
Abstract
Background:
Simulation plays an important role in surgical training. We developed a simulator for laparoscopic ventral hernia repair (LVHR) surgery based on porcine tissue, characterized by low cost and high reality.
Methods:
Our LVHR model is based on porcine tissue mounted in a human mannequin. The anterior abdominal wall is constructed to allow laparoscopic training. Training sessions are conducted in a simulated operating room environment.
Results:
During preliminary tests, the LVHR simulator was found to be highly realistic in terms of tissue feedback, instrumentation usage, and performing the key steps of the LVHR procedure. The model was evaluated as a very useful tool for residents' training allowing to gain laparoscopic skills, learn the key steps of LVHR, and practice team work.
Conclusions:
Our simulator, based on porcine tissue mounted in a mannequin, offers a very realistic and cost-effective model for simulating LVHR surgery.
Introduction
There is agreement that simulation training in surgery is very valuable. By enabling practice in simulated, standardized and safe conditions, it allows trainees to improve their technical skills without jeopardizing patients' care.1,2 It may also be a remedy for barriers that surgery residents encounter in their training such as downregulated work hours, limited operating room time, and health care safety policies. 3
Same as in many other minimally invasive procedures, the laparoscopic ventral hernia repair (LVHR) requires proficiency in basic and advanced laparoscopic techniques. Available surgical simulation modalities involve box trainers, virtual reality (VR) simulators, cadavers, and live animals. Each of these is characterized by specific limitations. Box-lap trainers can only simulate a variety of basic skills, including laparoscopic suturing, knot-tying, and coordination drills. 4 VR technology, while being a very useful and promising tool, has a high initial cost and lack of real tissue and instruments haptic feedback. Using cadavers and living animals in surgical simulation most closely approximate reality but its usefulness in LVHR training is limited not only by high costs and ethical aspects, but also by inability to simulate features of the disease itself.
The aim of this study was to describe the technical aspects of our new simulator for LVHR.
Methods
The University of North Carolina (UNC) LVHR simulation model is based on porcine tissue purchased in a slaughter house, including: (1) square 10″ by 10″ abdominal wall block harvested from pig's flank, including skin, subcutaneous tissue, fascia muscular layer, (2) a separate square 12″ by 12″ parietal peritoneum cleared from excessive preperitoneal fat, and (3) a 20″ long segment of the small intestine. All biological components are stored in a freezer. Although the quality of tissue remains acceptable for several weeks, our experience shows that it is at its best during the first 2 weeks. Before a simulation session, the tissue requires 24-hour defrosting in the refrigerator.
Anatomical modifications are performed on the block by excising a round opening in the innermost muscle layer surface with a diameter of 1.5″ to imitate the abdominal wall defect. A space for the hernia sac is created between the innermost muscle layer and the skin using blunt dissection. Next step of the preparation requires positioning of the peritoneum on the internal surface of the muscle and pushing the peritoneum through the created abdominal wall defect to imitate the hernia sac. A collagen-based glue is used to fix the peritoneum and stick the tissues together. Our experience showed that the best way to get an optimal adhesion is to sprinkle the glue powder on tissues, instead of preparing the water/glue solution. Next, the intestine and inside surface of the hernia sac are covered in glue powder and three loops of bowel are placed inside to fill the entire hernia sac.
After positioning of the tissue components, the whole block is placed in a zip-lock bag to prevent drying and placed in the refrigerator (40°F) for at least 6 hours to allow the adhesive to solidify. The tissue block should be used within 72 hours after being prepared. At the day of training, the tissue block is dyed with artificial blood (crime scene thin blood; Manhattan Wardrobe supply) and mounted in a human mannequin, in which the hard cover made of plastic is the base structure (Fig. 1).

UNC LVHR simulator mannequin (1). LVHR, laparoscopic ventral hernia repair; UNC, University of North Carolina.
The anterior abdominal wall cover is constructed with a Smooth-On product (Dragon Skin FX-Pro) that is poured into a thin sheet about 0.25″ thick and attached to the mannequin with Velcro straps to secure it in place. The thickness of the silicone also allows for the placement of laparoscopic trocars for laparoscopic training. To imitate insufflation and allow for the performance of the laparoscopic procedure on the anterior abdominal wall, we constructed the cover using a pregnant mannequin form (Fig. 2).

