
Abstract
Purpose:
Treatment of pneumothorax involves conservative treatment and surgery. The aim of this study was to assess the best approach of initial treatment and long-term outcomes of video-assisted thoracic surgery (VATS) for primary spontaneous pneumothorax in pediatric patients.
Patients and Methods:
From January 2009 until June 2019, 36 patients younger than the age of 18 who were treated for spontaneous pneumothorax were included into retrospective study. Patients were divided into 2 groups, non-VATS and VATS, depending on the way they were treated. The groups were compared regarding demographic and clinical data and outcomes of treatment (the length of hospitalization, the frequency of postoperative complications, and reoperations).
Results:
Out of 36 patients, there were 24 boys and 12 girls with median age of 16.5 years. Median duration of hospitalization was 8 days. Eight patients were treated by observation and 28 by chest tube insertion. In 14 patients with spontaneous pneumothorax, VATS was performed [indications were persistent air leak in 8 (57%) and recurrent pneumothorax in 6 (43%) children]. Patients who underwent surgery had significantly higher length of hospitalization (P < .001) and lower rate of recurrences (P = .003) than those who did not. In 12 (86%) patients, blebs were found intraoperative, and in all of them, pleurodesis was performed. Duration of chest tube insertion was significantly longer in patients who experienced recurrent pneumothorax (P < .001).
Conclusions:
VATS is successful, efficient, and safe method of treatment for spontaneous pneumothorax, due to its significantly lower rate of recurrence in comparison with chest tube insertion.
Introduction
Primary spontaneous pneumothorax is an abnormal accumulation of air in the pleural space. It is a relatively rare condition in children and adolescents with an incidence of 3.4 cases per 100,000 children. 1 Thin and tall young adolescents with asthenic type of constitution are most commonly affected, with a 4:1 male predominance. 2 The most common cause of primary spontaneous pneumothorax is rupture of subpleural blebs. Nonproportional growth of the thorax may cause an increase in negative pressure at the apex of the lung, leading to formation of subpleural blebs.1–3 Pediatric surgical community has not reached consensus on the optimal approach to treatment. In asymptomatic patients with small pneumothorax (up to 15%–20%) initial management usually involves breathing exercises and oxygen administration.
Larger pneumothorax is typically treated with drainage with a chest tube, although only needle aspiration has been recommended by recent studies. 4 Surgical management is indicated only in cases of recurrent or refractory pneumothorax.2,3,5 Nowadays, with the advent of minimally invasive thoracic surgery, definitive operative management of pneumothorax, with high success rates, can be achieved with faster recovery, better cosmetics, decreased pain, length of hospital stay, and morbidity.2,5 Nowadays, there is no general strategy for the treatment of spontaneous pneumothorax. Controversy exists regarding the timing of surgery, which can be performed either after the first episode (primary surgery) or after a recurrent pneumothorax has occurred (delayed surgery).
The argument against performing surgery in all patients after the initial episode of pneumothorax is that a significant number of patients will not develop a recurrence, resulting in overtreatment of a number of patients. We attempted to evaluate preferable treatment modality for the pediatric patients with a spontaneous pneumothorax regarding complications after surgery, recurrence rates, and total length of hospital stay. Few recently published studies have shown that management of children and adolescents suffering from primary spontaneous pneumothorax with chest tube insertion initially followed by video-assisted thoracic surgery (VATS), for patients who have a recurrence, appears to be the most appropriate treatment. This treatment protocol avoids unnecessary surgery in about 40%–50% of children who do not have recurrence after conservative treatment.2,3,5,6
Due to limited published studies, it still remains controversial what is the optimal time for surgical treatment. Some surgeons suggest early VATS for definitive disease resolution and earlier recovery, while others recommend reserving surgery only for those patients who fail nonoperative management.5–7
The aim of this study was to assess the best approach of initial treatment and long-term outcomes of VATS for primary spontaneous pneumothorax in pediatric patients.
