
Abstract
Background:
To compare the endoscopic thyroidectomy (ET) with the open thyroidectomy (OT) for patients with papillary thyroid carcinomas and share our experience of central lymph nodes dissection and recurrent laryngeal nerve exposure.
Materials and Methods:
From January 2015 to July 2017, 197 patients were enrolled in our hospital. Among them, 85 underwent ET and 112 underwent OT. The mean age of the patients was 38.15 ± 11.72 years in ET group and 47.79 ± 10.51 years in OT group. Unilateral thyroidectomy was performed in 47 patients of ET group and 63 patients of OT group. Bilateral thyroidectomy was performed in 38 patients of ET group and 49 patients of OT group. Intraoperative information, including operation time, hemorrhage, tumor size, capsular invasion, central LN metastasis, number of retrieved lymph nodes, hospital stay, cost, postoperative complication, and cosmetic satisfaction, was compared between the two groups.
Results:
The operation time of ET group was significantly longer (P < .05). There were no significant differences between the two groups in postoperative complications (P > .05). The patients in ET group were more satisfied with the cosmetic effects (P < .05).
Conclusion:
ET was a safe and effective alternative operation method for selected patients with papillary thyroid carcinomas.
Introduction
Since the standardized procedure of thyroidectomy was reported by Billroth and Kocher, great efforts were made to develop a less invasive approach with the development of endoscopic thyroidectomy (ET) in the past decades. 1 In 1997, Huscher performed the first ET for a 30-year-old woman with a 4 mm benign hypoechogenic nodule in the right thyroid. 2 Since then, various minimal incisions for the endoscopic surgery were designed, of which the cervical, auxiliary, and breast incisions were the three main approaches. Recently, the breast combined with the oral approach was put forward in a preliminary research. 3
Initially, ET was considered to be only appropriate for benign thyroid diseases since it could not completely remove the malignant lesions. 4 With the accumulated clinical experience and advanced surgical skills, the indications of ET were expanded to the malignant ones. For its cosmetic advantages, more and more cases of endoscopic thyroidectomies for malignant thyroid diseases have been performed.
Although ET has been favorably reviewed, it has not been fully accepted and is still limited to some high-volume centers. As with any other surgical technique, efficacious ET performance requires adequate training in both open and endoscopic procedures. Therefore, in our hospital, we creatively introduced the ET in anterior chest approach in 2007 and treated 85 patients with papillary thyroid carcinomas last year. The main difficulty in the surgery was the dissection of central lymph nodes and the exposure of recurrent laryngeal nerves. In this study, we compared the endoscopic thyroidectomies with the open ones, and shared our experience of central lymph node dissection and recurrent laryngeal nerves exposure in ET for patients with papillary thyroid carcinoma.
Materials and Methods
Patients and study design
From January 2015 to July 2017, 197 patients with papillary thyroid carcinomas were enrolled in our hospital. All patients were preoperatively diagnosed with papillary thyroid carcinomas by ultrasonography or a fine-needle aspiration. Eighty-five of them underwent the endoscopic thyroidectomies (ETs), and the others were treated with open thyroidectomy (OT). They were therefore divided into ET group and OT group.
The postoperative pathology reconfirmed the initial diagnosis. The indications of ET for papillary thyroid carcinomas were as follows: tumor size not exceeding 2.0 cm and no evidence of lymph nodes metastasis (except VI zone) and local invasion in the preoperation assessment. Meanwhile, the exclusion criteria included unilateral thyroid cancer, thyroid volume >25 mL, thyroid nodule diameter >5 cm, tumor diameter >2 cm, invasion of neck adjacent tissues or distant metastases, a history of neck surgeries or radiation therapy, accompanied parathyroid diseases. All the surgeries were performed by 1 surgeon (Dr. Donglin Sun) and strictly carried out based on the patients' own decisions after giving informed consent concerning the surgical risks. All patients underwent the laryngoscopy to assess the vocal cord motility before and after the surgery. This study was approved by the ethical committee of The Third Affiliated Hospital of Soochow University.
The ET procedure
Patients under general anesthesia were placed in a supine position with the neck extended by a shoulder pillow. The incisions of the anterior chest approach for ET were different from the conventional ones. A 1.0 cm incision for the 10 mm trocar was made at the manubrium sterni. Two 0.5 cm incisions were made at the second rib of the left and right midclavicular line, respectively, for the other two 5 mm trocars. A diluted epinephrine solution (1: 500,000) was subcutaneously injected into the anterior chest and cervical skin (Fig. 1A). A 10 mm 30° laparoscope was then inserted into the 10 mm trocar. The flap extended by the ultrasound scalpel from the thyroid cartilage superiorly to 4 cm below the suprasternal fossa inferiorly and laterally from just beyond the medial border of the sternocleidomastoid muscle under euthyphoria. The operation space was maintained by low-pressure CO2 insufflation at 6 mmHg.

