
Abstract
Background:
Safety and effectiveness of absorbable meshes for laparoscopic hiatus hernia repair are still debated. This may be due to patient selection, technique of repair, type and shape of mesh, definition of recurrent hernia, and length of follow-up. The aim of this study was to assess safety, short-term efficacy, and quality of life after laparoscopic repair of hiatal hernia reinforced with a biosynthetic absorbable mesh.
Materials and Methods:
A single-center observational cohort study was conducted in patients with large type III-IV hiatal hernia who underwent laparoscopic crural repair reinforced with Phasix ST®, a monofilament resorbable mesh (poly-4-hydroxybuterate) with a hydrogel barrier on one side. Patient data were extracted from hospital charts and a prospectively updated research database. Both generic Short Form-36 (SF-36) and disease-specific (Gastro-Esophageal Reflux Disease Health-Related Quality of Life [GERD-HRQL]) questionnaires were used to assess preoperative and postoperative quality of life.
Results:
From January 2017 to July 2019, 73 consecutive patients were implanted with Phasix ST mesh. The median follow-up was 17 (interquartile range 9–24) months. Recurrent hernia was found in 2 of 62 (3.2%) patients followed for more than 6 months after surgery, but none required reoperation. The overall postoperative morbidity rate was 8.2%. No mesh-related complications occurred. Compared to baseline, there was a statistically significant improvement of all items of the SF-36 questionnaire (P < .001) and of the median GERD-HRQL score (P < .001).
Conclusion:
The use of Phasix ST mesh to reinforce crural repair for large hiatus hernias is safe, is effective in the short-term follow-up, and is associated to improved quality of life.
Introduction
Laparoscopic repair is currently the surgical standard of care for patients with large type III-IV hiatal hernia. The high recurrence rate after simple suture of the crura in this patient population has led to the use of permanent or absorbable meshes to reinforce the hiatus to improve durability of the repair.1–4 Permanent mesh is durable, but is associated to the risk of erosion within 2 years from the implant, especially in patients with recurrent hiatal hernia. 5 Conversely, several studies have shown that absorbable mesh augmentation can protect from early anatomical recurrence and can decrease the risk of reoperation,6,7 but the long-term effectiveness has not been demonstrated yet. Therefore, the search for an ideal absorbable mesh that would enable to improve the strength of hiatal crura repair, reduce recurrences, and minimize complications is still ongoing. The aim of this study was to assess safety, short-term efficacy, and quality of life after laparoscopic repair of hiatal hernia reinforced with a biosynthetic absorbable mesh (Phasix ST®, C.R. Bard, Inc.,/Davol, Inc., Warwick, RI).
Methods
Study design
A single-center observational cohort study was conducted in patients with large hiatal hernia, who underwent laparoscopic crural repair reinforced with Phasix ST mesh and Toupet fundoplication. The study was approved by the Internal Review Board (protocol no. 2742, 2019), and written informed consent was obtained from all patients. Demographic and clinical patient data were extracted from hospital charts and a prospectively updated research database. Only patients with large (≥5 cm) type III and IV hiatal hernia, who had elective laparoscopic repair and no previous esophageal/gastric surgery, were included in the study.
All patients underwent a standard preoperative assessment, including medical history, physical examination, blood test analysis, electrocardiogram, chest X-ray, barium/gastrografin swallow study, and upper gastrointestinal endoscopy with biopsies. Esophageal manometry, 24-hour esophageal pH/impedance test, CT scan of chest and abdomen, cardiac magnetic resonance, and/or cardiopulmonary exercise test were performed in selected patients.
After surgery, patients were followed up with office visits at 1, 6, and 12 months, and then every year. Between 6 and 24 months after operation, an upper gastrointestinal endoscopy and/or barium/gastrografin swallow study was performed. Both the Short Form-36 (SF-36) and the Gastro-Esophageal Reflux Disease Health-Related Quality of Life (GERD-HRQL) questionnaires, 8 were administered preoperatively and at 6/12 months, and then yearly. Recurrent hernia was defined as the maximal length of stomach >2 cm above the diaphragmatic impression at endoscopy and/or barium swallow study.
