
Abstract
Background:
Laparoscopic posterior exenteration (total and supralevator) is a complex and rarely done procedure. In this study we describe the surgical technique and short-term perioperative outcomes in 7 female patients of locally advanced carcinoma rectum operated with laparoscopic pelvic exenteration.
Materials and Methods:
We report 7 cases of carcinoma rectum involving either posterior wall of the uterus or vagina, which were operated with a laparoscopic procedure. All perioperative and intraoperative data were collected retrospectively from prospectively maintained electronic data.
Results:
Nine female patients with the diagnosis of nonmetastatic locally advanced lower rectal adenocarcinoma were selected. In MRI 4 patients had uterus-cervix involvement and 3 patients had a posterior vaginal wall and anal sphincter involvement. Four patients were operated with laparoscopic supralevator posterior exenteration and 3 patients were operated with laparoscopic complete posterior exenteration. Three patients underwent vaginal reconstruction, which was done with bilateral V-Y plasty. All 7 patients received neoadjuvant chemoradiotherapy (NACTRT), 3 patients also received additional chemotherapy (CAPOX regimen) due to poor response to NACTRT. Mean body mass index (BMI) was 23.85 (range 19–27.20). Mean duration for complete posterior exenteration was 9.63 hours (range 7–12 hours). Mean duration for supralevator posterior exenteration was 6.81 hours (range 6.25–7.5 hours). The mean postoperative stay was 10.71 days (range 7–16 days). Mean blood loss was 700 mL (range 200–1800 mL). On postoperative histopathology, all margins were free of tumor in all cases.
Conclusion:
Laparoscopic approach for locally advanced carcinoma rectum in female patients is feasible with less morbidity and safe short-term oncological outcomes. Careful selection of patients based on MRI is a must before undertaking the minimally invasive surgery approach. Long-term outcomes are still unknown and will require long-term follow-up.
Introduction
Locally advanced rectal carcinoma in females necessitates sometimes resection of the uterus and the posterior vaginal wall along with the primary. Total posterior and supralevator posterior exenteration techniques have been described with an open approach, but laparoscopic resection is rarely done in view of the complexity of the procedure and locally advanced nature of the disease. With the help of preoperative MRI, we can carefully select patients for laparoscopic exenteration so that oncological safety is not compromised. The laparoscopic procedure with its inherent benefits decreases surgical morbidity to a considerable extent. In this study we describe 7 cases of laparoscopic posterior exenteration (3 complete and 4 supralevator) who were operated at Tata Memorial Hospital between August 2018 to September 2019.
