
Abstract
Introduction:
The past decade has witnessed numerous advances in colorectal surgery secondary to minimally invasive surgery, evidence-based enhanced recovery programs, and a growing emphasis on patient-centered outcomes. The purpose of this study is to benchmark outcomes and experiences of patients undergoing colorectal surgery at a tertiary Veterans Affairs Medical Center for a 10-year period.
Materials and Methods:
Veterans who underwent nonemergent colorectal procedures between 2008 and 2018 were identified using targeted Current Procedural Terminology (CPT) codes and the Computerized Patient Record System. Patient outcomes were captured using the Veterans Affairs Surgical Quality Improvement Program and focused on length of stay and aggregate postoperative morbidity profiles. SAS® Version 9.4 (SAS Institute Inc., Cary, NC) was used for all data analysis with P < .05 used to indicate significance.
Results:
In total, 327 patients underwent colon/rectal resection at our medical center. Of whom 95% of patients were male and the average age was 66 years. The median length of stay after surgery was 8 days. Within the 30-day postoperative period, the composite morbidity score was 24.1%: most notable being superficial surgical site infections (6.5%), wound dehiscence (4.6%), and pneumonia (3.1%). Over the course of the study period, the laparoscopic approach increased in utilization, with 22.2% of cases performed laparoscopically in 2008 that rose to 61.1% in 2018.
Conclusion:
Cataloging this decade of practice provides a foundation for future changes in the field of colorectal surgery and in the treatment of veterans. Understanding historical outcomes should help identify areas for ongoing process improvement and guide targeted approaches to quality metrics.
Introduction
Colorectal surgery has taken great strides over the past several decades, mainly through adoption of minimally invasive approaches and evidence-based enhanced recovery programs. The first laparoscopic colon case was credited to Moises Jacobs, who performed a laparoscopic-assisted right hemicolectomy in 1990. 1 The first true laparoscopic colon resection was a sigmoidectomy performed by Fowler and White later that year.1,2 Not long afterward, the standard in colorectal surgery became utilizing laparoscopy whenever possible, ranging simply for initial mobilization and eventually all the way to intracorporeal anastomoses. With this gradual shift toward a more minimally invasive approach, studies have shown fewer complications, shorter lengths of stay, and improved oncologic results for patients undergoing laparoscopic colorectal surgery when compared with the standard open approach.3–6 More recently, robotic colon resections have become utilized by many colorectal surgeons; however, the data are mixed on whether robotic surgery should be adopted as the standard, as it has similar oncologic outcomes but longer operative times and higher cost.7–9
Although the literature has supported the movement toward minimally invasive colon surgery in the general population, there have not been studies that examine the outcomes of colorectal procedures in the Department of Veterans Affairs (VA) system. The VA system is the biggest integrated health care system in the United States, providing care for veterans of military service, and thus serving a large portion of our country.10,11 The veteran population is vulnerable and has a higher rate of comorbidities than the civilian population. 12 Studies have shown that in addition to inherent comorbidities that VA patients are more likely to suffer, such as post-traumatic stress disorder and depression, their risk for developing other chronic diseases, such as cardiovascular disease, is significantly higher. 13
Based on the higher rate of comorbidities in the patient population, VA medical centers were experiencing higher rates of complications than the private sector. 10 To counter this, the VA medical centers implemented measures to improve the quality of care at its centers. The VA Surgical Quality Improvement Program (VASQIP) was created to objectively measure outcomes in surgery. Using the same parameters as the National Surgical Quality Improvement Program, VASQIP measures complication rates and outcomes of all surgical procedures at VA centers. This along with other measures implemented in the 1990s helped to improve the care delivered at VA medical centers across the country. 10
Several studies have compared various general surgery outcomes between the VA and non-VA centers, and results have been mixed. Fink et al. showed that after risk adjustment, morbidity and mortality in women veterans were similar in these two cohorts in general surgery procedures, and Lancaster et al. evaluated hepatic rejections and also saw no difference in outcomes.14,15 Henderson et al. found a slightly higher risk of 30-day mortality in veterans undergoing general surgery procedures, and Lautz et al. found that although women did not have worse postoperative mortality in bariatric operations, male veterans did.16,17 Few studies exist that focus specifically on colorectal surgery outcomes in veterans. The objective of this study is to benchmark the outcomes for patients undergoing colorectal surgery at the VA medical center using the VASQIP database and to compare their results with those of the general population.
