
Abstract
Purpose:
The effect of intracorporeal anastomosis (IA) versus extracorporeal anastomosis (EA) in laparoscopic right hemicolectomy is controversial. The aim of this study was to evaluate the safety, effectiveness, and functional outcomes of IA compared with EA and to explore the timely tendency variations favoring one treatment over another.
Materials and Methods:
PubMed, EMBASE, and Web of Science were consulted. A systematic review, pairwise meta-analysis, and cumulative meta-analysis were conducted.
Results:
Twenty-three studies (3755 patients) were included: 45.7% underwent IA, whereas 54.3% underwent EA. The estimated pooled postoperative infectious complications, anastomotic leak, and overall complications risk ratios were 0.51 (95% confidence interval [CI]: 0.31 to 0.84; P = .009), 0.64 (95% CI: 0.40 to 1.03; P = .063), and 0.78 (95% CI: 0.62 to 0.97; P = .028), respectively. The cumulative meta-analysis showed a statistically significant timely tendency in favor of IA while considering infectious and overall complications. The estimated pooled mean difference of time to first flatus, first defecation, first oral diet, and hospital stay were −16.68 (P < .001), −25.94 (P < .001), −16.35 (P < .001), and −0.72 (P < .001), respectively. Again, the cumulative meta-analysis showed a statistically significant timely trend in favor of IA. No differences were found in term of operative time, conversion rate, ileus, bleeding, reoperation, 30-day readmission, and 30-day mortality.
Conclusions:
Compared with EA, IA seems to be associated with reduced postoperative infectious and overall complications. The time to first flatus, time to defecation, time to liquid diet, and hospital length of stay were estimated to be lower. A statistically significant timely trend favoring IA was noticed for postoperative infectious complications, overall complications, and recovery parameters. Further studies are warranted to confirm these results and to deeply investigate the supposed timely tendency convergence in favor of IA.
Introduction
Laparoscopic Right Hemicolectomy (LRH) is considered by many the standard of care in the treatment of malignant and benign diseases of the right colon. Compared with open, it allows faster recovery, low rates of wound infections with analogous oncological results.1–4 Intracorporeal anastomosis (IA) and extracorporeal anastomosis (EA) have been described for ileocolic anastomosis. EA requires greater mobilization, mesenteric tractions, and exteriorization of the bowel through an abdominal incision. IA does not require bowel exteriorizations and reduces intestinal manipulation; however, it is technically demanding and mandates advanced laparoscopic skills. 5
Several observational studies assessed the safety and efficacy of IA versus EA with discordant results.6–15 These were limited by the study design, narrow population, and background bias. Published meta-analyses tried to analyze short-term outcomes, morbidity, mortality, and recovery parameters when comparing IA and EA.16–20 However, results were discordant and nonconclusive with a high between-study heterogeneity. Since recent studies have been published on this topic, we performed an updated systematic review and a cumulative meta-analysis.
The aim of this study was to evaluate the safety, effectiveness, and functional outcomes of IA compared with EA and to explore the timely tendency variations of the combined total effect.
Materials and Methods
This study was realized according to the Preferred Reporting Items For Systematic Reviews and Meta-Analyses (PRISMA) statement. 21 A literature search was conducted by three authors (A.A., G.G., E.R.). All English-written published articles that compared IA and EA in LRH from January 2009 to December 2018 were identified. Web of Science, PubMed, and Embase datasets were referred while applying the key words “Intracorporeal anastomosis AND extracorporeal anastomosis AND laparoscopic right hemicolectomy*.” The references of each article were assessed to complete the research.
Inclusion criteria: (1) outcomes comparison for IA versus EA in the setting of LRH; (2) English written; (3) papers with the longest follow-up or the largest sample size in case of articles published by the same study group or based on the same dataset. Exclusion criteria: (1) not English written; (2) no clear methodology; (3) no distinction between IA and EA; (4) articles with less than 10 patients per study arm.
All articles comparing IA and EA in the setting of LRH were incorporated in the review, and data were independently extracted by three authors (A.A., G.G., E.R.). Derived data: study characteristics (author's name, journal, and year of publication), patients' number, operative time, hospital length of stay (HLOS), 30-day reoperation, 30-day readmission, postoperative outcomes, recovery parameters, and 30-day mortality. Data were compared only at the end of the survey, and discrepancies were resolved by dissertation.