Methods
Patients
A retrospective database analysis of medical records on 36 patients, with the median age of 16.5 years, treated in our institution because of spontaneous pneumothorax between January 2009 and June 2019 was performed. The study was approved by the Ethics Committee of our hospital. The patients were divided into 2 groups regarding approach of treatment: Group 1 (non-VATS) consisted of all patients who were treated conservatively or with chest tube drainage and Group 2 (VATS) consisted of all patients who were treated by VATS. Indications for VATS were as follows: persistent air leak after chest tube placement, recurrent ipsilateral pneumothorax, occurrence of a contralateral pneumothorax, bilateral pneumothorax, and visible large blebs >1 cm in diameter on chest radiograph (Fig. 1A) or computed tomography (Fig. 1B).

Primary spontaneous pneumothorax in 17-year-old female patient.
The medical records included initial medical history, demographic data (age, gender, body mass index [BMI]), clinical data (presenting symptoms, duration of symptoms before surgery, localization, and size of pneumothorax—small, moderate, or large), as reported by the radiologist and documented in the medical record, comorbidity, operative findings (indication for surgery, surgical procedure, duration of surgery, intraoperative visualization of blebs), outcomes of treatment, and follow-up (duration of postoperative drainage, length of hospital stay, complications, number of recurrences, and readmissions to hospital).
Inclusion criterion was patients aged 0–17 years with pneumothorax. Exclusion criteria were patients older than 17 years of age, patients operated in another institution and followed-up at our outpatient clinic, those with incomplete data, or those who have been followed-up less than 3 months.
Outcome measurements
The primary outcome measures were outcomes of treatment, complications, number of recurrences, and reoperations. The secondary outcome measures were indications for surgery, duration of surgery, time to chest tube removal, and length of hospital stay.
Surgery
All VATS procedures were performed as a three-port technique, under general anesthesia in a position as for a posterolateral thoracotomy with the operating table flexed at 30° to open up the intercostals spaces. The 5 mm trocar for introduction of camera was placed in the seventh intercostal space in the midaxillary line. First, 12 mm working port was placed usually over the fifth intercostal space between the mid- and anterior axillary lines (usually at previous place of