
Abstract
Introduction:
Training in laparoscopic surgery seems to be an important aspect in gaining and maintaining professional competency. In experimental settings, camera navigation skills improved after simulation-based training, but the effect of camera work on the surgeon's performance is not well studied. The aim of this study was to investigate whether a fixed camera or an operated camera, as well as the experience of the camera operator has an effect on the performance of the surgeon.
Materials and Methods:
The study was performed on the LapSim laparoscopic training system. The task was to tie an intracorporal knot in a static surgical environment with three different camera conditions: fixed camera, camera operated by an inexperienced person (inexpert camera), and camera operated by an experienced surgeon (expert camera). The camera conditions were counterbalanced across trials. Performance variables were completion time in seconds and the extend of movements in path length and angular pathway. Gaze behavior was measured with eye-tracking glasses worn by the surgeon as well as the camera operator and was evaluated for performance-harming effects.
Results:
Completion time varied across conditions, with participants performing significantly longer in the fixed camera condition than in the expert or the inexpert condition. The expert and inexpert conditions did not differ. The performance-harming effect of non-focusing on the tissue was especially visible in the fixed camera condition but disappeared in the expert camera condition. Neither the camera operators' gaze behavior nor the surgeon–camera operator fixation agreement predicted task performance.
Discussion:
A camera operator can potentially eliminate performance-harming effects of maladaptive gaze behavior and promote optimal visual behavior of a surgeon. In our experimental task, there was no significant difference in whether the camera operator had previous training in laparoscopic surgery or not.
Introduction
Training and simulation is gaining traction as a means of training and maintaining competency in surgical procedures. 1 Simulation-based training seems to be valuable for every surgical discipline where skills are important to improve patient safety, minimize learning time to achieve professional competency, and increase surgical efficiency without endangering patients.2,3 There is a growing number of surgical training models in pediatric surgery, but a lack of randomized validation studies for them.3,4 A recent simulation study with medical students showed that camera work improved after participating in a laparoscopic course. 5 Another study with a box-trainer simulation model showed a significant decrease in the number of movements and errors when experts conducted the camera in laparoscopy. 6 On the other hand, it has also been demonstrated that camera navigation skills improved after simulation-based training with no clear benefit in the operating room. 7 Futuristic approaches and the development of robotic camera assistance shows promising results and benefits but will probably need time to be incorporated into the daily routine in laparoscopic surgery.8,9
The camera work in laparoscopic surgery is verbally transmitted to the assistant who is in charge of executing the desired movement and following the surgeon's movements. This requires previous knowledge of the procedure to predict the surgeon's movements and being able to follow with little guidance. 10
Eye-tracking glasses were used in previous medical fields to assess the attention of health care providers and they were also used in assessing the gaze behavior during surgery in open inguinal hernia repair.11,12
In our pilot study, we aimed at assessing eye movements, camera work, and the performance of experienced pediatric surgeons in a static- and a dynamic camera simulated task setting and also at evaluating the gaze behavior of inexperienced and experienced camera operators in comparison to the operating surgeon. The aim was to find out whether a fixed camera or dynamic camera control and the experience of the operator had an effect on the performance of the surgeon in predefined laparoscopic tasks.
Materials and Methods
We used a laparoscopic simulator, the LapSim training system (Surgical Science, Goeteborg, Sweden) for our experiment. The designated task was to tie an intracorporal knot with a needle holder and an assistant needle holder in a static surgical environment. We measured the completion time in seconds (time), the path length (path) in movements, and the angular pathway (angle). Longer completion time, longer path length, and longer angular pathway represented worse performance.