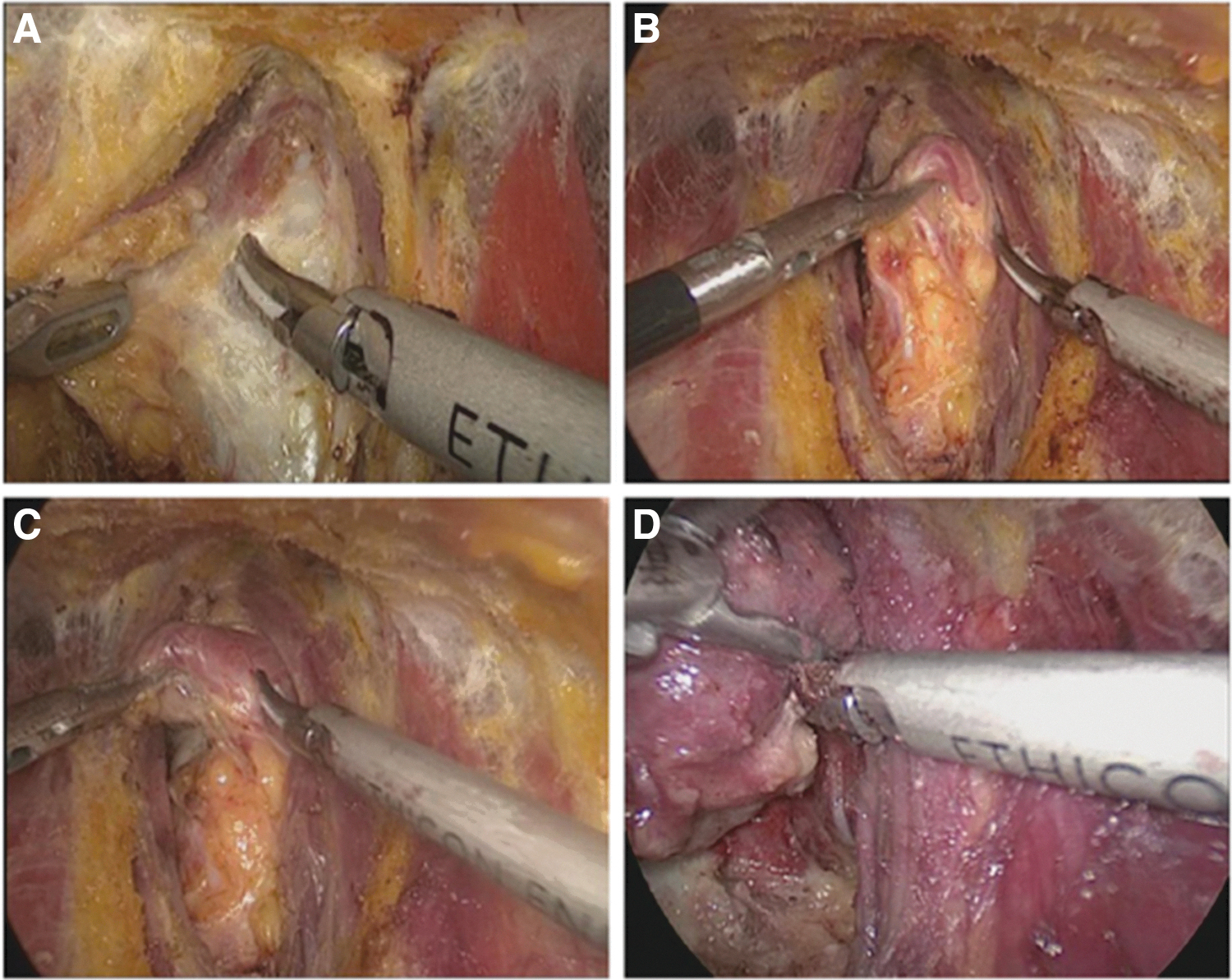
The midline of the strap muscles was identified and separated. Resection of the thyroid was initiated by dividing the isthmus from the trachea using a harmonic scalpel (Fig. 2A). Then, the inferior pole of the thyroid was carefully and meticulously dissected. The inferior thyroid vein and artery were dissected as close as possible to the surface of the gland (Fig. 2B). The main trunk of the inferior vessels was protected from compromising the blood supply to the parathyroid glands. When the inferior pole was freed, the thyroid was extracted to the inner superior pole with an assistant clamp. When the middle thyroid vein was clearly exposed and dissected off from the gland, the tracheoesophageal groove was disclosed (Fig. 2C). Generally, the recurrent laryngeal nerve was quite bright, which made it easier to be discriminated from the blood vessels. The recurrent laryngeal nerve could be partially exposed by the curved forceps (Fig. 2D).
