
Abstract
Background:
Type II endoleaks from a patent inferior mesenteric artery (IMA) occur in up to one-third of patients undergoing endovascular repair of abdominal aortic aneurysms. In the majority of patients, retrograde flow in the aneurysmal sac outside the endograft will seal over time and is rarely associated with sac enlargement or aortic rupture. Intervention is generally recommended in patients with progressively enlarging endoleaks, especially when the sac diameter increases >10 mm during the follow-up, and endovascular IMA embolization has a high rate of treatment failure.
Methods:
We report a procedure of laparoscopic IMA clipping combined with intraoperative indocyanine green (ICG) angiography to confirm vascular anatomy, colonic perfusion, and the technical success of the procedure.
Results:
Three selected octogenarian patients with persistent type II endoleak after endovascular repair of abdominal aortic aneurysm underwent IMA clipping with ICG angiography. Mean operative time was 58 ± 9 minutes. There were no procedure-related complications, and no hypersensitivity reactions nor other side effects associated with ICG dye administration occurred. All patients were discharged home on postoperative day 1 and are asymptomatic and free of recurrence at a mean follow-up of 15 months.
Conclusions:
Laparoscopic IMA clipping is a safe remedial procedure in patients with type II endoleak after endovascular repair of abdominal aortic aneurysms.
Introduction
There has been a paradigm shift in the management of abdominal aortic aneurysms after the introduction of endovascular aneurysm repair (EVAR). However, up to one-third of patients develop an endoleak defined as backflow in the aneurysmatic sac outside the graft detected on a routine computed tomography (CT) scan follow-up. 1 Retrograde filling through the inferior mesenteric artery (IMA) or the lumbar arteries is defined as type II endoleak. Although the natural history of type II endoleak is often benign, rupture of the aneurysmatic sac may occur and may be associated with sac expansion. Intervention has been recommended in case of progressively enlarging aneurysms, especially when the sac diameter increases >10 mm during the follow-up and when the endoleak originates from the IMA. 2
Selective embolization of the IMA is considered the first choice approach, but is associated with ischemic complications and a high failure rate, requiring secondary procedures. 3 If the endovascular treatment fails or is judged as technically difficult or unfeasible, a laparoscopic approach is a reasonable alternative option. A recent study comparing embolization with laparoscopic IMA ligation proved that both procedures are safe and feasible, but the latter is associated with less risk of reintervention. 4 When the IMA is not ligated at its origin, particularly in obese patients or when the aneurysmatic sac is large, residual feeding vessels can maintain endoleak progression. Precise identification of the vascular anatomy and assessment of colonic perfusion using near-infrared indocyanine green (ICG) video angiography can help to avoid bowel ischemia and to reduce the risk of reoperation.
Patients and Methods
A review of our prospectively collected database identified 3 patients with persistent type II endoleak, 2 men and 1 woman with a median age of 82 (range 81–82) years, who underwent primary laparoscopic clipping of the IMA between February and October 2018. All patients had previously undergone uneventful EVAR for an abdominal aortic aneurysm (diameter 75, 59, and 43 mm, respectively). Follow-up by a dedicated team of vascular surgeons included CT scan at 1 and 12 months or whenever needed based on the clinical suspicion of endoleak. Each patient was discussed by a multidisciplinary board with interventional radiologists, vascular surgeons, and general surgeons. Indications for reintervention were sac expansion associated with abdominal pain in 1 patient, and asymptomatic persistence of the endoleak with progressive enlargement up to 10–15 mm in the remaining patients. Informed consent for each surgical procedure was obtained.
The operation was performed under general anesthesia through a laparoscopic transperitoneal approach. The pneumoperitoneum was induced through a Veress needle. A 12 mm optical trocar and three additional trocars were used to achieve adequate triangulation. The aneurysmatic sac was identified and the retroperitoneum was opened just above the sacral promontorium. The IMA was dissected up to its origin, proximally to the takeoff of the left colic artery. After temporary IMA clamping, ICG was injected intravenously at a dose of 0.25 mg/kg to check for the absence of backflow to the aneurysmatic sac and to ensure that the left colon was well perfused. The IMA was then doubly ligated at its origin using nonabsorbable 10 mm clips (Hem-o-lok®) (Figs. 1 and 2), and the technical success of the procedure was again determined by assessing the absence of fluorescence enhancement of the aneurysmatic sac and the normal perfusion of the left colon. The follow-up was conducted at 1 year through CT angiography or duplex ultrasound.

Isolation of the inferior mesenteric artery (left upper); after intravenous injection of indocyanine green, both the main trunk and the left colic vessels are visualized (right upper); temporary clamping of the inferior mesenteric artery (lower images).
