
Abstract
Objective:
Currarino syndrome (CS) is characterized by the triad of sacral anomalies, presacral tumor, and anorectal malformation (ARM). This study evaluates the feasibility and outcomes of laparoscopic-assisted anorectal pull-through (LAARP) for CS.
Materials and Methods:
Children admitted for primary or redo repair of CS through LAARP between 2016 and 2019 were reviewed. The indication of redo included constipation with megarectosigmoid, residual presacral mass, anastomosis leak, and secondary fistula. ARM was corrected by excision of rectal stenosis, fistula, and its associated megarectosigmoid. This was followed by a complete surgical resection of the presacral tumor, with subsequent pull-through and anocolic anastomosis. This was done with a combined laparoscopic and transanal approach. The detailed surgical techniques, early postoperative complications, and mid-term functional outcomes were summarized.
Results:
Fourteen patients underwent LAARP for primary (N = 4) and redo (N = 10) repair of CS. Four of them had colostomy previously. Mean age at operation was 20.7 ± 13.9 months. Mean operative time was 120 ± 25 minutes. Median hospital stay was 8 days (range 7–9 days) postoperatively. None of the patients developed early postoperative complications such as anastomotic leaks, presacral abscesses, recurrent fistulas, and residual mass. Bowel function was assessed 1 year after LAARP in 10 patients. Mean follow-up time was 15.9 months. The frequency of bowel movements was 3.3 ± 1.5/day. Constipation occurred in 2 patients. Occasional soiling (<3 times/week) was reported in 4 patients and frequent soiling (>3 times/week) was in 1.
Conclusion:
LAARP for CS is safe and effective.
Introduction
Currarino Syndrome (CS)1,2 is a rare congenital malformation that presents with a triad of sacral agenesis most frequently hemisacrum, anorectal malformation (ARM) most commonly in the form of anorectal stenosis, and a presacral mass such as a teratoma, hamartoma, or anterior meningocele.
More than 50% of CS cases are familial with an autosomal dominant inheritance. Mutation of the motor neuron and pancreas homeobox 1 (MNX1) gene has been identified in almost all familial and 30% of sporadic cases.3–6 However, the incomplete penetrance of the mutations results in a significant intrafamilial and interfamilial phenotypic heterogeneity. Not all CS cases demonstrate the classic triad (complete CS). Some patients present with sacral anomalies with an ARM or presacral mass (mild CS) and some cases present with a hemisacrum only (minimal CS). 7 It is not uncommon for CS to be associated with other anomalies such as Hirschsprung's disease (HD).8,9
Appropriate treatment of CS relies on the correct diagnosis and complete management of the conditions of the triad. The presacral mass requires surgical excision, most commonly through a posterior sagittal approach. Anorectal stenosis can be treated with dilatation. The stenosis refractory to conservative management or imperforated anus requires limited or standard posterior sagittal anorectoplasty (PSARP) to repair the ARM and resect the presacral mass simultaneously.10–12 However, due to the rare nature of the disease and the nonspecific presentation (constipation) of CS, it is often misdiagnosed and receives inappropriate treatment. Incomplete treatment would probably (1) worsen constipation and megarectosigmoid, which can be ascribed to distal obstruction and inadequate treatment of constipation,13,14 and (2) leave an untreated or residual presacral mass. Such patients would require redo surgery. Conventional PSARP provides good exposure but can be difficult in redo surgery because of extension of the surgical scar and adhesions formed from previous surgery. Ligation of high fistula, mobilization of megarectosigmoid, and pelvic extension of the presacral mass are also challenging to perform through PSARP. Furthermore, PSARP requires cutting through and subsequent suture repair of the anal sphincter complex, which may affect the postoperative functional outcome.
To overcome the limitations of conventional surgery, we performed laparoscopic-assisted anorectal pull-through (LAARP) for our CS patients. In this study, we reported our surgical experience and postoperative outcomes of LAARP for CS, especially in redo cases.
Materials and Methods
Patients with CS admitted to the surgical unit of a national tertiary pediatric center in China from 2016 to 2019 were reviewed. Ethics approval from the Ethics Board of the Capital Institute of Pediatrics (China) was obtained. Written consent was obtained from the patients' parents before surgery.