Materials and Methods
We report 7 cases of locally advanced rectal adenocarcinoma, which were operated between August 1, 2018 and September 13, 2019 at Tata Memorial Hospital, Homi Bhabha National University, Mumbai. All patients were presented with carcinoma rectum involving either uterus, cervix, or posterior vaginal wall. After local imaging (MRI pelvis) (Fig. 1) and metastatic work-up (contrast-enhanced computed tomography of the thorax and abdomen), all patients were treated with neoadjuvant chemoradiotherapy (NACTRT). Of 7 patients, 3 patients also received additional neoadjuvant chemotherapy due to poor response post-NACTRT. With preanesthetic work-up and fitness 3 patients underwent laparoscopic complete posterior exenteration (en bloc abdominoperineal resection + bilateral hystero-salpingo-oophorectomy ± posterior vaginal wall resection ± lateral pelvic lymph node dissection + V-Y plasty) and 4 patients underwent supralevator posterior exenteration (en bloc low anterior resection bilateral hystero-salpingo-oophorectomy ± lateral pelvic lymph node dissection). Lateral pelvic node dissection was performed only when significant nodes were present on post-CTRT MRI scan. All perioperative and intraoperative data were collected retrospectively from prospectively maintained electronic data. (Tables 1, 2 and 3)
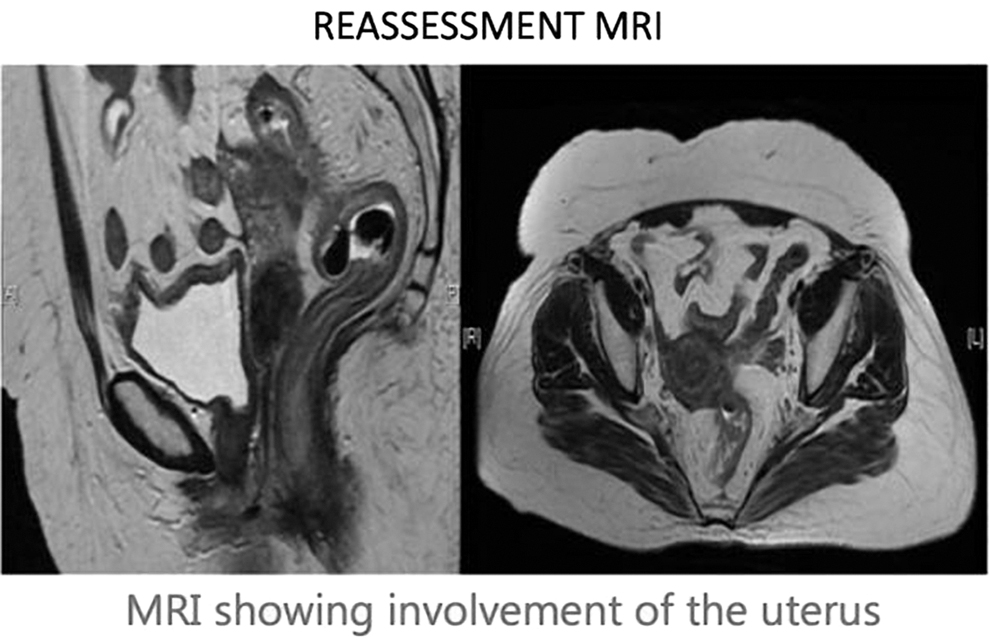
MRI showing involvement of uterus by carcinoma rectum.
Demographic Parameters
ASA, American Society of Anesthesiologists; BMI, body mass index; ECOG, Eastern Cooperative Oncology Group.
Clinical Parameters
F/B Chemo, followed by chemotherapy; MDAC, moderately differentiated adenocarcinoma; NACTRT, neoadjuvant chemoradiotherapy.
Intraoperative and Postoperative Parameters
CRM, circumferential resection margin; DRM, distal resection margin; LPLND, lateral pelvic lymph node dissection.
Surgical technique
With epidural and general anesthesia, the patient was placed in Lloyd-Davis position. Small towel bolster was placed under the buttocks. Shoulder support and chest belt were enforced so that steep Trendelenburg position and right lateral tilt can be given safely. It assists in removing small bowel out of the pelvis and facilitates good exposure of the operative area. Camera port (12 mm) was inserted at the umbilicus with open Hassan's technique, four ports were inserted (two 12 mm and two 5 mm) as depicted in the picture (Fig. 2).