Postoperative infectious complication was defined in conformity with the Center for Disease Control and Prevention (CDC) guidelines and categorized as organ/space, deep, or superficial surgical site infection, pneumonia, sepsis, and urinary tract infection. The anastomotic leak was clinically or radiologically diagnosed as a weakness of the intestinal wall with luminal content extravasation. 22 If independently reported, the development of intra-abdominal abscess was investigated separately to anastomotic leak. 23 Postoperative morbidity was defined according to authors reporting or to the Clavien-Dindo classification. 24 Time to first flatus, time to defecation, time to oral diet, operative time, and HLOS were defined in accordance to different studies. All surgeries required within 30 days after surgery were categorized as reoperation. Incisional hernias were detailed as protrusions of the abdominal contents through a wall defect.
The Newcastle-Ottawa Scale (NOS) was independently used by three investigators (A.A., G.B., D.B.) to assess the quality of the papers. Final judgment is established on a “star system” based on the study group's selection and evaluation of the outcome of interest. A total of nine star is the maximum score for each article. 25 The randomized controlled trial (RCT) quality was appraised by using the Jadad scale. 26 A three-point questionnaire forms the basis for the Jadad score; a trial could receive a score of between zero (poor quality) and five (rigorous). The PROSPERO (International prospective register of systematic reviews) study protocol was CRD42019128580.
Statistical analysis
A Frequentist meta-analysis of pooled risk ratio (RR) and raw mean difference was performed. Cumulative meta-analysis was executed in chronological order to inspect how the evidence changed over time. 27 Inverse-variance method and DerSimonian-Laird estimator were performed for variance effect size (τ 2 ).28,29 I2 index and Cochran Q test were used to appraise the study's heterogeneity that was considered significant if P < .10 or I2 >50%.30,31 I2 index was calculated according to Higgins, whereas Wald-type 95% confidence interval (CI) was computed for pooled measure. 32 Prediction interval for treatment effect of a new study was measured. 30 Variance for continuous outcomes was estimated according to Hozo et al. 33 Sensitivity analysis was performed to corroborate the strength of results. P value <.05 was considered statistically significant. R software (version 3.2.2) was used for statistical analysis. 34
Results
Systematic review
