
Abstract
Introduction:
Minimally invasive techniques have been suggested to achieve enhanced recovery and improved outcome after pancreaticoduodenectomy (PD). This study describes our experience and a stepwise technical implementation of the laparoscopic pancreaticoduodenectomy (LPD) during early introduction in 2016.
Methods:
A team of three hepatopancreaticobiliary surgeons with extensive experience in open pancreaticoduodenectomy (OPD) and with advanced laparoscopic skills started a proctor-guided program with LPD. The first 20 carefully selected cases were prospectively reviewed and compared with a matched OPD cohort.
Results:
In 20 months, 20 minimally invasive PDs were performed. Reviewing the first 10 LPD cases, 7 patients (70%) had anastomosis-related complications, versus 16% in OPD (P = .001). After consulting an international LPD expert, the team switched to a hybrid technique consisting of LPD followed by open reconstruction through midline minilaparotomy (LPD-OR). In the following 10 cases of LPD-OR, no anastomosis-related complications did occur (P = .342 OPD versus LPD-OR).
Conclusion:
Safe introduction of new techniques in minimally invasive major abdominal surgery is imperative. Based on our single-center experience, LPD-OR may be safer in the earliest phase of the learning curve of minimally invasive PD, as part of a stepwise implementation toward the fully laparoscopic technique.
Introduction
Laparoscopic pancreaticoduodenectomy (LPD) or Whipple's procedure is rapidly gaining popularity. As an open procedure, pancreaticoduodenectomy (PD) is a technically demanding operation requiring outstanding skills and experiences. Centralization has probably been the most important factor in the reduction of perioperative mortality in the last three decades. In the Netherlands, pancreatic resections are currently restricted to centers with a yearly volume of >20 PDs. After the introduction of minimally invasive techniques in different areas of gastrointestinal surgery, pancreatic surgery has followed. The main goal of minimally invasive surgery is enhanced recovery. While this has been achieved for relatively simple procedures such as cholecystectomy and more complex procedures such as colorectal resections, enhanced recovery after minimally invasive PDs is not well established as yet.
After open pancreaticoduodenectomy (OPD), median hospital stay is 12 days. Prolonged hospital stay is almost always caused by complications. Complications will occur in 60% patients after PD with an in-hospital mortality of ∼4%. 1 In an effort to reduce hospital stay and improve outcomes after pancreatic surgery, the laparoscopic technique has been introduced. In 1994, the first LPD was reported. 2
Introduction of major laparoscopic surgical procedures has come at a price: the extended learning curve. The transition takes time, and is dependent on the complexity of the procedure and the existing laparoscopic skills of the surgeon. Furthermore, laparoscopy comes with new challenges due to different sealing and suture techniques and limitations to exposure and overview of the surgical field. Ideally, the introduction of a new surgical technique will immediately give better results for the patient. Unfortunately, this is not realistic for any laparoscopic procedure. While in the past the introduction of new laparoscopic procedures was not guided by structured training and proctoring programs, 3 this has recently been realized in the Netherlands with the Longitudinal Assessment and Realization of Laparoscopic Pancreatic Surgery in the Netherlands (LAELAPS) program for laparoscopic pancreatic surgery 4 and LAELIVE for laparoscopic major liver resection. 5
In 2014, we introduced laparoscopic distal pancreatectomy in our hospital with a proctor-guided program (LAELAPS 1). In this study, we describe the difficulties and pitfalls of the introduction of minimally invasive PD in 2016 (LAELAPS 26).
Methods
Pancreatic surgery
Isala is a nonuniversity teaching hospital and a tertiary referral center for hepatopancreaticobiliary (HPB) disorders. The HPB unit with three consultant HPB-surgeons is responsible for pancreatic surgery (2017; 60 pancreatic resections), complex biliary surgery (advanced laparoscopic cholecystectomy, laparoscopic common bile duct [CBD] exploration, bile duct injury repair), and liver surgery (2017; 82 resections of which 30% laparoscopic). The yearly volume of pancreatic surgery has increased over the years due to regional collaboration with Gelre Hospital Apeldoorn (start March 2016), see Figure 1.