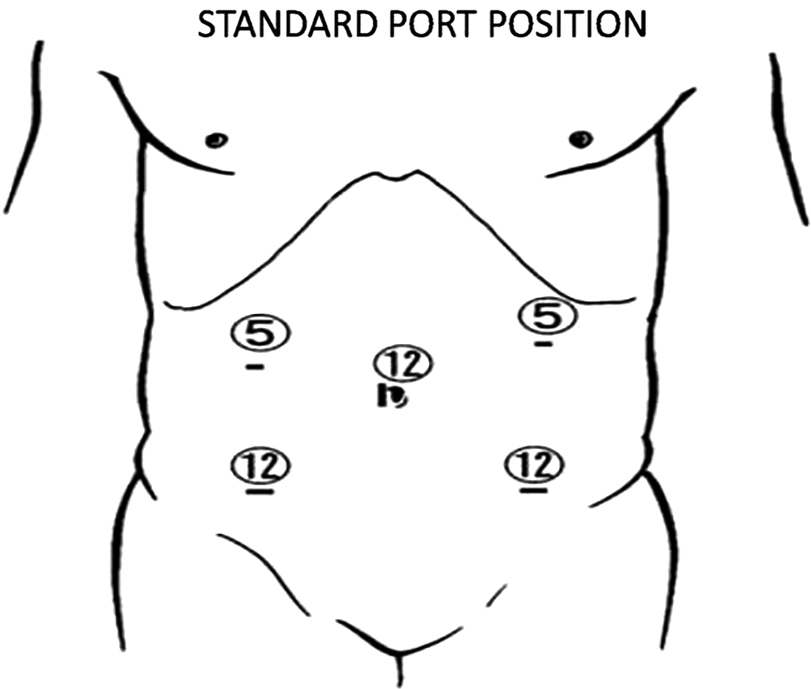
Port position.
The small bowel was positioned out of the operative field. With surgeon standing on the right side of the patient, medial to lateral dissection was made out to mobilize rectosigmoid and left colon. Inferior mesenteric vein (IMV) identified lateral to duodenojejunal flexure. The plane was identified below IMV and dissected superolateral till the inferior edge of the pancreas and spleen was identified (Fig. 3). This step helps in further mobilization of splenic flexure at the later stage of operation. Downward with assistant giving traction to sigmoid mesentery areolar plane identified between the sigmoid mesentery and retroperitoneum. Further medial-to-lateral dissection of the rectosigmoid mesentery was done, until the left lateral abdominal wall reached (Fig. 4). An inferior mesenteric artery was ligated and cut at the origin (Fig. 5). Retro rectal space was dissected until the origin of levator ani muscle (Fig. 6). Then peritoneal cuts were made along bilateral external iliac vessels reaching up to the medial umbilical ligament. The round ligament was identified and cut. Infundibulopelvic ligament with ovarian vascular pedicle was ligated and cut.
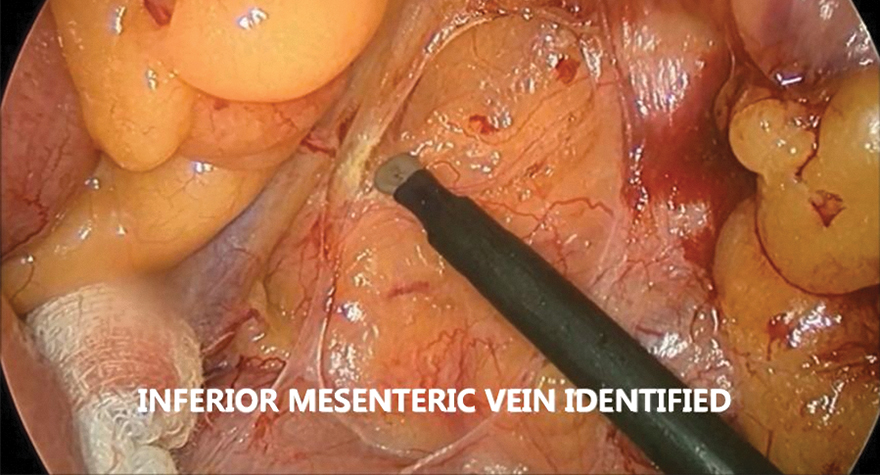
Inferior mesenteric vein dissection.