chest tube). A third 5 mm trocar was placed also in fifth intercostal space, but posteriorly behind scapula. After careful examination of the lung, blebs were identified (Fig. 2A) and resected by endostapler (endoGIA®; Ethicon Endosurgery, Cincinnati, OH) (Fig. 2B). At the end of the procedure pleural abrasion was performed. The parietal pleura was abraded with a rough sponge by scrubbing the parietal pleura until a uniform aspect of bloody pleura was achieved (Fig. 2C) and a chest tube was inserted under the visualization of camera (Fig. 2D). The chest tube was typically removed when the air leak ceased and postoperative chest radiographs showed no residual pneumothorax.
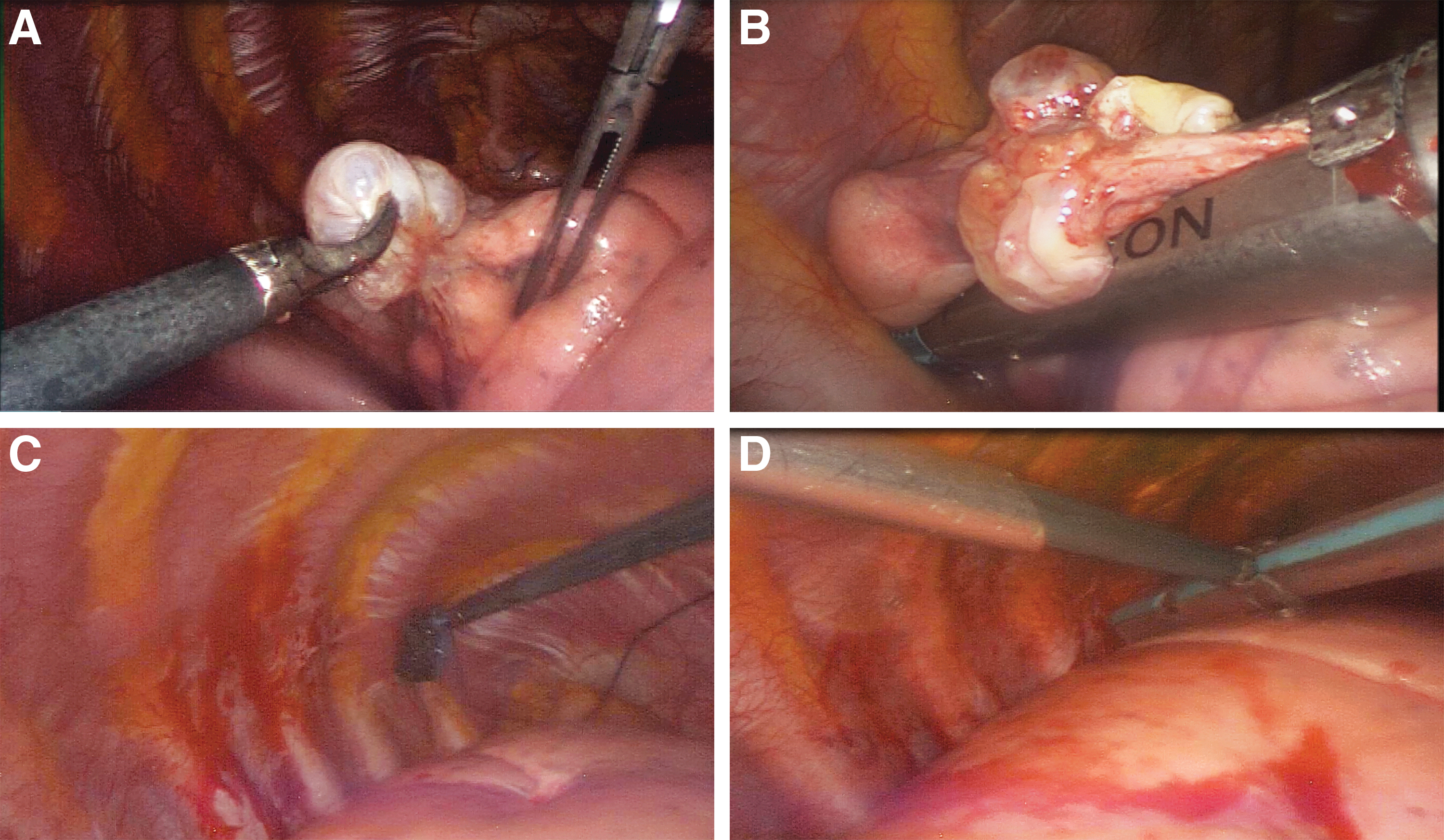
Intraoperative findings in 16-year-old male patient with recurrent spontaneous pneumothorax.
Statistical analysis
The data were analyzed using SPSS® 24.0 (BM Corp. Released 2016. IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp.) software program. Quantitative data were expressed as median and interquartile range (IQR). Mann–Whitney U test and ANOVA (analysis of variance) were used to test differences in median values of quantitative variables. Categorical data were presented with absolute rates and percentage. The chi-square test was used for the statistical analysis of the categorical data. All values of P < .05 were considered statistically significant.
Results
A total of 36 pediatric patients meet inclusion criteria and were included in study. The majority of patients were male (n = 24; 67%), with a median age of 16.5 (IQR 14.5–17) years and median BMI of 20.0 (IQR 16.5–21) kg/m2. Left side was affected in 20 (55%) patients while pneumothorax on right side was found in 16 (45%) of the patients. Smoking history was not recorded in any of the patients. The most common presenting symptoms were chest pain (83%), dyspnea (50%), and cough (17%). Median hospital stay was 8 days (IQR 7–12).
The initial management of the patients with spontaneous pneumothorax consisted of supplemental oxygen and breathing exercises in 8 patients, 28 received chest tube drainage, while 8 patients from the same group underwent VATS shortly after drainage because of the persistent pneumothorax. Six patients of the group that was initially managed nonoperatively had recurrence of the pneumothorax after discharge from the hospital and they were also treated by VATS afterward. So the end result was 8 (22%) patients being treated conservatively, 14 (39%) with a chest tube drainage, and 14 (39%) with VATS. Algorithm of treatment has been shown in Figure 3.