Materials and Methods
This is a retrospective review of a single VA institution using the VASQIP database. Institutional Review Board approval was obtained through the standard protocol of our institution. All patients who underwent a colorectal surgical procedure from January 2008 to June 2018 were included. Patients were identified for inclusion in the study using targeted CPT codes for any colon or rectum resection, with or without anastomosis. The resulting CPT codes used during this time period are listed in Table 1. Median predicted morbidity was calculated by the VASQIP database, which uses logistic regression analysis to calculate the probability of morbidity or mortality based on preoperative risk factors. Associations were made using Fischer's exact test, chi-square test, and ANOVA tests between methods of interest (laparoscopic, open, and open–laparoscopic conversion procedures) using several variables of interest (age, gender, length of stay, malignancy percentage, complication rate, and VASQIP complications). SAS® Version 9.4 (SAS Institute Inc., Cary, NC) was used for all data analysis with P < .05 used to indicate significance.
CPT Codes used for Colon Resection in the Past 10 Years at a VA Medical Center
CPT, Current Procedural Terminology; VA, veterans affairs.
Results
There were 327 patients over the study period who underwent elective colon and/or rectal resection at our medical center. In total, 94.8% of patients were male, and the average age was 66 years. In total, 57.5% of the operations were for malignancy, whereas the remainder were for benign disease. The median length of stay after surgery for all patients was 8 days (range 1 to 237 days). Within the 30-day postoperative period, the composite morbidity score was 24.1%. The most frequent morbidities were superficial surgical site infections (SSIs) (6.5%), wound dehiscence (4.6%), and pneumonia (3.1%). Median predicted morbidity across this cohort based on VASQIP risk algorithms indicated that patients had a 24.32% chance of any postoperative morbidity.
Comparisons were then made between three groups: patients who underwent a standard open approach, those who underwent a laparoscopic or laparoscopic-assisted approach, and patients who had a conversion from laparoscopic to open surgery. The average length of stay was 18.5 days in the open group and was significantly less in the laparoscopic group at 10.6 days (P = .03). There were more VASQIP complications in the open (29.2%) and conversion to open (31.9%) groups than the laparoscopic group (16.8%, P = .05). SSIs were more common in the open group with 10 instances compared with the 4 occurrences in the laparoscopic group (P < .05). Detailed demographics and outcome are listed in Table 2.