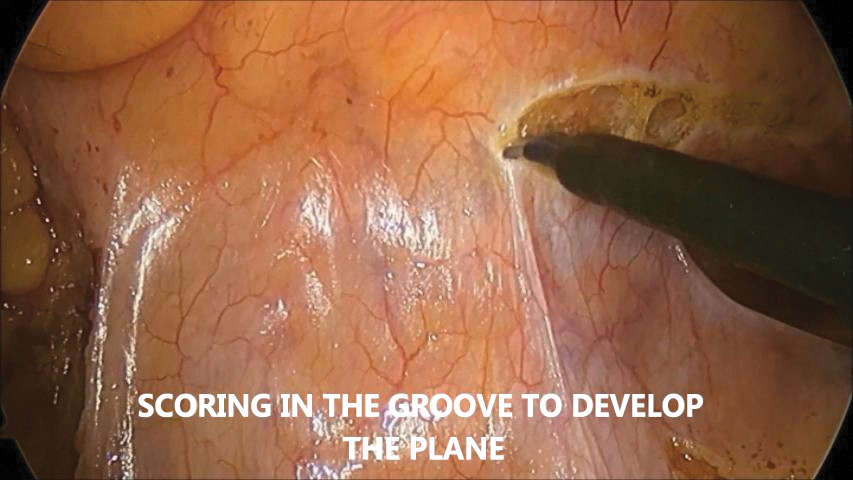
Medial to the lateral dissection of left colon mesentery.
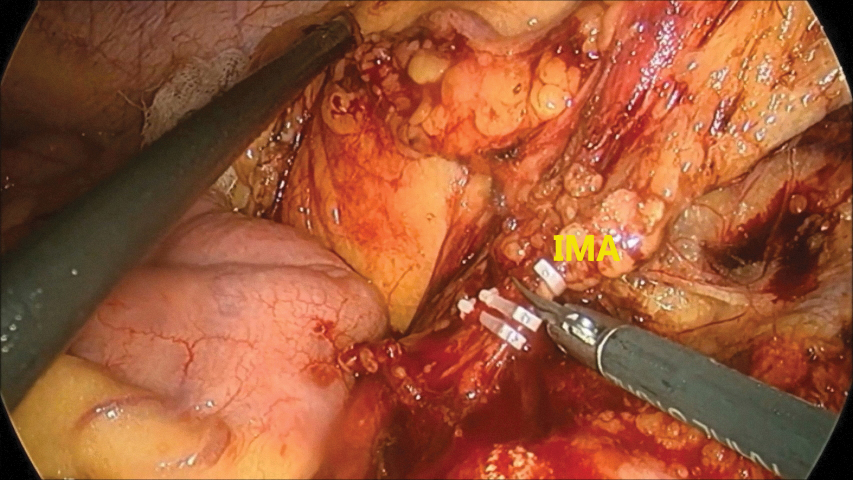
IMA ligation. IMA, inferior mesenteric artery.
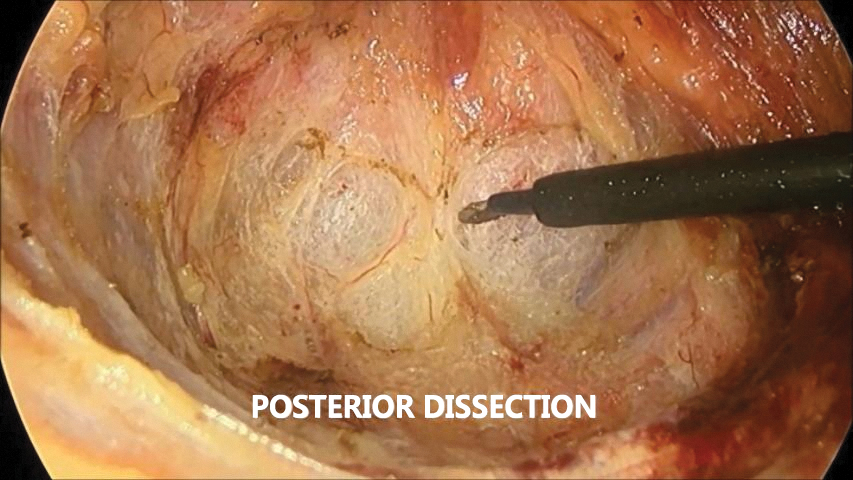
Retrorectal space dissection.