Surgical technique
The patient was placed in a reverse Trendelenburg Lloyd Davies position with the first surgeon standing between the patient's legs. Five trocars were used for the laparoscopic approach. After extensive mediastinal dissection with reduction of herniated organs and excision of the hernia sac, the pneumoperitoneum was set at 8 mmHg and a posterior cruroplasty was performed with interrupted, nonabsorbable prolene sutures. In patients with large oval-type hiatal defects, additional sutures were placed to approximate the left crus to the central tendon of diaphragm. A 7 × 10 cm piece of monofilament resorbable mesh made of poly-4-hydroxybutyrate with a hydrogel barrier on one side (Phasix ST) was shaped with “U” configuration, marked with metal clips at the corners, and fixed over the approximated hiatus surface with three interrupted absorbable sutures. Finally, after division of the upper short gastric vessels with harmonic scalpel, a 270° Toupet fundoplication was performed. At the end of the procedure, a J-Vac mediastinal drain was left in place for 24 hours.
Postoperative care
The nasogastric tube was routinely removed at the end of the operation. To prevent postoperative nausea and vomiting, intravenous Ondansetron 4 mg and Dexamethasone 8 mg were administered. All patients had a chest X-ray and gastrografin swallow study on the first postoperative day to check for the correct placement of the mesh and the position of the gastroesophageal junction. Patients were then allowed a soft diet and were discharged home usually on postoperative day 2.
Statistical analysis
Continuous data are reported as mean ± standard deviation or median and interquartile range (IQR), as appropriate. Categorical data are reported using frequencies and proportions. Wilcoxon signed rank for paired data was performed as appropriate. Two-sided P values were computed. Statistical significance was considered when P value was equal or less than .05. All analysis was performed with IBM SPSS® Statistics (IBM Corp. Released 2017. Version 25.0. Armonk, NY: IBM Corp.).
Results
From January 2017 to July 2019, 73 consecutive patients underwent primary augmented laparoscopic crural repair with Phasix ST™ mesh and Toupet fundoplication for large hiatal hernia. The demographic and clinical characteristics of the patient population are shown in Table 1.
Demographic and Clinical Characteristics of the Patient Population (n = 73)
IQR, interquartile range; PPI, proton pump inhibitor; SD, standard deviation.
All operations were completed laparoscopically. The mean duration of surgery was 165 minutes (±68.9). The posterior cruroplasty was performed with a median number of 4 (IQR 3–5) stitches, and additional stitches to approximate the left crus and the central tendon were required in 38 (52%) patients. No intraoperative complications occurred. At postoperative radiologic examination, the mesh appeared in the subdiaphragmatic position in all patients. The median length of hospital stay was 3 (IQR 2–4) days. The overall postoperative morbidity was 8.2% (4 patients with transient gastric dilatation, 1 with pneumonia, and 1 with pneumothorax). The median follow-up was 17 (IQR 9–24) months. No mesh-related complications occurred.
Upper gastrointestinal endoscopy and/or barium/gastrografin swallow study were performed in 59/63 (93.6%) patients followed for at least 6 months after surgery, and a recurrent hiatal hernia was found in 2 of 63 patients (3.2%) at 12 and 16 months after surgery, respectively. None of the patients required reoperation for symptomatic hernia recurrence. Compared to baseline, there was a statistically significant improvement of all domains of the SF-36 questionnaire (P < .001) (Fig. 1 and Table 2) and a statistically significant reduction of the GERD-HRQL score (P < .001) (Fig. 2).

Radar plot showing Short Form-36 domain scores (black line = baseline and red line = postoperative follow-up). BP, bodily pain; GH, general health; MH, mental health; PF, physical function; RE, role emotional; RP, role physical; SF, social function; VT, vitality.