Patients were placed supine in the Trendelenburg position. The entire abdomen and lower limbs were draped. A 30° laparoscope (26046BA; Karl Storz GmbH & Co. KG, Tuttlingen, Germany) was inserted through an umbilical port. Two working ports were placed at the bilateral borders of the rectus muscles at the umbilical level. Carbon dioxide pneumoperitoneum was established with a pressure between 8 and 12 mmHg.
For presacral tumor and anorectal stenosis with megarectosigmoid
The grossly dilated rectum and/or sigmoid was mobilized with laparoscopic harmonic scalpel and diathermy. The rectosigmoid mesentery was divided while carefully preserving the marginal artery. The mobilization was carried out until the proximal end (above the dilated bowel) was able to be retracted deep into the pelvis without tension. Distal dissection was performed close to the rectal wall before reaching the peritoneal reflection anteriorly, and 2–3 cm below the peritoneal reflex posteriorly. The child was then repositioned to a lithotomy position and endorectal pull-through was performed. The perineal dissection was started 1 cm above the dentate line. The anterior rectum was mobilized at the submucosal plane and the posterior rectum was mobilized at full thickness in the Swenson-like plane until the pelvic cavity was reached and bowel could be pulled through. After resection of the rectal stenosis and its associated megarectosigmoid, the proximal end of the colon was then closed temporarily and returned to the abdominal cavity to expose the presacral space for mass resection (Fig. 1). Small and low presacral masses (below S3) could be resected through a transanal approach, while large and high presacral masses (extending above S3) would need dissection from both transanal and laparoscopic approaches (Fig. 1). If further laparoscopic dissection was required, the anal canal would be packed with gauze to maintain the pneumoperitoneum. After complete excision of the presacral mass, the transected bowel was pulled through again, and anocolic anastomosis was performed. A frozen section was performed before anastomosis to ensure the presence of ganglion cells at the anastomotic site.
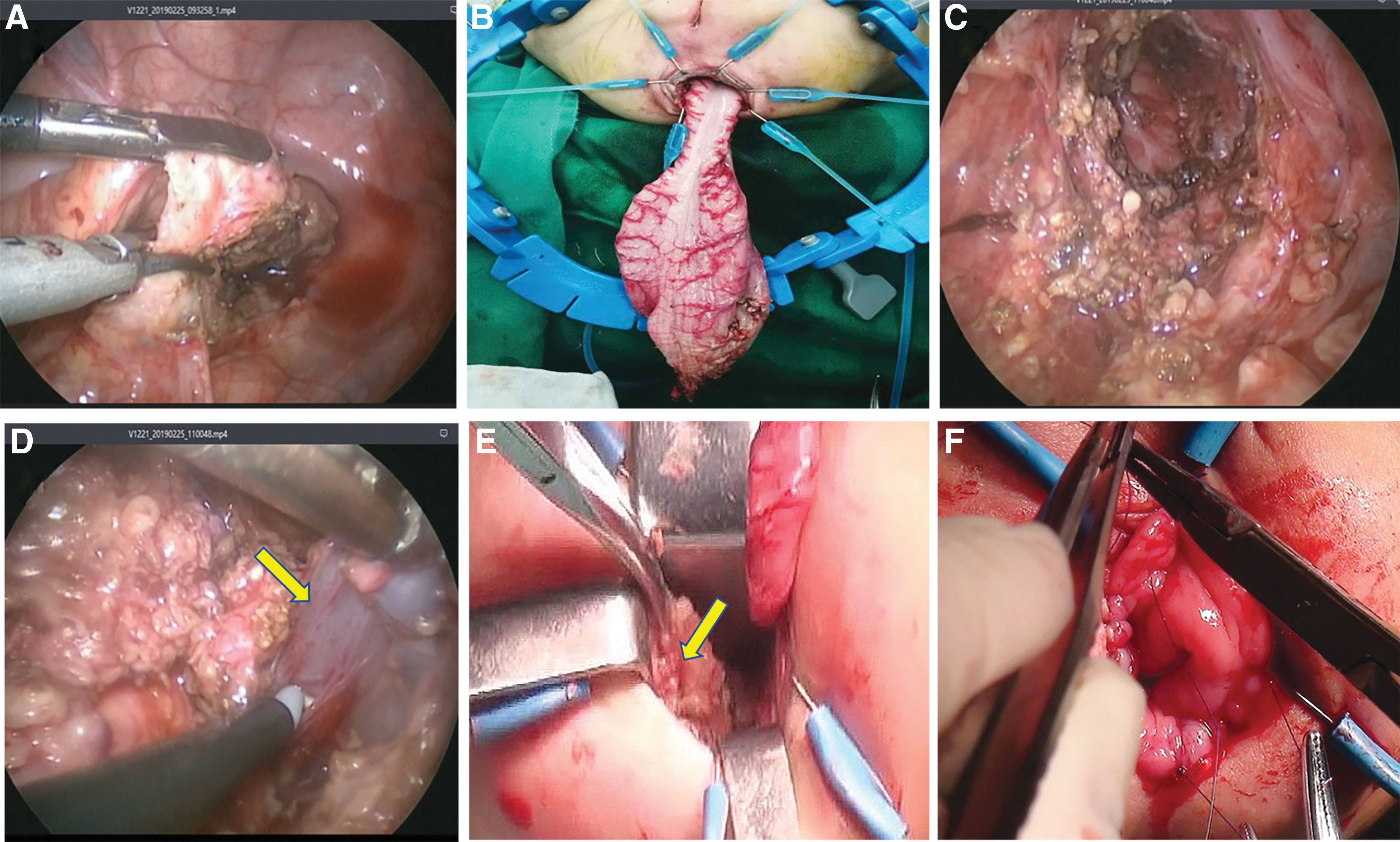