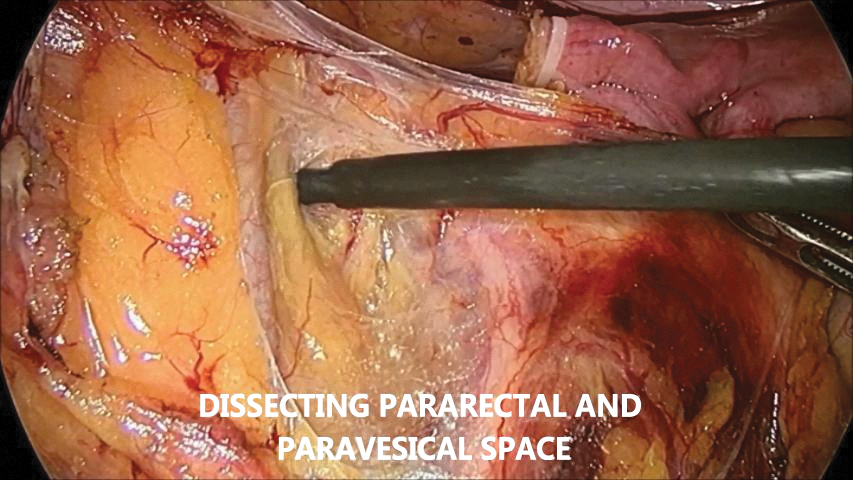
Pararectal spaces were developed on both sides after mobilizing and medializing ureters. Paravesical spaces were developed after dissecting obliterated umbilical artery in it (Fig. 7). Both spaces were connected after ligating uterine artery at its origin (Fig. 8). The ureter was dissected in ureteral tunnel till ureterovesical junction. Uterine veins below ureter were taken with energy device. The ureter was lifted laterally and all fibrofatty tissue, including parametrium, was cut till levator ani muscle.
Pararectal space dissection with medialization of the ureter. LIA, left iliac artery; LU, left ureter.

PV and PR dissection. OUA, obliterated umbilical artery; PR, pararectal; PV, paravesical; UA, uterine artery.
Similar steps were carried on the opposite side. Anterior dissection consists of mobilizing uterus from a urinary bladder. After exposing the anterior vaginal wall, a transverse cut was taken and vagina opened. This anterior cut is placed at a secure distance from tumor involving vaginal vault (Fig. 9). The posterior wall of the vagina was then cut to reach the mesorectal plane (Fig. 10). The posterior cut was carried at a lower level than anterior if the posterior vaginal wall is involved in MRI. As sometimes uterus gets rotated over the rectum and make the terminal part of dissection difficult. To keep off this stitch was taken from the fundus of the uterus to the rectum that facilitates further dissection.
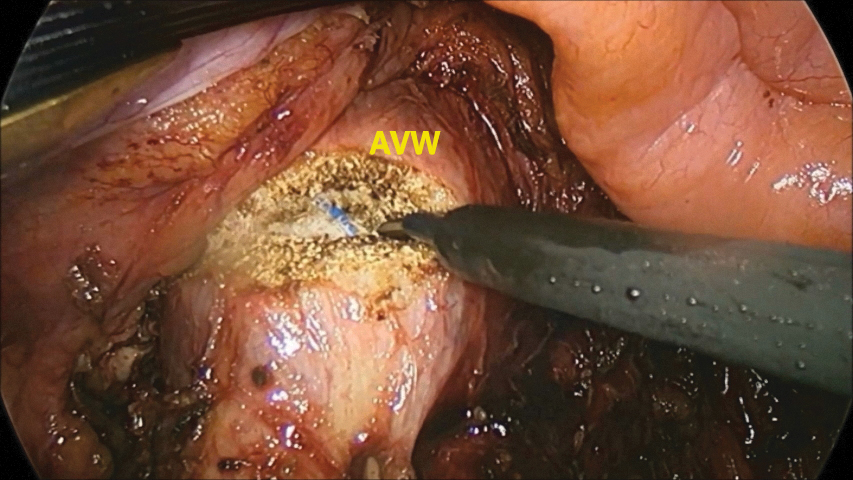
AVW cut taken. AVW, anterior vaginal wall.