UNC LVHR simulator mannequin (2). LVHR, laparoscopic ventral hernia repair; UNC, University of North Carolina.
The tissue block is positioned on the anterior cover with the hernia defect in the midline. A pediatric coagulation pad is placed between the cover and the tissue block in appropriate distance from the hernia to allow for dissection and suturing. The tissue block is then mounted to the cover with multiple sutures placed evenly on the entire contact surface (Fig. 3).
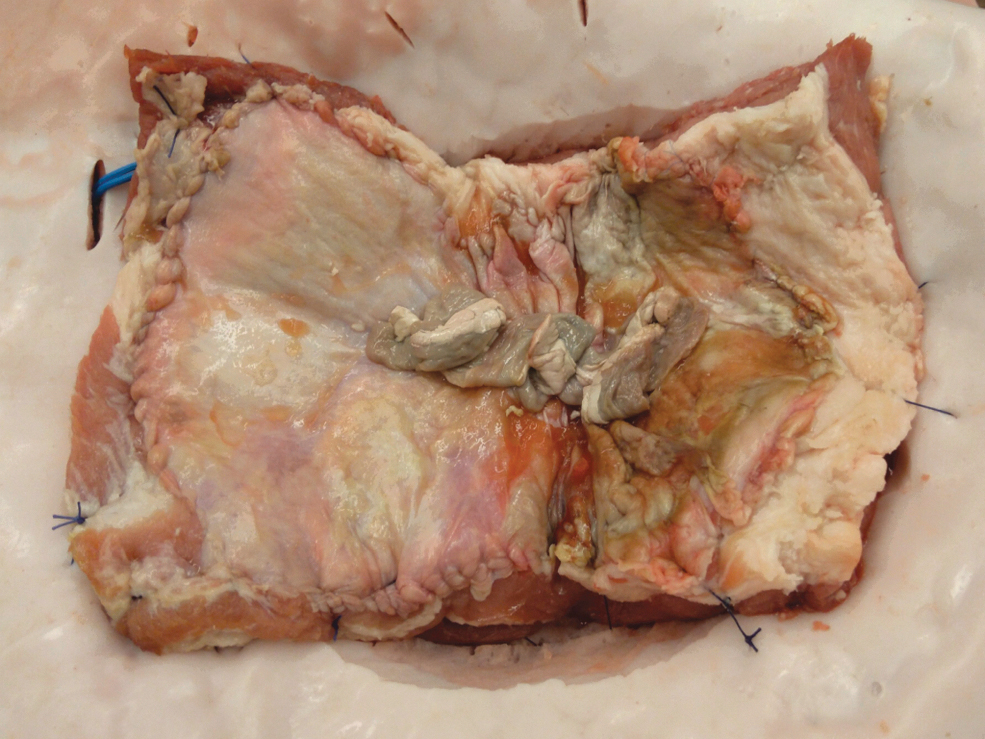
Tissue block mounted in the mannequin.
The room is finally set up the same way as the OR to simulate a clinical environment involving: operating table, Mayo stand with instruments, laparoscopic tower with a 30° scope and monitor, electrocautery unit, and suction tubing to evacuate smoke (Fig. 4). We additionally use a second monitor to simulate patient's vital signs and sounds using a simulation software (National Instruments, LabVIEW).

Simulated operating room set up for training session.
Results
The initial cost of the simulator (mannequin torso, silicone-based abdominal wall, tissue block, glue, and artificial blood) is about $300. All the laparoscopic instruments are disposable, and can be washed and reused. Once the initial expenses are covered, the simulator cost is $50 for each surgical training session (tissue block, glue, and dye).
The simulator is suitable for simulating all of the LVHR key steps. It enables performing the entire procedure utilizing real surgical instruments, giving the best possible feedback to the trainee. It facilitates acquiring basic skills common to all laparoscopic procedures like operating room ergonomics, locating the appropriate site for skin incisions and trocar placement, navigating the laparoscope to achieve the proper exposure, and instrument handling (Fig. 5). Furthermore it allows performing advanced steps of hernia repair such as adhesiolysis, excision of the hernia sac (Fig. 6), defect measurement, defect closure using a laparoscopic suture passer (“shoelacing” technique) 5 (Fig. 7), positioning of the mesh, and adjusting for appropriate internal and external counterpressure for appropriate fixation methods (Fig. 8).

Laparoscopic view of the simulator.

Excision of the hernia sac.

Closure of the hernia defect using the shoelacing technique.

Tacker mesh fixation.
Discussion
Nowadays, training in surgery faces many obstacles. Among these, one should mention reduced resident work hours, pressure of operating room time efficiency, more technically demanding procedures, and increasing number of lawsuits. All these factors, when added up, lead to decrease in the faculty's ability to transfer knowledge to residents during procedures. In these conditions, surgical simulation becomes an extremely important element of training.
Our goal was to develop a simulator that gives residents the opportunity to train in a realistic environment and at the same time would be relatively inexpensive and easy to use on a weekly basis. The majority of surgical simulation programs are focused on teaching only basic skills.6,7 Box-trainers give opportunity to develop essential psychomotor abilities, while being cheap and easy to maintain. For the last decade, along with the development of technology, VR simulation is gaining increasing popularity. 8 VR simulators, in addition to simple skills, provide the opportunity to simulate entire surgical procedures. 9 It was reported that VR training increases residents' surgical performance in the OR.10,11 Cadaver training is the best way to simulate anatomical features of surgical procedures, giving the trainee real tissue and instrument feedback. However, this type of simulation is linked to many difficulties such as high cost, low availability, risk of infection, and inability to simulate ventral hernias in standardized conditions, leading to reduced usability.
Our simulator based on porcine tissue, mounted in a space comparable to an insufflated human abdominal cavity, has similar surgical anatomy to humans. Porcine models have proven to be a valuable tool to learn complex laparoscopic procedures.12,13 Our preliminary tests indicate high realism in terms of operative space, tissue compliance, and haptic feedback while using laparoscopic instruments, making it an excellent training tool for surgical residents. LVHR is considered to be a demanding procedure requiring advanced laparoscopic skills. We believe acquiring proficiencies, such as dissection, suturing, mesh positioning and fixation, using our model, could reduce learning curve for LVHR.
Evaluations of LVHR simulation training has shown decreased numbers of errors and failure among trainees. 14 Many features found in the model developed by Seagull et al., has proved simulation effectiveness in increasing trainees level of confidence during the procedure. 15 In addition, training in a simulated OR setting may help to increase leadership skills and promote team work as it was reported in trauma care simulation. 16 For our training sessions, we set up our model in the simulated OR, where a complete surgical team is trained: surgeons, assistants, and scrub nurses. As surgical simulation still has many financial barriers, especially in low-income countries,17–19 our simulator provides a very cost-effective and reproducible model, with minimal financial burden.
This is a preliminary report and we do acknowledge some limitations. The model was evaluated only by surgeons involved in designing and developing the simulator, among which only one was an expert in minimally invasive hernia surgery. Regarding the simulator, one of the problems we faced was the inability to simulate tissue bleeding. Further testing by a larger group of experienced surgeons, as well as trainees, will be the next to determine the value of this simulator for training.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.