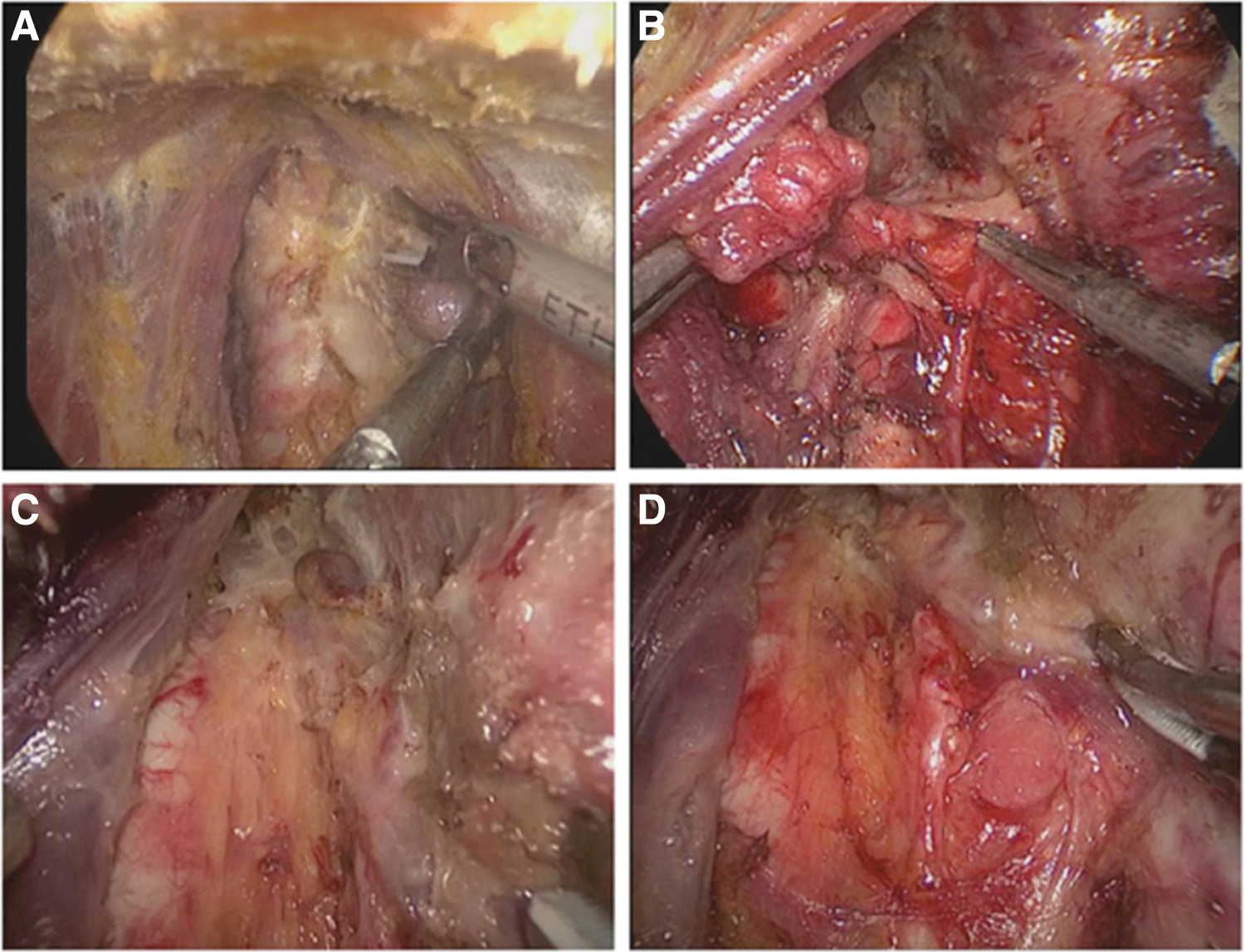
The entire gland was pulled downward, and Berry's ligament and upper pole of the thyroid were revealed and dissected (Fig. 3A). As the gland near the recurrent laryngeal nerve entering larynx was not separated, this procedure needed multiple combinations of front and back movements of the upper pole. Eventually, curved forceps were able to separate the point where the nerve entered the larynx near the inferior horn of thyroid cartilage (Fig. 3B). The specimen was placed into a bag and pulled out from the 10 mm trocar. The central lymph nodes were carefully dissected to prevent the parathyroid gland (Fig. 3C) and recurrent laryngeal nerve (Fig. 3D) from being injured. The strap muscles were sutured, and drainage tubes were placed into the operation field through the 5 mm trocars. Finally, all the incisions were sutured.