LAARP for Currarino syndrome.
For presacral tumor and imperforate anus with rectouretheral, rectovaginal, rectoperineal fistula, or without fistula
The distal dilated rectal pouch with/without fistula was mobilized through laparoscopic-assisted technique as previously reported.15–18 The center of the external sphincter was mapped using a transcutaneous electrostimulator externally. The midline incision was made at the site of the proposed anal orifice and extended posteriorly 1–2 cm (limited PSARP) for resection of the presacral mass, anoplasty, and duroplasty (if present of anterior sacral meningocele). The rectum was then pulled through the tunnel to the perineal wound. Grossly dilated distal rectum was then excised followed by an anocolic anastomosis.17,18
Some patients developed dermoid-cutaneous fistula or acquired rectocutanous fistula iatrogenically. For such cases, the internal opening and the tract of the fistula has to be resected completely together with the presacral mass and rectum. The pulled-through bowel would cover the resected fistula bed. The external fistula opening can be left open to heal spontaneously.
Postoperatively, patients were given broad-spectrum antibiotics for 3–7 days. Oral clear fluids were permitted once the child passed flatus. Anal dilatation started on postoperative day 14, and continued for a period of 3 months.
Patients were followed up at 3, 6, 12, and 24 months after surgery. The outcome measures included both postoperative complications (anastomotic stricture, rectal prolapse, fistula, and tumor recurrence) and functional outcomes (constipation, soiling, and urinary retention). In this study, constipation was defined as the voluntary bowel movement less than twice per week for at least 2 weeks. Soiling was defined as involuntary leaking of small amounts of stool or liquid requiring change of underwear or diapers. Soiling was considered occasional if it occurred once or twice per week, and frequent if thrice or more per week.
Statistical analysis
The data were analyzed using SPSS® software version 19.0. (IBM Corp. Released 2010. IBM SPSS Statistics for Windows, Version 19.0. Armonk, NY: IBM Corp.) The data were presented as mean ± standard deviation.