Patient Demographics and Outcomes of Colon Operations in the Last 10 Years
C. Diff, Clostridium Difficile Infection; DSI, deep incisional infection; DVT, deep vein thrombosis; MI, myocardial infarction; OSI, organ space infection; PE, pulmonary embolism; PNA, pneumonia; SSIs, surgical site infections; UTI, urinary tract infection; VASQIP, Veterans Affairs Surgical Quality Improvement Program.
Over the course of the 10 years captured in this query, 56.6% of patients underwent an open colon or rectal resection, 29.1% patients underwent laparoscopic or laparoscopic-assisted operation, and 14.4% of patients had a conversion from laparoscopic to open surgery. During this time, the laparoscopic approach increased in frequency, with 22.2% of cases done laparoscopically in 2008 that rose to 61.1% in 2018. Meanwhile the open approach decreased from 77.8% of cases in 2018 to 16.7% in 2018. Conversion rates were consistent, occurring ∼20% of the time (Fig. 1). The percentage of patients who had a complication during the study period was variable but generally decreased as the utilization of laparoscopy increased (Fig. 2).
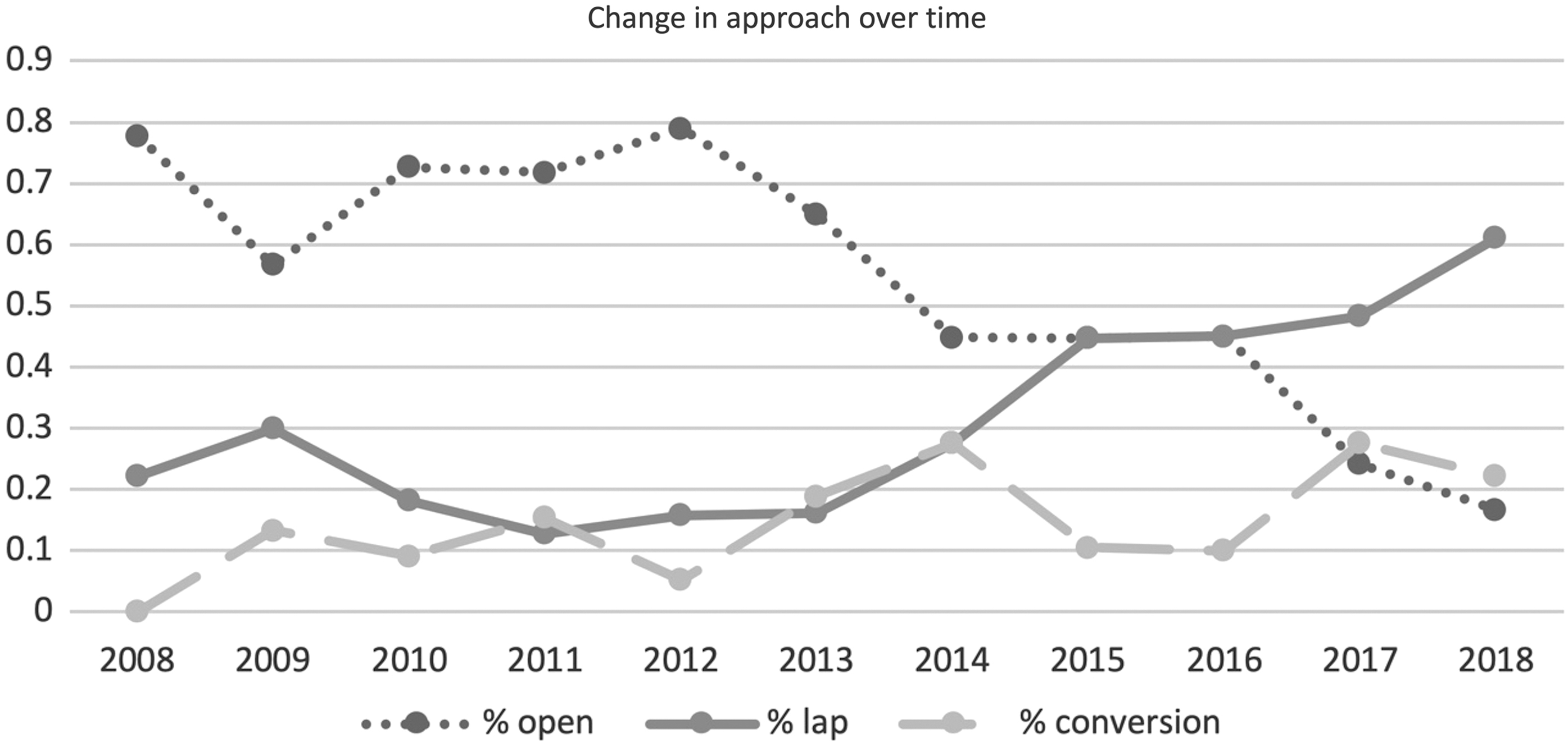
Percentages of surgical approach utilized, per year.
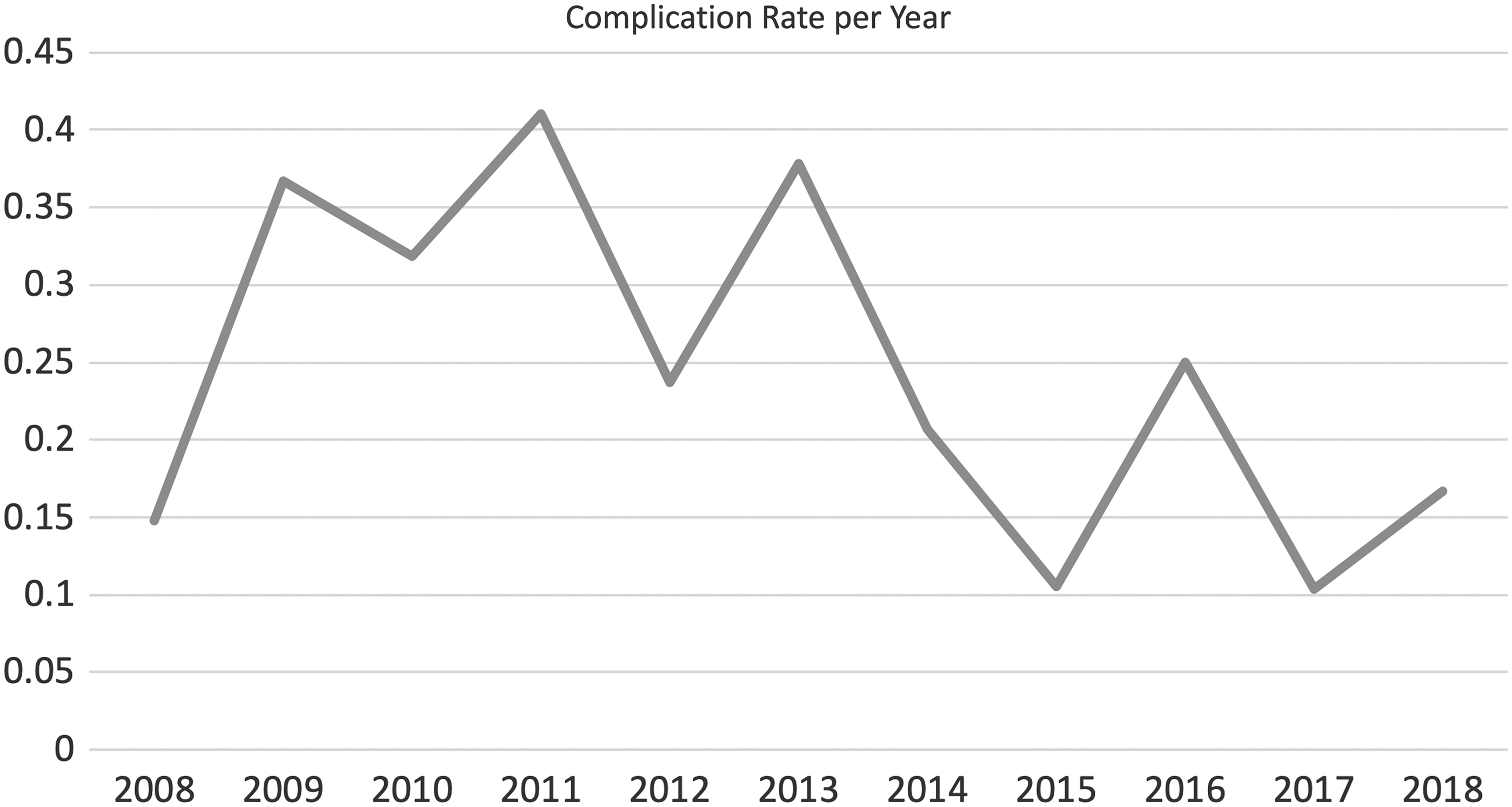
Complication rate per year, all approaches.
Discussion
Our results show that patients undergoing colon and rectal surgery at this VA medical center experience similar trends as those in civilian populations. Just as has been observed in the general population, open surgery has become less common, and laparoscopic and laparoscopic-assisted surgery have become the norm (Fig. 1). When comparing between patients who underwent open surgery versus laparoscopic surgery versus laparoscopic converted to open surgery, we see similarities with the outcomes reported in the private sector. The rate of wound infection was lower in the laparoscopic cohort than in the open group. Our cohort also demonstrated that the open surgery group had a significantly longer length of hospital stay than the laparoscopic cohort. Furthermore, as the utilization of laparoscopy increased, the rate of complications decreased in the cohort. This is all consistent with the numerous trials completed previously comparing laparoscopic with open colectomy in the non-VA population.18–21
With regard to how the outcomes in VA hospitals compare with the outcomes in non-VA hospitals, the results were mixed. The overall complication rate and the distributions of different types of complications were similar to reports from the private sector. However, complication rate was not as low.18,21 This could be due to the higher risk adjusted morbidity of veterans versus the general population. Agha et al. have noted stark differences in socioeconomic status between veterans and the general public, which should be taken into consideration when comparing these groups. 12