Three pediatric surgeons with experience in minimally invasive surgery participated in this trial. On a rotating basis, each surgeon completed four practice trials to familiarize themselves with the simulator and study protocol. Then, each of them followed 12 procedures: In four trials, the camera was operated by an experienced person (expert condition); in another four trials, the camera was operated by an inexperienced person (inexpert condition); and in four trials, we used a fixed camera setting without any camera movement (fixed camera condition). The camera conditions were counterbalanced across procedures. The expert camera operators were the participating surgeons, the inexpert camera operators were two male research fellows who were inexperienced in surgery and camera work, and the fixed camera condition was a standard option provided by the LapSim (Surgical Science) software. The intraoperative camera movements were verbally guided by the operating surgeon.
Surgeons' and camera operators' gaze behaviors were measured simultaneously with two Tobii Pro 2.0 eye tracking glasses (Tobii Pro, Stockholm, Sweden). Eye movements were sampled at a rate of 50 Hz. The recording produced a first-person video with an overlying pupil fixation showing where the surgeon and the camera operator were looking in real time. The data were then uploaded to a secured study computer and analyzed with the Tobii Pro Glasses Analyzer software (Tobii Pro, Stockholm, Sweden). Clinical experts in the research team determined two key areas of interest (AOIs): (1) the tissue area where the knot should be tied, and (2) laparoscopic instruments. We measured participants' dwell time (i.e., total fixation duration on a specific area) on each of the AOIs mentioned earlier and also outside of the AOIs (referred to as “elsewhere”), and we analyzed it as a proportion of task completion time. The higher the dwell time, the longer the participant focused on the respective AOI during the task. In addition, we also analyzed the surgeons' and camera operators' joint attention to the AOIs, which means the fixation agreement on each AOI. The higher the agreement, the more often the surgeon and the camera operator simultaneously focused on the same AOI during the task.
Statistical analyses were performed with SPSS 24.0 (IBM Corp., Armonk, NY). Because of a nested data structure, two-level linear models (Level 2 = surgeons, Level 1 = trials) were computed to test the differences among the three camera conditions and to estimate correlations among eye-tracking parameters and task performance. Predictor (fixed) variables consisted of intercept and condition (or an eye-tracking parameter), and random effects included a random intercept. All variables were standardized before their inclusion into the analyses. The level of significance was set at P ≤ .05 (two tailed).
Results
Table 1 shows differences in performance, dwell time, and joint attention among the camera conditions. Angular pathway varied significantly across the conditions, F(2, 31) = 3.40, P = .046, with surgeons moving laparoscopic instruments less economically (i.e., with larger angular paths) in the fixed camera condition than in the expert condition (P = .028) and, marginally, the inexpert condition (P = .057). The expert and inexpert conditions did not differ in angular pathway (P = .93). The camera conditions had only a marginal effect on completion time and path length (Table 1).
Mean Values (Standard Devations) of the Main Study Variables Across Conditions
Dwell time represents the proportion of task completion time that participants fixated on each of the AOIs. Agreement represents the proportion of all fixations that surgeons and camera operators made on each of the AOIs at the same time.
AOIs, areas of interest.
Figure 1 depicts heat maps for surgeons' gaze behavior in the fixed camera condition and the operated camera conditions (aggregated over the expert and inexpert conditions). Overall, surgeons spent 32% of time focusing on the tissue area, 54% of time focusing on instruments, and 7% of time focusing elsewhere, with no significant differences among the camera conditions (Table 1). However, we found statistically significant differences in the camera operators' gaze behavior between the two operated camera conditions (the fixed camera condition was not included as there was no camera operator in this condition). Expert camera operators fixated longer than inexpert camera operators on task-irrelevant areas (elsewhere), F(1, 20) = 10.51, P = .004. Regarding surgeons' and camera operators' joint attention to the AOIs, we found no differences in the fixation agreement between the expert and inexpert camera conditions. Inexpert camera operators showed the same coordinated attention with surgeons as expert camera operators.

Heat maps for the fixed camera condition (left) and the operated camera condition (right).