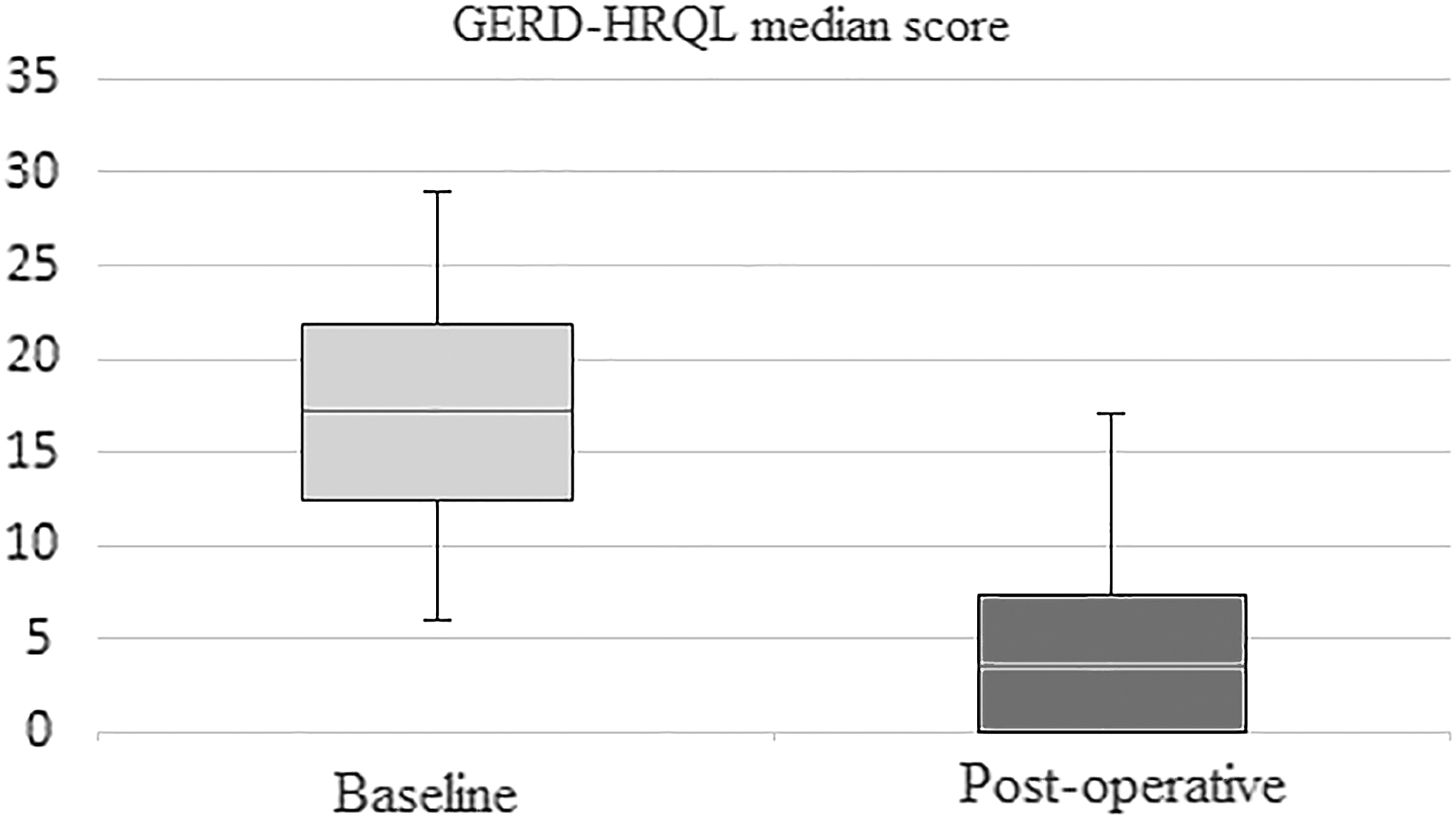
Box plot showing gastroesophageal reflux disease-health-related quality-of-life scores before and after mesh-augmented hiatal hernia repair (P < .001). GERD-HRQL, Gastro-Esophageal Reflux Disease Health-Related Quality of Life.