The length of stay observed was longer overall in the VA population than the general population. Median length of stay in our group was 8 days, which was slightly longer than the private sector of ∼5–7 days.18,21 This, in part, could be due to the fact that VA patients tend to have more socioeconomic disparities versus the general population. VA patients may be more likely to have a difficult disposition plan due to increased rates of homelessness and social challenges.
One instance where our institution has lagged behind somewhat is in robotic surgery. Since the conception of this study, there has been a steady rise in robotic surgeries at this VA, but at present there is not enough data to determine the impact it has had on outcomes relative to other approaches both at our institution and in the non-VA sector. Furthermore, as many hospitals have had an enhanced recovery after surgery (ERAS) program in place for many years, the institution in this study has only recently implemented its own ERAS protocol. Once fully instituted, it is likely that outcomes in colorectal surgery will approach the national average, as ERAS has been shown to significantly reduce the length of stay in colon surgery.22,23
There are several limitations in this study. The inherent weaknesses of a retrospective database review are present. The sample size of the 10-year cohort was also somewhat small, which may have prevented us from having the power to detect more statistically significant differences between groups. Furthermore, there was a relatively limited number of operators during the given time period, some of whom may have been limited in their experience in laparoscopy, thus creating a preference for an open approach or an increased likelihood of conversion to open surgery. In addition, our database did not capture the comorbidities of its subjects, which prohibited authors from accounting for the health disparities in VA patients versus the general public, which could have influenced the outcomes observed in our cohort.
Conclusion
Colorectal surgery for both benign and malignant disease at our VA center has outcomes comparable with those of the general public. Laparoscopic approaches have helped to decrease the complication rate and length of stay for patients undergoing colon resections at the VA. With the implementation of newer technologies and methods such as robotic surgeries and ERAS protocols, the VA center should continue to improve and see results that are equivalent to non-VA hospitals.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.