PVW cut taken. PVW, posterior vaginal wall.
Further dissection was carried along in the mesorectal plane along the rectovaginal septum till levator ani is reached. After confirmation of tumor-free margin, the lower rectal wall was identified below mesorectum and cut with echelon stapler (Fig. 11). All tissue medial to the illiac vessels was included in the specimen. Proximally sigmoid colon was cut with echelon stapler and the specimen was delivered through 5 cm transverse incision at left iliac fossa. Anvil of circular stapler was inserted in the distal sigmoid colon end and the bowel was returned to the pelvis. The vaginal vault was closed with absorbable suture in a continuous manner (Fig. 12). After mobilizing splenic flexure further tension-free colorectal anastomosis was performed with a circular stapler (Fig. 13). The integrity of the anastomosis was checked with the air leakage test.
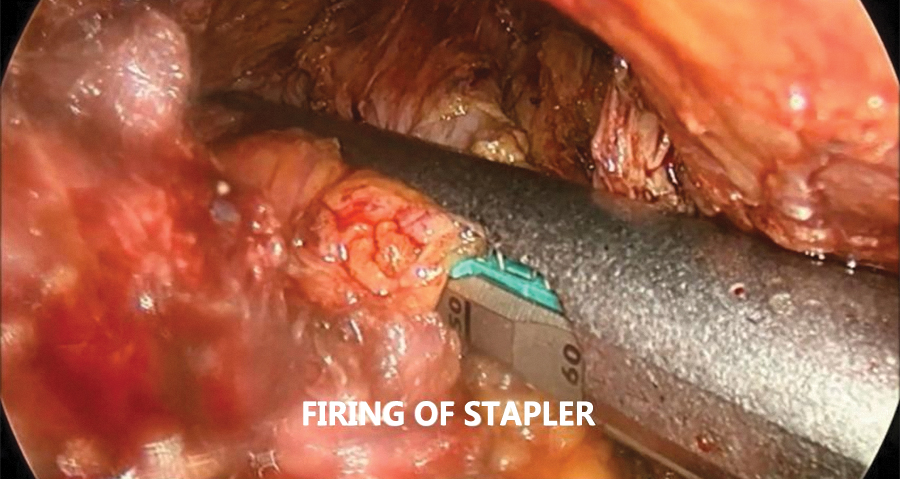
Lower rectum transected with the stapler.
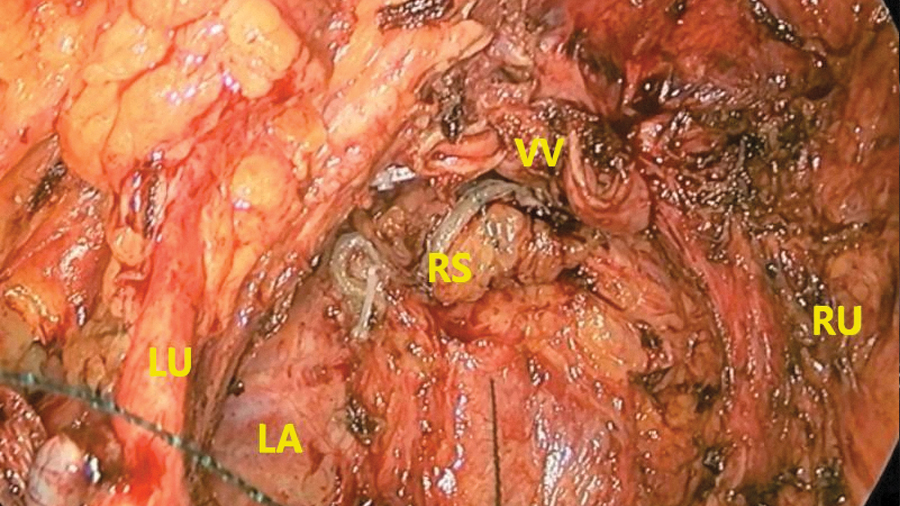
VV sutured. LA, levator ani; LU, left ureter; RS, rectal stump; RU, right ureter; VV, vaginal vault.
