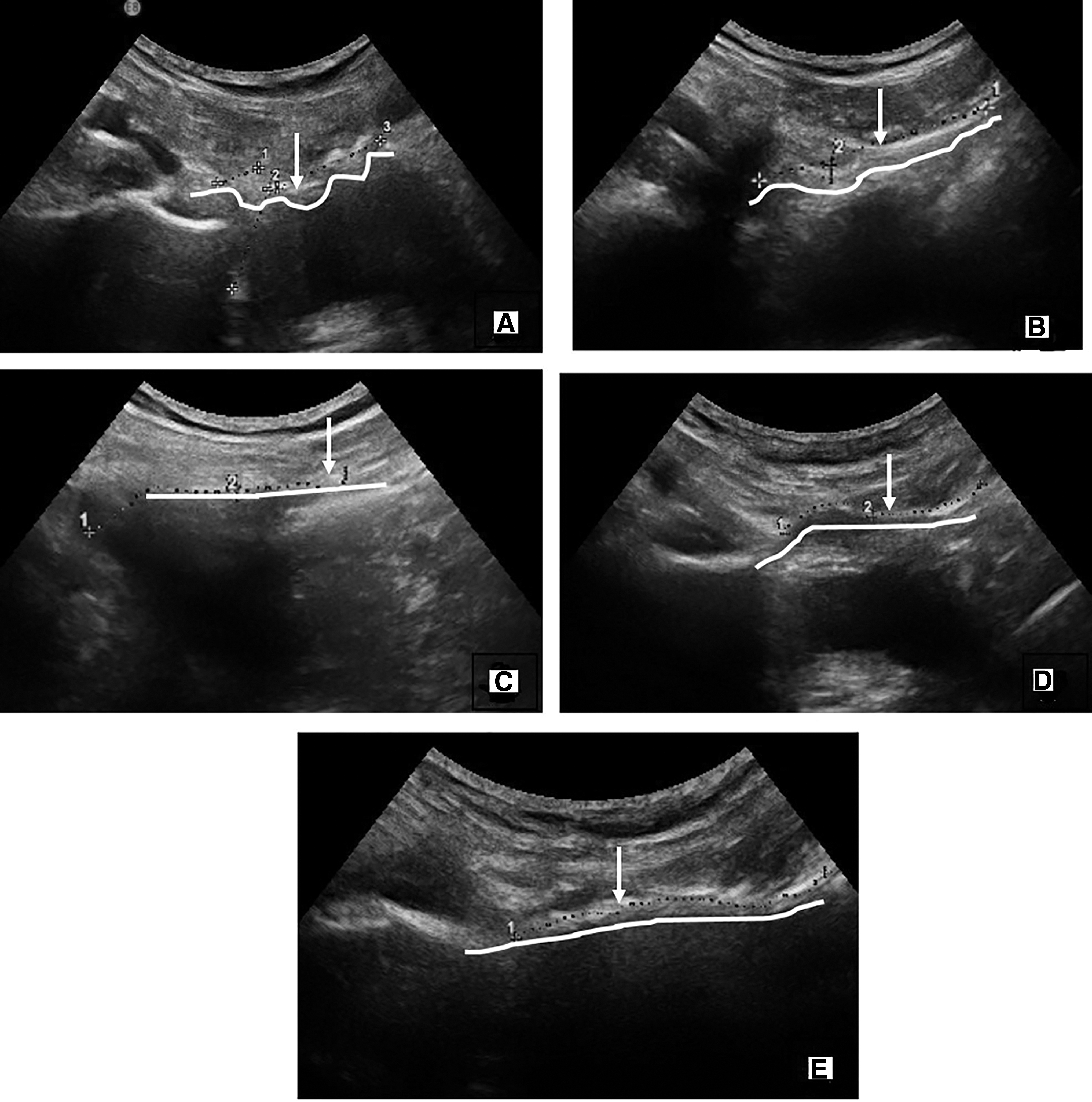
Ultrasound images. Changes in the appearance of a nonfixed mesh throughout 12 months of follow-up period.
Changes in Meshes Geometry According to the Ultrasonography Data During the 1-Year Follow-Up Period
In contrast, among patients with mesh fixation, the implant had an echogenic linear appearance in the immediate postoperative period but became wavy starting from month 3 onward (Fig. 4).