Algorithm of treatment of the patients with pneumothorax. VATS, video-assisted thoracic surgery.
Small pneumothorax (≤4 cm) was found in 20 (55%) patients, pneumothorax of moderate size (4–8 cm) was recorded in 10 (28%) patients and large (>8 cm) pneumothorax in 6 (17%) children. Complications were recorded in 4 patients (20%) with small pneumothorax, in 2 (20%) patients with pneumothorax of moderate size and in 3 (50%) patients with large pneumothorax. Median length for hospital stay was 8 (IQR 7–10) days for patients with small pneumothorax, 8.5 (IQR 6.5–12) days for pneumothorax of moderate size, and 10 (IQR 7–14) days for large pneumothorax. Statistically significant correlation between the size of pneumothorax (P = .301) as well as length of hospital stay (P = .396) and incidence of complications was not found (Table 1).
Length of Hospital Stay and Complications with Regard to Size of Pneumothorax
Chi square test.
Analysis of variance.
IQR, interquartile range.
Conservative treatment or chest tube insertion was the method of final treatment in 22 (61%) patients (non-VATS group), while 14 (39%) patients underwent VATS (VATS group). These 2 groups were similar with regard to age (P = .901), gender (P = .628), BMI (P = .751), size of pneumothorax (P = .148), lateralization (P = .878), duration of symptoms (P = .470), lung expansion (P = .107), and complications (P = .141). The length of hospital stay was significantly higher in patients who underwent VATS (P < .001). An incidence of recurrences was significantly lower in patients who underwent VATS compared to the patients who were treated conservatively or with chest tube insertion (P = .003) (Table 2).
Comparison of Outcomes of Different Methods of Treatment of Pneumothorax, n = 36
Mann–Whitney U test.
Chi square test.
BMI, body mass index; ICU, intensive care unit; IQR, interquartile range; VATS, video-assisted thoracic surgery.
Characteristics of the patients who underwent VATS are shown in Table 3. Persistent pneumothorax was an indication for surgery in 8 (57%) patients and recurrent pneumothorax in 6 (43%) of them. No serious complications were recorded. From total number of the patients who underwent VATS, in 12 of them chest tube insertion was initial treatment, with median duration of 7 (IQR 1.5–9.8) days before surgery. Seven (50%) of the patients experienced previous episodes of pneumothorax in the past that were treated conservatively. The median surgical time was 40 (IQR 55–120) minutes. Blebs were visualized in 12 (86%) patients intraoperative, and pleurodesis was performed in the same number of the patients. In 2 patients where no blebs were identified intraoperatively, stapled apical lung wedge resection was performed to decrease possibility of recurrence.
Outcomes of Treatment of the Patients Treated with Video-Assisted Thoracic Surgery; n = 14
Patient did not undergo pleurodesis.
IQR, interquartile range.
Median duration of postoperative drainage was 5 (IQR 3–5) days. Recurrence of the pneumothorax after VATS was recorded in only 1 patient (7%), who did not undergo pleurodesis during the surgery. That patient experienced recurrence of pneumothorax 5 weeks after discharge from hospital. At the time of recurrence, he was treated by chest tube drainage, but due to the persistent pneumothorax, redo surgery (VATS with pleurodesis) was performed.
Discussion
In the present study outcomes of VATS for the treatment of primary spontaneous pneumothorax in pediatric patients were evaluated. Although retrospective, this study provides clear evidence that early VATS for primary pneumothorax in children and adolescents is associated with excellent outcome, fast recovery, and low incidence of complications and recurrences. Among a typical population of adolescent patients with spontaneous pneumothorax, treated in our institution, initial nonoperative management was treatment of choice. The majority of our patients were initially managed with insertion of a chest tube.