Results
Between 2016 and 2019, 14 children with CS underwent LAARP in our center. As shown in Table 1, all 14 children presented with the triad of complete CS except 1 patient, who presented with sacral agenesis and anorectal stenosis only (mild CS). Typical presentation of Currarino triad was shown in Figure 2. Anorectal stenosis with special appearance of funnel anus (Fig. 2) was the most common (8 cases) type of ARM, followed by ARM with rectoperineal fistula (3 cases), ARM with rectovaginal fistula (1 case), ARM with rectourethral fistula (1 case), and high ARM without fistula (1 case) (Table 1).
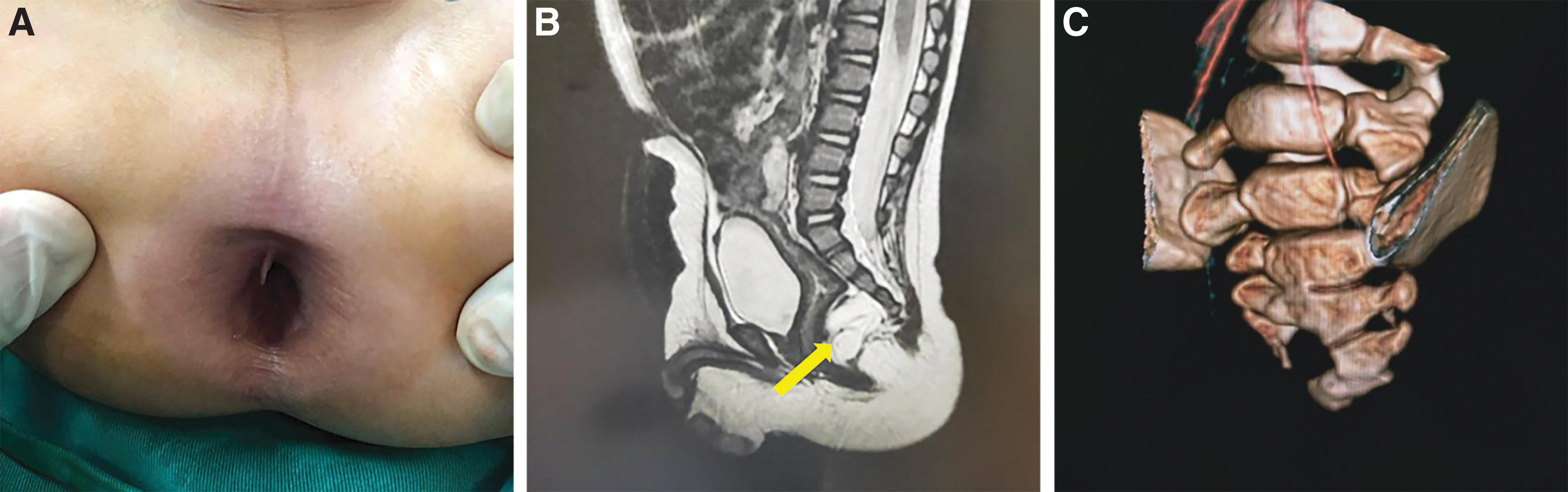
Typical presentation of Currarino triad.
Case-Specific Details, Including Presenting Features and Surgical History
ARM, anorectal malformation; CS, Currarino syndrome; LAARP, laparoscopic-assisted anorectal pull-through.
Five cases were found to have familiar inheritance. Three underwent genetic testing and two were identified to have MNX1 mutation.
Most of the patients (10 cases) received incomplete perineal surgery in other hospitals before definitive repair. These included 5 cases of resection of presacral mass through a posterior sagittal approach (incomplete resection in 4 of them), 1 case of LAARP for ARM without resection of presacral tumor, 4 cases of anoplasties (cutback) for anorectal stenosis (2 cases) or rectoperineal fistula (2 cases). Neurological surgeries (tethered cord detethering and duraplasty) were performed alone or in combination with presacral tumor resection or anoplasty in 4 patients. Three patients only had colostomy without perineal surgery and one had colostomy after anoplasty because of the refractory constipation (Table 1).
All of the patients without colostomy presented with severe constipation with megarectosigmoid before definitive repair. HD was found in 2 cases in subsequent surgery.