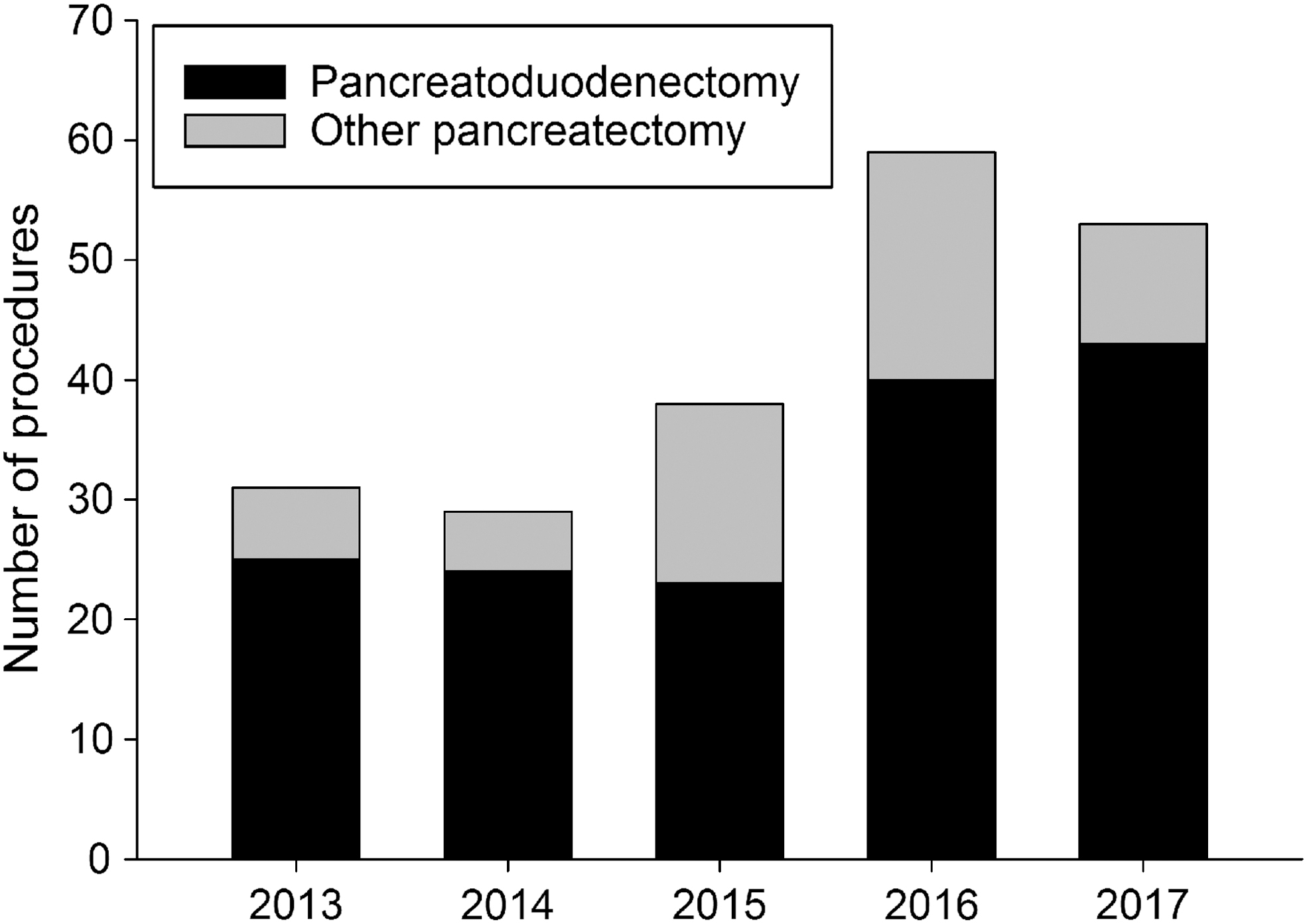
Yearly volume of pancreas resection in Isala clinics.
