
Abstract
Background:
Peritoneal dialysis (PD) is an increasingly utilized treatment modality for renal replacement therapy that affords medical and lifestyle benefits to the patient and financial savings to the health care system. Successful long-term use of PD is reliant upon an optimally functioning catheter. Many potential catheter-related complications can be avoided through utilizing optimal placement technique. As widespread use of PD as a renal replacement modality continues to increase, the need for a safe, standardized, catheter placement technique has become more evident.
Objectives:
To present a succinct synopsis of the rationale and elements of our current surgical management strategy for patients undergoing evaluation for PD and to provide a detailed stepwise description of our operative technique for PD catheter placement. This review describes potential pitfalls that may prevent optimal catheter function and describes each step taken to prevent potential complications. This description is combined with intraoperative photographs to highlight key steps.
Conclusion:
Following a defined reproducible stepwise approach, laparoscopic placement of continuous ambulatory peritoneal dialysis catheters can be performed safely and known potential complications hindering optimal catheter function can be addressed prophylactically.
Introduction
Peritoneal dialysis (PD), first described as a long-term management modality for end-stage renal disease (ESRD) in 1976, is becoming an increasingly utilized method for renal replacement therapy. From 1996 to 2016, the incidence of ESRD in the United States has steadily increased from 77,003 to 124,675 patients per year and PD was the renal replacement treatment modality employed for 10% of new patients requiring dialysis in 2016. 1 Since 2011, Medicare has bundled payments for ESRD patients, and in 2015, the Centers for Medicare and Medicaid Services (CMS) issued a Comprehensive ESRD Care Model striving to create incentives to enhance care and ultimately improve health outcomes for ESRD patients. Two of the largest dialysis providers in the United States, DaVita and Fresenius, have each publically stated goals to increase the number of patients on home dialysis. DaVita currently has 13% of patients on home dialysis with goals to reach 25% by 2025. Fresenius is aiming to increase home dialysis prevalence from 12% currently to 25% by 2022. 2 As the health care system strives to meet these goals, the need for high-quality and standardized reproducible CAPD catheter placement techniques must be addressed.
PD offers several advantages in comparison to tradition hemodialysis renal replacement, including lower dialysis cost, improved quality of life, in-home dialysis, better blood pressure control, and fewer dietary limitations.3–5 Drawbacks of PD include the need for anesthetic induction for catheter placement, the need for PD to be performed daily, and requirement of an external catheter, which some patients may find cosmetically unappealing.
Surgical techniques for catheter placement include open laparotomy, percutaneous puncture, and laparoscopic technique. Every step of this described approach is specifically designed to achieve optimal catheter placement and promote long-term catheter function. The laparoscopic placement offers several advantages over percutaneous puncture approach, as described in this article, including performing the procedure under direct visualization and confirming catheter placement and orientation in the pelvis. The laparoscopic approach also allows for evaluation of the omentum and for omentopexy to be performed in patients whose omentum reaches to the pelvis. In addition, the laparoscopic approach affords ability to tunnel the catheter through the preperitoneal plane, an option not available when placing catheters using the percutaneous puncture method. Other than the moribund patient unable to tolerate general anesthesia, we believe most patients should be offered the proposed laparoscopic approach.
While perioperative morbidity is low and mortality negligible, there are multiple well-described complications of PD, including peritonitis, infection, catheter outflow obstruction, leakage, and migration, which hinder optimal functioning of the PD catheter. 6 Specific techniques during laparoscopic catheter placement have been developed to address many of the common complications of Tenckhoff catheter placement described above. These techniques include omental fixation,6–8 extraperitoneal tunneling, 9 adhesiolysis, 6 paramedian placement, 10 and catheter fixation. 11 A method combining all of these techniques and introducing other techniques to optimize catheter placement has been described and demonstrated improvement in the incidence of mechanical flow obstruction. 7 Herein, we describe a novel technique expanding upon prior described methods of PD catheter placement through the addition of several other steps to address known potential complications. A feasibility and efficacy review using this technique for 20 patients over the course of 1 year demonstrated a 95% success rate for catheter placement with average operative time of 37 minutes with 0% mortality rate. 12 The 30-day morbidity was 15%, including 1 patient with intra-abdominal bleeding, 1 patient with urinary retention, and 1 patient with catheter site cellulitis. 12 Our technique offers a safe and standardized reproducible method for laparoscopic placement of CAPD catheters. This is a fully illustrated description with figures and intraoperative photographs to highlight and emphasize key anatomy and critical surgical steps.