Baseline and Postoperative Results of the Short Form-36 Questionnaire
SF-36, Short Form-36.
Discussion
This study shows that the Phasix ST mesh is safe and effective over a short-term follow-up and may represent a useful adjunct to laparoscopic repair of large hiatal hernia. Laparoscopic repair with mesh-reinforced cruroplasty has become an increasingly common surgical approach in patients with large hiatal hernia. A recent systematic review and meta-analysis showed that the use of mesh is associated with a reduced recurrence rate compared to suture repair over a short- to middle-term follow-up, with a nearly 50% drop in odds of recurrence rates. 9 A recent European survey reported that two-third of the surgeons use mesh for crural repair, and that a separate pooled analysis of synthetic and biological meshes found a significant reduction of the recurrence rate in the nonabsorbable group; however, this was attributed to the type of biological mesh used, that is, porcine intestinal submucosa. 10 In fact, the results of Oelschlager's initial trial 6 with the use of a biological mesh (porcine intestinal submucosa) were not confirmed at the 5-year follow-up and no significant difference between mesh-augmented repair and suture cruroplasty was recorded (54% versus 59%, respectively). 11
In this study, which only included large hiatal hernias, the recurrence rate was 3.2% at a median follow-up of 17 months. Most recurrences of hiatal hernia occur during the first year of follow-up.12,13 In a previous comparative study from our group, crura repair with a polyglycolic acid/trimethylene carbonate mesh decreased the failure rate at 12 months, and there was no need for reoperation. 12 The Phasix ST mesh has a full reabsorption time of 12–18 months, compared to 6–12 months of Surgisis and 12 months of Bio-A, and therefore preserves its mechanical strength for a longer period of time. 14 Abdelmoaty et al. 15 reviewed their series of 50 patients implanted with a Phasix-ST mesh. No mesh-related complications such as infection and erosion occurred, and the objective recurrence rate at a median follow-up of 12 months was 8%.
We have previously reported that quality of life is significantly improved after mesh-augmented laparoscopic repair of large hiatus hernia. 16 In a meta-analysis, improvement of quality of life assessed by SF-36 and GERD-HRQL after biological mesh-reinforced cruroplasty was significantly greater compared to primary suture repair (mean differences = 13.68, 95% confidence interval = 2.51–24.85, P = .02). 17 Also, a multicenter prospective clinical trial investigating the use of a hepatic derived porcine mesh for crura augmentation showed significant quality-of-life improvement up to 24-month follow-up. 18 Overall, these data indicate that a biosynthetic mesh may represent a safer option compared to permanent mesh because the risk of dealing with a recurrent hernia is less than the risk of resecting the esophago-gastric junction.
This is the first large study including more than 70 patients undergoing primary laparoscopic large hiatal hernia repair with Phasix ST mesh. Main study limitations are the observational retrospective study design and the short length of follow-up.
Conclusion
This study shows that the Phasix ST mesh to reinforce cruroplasty during laparoscopic hiatal hernia repair is safe and effective in the short-term follow-up in patients with large hiatal hernia and is associated with a significant improvement of generic and disease-specific quality of life. None of our patients required reoperation for symptomatic hernia recurrence. Long-term follow-up studies and, ideally, a randomized clinical trial would be necessary to confirm the long-term effectiveness of crura augmentation with Phasix ST mesh.
Authors' Contributions
T.P.T., A.C.S., E.A., and L.B. designed the research study. T.P.T. and A.C.S. collected the data. T.P.T. and L.B. analyzed the data and wrote the article. All authors reviewed the final version of the article.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by AIRES (Associazione Italiana Ricerca ESofago).