All surgeons had specialized HPB fellowship training after their surgical training. Each surgeon performed >100 OPDs, and laparoscopic skills were widely present (each surgeon >500 advanced laparoscopic procedures). According to the national LEALAPS 2 training program, training sessions of live LPD were followed, videos were studied, and perioperative and surgical protocols were devised. Also, the entire operative team received training before the program was started, and the first five laparoscopic PDs were supervised by an experienced proctor in the OR.
Patient selection
For laparoscopic resections only patients without vascular involvement of the tumor and without signs of pancreatitis were selected. A displaced right hepatic artery from the superior mesenteric artery was a contraindication for LPD, as well as a body mass index (BMI) >35. Minor previous abdominal operations such as appendectomy and cholecystectomy were no contraindications.
Patients were informed that the surgeons were in the early learning curve of the laparoscopic PD program, and patients informed gave consent in the outpatient clinic after counseling with oral and written information.
Surgical techniques
All surgeons employed the same technique for OPD and for laparoscopic PD. PD was done in a routine manner with lymphadenectomy (stations 8; 12; 14; and 16a). The techniques used are described below.
OPD was done through a bilateral subcostal incision. The pancreas was divided with a knife, and hemostasis was achieved with prolene 5-0 stitches. The 3 and 9 o'clock arteries of the hepatic duct were oversewn with prolene 5-0. A Billroth-II reconstruction with a dunking, end-to-side pancreaticojejunostomy was created at the beginning of the jejunal limb (running prolene 3-0) followed by an end-to-side hepaticojejunostomy (running PDS 4-0 for ducts >8 mm; interrupted PDS 5-0 for ducts ≤8 mm) and an end-to-side duodenojejunostomy (running PDS 3-0) in case of a pylorus-preserving technique or a side-to-side gastrojejunostomy (running PDS 3-0) for a classic Whipple's resection. All staple lines were oversewn with PDS 4-0. Portal and superior mesenteric vein branches as well as the gastroduodenal artery and inferior pancreaticoduodenal artery stumps were clipped and oversewn with prolene 4-0. Routinely, two silicon drains were left behind: one behind the hepaticojejunostomy and the other behind the pancreaticojejunostomy.
A fully LPD was initially chosen using a six-port access (12 mm umbilical, 12 mm left and right para-umbilical, 5 mm left and right subcostal, 5 mm subxyphoidal) and a small Pfannenstiehl incision for specimen extraction. Ligasure™ (Medtronic) was used for dissection and vessel sealing. Monopolar and bipolar cautery was used for additional hemostasis. The gastroduodenal artery was divided with double clips (Hem-o-Lok®, Teleflex). The pancreas was divided with monopolar diathermy; the pancreatic duct was divided with scissors. The first jejunal limb was dissected with a stapling device (Echelon flex™). After dissection of the uncinate process, the gallbladder was taken down from the liver together with station 12, and the CBD was transected with scissors. The 3–and 9 o'clock arteries were sealed with bipolar diathermy. The specimens were placed in an extraction bag for removal through a Pfannenstiehl incision.
After a 30 minute break, the primary and assisting surgeon switched, and the anastomoses were created. A Billroth-II reconstruction was used in all cases. First, hepaticojejunostomy was performed with a running PDS 4-0 for bile ducts >8 mm and with interrupted PDS 5-0 for bile ducts ≤8 mm. Second, pancreaticojejunostomy was performed with a dunking technique similar to the open technique using V-Loc™ 3-0 sutures (Medtronic). Finally, a stapled side-to-side gastroenterostomy was created with Echelon flex, the remaining defect was closed with V-Loc 3-0. Two silicon intra-abdominal drains were left behind identical to the open technique.
After 10 LPD cases, we evaluated the results and discussed these with an international expert. We decided to switch to a hybrid technique with an LPD and open reconstruction (LPD-OR) through a small (7 cm) upper midline incision. The last 10 cases were done using the LPD-OR technique. The resection phase was identical to the LPD, and the reconstruction phase was identical to the OPD.
Data collection
Since 2014, all pancreatic resections have been prospectively registered in the pancreas database. All data were retrieved from this database, and case records were reviewed retrospectively where necessary.