Twenty-three studies matched the inclusion criteria (Fig. 1). Thirteen studies had a retrospective design, six had a prospective design, three had a propensity score-adjusted analysis, and one was a Randomized Controlled Trial interim analysis. All included studies earned a modified NOS score of 6 or 8 (median 7.1). The Jadad scale for the included RCT was three, suggesting a fair methodological study quality.
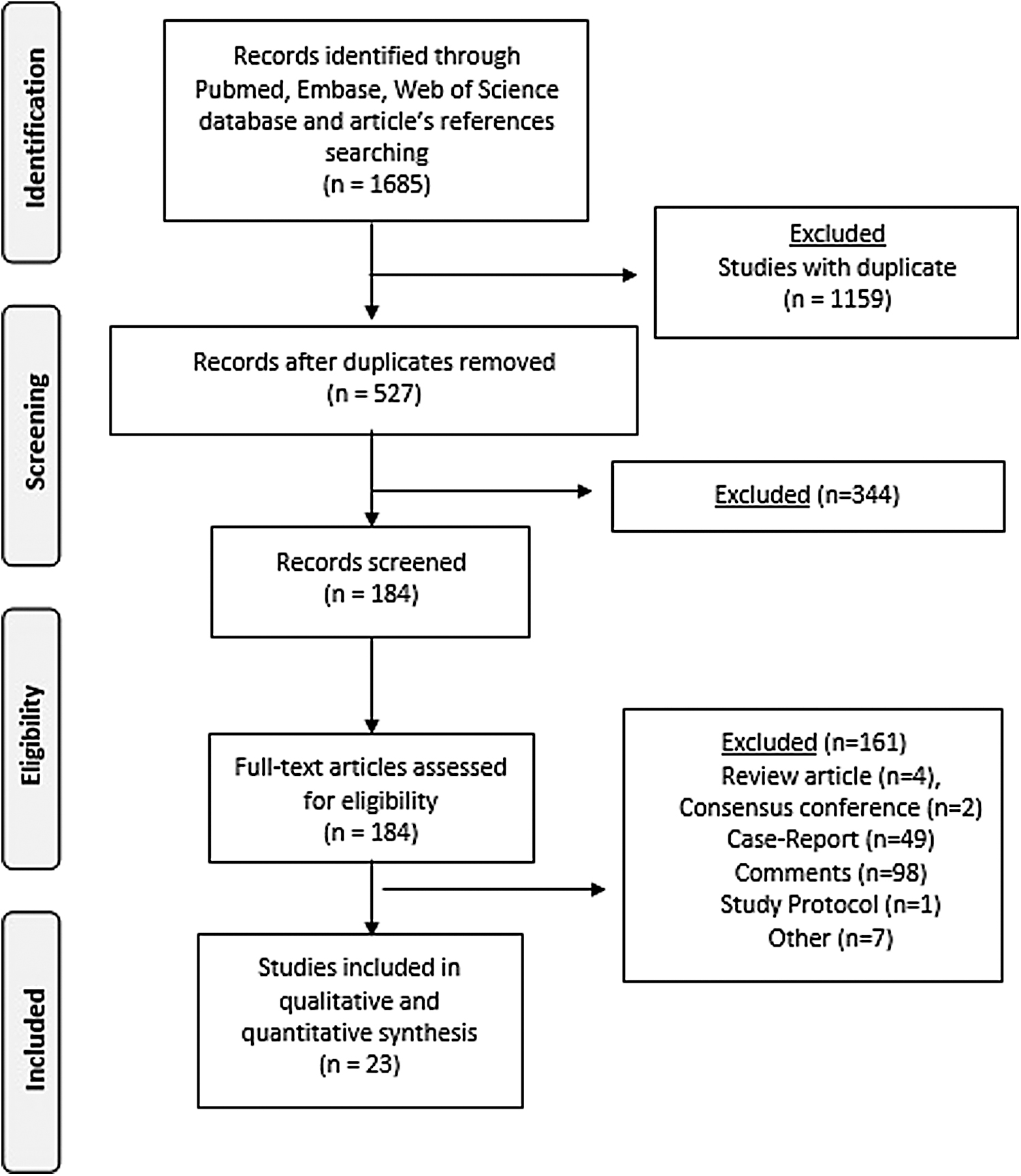
The PRISMA diagram. PRISMA, preferred reporting items for systematic reviews and meta-analyses.
Overall, 3755 patients were included for final analysis: 1720 (45.7%) underwent to IA, whereas 2035 (54.3%) underwent EA. The sample size of the studies ranged from 30 to 1029. Demographic, clinical, and operative variables of the patient sample are shown in Table 1. Overall, 2642 patients underwent right hemicolectomy for malignant disease whereas 891 patients underwent operation because of benign disease. Two studies reported aggregated results for malignant and benign disease (n = 222). The age ranged from 58.9 to 74.5 years, half were females, and the body mass index (BMI) ranged from 21 to 28.6. Nine studies reported the cancer localization, and 11 reported the TNM Classification of Malignant Tumors (TNM) or tumor stage. One study reported the medium-term follow-up and related outcomes.
Demographic and Clinical Characteristics of Patients Undergoing Laparoscopic Right Hemicolectomy with Intracorporeal Anastomosis and Extracorporeal Anastomosis
Data are reported as mean (standard deviation) or median (range).
B, benign; BMI, body mass index; EA, extracorporeal anastomosis; HLOS, hospital length of stay; IA, intracorporeal anastomosis; M, malignant; nr, not reported; Pros, prospective; PS, propensity score matching; RCT, randomized controlled trial; Ret, retrospective.
A stapled or hand-sewn side-to-side ileocolic anastomosis was fashioned in all cases. Enterotomies were closed by using different techniques. In the IA group, the specimen extraction site was different with the majority of the studies reporting a Pfannenstiel incision (88.9%), midline periumbilical (10.6%), and transvaginal (0.5%). In the case of EA, the most commonly reported incision for specimen extraction was the median periumbilical (94.3%). An upper right quadrant incision, right flank incision, and right lateral mini incision were adopted in 5.2% of patients. Pfannenstiel incision was used in 0.5% of cases.
The mean operative time ranged from 78 and 230 minutes, and the postoperative HLOS ranged from 4 to 12 days. The overall morbidity rate was 25.4%, and the overall anastomotic leak rate was 2.2%. The 30-day mortality was 0.51%. The postoperative pain was assessed in six studies and the time to first bed mobilization in one study. Global cost and the survival curves were not reported.