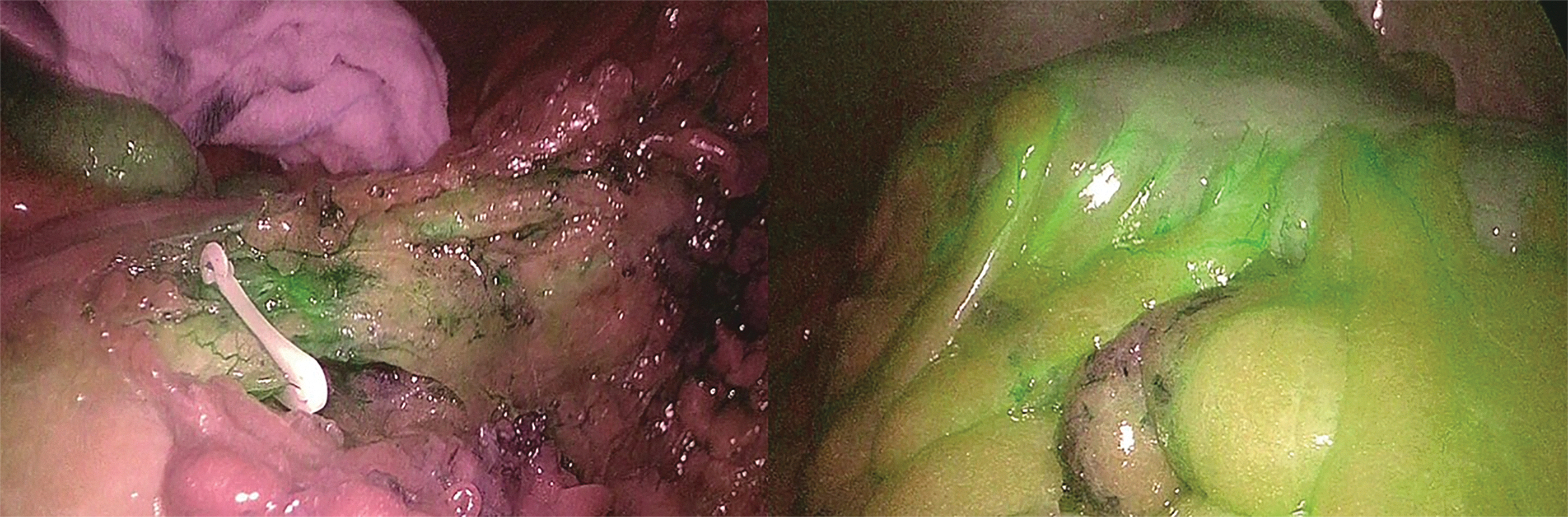
Clipping of the inferior mesenteric artery and evidence of satisfactory bowel perfusion (right).
Results
The mean operative time was 58 ± 9 minutes. Exploration of the abdominal cavity confirmed the presence of the aneurismatic sac without active bleeding in all patients. There were no procedure-related complications and no hypersensitivity reactions nor other side effects associated with ICG dye administration occurred. All patients were discharged home on postoperative day 1 and are currently asymptomatic and free of recurrence at a mean follow-up of 15 months.
Discussion
The term endoleak appeared in the medical literature in 1996 when White et al. 5 first described an “incomplete aneurysm exclusion by an endoluminal graft.” In a recent large cohort including 545 patients, the incidence of type II endoleak was 18.9%, representing the most common subtype. 6 Most type II endoleaks occurring after EVAR are benign, and rupture of the aneurysmatic sac has been described in 0.9% of patients. 2 Current guidelines recommend that type II endoleaks should be treated when the sac diameter expands >10 mm during follow-up. 7 However, management of type II endoleak is not standardized. The efficacy of preoperative IMA embolization to prevent this complication is still debated8–10 as it has been associated with prolonged radiation exposure, renal failure due to intravenous contrast administration, ischemic colitis, and paraplegia due to spinal cord ischemia. 11
Laparoscopic clipping of the IMA performed in centers with expertise in laparoscopic surgery has been reported as a definitive treatment if no additional feeding branches, such as lumbar arteries, have been identified at preoperative CT.11,12 A recent review, 13 including 13 studies for a total of 40 patients, found an overall procedural success rate of 90% and a recurrence rate of 22.5% over a mean follow-up of 37 months. Of interest, 35% of these patients had previously undergone failed endovascular interventions. Near-infrared fluorescence imaging using ICG has proven to be safe and helpful to identify vascular anatomy and tissue perfusion in esophagogastric, colorectal, and liver surgery. 14 In patients with type II endoleaks, use of near-infrared ICG angiography allows easy detection of the main trunk of the IMA, which could be demanding at surgical exploration due to the distorted anatomy and a dense inflammatory retroperitoneal reaction surrounding the aorta and the endovascular graft.15,16 In addition, IMA clamping allows to check reduced fluorescence in the aneurysmatic sac and preservation of left colonic perfusion.
Through collaboration of vascular and general surgeons in specialized centers, laparoscopic clipping of IMA represents a safe treatment for selected patients with type II endoleak. ICG angiography has the potential to increase surgical accuracy and should be part of the process of anatomical identification and confirmation of the technical success of the procedure.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.