This study has shown that among those patients who initially managed with a chest tube, the presence of an air leak and partial lung expansion on chest X-ray are strong predictors of failure of conservative management. In these cases early VATS should be considered as possible treatment option. Initial management of primary spontaneous pneumothorax may be dictated by physician preference, patient or disease characteristics, or radiologic imaging findings.1–12 In most of the pediatric centers initial management of pneumothorax is conservative with supplemental oxygen only or a chest tube insertion.2,4,7,12
There are some recent studies that doubt whether primary surgery for spontaneous pneumothorax is better than conservative treatment in pediatric population and adolescents. Some of the authors suggest primary surgery, while others suggest conservative treatment initially.2,5,12 Our observed overall recurrence rate was 39%, which is slightly lower than in other recent single-center reviews of pediatric patients with primary spontaneous pneumothorax where recurrence rates varies from 46% to 54%.2,6,12 A closer analysis of the data has shown that only 39% of patients with primary pneumothorax were managed with a chest tube alone at the first presentation had a recurrence. This suggests that if a strategy of primary surgery was performed on all such patients, 61% of our patients would undergo unnecessary surgery. Similar findings were reported in other single-center reports of pediatric patients with primary spontaneous pneumothorax.2,3,5,12 With regard to the initial management approach, some authors suggest chest tube alone within the first 2 days and the clinical course and patient preference were then used to eventually decide on surgical intervention. 5
The demographic data of our study population showed that primary spontaneous pneumothorax is the most common among thin, adolescent males. Chest pain and dyspnea were the most common presenting symptoms. These findings are similar to the published reports.1–3 Statistically significant correlation between the size of pneumothorax as well as length of hospital stay and incidence of complications was not found in our study. Regarding the size of the pneumothorax in children who received VATS, the majority of pneumothorax in our study was moderate size, but we did not find significant correlation with the outcome of treatment. Such result is in accordance to most of the published literature.5,8
Median of surgical time in our study was 40 minutes, which is lesser than in published literature whose median surgical time was 60 minutes.3,9,10 Median of postsurgical drainage was 5 days, which fits findings of other published studies.3,5 This study also found that duration of chest tube drainage was longer in patients with recurrent pneumothorax. In our group of patients treated with VATS, only 1 patient had recurrence. That patient did not undergo pleurodesis. Other published studies are mostly in accordance to our findings.2,3,9–14 Recurrence after VATS has also significantly decreased according to their results. They suggest that VATS should be considered in earlier stages of pneumothorax and only few days after ineffective conservative treatment, especially in patients with recurrent or persisting pneumothorax.
It was pointed out in previously published studies that the length of hospital stay was lower in patients who underwent VATS than in those who first underwent conservative treatment.2,12 In our study, blebs were visualized in 86% of the patients. Same number of patients underwent pleurodesis. The outcome of treatment was excellent; none of them had recurrence, which may indicate that pleurodesis has important impact on the efficacy of treatment, although there are some reports in literature where correlation between pleurodesis and recurrence rate was not found. 9 Most of the published studies recommend pleurodesis as important part of the procedure.3,13,14 Some authors even suggest contralateral pleurodesis as a prevention of possible future contralateral pneumothorax.13,14 Detailed exploration of lower lobes might also be the key to prevention of recurrence since two of their patients experienced it because of the blebs found there. 3
The main limitation of this study is retrospective character, although we have implemented multiple plausibility checks and cross validations in our data collection tool. Also, due to the fact that surgical treatment of pneumothorax is not very common condition in pediatric patients, there is a relatively small number of patients included in the study.
We believe that this study may serve as a foundation for prospective studies and the development of a predictive model that can serve as a clinical decision-making tool for the management of primary spontaneous pneumothorax (early surgery versus conservative treatment) in children and adolescents. Prospective studies can validate the impact of earlier surgical intervention on length of hospital stay, recurrence rates, and need for subsequent procedures.
Conclusions
Based on our results, we recommend that initial chest tube insertion should be used as primary therapeutic line in pediatric patients with spontaneous pneumothorax, and VATS should be performed only for recurrence. According to the results of our study VATS is an effective, successful, and easily performed surgical method with excellent outcomes. Pleurodesis might also play a major role in the efficacy of treatment and especially in prevention of future episodes.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.