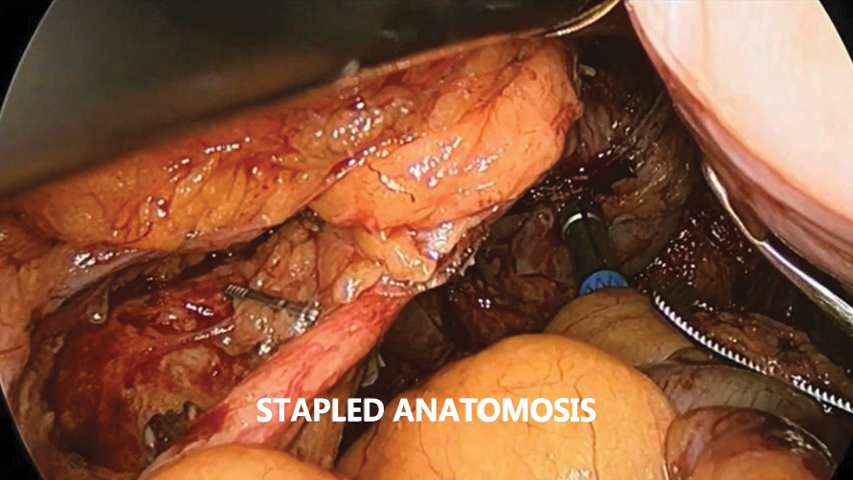
Circular stapler coloanal anastomosis in supralevator posterior exenteration.
Patients who had anal sphincters involved in MRI were planned for abdominoperineal resection. Here surgical steps till the anterior vaginal wall cut are the same, then with concern to safeguard mobilized ureter posterior vaginal wall was excised with the specimen. After this result of dissection was done through a perineal approach similar to a standard abdominoperineal resection. Posterior vaginal wall reconstruction and perineal wound closure were performed with a bilateral V-Y plasty procedure in a prone position (Fig. 14). End sigmoid stoma was fashioned at left iliac fossa and matured (Supplementary Video S1).
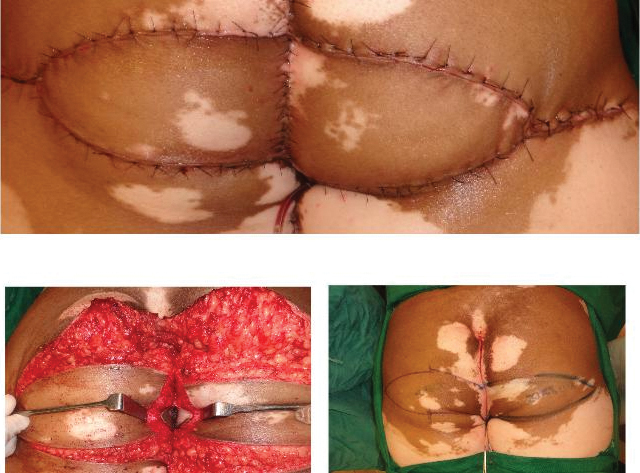
Posterior vaginal wall reconstruction with V-Y plasty.