The OT procedure
Open total thyroidectomy was performed on patients in this group with central lymph node dissection in the supine position with neck extended under general endotracheal anesthesia. A 5–8 cm transverse collar skin incision was made 2 cm above the sternal notch, and the lower layer of the platysma was exposed. To achieve an adequate working space from the sternal notch to the hyoid bone superiorly, and both the medial side of the anterior border of the sternocleidomastoid muscle laterally, subplatysmal flap dissection was performed. The thyroid gland was exposed when the strap muscle was divided vertically. A total thyroidectomy was performed in the same manner as the endoscopic procedure. The central lymph nodes were then dissected, and laryngeal nerves were exposed. The incisions were sutured by the absorbable material in an interrupted cutis method.
Postoperative care
All the patients underwent the same postoperative care. Laryngoscopy was performed in all patients to check vocal cord motility. Recurrent laryngeal nerve palsy could lead to a hoarse voice, and permanent palsy was diagnosed as it did not recover within 12 months after surgery. Follow-up evaluation was obtained by outpatient consultation. Hypocalcemia, which could lead to a convulsion of the limbs, was defined as the serum level of calcium falling below 2.0 mmol/L. Patients with hypocalcemia were given a calcium supplementary therapy orally or intravenously even if they were asymptomatic.
Observation index
The clinical data of all the patients, including tumor size, operation time, number of retrieved lymph nodes (RLNs), postoperative complications, hospital stay, expenditure, and cosmetic satisfaction, were compared and analyzed to evaluate the effectiveness of and draw lessons from the surgery.
Statistical analysis
All statistical analysis was performed by using the Statistical Package for the Social Sciences (SPSS), version 20.0, for Windows (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp.). All the continuous variables were expressed as the mean ± standard deviation. The data were analyzed for statistical significance using Student's t-test and chi-square test, and P-values <.05 was considered significant.
Results
Basic characteristics
The clinical data of 197 patients of ET and OT groups are summarized in Table 1. The mean age of patients in the ET group was 38.15 ± 11.72 years (ranged from 18 to 64 years) and those in the OT group were 47.79 ± 10.51 years (ranged from 19 to 78 years) (P < .01). The female-to-male gender ratio was 84.71% in ET group (13 males and 72 females) and 66.07% in OT group (38 males and 74 females) (P = .003). Unilateral thyroidectomy was performed in 47 patients of ET group and 63 patients of OT group, whereas bilateral thyroidectomy was performed in 38 patients of ET group and 49 patients of OT group (P = .894).
Basic Characteristics of Patients in Endoscopic Thyroidectomy and Open Thyroidectomy Group
General information of the patients.
Values were given as mean ± SD. Patients with unilateral or bilateral lesions were treated with unilateral or bilateral thyroidectomy.
ET, endoscopic thyroidectomy; OT, open thyroidectomy; SD, standard deviation.
Comparison of the intraoperative information
The operation time of the ET group was obviously longer than that of the OT group (102.975 ± 15.289 versus 63.140 ± 9.579, P < .01). While, there were no significant differences of intraoperative hemorrhage (35.612 ± 5.834 mL versus 34.458 ± 6.267 mL, P = .189) and number of RLNs (6.125 ± 1.951 versus 5.693 ± 2.022, P = .133) between the two groups. The mean hospital stay of the two groups was not significantly different (3.325 ± 0.526 versus 3.228 ± 0.756, P = .313), while the expenditure of ET group was higher than that of OT group (11,658.950 ± 1960.323 versus 10,630 ± 533.374, P < .001) (Table 2).
Intraoperative Information of Endoscopic Thyroidectomy and Open Thyroidectomy Group
Intraoperative information.
Results were expressed as mean ± SD.