Meta-analysis
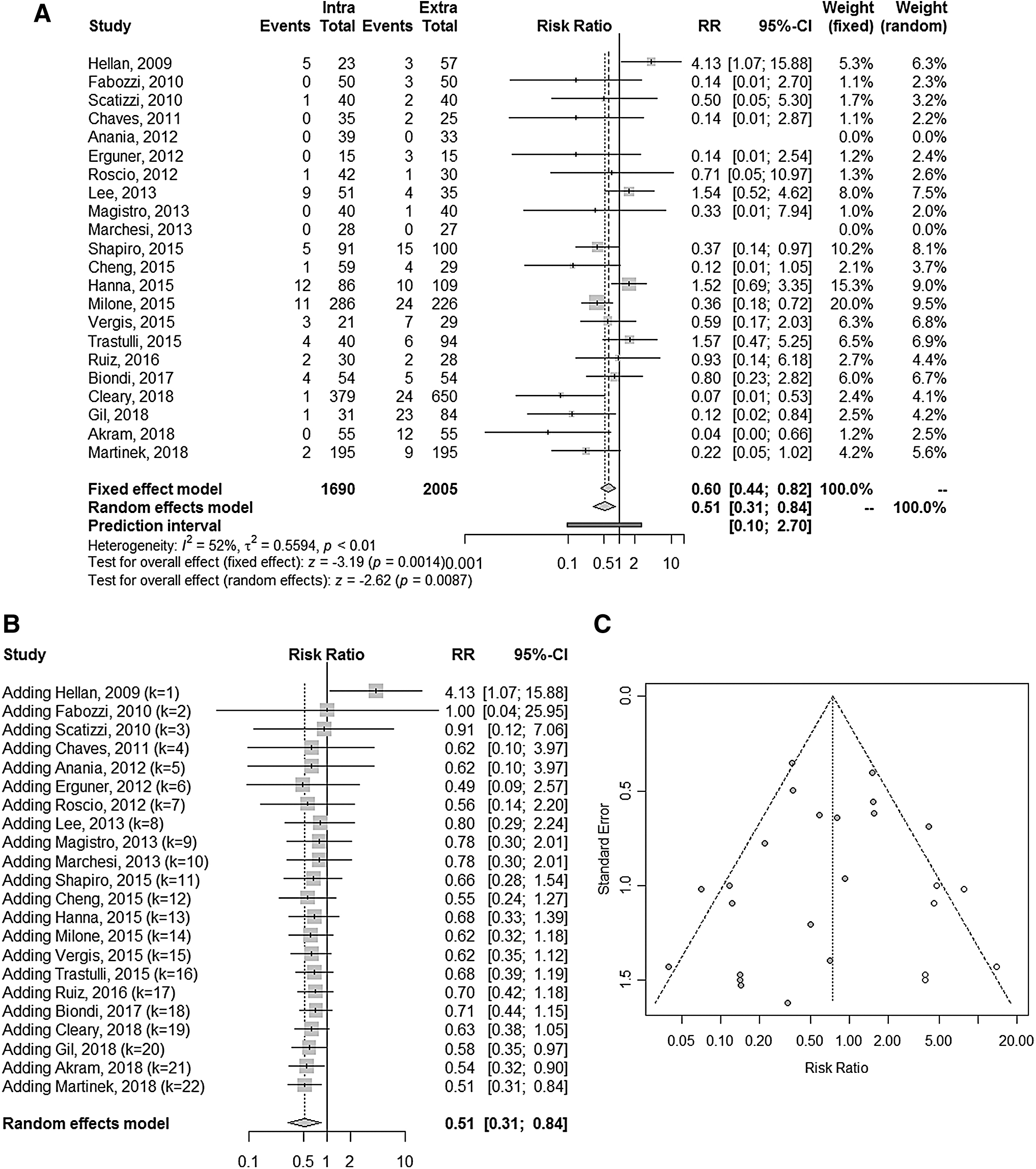
The estimated pooled postoperative infectious complications RR, resulting from 20 studies (3568 patients), is 0.51 (95% CI: 0.31 to 0.84; P = .009). The lower and upper limits are predicted to be 0.10 and 2.70, respectively. The heterogeneity is moderate (I 2 = 52%, 95% CI: 22.4 to 73.2; P = .003) and τ 2 = 0.625. Visual inspection of the Trim and Fill Funnel plot suggests the presence of publication bias effect confirmed by the adjusted Trim and Fill RR 0.81 (95% CI: 0.46 to 1.42; P = .463; I2 = 60.8%) and Egger test (P = .051). The sensitivity analysis shows the robustness of these findings in terms of point estimation, relative CIs, and heterogeneity. The cumulative meta-analysis showed a significant timely tendency in favor of IA (Fig. 2A–C). The estimated pooled wound infection RR (13 studies, 1928 patients) is 0.50 (95% CI: 0.31 to 0.80; P = .004). The heterogeneity is low (I 2 = 27%, 95% CI: 0.0 to 54.3; P = .204). The estimated pooled intra-abdominal abscess RR (7 studies, 1219 patients) is 1.04 (95% CI: 0.40 to 2.69; P = .932). The heterogeneity is zero (I 2 = 0.0%, 95% CI: 0.0 to 38.0; P = .851).