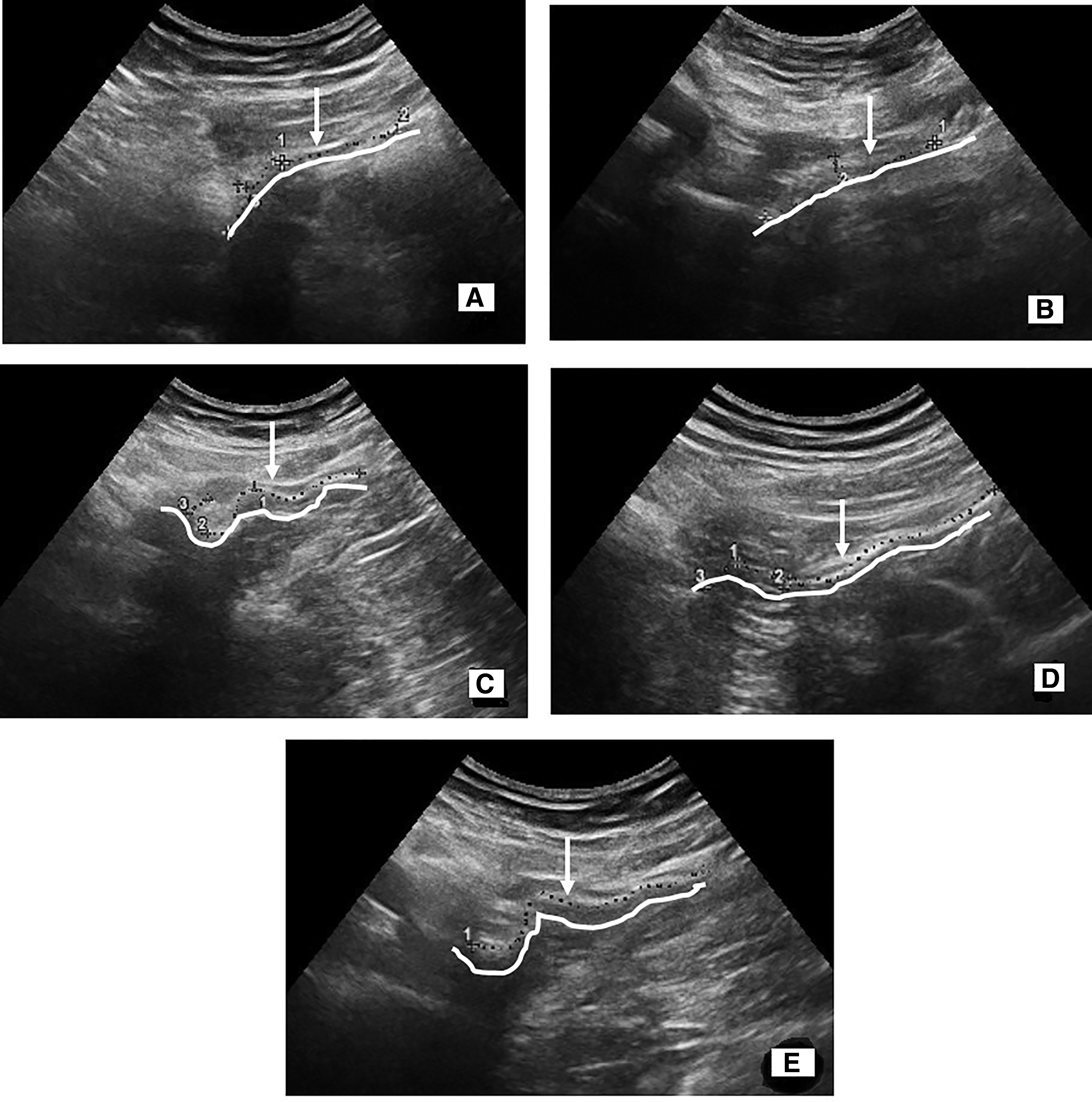
Ultrasound images. Changes in the appearance of a fixed mesh throughout 12 months of follow-up period.