We reviewed the first 20 minimally invasive cases (10 LPDs and 10 LPD-OR) and compared them with OPD cases from 2014 to 2016 matched to no vascular involvement and a BMI <35 (n = 68). The primary outcome was all anastomosis-related morbidity (grade B/C postoperative pancreatic fistula 7 ; bleeding from the pancreatic transection plane; bile leak; stenosis of the hepaticojejunostomy; leakage or bleeding from the gastrojejunostomy). Secondary outcomes were mortality, hospital stay, and other morbidity such as delayed gastric emptying, chylous leakage, infectious complications, and cardiopulmonary complications.
Statistical analysis
Descriptive statistics are used to show the outcomes in the different groups. Since this study was not designed as comparative study between different techniques, we elected to limit the statistical comparisons to the primary outcome: anastomosis-related complications. This was analyzed with an intention-to-treat analysis; chi-square tests were used with Fisher's exact test to detect differences between groups. A two-sided significance level of P < .05 was chosen.
Results
In a period of 20 months, we performed 20 minimally invasive PDs. In Table 1, the patient characteristics are summarized. After reviewing the first 10 LPD cases, we observed a high number of anastomosis-related complications, concerning four times the pancreaticojejunostomy, four times the hepaticojejunostomy, and two times the gastrojejunostomy. We discussed our results with an international LPD expert and decided to change from a full laparoscopic approach to a hybrid approach in which the anastomoses were done through a small midline laparotomy (LPD-OR), with the exception of one case where the hepaticojejunostomy was created laparoscopically for reason of a far lateral position of the hepatic duct after resection.
Patient Characteristics in Open and Minimally Invasive Pancreaticoduodenectomy
ASA, American Society of Anesthesiologists Classification; BMI, body mass index; IPMN, intraductal papillary mucinous neoplasm; OPD, open pancreaticoduodenectomy; LPD, laparoscopic pancreaticoduodenectomy; LPD-OR, laparoscopic pancreaticoduodenectomy with open reconstruction; PPPD, pylorus-preserving pancreaticoduodenectomy.
In the first 10 patients, a full laparoscopic approach was attempted (LPD group), 2 patients were converted in an early stage, one for pancreatitis and one for poor exposure due to intra-abdominal fat. In the LPD-OR group, one procedure was converted in a late phase due to ingrowth of the tumor in the portal vein for which a wedge resection of the portal vein was done through a bilateral subcostal incision. The primary endpoint (anastomosis-related complications) was reached in 7 of 10 LPD patients, in the LPD-OR no anastomosis-related complications occurred (P = .003). In the OPD group, 16% had anastomosis-related complications (P = .001 OPD versus LPD; P = .342 OPD versus LPD-OR).
Table 2 describes the postoperative results. There was one mortality in the LPD group: bleeding from the gastrojejunostomy followed by myocardial infarction (confirmed by postmortal examination). One patient died after OPD due to pulmonary complications. The median hospital stay was 13, 16, and 9 days in the OPD, LPD, and LPD-OR groups, respectively.
Postoperative Characteristics in Open and Minimally Invasive Pancreaticoduodenectomy
Chi-square test (Fisher's exact test): LPD versus OPD P = .001.
Chi-square test (Fisher's exact test): LPD-OR versus LPD P = .003; LPD-OR versus OPD P = .342.
LPD, laparoscopic pancreaticoduodenectomy; LPD-OR, laparoscopic pancreaticoduodenectomy with open reconstruction; OPD, open pancreaticoduodenectomy.
Discussion
LPD is one of the last major minimally invasive operations to be introduced to routine clinical practice. There are several reasons for the reluctance to do a PD laparoscopically. The main reason is the technical difficulty during the resection and the reconstruction phase. For the resection phase, laparoscopy may offer some technical advantage. With the help of the camera magnification, a more detailed vision of the operative field can be achieved. However, management of major bleeding can be challenging during laparoscopy. Before starting a laparoscopic PD program, the surgeons need to have considerable experience in controlling major bleeding. This was in our unit the case since all three surgeons had done large numbers of advanced laparoscopic procedures. Especially laparoscopic distal pancreatectomy is a useful operation to gain experience in management of major venous and arterial bleeding. Two years before the start of the laparoscopic PD program, we adopted the laparoscopic distal pancreatectomy.