Table 2 presents the association between gaze behavior and performance. Surgeons' dwell times on the tissue and laparoscopic instruments significantly predicted performance. The more time surgeons attended to the tissue, the better was the task performance in terms of shorter path length, b = −0.35, t(33.07) = -2.16, P = .038, and angular pathway, b = −0.33, t(33.18) = −2.03, P = .050. Fixating on laparoscopic instruments had the opposite effect. The longer surgeons focused on the needle holders, the longer the task completion took, b = 0.43, t(32.31) = 3.27, P = .003, and the greater were path length, b = 0.47, t(32.96) = 3.12, P = .004, and angular pathway, b = 0.44, t(33.16) = 2.85, P = .007. We further found a significant interaction between the surgeon's dwell time on the tissue and camera condition on path length, F(2, 30) = 4.01, P = .029, and angular pathway, F(2, 30) = 4.48, P = .020, indicating that the performance-harming effect of non-focusing on the tissue was especially visible in the fixed camera condition but disappeared in the expert camera condition (Fig. 2). The camera operators' gaze behavior was unrelated to task performance (Table 2). There was also no interaction between camera operators' dwell times and camera condition on performance. Finally, surgeons' and camera operators' joint attention to the AOIs did not predict performance.
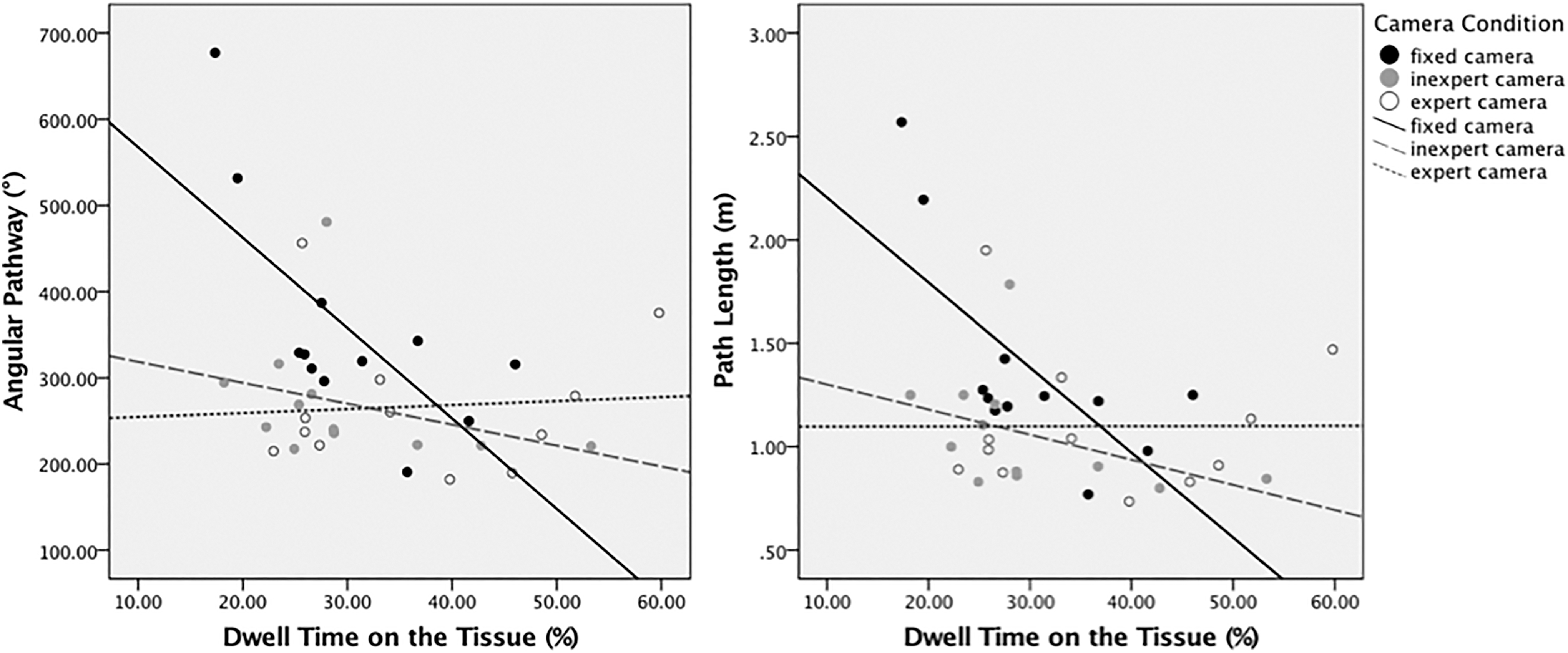
The interaction between surgeons' dwell time on the tissue area and camera condition.