Results
Seven female patients with the diagnosis of nonmetastatic locally advanced lower rectal adenocarcinoma were selected for a laparoscopic procedure. In MRI 4 patients had uterus-cervix involvement and 3 patients had a posterior vaginal wall and anal sphincter involvement. Four patients were operated with laparoscopic supralevator posterior exenteration and 3 patients were operated with laparoscopic complete posterior exenteration without conversion to open surgical operation. Lateral pelvic lymph node dissection was performed in 3 patients, who had nodes involved in post-NACTRT MRI. Three patients underwent posterior vaginal wall resection, in whom vaginal reconstruction was done with bilateral V-Y plasty. All 7 patients received NACTRT, 3 patients also received additional chemotherapy (CAPOX regimen) due to poor response to NACTRT. Mean BMI was 23.85 (range 19–27.20). Average duration for complete posterior exenteration was 9.63 hours (range 7–12 hours). Mean duration for supralevator posterior exenteration was 6.81 hours (range 6.25–7.5 hours). The mean postoperative stay was 10.71 days (range 7–16 days). Mean blood loss was 700 mL (range 200–1800 mL). On histopathology, all patients had a free circumferential resection margin and distal resection margin. Postsurgery 2 patients developed a perineal wound infection. One patient developed prolonged ileus. One patient developed anastomotic dehiscence, which was managed conservatively (Table 3).
Discussion
The role of minimally invasive surgery in rectal cancer surgery has been shown to have equivalent oncological outcomes and better short-term outcomes such as the length of incision, pain control, and early discharge.1–4 Nevertheless, these studies included only total mesorectal excision (TME). Data regarding minimally invasive surgery (MIS) in beyond TME is usually concerned with total pelvic exenteration.5–9
As minimally invasive surgery is progressing and more experience is gained, even for complex advanced rectal cancers laparoscopy-guided procedures has shown better short-term outcomes compared with open procedures. T4 rectal cancer has bad prognosis and survival. Although neoadjuvant treatments have improved outcomes, exenteration procedures remain the lone option for a cure.
Laparoscopic posterior exenteration in females is a rarely done procedure mainly for locally advanced gynecological malignancies.10,11 MIS for gynecological malignancies is usually performed as an alternative to chemoradiation (CTRT), hence dissection is less tedious and morbidity of procedures such as ureteral tunneling and pelvic node dissection is less. However, salvage surgery for recurrence after CTRT in gynecological malignancies is associated with CTRT. As well, the benefits of such surgery are offset by limited lifespan in such salvage cases. 10
As far as we know there are just a few case reports available of laparoscopies posterior exenteration for carcinoma rectum. 12 Although open posterior exenteration is a known established procedure, it has been rarely performed with the complete minimally invasive approach. Ours is a high volume center where each year >300 rectal cancer surgeries are done with an MIS approach. Our data show comparable short- and long-term outcomes. 13 We also have experience of extended TME and pelvic exenteration surgeries through the MIS approach. 5
In this study we present 7 cases of locally advanced rectal cancer involving the uterus and posterior vaginal wall who were operated with the complete laparoscopic approach. We have carefully selected patients having central involvement for the laparoscopic procedure as we believe that these are the best candidates for a laparoscopic procedure. MRI is an investigation of choice and mandatory for planning surgery. All patients received NACTRT i/v/o locally advanced disease as it has shown to decrease the rate of local recurrence. Three patients who had a poor response to NACTRT received an addition three to four cycles of neoadjuvant chemotherapy. Patients having lateral pelvic wall involvement were excluded and operated with an open operation.
We have found the mean duration of the procedure was comparable with an open procedure that we have done at our institute (9.63 hours for complete and 6.81 hours for supralevator). Mean postoperative stay (10.71 days) and blood loss (700 mL) are less compared with an open procedure; we have found that the laparoscopic procedure has considerably decreased immediate postoperative morbidity with faster recuperation.
Immediate oncological outcomes have shown complete R0 resection with all margins free of disease. Long-term oncological outcomes are not known for which there should be large, comparative, and long-term follow-up. We can conclude that for selected central T4 rectal cancers in females, the laparoscopic procedure provides a less morbid and oncologically safe option.
Conclusion
Laparoscopic approach for locally advanced carcinoma rectum in female patients is feasible with less morbidity and safe short-term oncological outcomes. Careful selection of patients based on MRI is a must before undertaking the MIS approach. Long-term outcomes are still unknown and will necessitate long-term follow-up.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.