The initial thickness of the mesh used in this study was 0.4 mm. During the ultrasound examination, it presented as a thin hyperechoic band, with variable thickness from 1.2 to 3.9 mm depending on the time elapsed after the procedure (Table 4). The mean mesh thickness was 2.2 ± 0.1 mm on the first day after the procedure and increased to 2.8 ± 0.2 mm at month 1 and then decreased from 2.3 ± 0.2 mm at month 3 to 1.9 ± 0.1 mm at month 6 and to 1.6 ± 0.05 mm at month 12 of the follow-up period. No significant differences in thickness between patients with fixed or nonfixed mesh were observed at the end of the study; however, the thickness of the mesh has decreased at a slightly faster pace with patients who underwent the fixation by stapling.
Ultrasound Characteristics and Position of Meshes at Different Time Points of the Follow-Up Period
P < .05 comparison with the same indicator after 1 day, 1–3 months after transabdominal preperitoneal.
No associations between the presented changes in the appearance of the mesh due to gender, age, body weight, concomitant diseases, and the nature of the procedure performed were found.
Discussion
The effects of mesh material and technique of its fixation on the phenomena of prosthesis contraction and migration are not fully understood and are currently under research. However, in vast majority of cases, retraction, dislocation, and structural changes of the implant after hernia repair are studied only in the experimental settings.17,18 Studies have shown that morphological changes during the reparative process are of the same type and include aseptic inflammation around the mesh, angiogenesis, and the formation of connective tissue. The efforts to minimize the rates of postoperative complications (chronic pain, discomfort, and foreign body sensation in the site of intervention) led to the development of new polymeric materials for the open and endoscopic hernia repair. In this regard, the state of the mesh after TAPP is of great interest.
This study made it possible to establish that the mesh implant shape undergoes significant changes in the immediate and late postoperative period. The discomfort and foreign body sensation in the site of intervention were reported only by 2 patients with mesh fixation. Ultrasonography shows that in patients without stapling the implant appearance on the first day after the procedure is wavy, but after 3 months from the procedure, the implant is entirely “straightened” and it becomes linear in appearance. It might happen due to the integration of mesh with the surrounding tissues and the formation of a dense connective tissue scar. On the contrary, in the group of patients with mesh fixation, the prosthesis shape is linear on the first day and in the 3 months after the procedure, but later it became wavy, up to month 12 of the follow-up period. Such changes in the ultrasound appearance of the mesh may be due to its fixation to the muscles of the anterior abdominal wall, and their functional contractions lead to implant corrugation.
The changes in the mesh thickness can reflect the consecutive stages of the reparative process in the postoperative period. The implant used for the repair had the thickness of 0.4 mm, but even on the day 1 postprocedure it had the ultrasound appearance of an echogenic strip with a thickness of 1.6 to 2.8 mm (2.2 ± 0.1 mm), probably due to the presence of postoperative amount of fluid in the mesh and surrounding tissues. The development of aseptic inflammation around the implant was accompanied by its further thickening (up to 2.8 ± 0.2 mm on the average) by month 1 of the postoperative period, and the following attenuation of inflammation with mesh fibrillization and proliferation of the connective tissue contributed to reduction in the prosthesis thickness to 1.9 ± 0.1 mm at 6 months and up to 1.6 ± 0.05 mm at 12 months after the procedure.
The study had limitations due to a small number of participants, lack of three-dimensional imaging of mesh implants, and operator-dependent ultrasound examination. It is worth mentioning that during this study, the ultrasonography was performed by the same experienced sonologist throughout the entire follow-up period in each patient. This study results could be considered when choosing the TAPP, evaluating the treatment results, and predicting the risk of the inguinal hernia recurrence.
Conclusion
The findings from this study suggest that there are significant changes in the ultrasound appearance of mesh used in the TAPP depending on the time elapsed postoperatively. Moreover, the ultrasound data confirmed the occurrence of aseptic inflammation in the wound and around the mesh, with its consecutive stages reflecting the change in the implant thickness. The study demonstrated that the position of the endoprosthesis remained stable, with no migration in the inguinal triangle whether it was fixed or not.
Authors' Contributions
Study concept and design were by S.G.G. and D.A.C. S.G.G., G.D.S., and D.A.S. wrote the article. Statistical analysis was done by G.D.S. and D.A.S. S.G.G., D.A.S., and D.A.C. reviewed the draft. Final approval was by S.G.G., D.A.S., D.A.C, and G.D.S.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.