Preoperative Management
The scope of developing a new PD catheter placement technique was to address known potential pitfalls and optimize catheter function. All patients referred for PD catheter placement are evaluated as potential candidates in the surgery office. This initial assessment is critical as it affords the surgeon opportunity to assess patient-related factors, including body habitus, prior surgical scar location, presence of hernias, ostomies, skin lesions, and medical comorbidities. The patient is best evaluated in an upright sitting position with care taken to note the level of skin folds, belt line, and other potential abdominal lesions as to select an appropriate catheter exit site. Care is taken to exclude patients in whom PD is contraindicated.
Preoperative preparation includes clipping of body hair present in the surgical field. This is ideally performed with electric clippers as opposed to straight razor blades to avoid microabrasions and local skin trauma creating a potential route of infection. A prophylactic antibiotic regimen used for all operations is dosed appropriately by patient weight and is administered within 30 minutes of skin incision. We routinely use Cefazolin, and in penicillin allergic patients we use Clindamycin. The surgeon and assistant should wear two pairs of gloves as an added precaution to prevent contamination, should a breach in glove integrity occur. Patient voiding to decompress the bladder immediately before surgery is not a component of our technique. We prefer the bladder to be distended, allowing for rapid identification of the bladder dome, which assists in avoiding iatrogenic bladder injury during catheter tunneling.
Operative Technique and Potential Complications
The operative technique is illustrated with intraoperative photographs to highlight key procedural steps. Potential complications are identified and addressed throughout the description of the procedure.
Incision Planning