Besides management of bleeding, exposure can be difficult during laparoscopic PD. Especially the area of the uncinate process close to the superior mesenteric vein can be difficult to visualize. This can be overcome by using the right paraumbilical trocar as optical port. Dissecting techniques are quite similar to the OPD. Based on our result, we experienced most problems with the anastomosis. Compared with an OPD, the resection phase of LPD is quite similar. The reconstruction phase however is quite different. We tried to use the same anastomosis technique as in OPD. However, the finesse in making complex biliary and pancreatic anastomosis obtained with years of experience with OPD is not directly derived in LPD. For instance, pancreatic transection was performed by diathermy in LPD instead of by knife and sutures, overview of the anastomosis is less in LPD, and a different suture was used for the pancreatic anastomosis (prolene versus V-Loc).
Too many alterations may be one of the reasons for a relatively high number of anastomotic complications in our first 10 LPD patients. When switching to the hybrid technique, we could rely on the more routine open reconstruction techniques, and the number of anastomotic complications decreased to zero in the next 10 patients. This led to the consideration that the LPD-OR might be a safer alternative in the early learning curve phase, compared with the fully laparoscopic approach.
An alternative explanation for the observed increased rate of anastomosis-related complications may be due to selection of patients with smaller tumors with mostly soft pancreatic parenchyma, which is known to be prone to pancreatic fistula complications.
In the literature, several studies describe positive and negative aspects of LPD, but there is a lack of high-quality, prospective, and/or randomized trials. Best evidence suggests that minimally invasive PD has comparative outcome compared with OPD. 8 Nevertheless, there have been several studies that reported problems with the introduction of LPD, such as longer operative time, higher morbidity, and higher mortality compared with OPD.9–11 Van Hilst et al. presented the results of a Dutch randomized controlled trial, which was early terminated because of high mortality in the LPD group, 12 although this was mainly caused by complication related to the resection phase and was not anastomosis related.
When introducing minimally invasive techniques in colorectal surgery, lessons have been learned. Especially the learning curve might have been underestimated. 13 For minimally invasive pancreatic surgery, several studies suggest that the complete learning curve should cover ∼30 LPD procedures for each individual surgeon.14,15 Furthermore, structured training programs seem to be indispensable in the introduction of LPD. 16
Minimally invasive techniques were combined with open techniques to help enhance the learning curve. 17 A hybrid technique has previously been described as stepwise implementation strategy toward a fully laparoscopic approach, and has been valuable in efficiently and safely implementing LPD.10,18 Although LPD-OR might eventually have no advantage over LPD, 19 LPD-OR is likely to have the advantages of a more minimally invasive surgery compared with OPD.20–22 Of note, this study is not a comparison of different surgical techniques, and the numbers are too low, within the learning curve, to draw conclusions. However, this report shares our experience with difficulties and strategies during the introduction of a minimally invasive PD. To achieve a safe introduction, LPD-OR might be valuable as stepwise implementation strategy in the early learning curve.
To date, convincing evidence of LPD being superior to OPD is lacking. Complications, including pancreatic fistula, other anastomotic complications, delayed gastric emptying, or chylous leakage, largely determine morbidity and length of stay instead of larger incisional wounds. Perhaps robot-assisted PD may eventually be able to reduce post-PD morbidity and induce enhanced recovery, and might have several technical advantages over OPD and LPD (Table 3). Evidence suggests that robot-assisted PD is a more promising minimally invasive strategy, rather than LPD, and might in fact become superior to OPD. 23
Drawbacks of Different Approaches of Minimally Invasive Pancreaticoduodenectomy
+ = drawback present; − = drawback not present.
LPD, laparoscopic pancreaticoduodenectomy; LPD-OR, laparoscopic pancreaticoduodenectomy with open reconstruction; RAPD, robot-assisted pancreaticoduodenectomy.
Conclusions
Anastomosis-related complications were frequently seen in the early phase after the introduction of LPD. The hybrid approach LPD-OR may be safer in the earliest phase of the learning curve of minimally invasive PD.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.