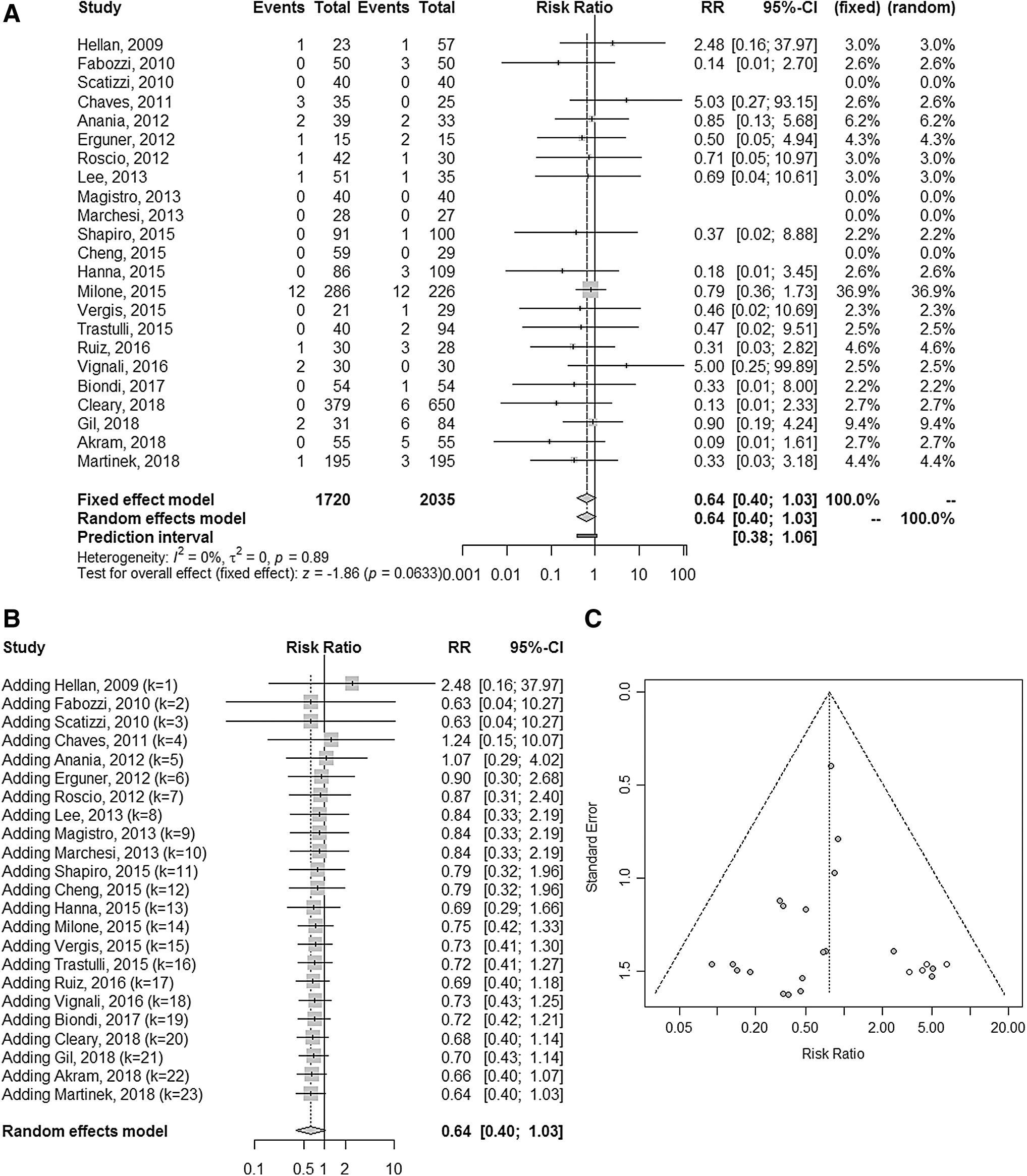
Again, the estimated pooled RR of anastomotic leak (20 studies, 3452 patients) is 0.64 (95% CI: 0.40 to 1.03; P = .063). The lower and upper limits are predicted to be 0.38 and 1.06, respectively. The heterogeneity is zero (I 2 = 0.0%; 95% CI: 0.0 to 25.5; P = .892) and τ 2 = 0.0. Trim and Fill Funnel plot does not show publication bias effect according to Egger test (P = .280). The adjusted Trim and Fill RR is 0.76 (95% CI: 0.46 to 1.23, P = .261; I2 = 0.0%). The sensitivity analysis shows the robustness of these findings in terms of point estimation, relative CI, and heterogeneity. The cumulative meta-analysis showed a timely trend in favor of IA that does not reach statistical significance (Fig. 3A–C).