Correlation Estimates Between Gaze Behavior and Performance
Coefficients marked with an asterisk depict significant correlations (*P < .10 and **P < .05). Positive values indicate that longer dwell time on an AOI is related to longer completion time, path length, and angular pathway (i.e., worse performance). Negative values indicate that longer dwell time on an AOI is related to better performance.
Discussion
In our experimental settings, we found that an operated camera was better for laparoscopic performance than a fixed camera. Surgeons' instrument movements were significantly less economic with larger angular pathways when the camera was fixed than when operated by another, even inexperienced, person. Surgeons also needed more time for task completion and showed longer path lengths during the fixed camera condition than when the camera was operated by another person, but these differences were only marginal (P ≤ .10), indicating statistical trends. 13 These results seem to preliminary support the previously discussed literature on the assumption that dynamic camera operation is superior to a static view, but a broader study with more power is still needed.
In our findings, there were no significant differences in surgeons' performance between the expert and inexpert camera holder. On the descriptive level, an expert camera operator helped a surgeon to fixate more on the most important AOI (the tissue area) than when the camera was operated by an inexpert person, but this did not translate into better performance. Similarly, the surgeons' and camera operators' joint attention on the tissue was higher when the camera was operated by an expert, but without an effect on performance. A possible explanation is that the camera work in this study was relatively simple in which the verbally given commands were easily applied and postulated and, thus, the experience in camera work could not become evident. Using a more complex, dynamic laparoscopic task in which the expertise of the camera operator would be more challenged might help detect stronger effects.
Inexpert camera operators fixated largely on the tissue area and instruments, but rarely elsewhere. In contrast, expert camera operators fixated less often on the laparoscopic instruments and were more “composed” in terms that they more often looked elsewhere when compared with inexpert camera operators. This “composure effect” might be explained by the routine of the expert camera operators as they had been trained in camera work previously and, in turn, presumably feel more confident in keeping the camera in the right position without losing the tissue target out of the surgeon's focus.
We further found that the more time the surgeons fixated on the target (the tissue area), the shorter the path length and angular pathway (i.e., the better performance) were. Fixating on instruments had the opposite effect; the longer the fixation, the worse was the task performance. On the one hand, these results support prior evidence from performance psychology showing that focusing too much on the mechanics of doing (here: laparoscopic instruments) instead of target area (here: the tissue) can worsen a skilled motor performance. 14 On the other hand, a poor performance due to repeated troubles with grasping the tissue or losing the needle could make the surgeons fixate more on the instruments to correct their position and improve the task execution.
Regardless of which of the explanations just provided holds true, we found that the effect of maladaptive gaze behavior on performance can be partly compensated by camera work. As evidenced by the significant interactions (Fig. 2), the detrimental effect of non-attending to the tissue area impaired surgeons' performance, especially in the fixed camera condition, much less in the inexpert camera condition, and the effect fully disappeared in the expert camera condition. Hence, camera work seems to be essential in laparoscopic surgery, even when surgery is conducted by less experienced camera operators. In our simple, static experimental task, it was probably sufficient to give verbal instructions to the camera operator during the task to complete the task sufficiently. However, it is unclear whether or not verbal instructions would be enough to promote good performance in a more complex, dynamic task. Future researchers should, therefore, employ complex laparoscopic tasks that require numerous camera movements to test the relevance of expertise in the camera world and its effects on surgical performance.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no specific funding or conflict of interest for this work.