ET, endoscopic thyroidectomy; LN, lymph node; OT, open thyroidectomy; RLN, retrieved lymph node; RMB, Ren Min Bi; SD, standard deviation.
Comparison of postoperative complications
The postoperative complications including bleeding, hoarse voice, hypocalcemia, seroma, and incision infection were compared (Table 3). Postoperative bleeding occurred in only one case of OT group and led to a reoperation. There were no significant differences in hoarse voice (2 versus 3, P = .754), hypocalcemia (1 versus 3, P = .602), seroma (1 versus 0, P = .890), and incision infection (0 versus 2, P = .602) between the two groups. There were no cases of permanent recurrent laryngeal nerve palsy and hypocalcemia in both groups.
Postoperative Complication of the Endoscopic Thyroidectomy and Open Thyroidectomy Group
The postoperative complication.
ET, endoscopic thyroidectomy; OT, open thyroidectomy.
Comparison of cosmetic satisfaction
A simple questionnaire was used to evaluate and compare the cosmetic effect of the two surgeries (Table 4). Among the 85 responses in the ET group, 56.471% (48/85) were “Excellent,” 37.647% (32/85) were “Good,” 5.882% (5/85) were “Acceptable,” and there were no “Poor” responses. Among the 112 responses in the OT group, 10.714% (12/112) were “Excellent,” 22.321% (25/112) were “Good,” 59.821% (67/112) were “Acceptable,” and 7.143% (8/112) showed no “Poor” responses. Patients in the ET group had significantly better cosmetic satisfaction than those in the OT group (P < .05). The mean follow-up period of all the patients was 12.08 ± 3.06 months, and no tumor recurrence was observed.
Cosmetic Satisfaction of Endoscopic Thyroidectomy and Open Thyroidectomy Group
The cosmetic satisfaction.
ET, endoscopic thyroidectomy; OT, open thyroidectomy.
Discussion
In this study, we compared the ET with the OT for patients with papillary thyroid carcinoma. The operation time of ET was longer, but the postoperative complications were similar between the two surgery methods. The cosmetic effects of ET were better.
The incidence of malignant thyroid tumors has been significantly increased in the last 20 years in China. A large number of the cases were diagnosed by routine physical examinations. Papillary thyroid carcinomas occurred in more and more young patients with a female predominance. 5 Patients were not only focused on the surgical treatments but also on the recovery of the scar by the operation on the neck and the cosmetic effects, especially the young female ones. With the development of laparoscopic equipment and accumulated clinical experience, surgeons devoted to make less invasive approaches not only for benign thyroid tumors but also for malignant ones. 6
Conventionally, OT was considered as the first-line treatment for malignant thyroid tumors. 7 Then, the prospective study of ET for patients with papillary thyroid carcinomas was first done by Miccoli et al. 8 However, the application of ET for malignant thyroid tumors was still under controversy. Recently, some comparative studies of endoscopic and OT had been reported.6,7,9–11 Those studies revealed that there were no significant differences between open and ET in technical safety, but ET had many other advantages, including better cosmetic effects.9,10,12–15 In this study, the patients in ET group were younger than those in the OT group, and there were also more females in ET group compared with OT group. This might also be attributed to that young patients cared more about cosmetic effects of the incisions, especially the female ones, and were more likely to choose ET.
Some researchers made efforts to define the indications and contraindications of ET for malignant ones. Kitano et al. reported that the indications of endoscopy for malignant thyroid carcinomas were as follows: age <45 years, tumor size <2.0 cm, and no evidence of lymph node metastasis or local invasion. 16 Miccoli et al. showed that the prognosis of minimally invasive video-assisted thyroidectomy for malignant cancers not exceeding 3.5 cm in diameter was similar to that of OT.8,17
The dissection of central lymph nodes and the exposure of recurrent laryngeal nerves were the main difficulties during ET. However, research studies revealed that there were no significant differences in cervical lymph node dissection and postoperative recovery between endoscopic and OT.18–21 Jeong et al. reported that the average number of RLNs was 5.05 ± 2.94 (range 1–16) in ET, and found no statistical differences between ET and OT. 6 In our study, the number of RLNs was 6.125 ± 1.951 in ET group and 5.693 ± 2.022 in OT group. This result also suggested that ET could retrieve as many lymph nodes as OT.