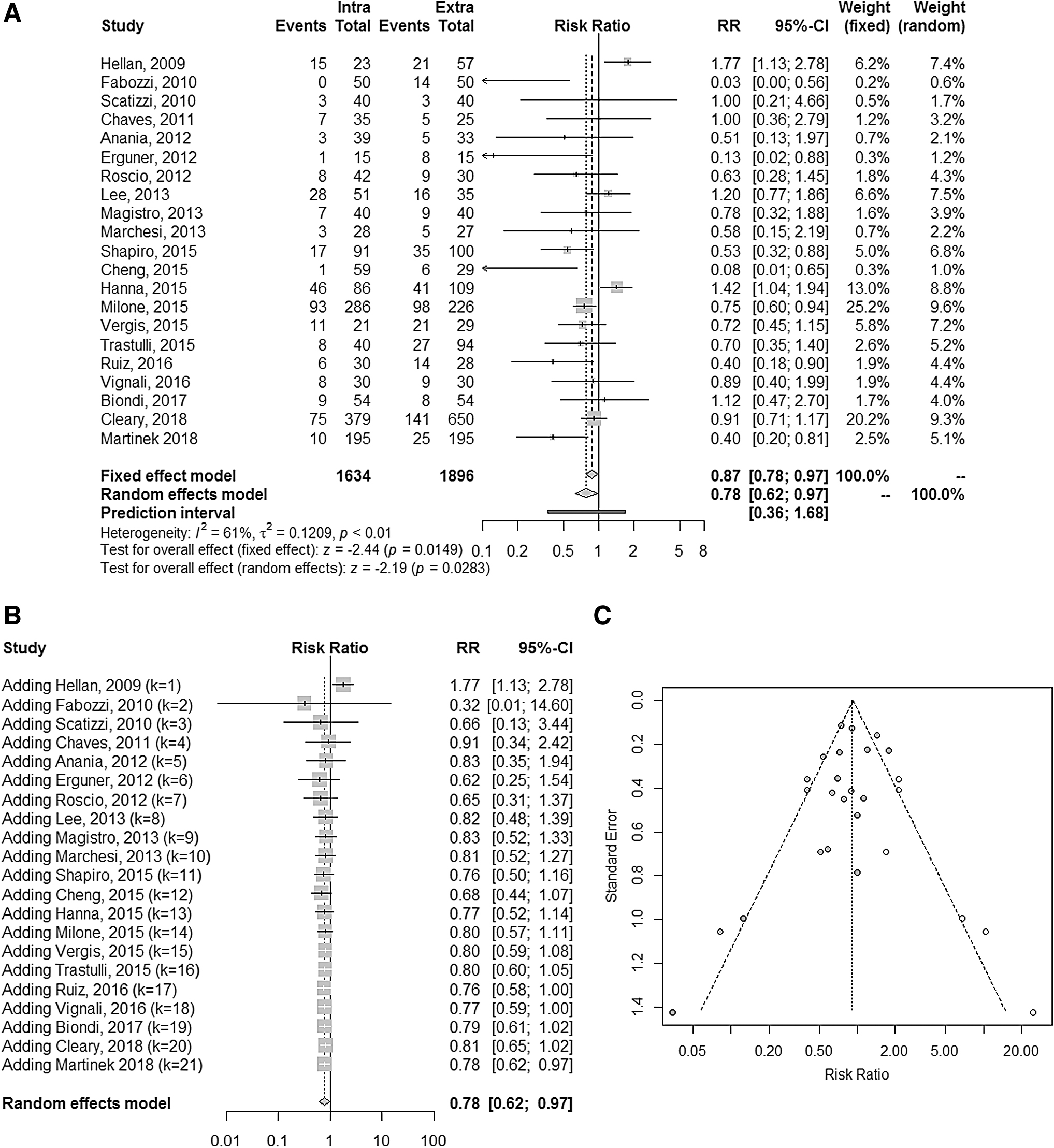
The estimated pooled overall complication RR (21 studies, 3530 patients) is 0.78 (95% CI: 0.62 to 0.97; P = .028). The lower and upper limits are predicted to be 0.36 and 1.68, respectively. The heterogeneity is high (I 2 = 61%; 95% CI: 36.4 to 76.6; P < .001) and τ 2 = 0.126. Trim and Fill Funnel plot shows that publication bias effect could not be excluded according to Egger test (P = .416). The adjusted Trim and Fill RR is 0.76 (95% CI: 0.46 to 1.23, P = .261; I2 = 0.0%). The sensitivity analysis shows the robustness of these findings in terms of point estimation, relative CI, and heterogeneity. The cumulative meta-analysis showed a significant timely tendency in favor of IA (Fig. 4A–C).