After general endotracheal tube anesthesia induction, the skin is prepped with chlorhexidine scrub and an adhesive Betadine skin barrier is placed. The Betadine skin barrier serves as an added precaution to ensure that direct contact between the PD catheter and the skin does not occur.13,14 The incisions are planned for abdominal entry at Palmer's point, the right lower quadrant catheter exit site, and the operative port in the left mid-abdomen at the level of the umbilicus. Additional care should be taken to plan an appropriate catheter exit site location. With performance of PD, gravity results in fluid accumulation in the lower abdomen. If the catheter exit incision is placed too inferiorly, pooling fluid will place undue stress on the incision potentially, leading to fluid leaking around the catheter exit site or development of incisional hernia. As a precautionary measure, the planned catheter exit incision should be in the right lower quadrant ∼3 cm lateral and slightly inferior to the umbilicus. In addition, catheter exit site should not be placed in a skin fold or through areas of compromised skin integrity. Optimal port site and tunneling site locations are depicted in Figure 1.
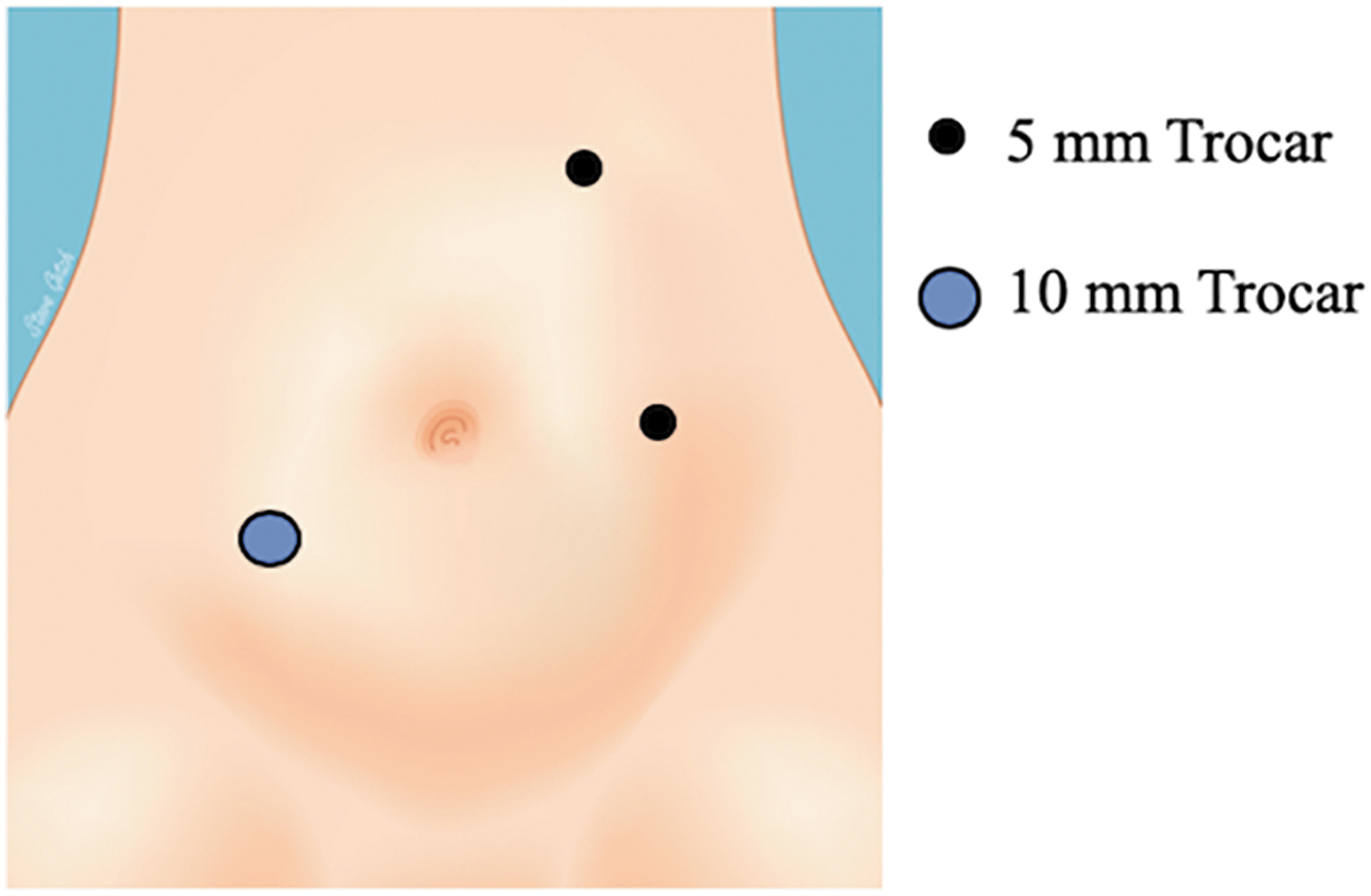
Location of 5 mm port sites and 10 mm tunneling trocar placement.
Abdominal Entry
Peritoneal access is obtained in the left upper quadrant at Palmer's Point using a 5 mm optical muscle spreading trocar. Veress needle entry followed by introduction of muscle-spreading trocar is also acceptable. Pneumoperitoneum of 15 mmHg is obtained. Safe abdominal entry is critical as inadvertent enterotomy mandates repair and abortion of catheter placement due to risk of infection. The patient is then placed in slight Trendelenburg position to assist in exposure through rotation of small bowel out of the pelvis. A 5 mm muscle-spreading trocar is placed in the left mid-abdomen at level of umbilicus under direct visualization. A second 5 mm muscle-spreading trocar is placed under direct visualization through the planned catheter exit site in the right lower quadrant ∼3 cm lateral and slightly inferior to the umbilicus. Use of muscle-spreading trocars is recommended as their use has been demonstrated to reduce incidence of incisional hernia, hematoma, and other trocar-related complications when compared to the use of bladed trocars. 15 After placement of all trocars, the abdominal cavity is surveyed for potential obstacles to catheter placement such as ascites, neoplasm, dense adhesions, or large hernias.