The key of endoscopic total thyroidectomy for papillary thyroid carcinomas with central lymph node dissection was to prevent the recurrent laryngeal nerve and parathyroid glands from being injured. The incidence of transient recurrent laryngeal nerve palsy after OT was 0% to 6%, and the permanent palsy was <1%. 22 The incidence of transient hypocalcemia after OT was 7.3% and that of permanent hypocalcemia was 1.5%. 23 In our experience, the thyroid should be dissected as close as the thyroid capsule, and the recurrent laryngeal nerves, as well as the parathyroid glands, were easily discriminated due to the magnifying effects of the video lens.
There were five anatomical landmarks to help us recognize and expose recurrent laryngeal nerve. They were the inferior horn of thyroid cartilage, suspensory ligament, inferior thyroid artery, plexas thyreoidea inferior, and sulcus esophagus. The inferior horn and the suspensory ligament were the most reliable ones. Therefore, we separated and abscised the connective tissues with the curved forceps and ultrasonic scalpel along the tracheoesophageal groove slightly, especially near the inferior horn of thyroid cartilage. By the magnified endoscopic lens, the recurrent laryngeal nerve was a shining bright white streak laying in the groove that could be easily observed. In this way, we could easily preserve the recurrent laryngeal nerve and parathyroid gland.
To avoid the injuries of esophagus, the ultrasonic scalpel must be kept 0.5–1.0 cm away from the tracheoesophageal groove. In our study, 2 patients in ET group and 3 patients in OT group suffered from hoarse voice, which was caused by recurrent laryngeal nerve palsy and recovered 2–6 months later. This might be attributed to the thermal injuries of recurrent laryngeal nerve by ultrasonic scalpel. Dhiman and Inabnet 15 had also reported the disadvantages of ET for malignant thyroid diseases, including >2 assistants, the steeper learning curve, longer surgical time, inapplicable for thyroid glands >20.0 mL, and higher expenditure in hospital stay. In our study, only one assistant was needed to hold the video lens, while two were needed in OT. The expenditure of ET group was obviously higher than that of OT.
ET in anterior chest approach was first applied for benign tumors since 2007 and for malignant ones since 2010 in our hospital. In contrast to the breast areola and axillary approach, the anterior chest approach could reduce the area of free flap and shorten the distance between thyroid and operation incisions, which made it easier for central lymph nodes dissection. In the breast areola approach, the sternoclavicular joint was the blind angle for central lymph node dissection, while in the auxiliary approach only unilateral thyroid nodes could be resected.
In this study, the diagnosis of papillary thyroid carcinoma was relative. Therefore, there were no discordant cases in this study. However, when the discord happened, if the final diagnosis was still malignant tumor, the extent of resection was the same as the current surgery, but a different medical treatment should be given. If the final diagnosis was benign tumor, the extent of resection was already expanded, but the prognosis was still good in our experience with this kind operation. Finally, the different surgery methods would not affect the concordance of the diagnosis.
There were also some limitations in our study. The ET and OT were not performed in the totally same period. The ET was performed more recently, thus more experience with the OT may have led to shorter operation time and better outcomes. OT showed a trend of higher number of positive nodes and increased capsular invasion than the ET. However, the difference was not statistically significant. Therefore, it would not affect our results in this study, but further investigation was still needed. The information on tumor-node-metastasis (TNM) stage and follow-up was not evaluated. The sample size was relatively small, and this study was performed in one center. Further study with lager sample size and more strict design was needed. The short-term and long-term prognosis of this surgery method was also needed to be evaluated in a further study. The central lymph nodes were all dissected in our study, but the central lymph nodes were not always negative. However, we believe it is not necessary to routinely take the other lymph node stations although there might be still controversy on this choice. The final treatment for the patients with positive central lymph node would depend on the number of positive central lymph nodes and the postoperative thyrobolulin. Further study to evaluate the efficiency of the different treatments was needed.
Conclusion
In conclusion, ET for papillary thyroid carcinomas in anterior chest approach was as safe and effective as open surgery. Compared with open surgery, ET in the anterior chest approach could not only make the scars less invasive but also hide them below the collar. ET for patients with papillary thyroid carcinomas in anterior chest approach is an effective alternative for the open surgery in the future.
Footnotes
Authors' Contributions
Y.Y. is responsible for the integrity of the entire study, study concepts and design, definition of intellectual content, literature research, clinical studies, data acquisition and analysis, statistical analysis, article preparation and editing; D.S. is responsible for data acquisition; J.Y. is responsible for the literature research and data acquisition; J.C. is responsible for the data analysis and statistical analysis; Y.D. is responsible for clinical studies, article editing, and review.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the Jiangsu Province's 5th “Project 333” Training Fund Project (BRA2017118).