The estimated pooled mean difference of time to first flatus (hour) (12 studies, 1462 patients) is −16.68 (95% CI: −21.26 to −12.10; P < .001). The lower and upper limits are predicted to be −31.84 and −1.51, respectively. The heterogeneity is high (I 2 = 77.0%, 95% CI: 58.9 to 87.1; P < .001). The estimated time to first defecation (hour) (9 studies, 1636 patients) is −25.94 (95% CI: −32.68 to −19.19; P < .001). The lower and upper limits are predicted to be −46.02 and −5.85, respectively. The heterogeneity is high (I 2 = 72%, 95% CI: 41.3 to 86.2; P = .009). The estimated time to oral diet (hour) (7 studies, 615 patients) is −16.35 (95% CI: −24.05 to −8.65; P < .001). The lower and upper limits are predicted to be −36.64 and −3.94, respectively. The heterogeneity is moderate (I 2 = 59.3%, 95% CI: 6.4 to 82.3; P = .022). Similarly, the estimated HLOS (day) (20 studies, 3285 patients) is −0.72 (95% CI: −1.08 to −0.37; P < .001). The cumulative meta-analysis showed a significant timely trend in favor of IA for all these outcomes.
The abdominal incision length (mm) and the postoperative incisional hernia RR were significantly reduced for IA (md = −19.58, P < .001 and RR = 0.31, P < .001, respectively). No differences were found in term of operative time, conversion rate, postoperative bleeding, postoperative ileus, reoperation, 30-day readmission, and 30-day mortality (Table 2). The pooled analysis for postoperative pain (six studies) and time to first bed mobilization (one study) were not performed because of the heterogeneity in studies reporting and lack of data, respectively.
Summary of the Analysis of the Categorical and Continuous Outcomes Comparing Intracorporeal Anastomosis and Extracorporeal Anastomosis
CI, confidence interval; HLOS, hospital length of stay; I2, heterogeneity; md, mean difference; RR, risk ratio.
Discussion
This meta-analysis shows that the risk of postoperative infectious and overall complications were significantly reduced in patients who underwent LRH with IA, with no differences in term of anastomotic leak. Time to first flatus, time to first defecation, time to liquid diet, and HLOS were estimated to be lower in the IA compared with the EA group. A statistically significant time-shift timely trend in favor of IA was noticed for postoperative infectious complications, overall complications, and all recovery parameters.
Since its introduction in 1991, LRH has progressively gained worldwide acceptance and to date is considered by many the gold standard treatment for benign and malignant right colonic diseases.4,35 Intestinal continuity is restored via ileocolic IA or EA. IA is less performed because of the technical difficulties, the longer learning curve, and the need to perform laparoscopic sutures. By contrast, EA allows hand-sewn closure of the enterotomies but requires considerable mesial mobilization with intestinal exteriorization through an extended abdominal incision with a presumed higher risk of mesenteric twisting.6,36 Observational retrospective, prospective, and one randomized clinical trial interim analysis have been published comparing IA with EA in the setting of LRH.6–15,36–47 Five meta-analyses16–20 have been previously performed mainly focusing on short-term outcomes with controversial results generated by underpowered analysis and statistical methodological flaws. To overcome these limitations, two recent meta-analyses were published in 2017 by Ricci et al. and Milone et al., with a literature search ending up in 2016.48,49 Compared with these meta-analyses, we broadened the literature search until December 2018, including seven articles for a total of more than 1500 patients. We specifically focused on postoperative infectious complications and recovery parameters that were secondarily analyzed by Ricci et al. and not conclusive in the analysis by Milone et al. Finally, we performed a cumulative meta-analysis in an attempt to chronologically identify when a characteristic or statistically significant change first occurs. 50 This chronological combining allows to explore the consistency of results in consecutive experiments, thus indicating the point at which no further research is needed because results continually favor one treatment. Compared with traditional meta-analyses, cumulative meta-analysis allows to capture the tendency timely variation of the combined total effect, possibly facilitating new research.51–52
The pooled postoperative infectious complications RR was significantly lower in the IA group, with an estimated 50% reduction compared with EA (RR = 0.51; P = .009; I2 = 52%). This result was mainly driven by the significant reduction of wound infection (RR = 0.50; P = .004). It is expected that the extraction of the transverse colon, ileum, and enterotomies through an abdominal incision is presumably associated with higher tissue trauma and higher risk of nearby soft tissue contamination despite the presence of wound protector devices. By contrast, it has been postulated that the fashioning of an intracorporeal suture may increase the risk of intraperitoneal contamination because of the presumed high risk of intestinal content spillage. 19 However, no differences were found in terms of intra-abdominal abscess (RR = 1.04; P = .932). The preoperative mechanical bowel preparation, the use of laparoscopic bulldogs, and the pneumoperitoneum (higher than the intraluminal pressure) may explain this result. 46 Globally, an up to 22% reduction of overall complications was noticed in the IA group (RR = 0.78; P = .028; I2 = 61%).