Omentopexy
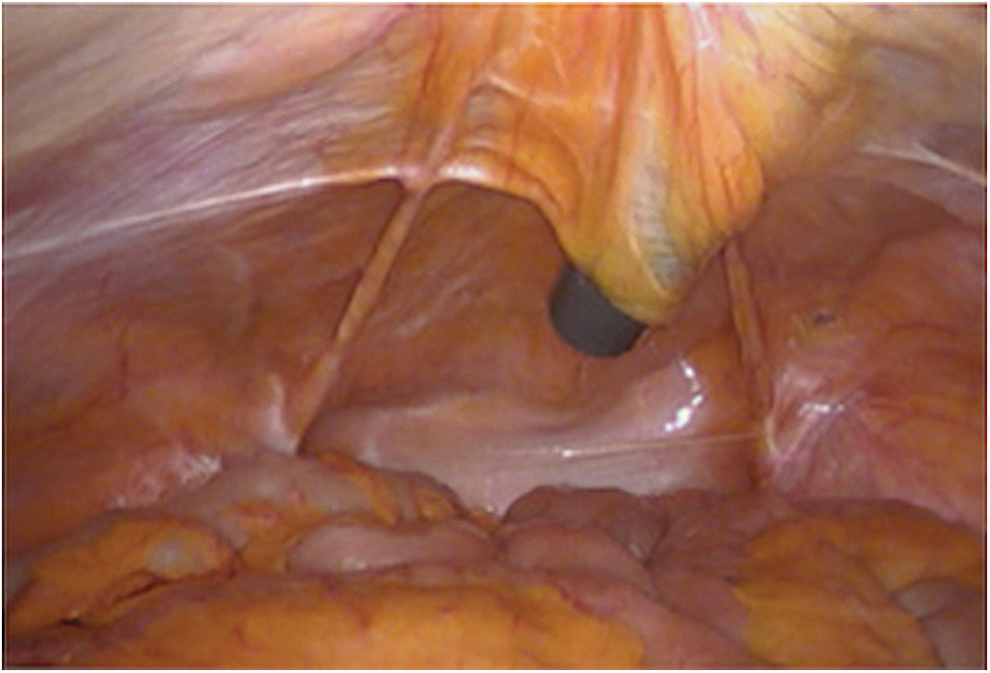
The omentum, if present, is identified. When present and mobile to the pelvis, the omentum is reflected to the right upper quadrant and secured to the abdominal wall with 2-0 silk suture secured intracorporeally in a figure-of-eight manner. The omentopexy is performed in the right upper quadrant through a stab incision and with assistance of a suture passer as demonstrated in Figure 2.

Omentum unable to reach the pelvis after omentopexy.
Historically, placement of PD catheters was performed by open surgical technique. A major complication of this method was development of mechanical outflow obstruction due to omental wrapping around the catheter. The advent of laparoscopic catheter placement introduced omentopexy as a key step, which has been demonstrated to prevent mechanical obstruction caused by omental wrapping.8,16,17
In patients where the omentum is not present or is present and not mobile to the pelvis, the potential for omental entrapment is negligible and omentopexy is not necessary.
Placement of the Dialysis Catheter
The right lower quadrant trocar is then removed and exchanged for a 10 mm blunt trocar placed through the right lower quadrant planned catheter exit site incision and tunneled in the preperitoneal space to a point just above the bladder. A Tenckhoff catheter is used for all patients. When performing the tunneling, it is imperative to create ample length of tunneling tract and assure the catheter tunnels correctly through the preperitoneal plain. Having too short of a tunnel length can result in near overlapping of skin opening and peritoneal opening. This proves problematic as the tissue ingrowth cuffs do not rest appropriately and a direct path for peritoneal fluid leakage is present. Conversely, too long of a tunnel length prevents the coiled portion of the catheter from reaching the pelvis. A total tunnel length of 3–4 cm is most advantageous as the tissue ingrowth cuffs are properly offset and the catheter retains appropriate length to rest in the pelvis. Tunneling through incorrect planes can result in increased postoperative pain, hematoma, neurovascular injury, and sharp angles in the catheter tubing. The direction of the tunneling path should maintain a linear orientation of the catheter into the pelvis. This assists in preserving catheter position and hinders catheter migration. Optimal tunneling position is demonstrated in Figure 3.
The direction of the tunneling path providing a linear orientation of the catheter into the pelvis.
The catheter is then placed through the 10 mm trocar with the coil carefully positioned in the retrovesicular space in the dependent portion of the pelvis. The two tissue ingrowth cuffs of the catheter are confirmed to be in the preperitoneal space and subcutaneous tissue, respectively, as the trocar is removed. Ideal placement of the tissue ingrowth cuffs optimizes long-term position of the catheter. In cases where the catheter remains mobile, despite correct initial positioning in the pelvis, consideration for securing the catheter in place with a 2-0 transfascial polypropylene suture placed cephalad to the dome of the bladder is warranted. The ideal final position of the catheter, centered cephalad to the bladder, is demonstrated in Figure 4.