The cumulative meta-analysis for infectious complications showed a timely tendency in favor of IA (Fig. 2B). When adding the 115 sample size study by Gil et al., 45 the result becomes statistically significant. It was observed that, as the number of cases increased, the test efficacy improved; the 95% CI gradually narrowed, reaching a significant final P value (P = .009). Similarly, the cumulative meta-analysis for overall complications showed a chronological progression toward significant results in favor of IA after adding the study by Martinek et al. 47 (P = .028) (Fig. 4B). The related heterogeneity for infectious and overall complication was moderate (52% and 61%, respectively). The meta-regression analysis showed a partial effect by the American Society of Anesthesiologists (ASA) score and longer operative time when considering infections and by age, BMI, ASA score, longer operative time, and previous abdominal surgery when considering overall complications. The surgical technique, the learning curve, surgical indication (benign versus malignant), the need to perform a complete mesocolic excision in malignant lesions, the presence of drainages, the surgeon experience, and the presence of unmeasured and unmeasurable covariates may further influence the related heterogeneity.
Laparoscopic suturing is considered one of the most difficult and time-consuming tasks in minimally invasive surgery because of the confined space and narrow visualization with a consequently supposed higher anastomotic leak rate.5,18 In this study, the overall anastomotic leak rate was 2.2% and the pooled results for anastomotic leakage were similar comparing IA and EA (RR = 0.64; P = .063). The related CI was narrow and the heterogeneity was 0.0%, making us confident that the result is robust. However, this should be interpreted cautiously because of the variability in the anastomotic technique, techniques for enterotomies closure (single-layer, dual-layer, interrupted sutures, barber sutures), and surgeon experience. Notably, the cumulative meta-analysis showed a temporary trend in favor of IA that does not reach statistical significance.
Finally, a significantly shorter time to first flatus (md = −16.68; P < .001), first defecation (md = −25.94; P < .001), and time to liquid diet (md = −16.35; P < .001) with a concomitant reduced HLOS (md = −0.72; P < .001) were estimated for IA. These results may be explained by the reduced manipulation and mobilization of transverse colon, mesocolon, and small bowel with consequent faster recovery, faster restoration of physiological bowel function, and consequent earlier re-introduction of oral diet and hospital discharge.19,37 The related heterogeneity was high in all outcomes. The meta-regression for time to first flatus was influenced by age, and previous abdominal surgery partially influenced the result. Similarly, the meta-regression for time to defecation was influenced by age, male gender, and previous abdominal surgery. Time to liquid diet was influenced by age and HLOS by age, BMI, ASA score, and previous abdominal surgery. These data should be interpreted with caution because of the extremely different postoperative management and institution protocols. Particularly, a fast track protocol was commonly reported for IA cohorts whereas it was rarely described for the EA groups. Finally, different health care systems and lack of predefined discharge criteria could further influence the baseline heterogeneity. No differences were found in terms of operative time, conversion rate, postoperative bleeding requiring transfusion, reoperation, 30-day hospital readmission, and 30-day mortality.
Our study presents the typical limitations of a meta-analysis with observational fair quality studies. The lack of inclusion criteria defined a priori, the lack of standardized surgical techniques, the lack of a globally defined postoperative management, and the interstudy heterogeneity in definition of outcomes represent principal limitations. However, the study was planned in agreement with PRISMA guidelines with an a priori methodology stated in the PROSPERO protocol. This included comprehensive outcome measures and independent evaluation of the quality of included studies. The selection criteria led to a homogenous population for some of the primary outcomes, as confirmed by low heterogeneity.
Conclusion
The IA in the setting of LRH seems to be associated with reduced postoperative infectious and overall complications. Similarly, time to first flatus, time to liquid diet, time to defecation, and overall HLOS seem to be reduced. A statistically significant timely trend favoring IA was found for postoperative infectious complications, overall complications, and all recovery parameters. Similarly, a timely trend favoring IA was noted for anastomotic leak. These data should be interpreted cautiously because of the presence of significant between-study heterogeneity. Additional studies are warranted to confirm these results and to further investigate the supposed timely tendency convergence in favor of IA.
Footnotes
Authors' Contributions
A.A., G.G., E.R., and D.B. did the literature search. A.A., D.B., and G.M. formed the study design. Data collection was done by A.A., G.G., E.R., and G.B.; A.A., G.B., and D.B. analyzed the data. A.A., D.B., G.C., and G.M. interpreted the data. A.A., G.G., and G.M. wrote the article. A.A., G.C., D.B., and G.M. critically reviewed the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.