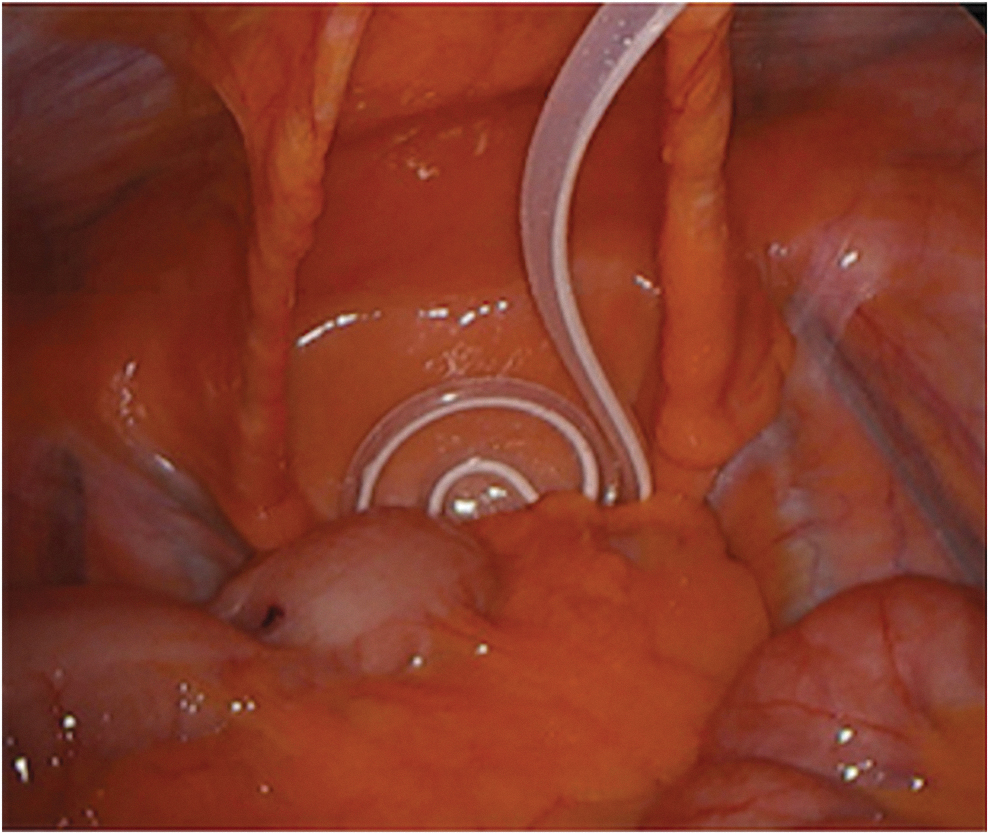
PD catheter in appropriate position centered cephalad to the bladder. PD, peritoneal dialysis.
Neither the fascia at the 5 mm camera port nor the fascia at the 5 mm surgical port is closed. Pneumoperitoneum is released and the catheter position is observed with the camera as desufflation commences.
External Fixation of the Dialysis Catheter
Betadine is then dripped into the skin wound through which the catheter exits. A silk suture placed in a simple interrupted manner is used to reapproximate the skin around the catheter at the exit site to close the incision around the catheter and expedite healing. Appropriate closure of this site is critical as to eliminate a potential route of dialysis fluid leakage. A drain stitch is placed to secure the catheter in place. A second suture is placed to anchor the catheter to the skin at a separate location to avoid inadvertent catheter dislodgement. Should the catheter catch or the patient inadvertently pull on the catheter end, the force is transmitted to this suture and tugs on the skin rather than transmitting a force that may result in catheter dislodgement. Bacitracin is applied to the closed catheter exit site. The remaining port sites are closed with 4-0 absorbable suture placed in a subcuticular manner. The catheter is flushed with heparinized saline to prevent fibrin clot formation before the catheter use begins.
Postoperative Management
Postoperatively, the patient is transported to the postanesthesia care unit for recovery and either discharged home or admitted to the hospital. Any patient admitted to the hospital is followed during their hospitalization for evidence of acute complications. Patients discharged home receive oral pain medication and instructions to follow up with the surgeon in 2 weeks. At the follow-up visit, the silk sutures are removed and the catheter is inspected. Flushing of the catheter with low volume solution is started on postoperative day 2, and unrestricted PD is allowed to commence 5 days after catheter placement.
Conclusions
There is an increasing need for optimal PD catheter placement and a refined ideal placement technique is imperative to provide patients with the highest chance of success. The description presented above provides a detailed, logical, stepwise PD catheter placement technique and describes rational for each decision. Overall, this is a safe and highly reproducible surgical technique focused on promoting optimal catheter function and addresses known potentially preventable complications.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.