All patients successfully underwent definitive repair by LAARP, except for 1 case which required conversion to open surgery. Mean age at laparoscopic-assisted repair was 20.7 ± 13.9 months (range 3–48 months). Mean operative time was 120 ± 25 minutes (range 90–150 minutes). Median hospital stay was 8 days (range 7–9 days). All patients recovered uneventfully without cerebrospinal fluid (CSF) leak, CNS infection, anastomotic leak, postoperative bleeding, presacral abscesses, strictures, prolapse, recurrent fistula, or residual mass.
Bowel function was assessed 1 year after operation in 10 patients. The follow-up period was 15.9 ± 3.3 months (range 12–22; age range 23–61 months). As shown in Table 2, the mean number of bowel movements was 3.3 ± 1.5/day. Two cases (20.0%) developed constipation. Occasional soiling (<3 times/week) was reported in 4 patients, and frequent soiling was in 1 (>3 times/week) (Table 2). No cases developed complete loss of bowel control or urinary retention.
Patient Characteristics and Postoperative Outcome
CSF, cerebrospinal fluid; LAARP, laparoscopic-assisted anorectal pull-through; SD, standard deviation.
Discussion
CS is a rare congenital disease, which mainly presents with refractory constipation.11,19 The constipation is caused by the combined effect of the triad in CS: the anorectal stenosis or rectocutaneous fistula from ARM, pressure effects from the presacral mass, and neurological deficit from sacral agenesis.11,19 Furthermore, wide variation is reported in the prevalence of megarectosigmoid (10%–50%) in ARM patients, and distal obstruction and inadequate treatment of constipation are recognized as important pathogenic factors of megarectosigmoid,13,14 which compromises the peristalsis and in turn provokes a more severe constipation.
A proper treatment of CS requires addressing all the pathogenetic factors that induce constipation, including complete resection of presacral mass, repair of the ARM, correction of neurological deficits, and management of megarectosigmoid.
Conventional limited or standard PSARP are commonly used to treat CS.10–12,19 Although PSARP provides a good exposure for ARM repair and resection of a lower presacral mass, we found some limitations in previous cases. First, the rectum occupies the presacral space, which makes dissection of the upper border of a large presacral mass very difficult. Second, the mobilization of the proximal rectum and sigmoid colon is often insufficient through PSARP approach, leading to excessive tension at the anastomosis. Third, PSARP requires splitting and suturing back of the sphincter complex, which would be exceptionally difficult in redo cases and predispose to wound complications and poorer functional outcomes.
In this cohort, 5 patients had undergone excision of a presacral mass in another hospital before admission to our center. Eighty percent of the patients (4/5) still had a residual tumor. All the redo cases were performed through LAARP. LAARP allows full mobilization of the presacral tumor in pelvis. Furthermore, after resection of rectum and megacolon laparoscopically, the presacral place can be fully exposed for dissection of a low siting presacral tumor transanally. With combined laparoscopic and transanal approach, we managed to completely resect the presacral tumor in all of our patients. None of the patients had tumor recurrence or a residual mass during follow-up.
Apart from dissection of the presacral tumor, LAARP also demonstrated a few advantages in the management of the ARM.15–18 First, laparoscopic dissection allows resection of the megarectosigmoid, which is one of the main culprits of constipation after ARM repair. One previous histopathological and immunohistochemical study on ARM showed that dilated rectal pouches had distinct defects in the neuromusculature, which compromised its function as a reservoir and evacuation capability. 20 So, the grossly dilated rectum was excised for better outcome in the laparoscopic-assisted anorectoplasty.17,18 Moreover, many centers advocated to resect the megarectosigmoid for the refractory postoperative constipation.13,21,22 Second, laparoscopy can mobilize the mesocolon to a great extent while preserving the marginal blood supply to the bowel, which allows a tension-free anastomosis and prevents postoperative wound breakdown. Third, LAARP is associated with smaller wound and minimal trauma to the anal sphincter complex. It was reported that LAARP had lesser wound infection/dehiscence and lower incidence of constipation compared with PSARP for high/intermediate ARM.23,24
Although LAARP avoids cutting through the anal sphincter, it requires a lot of anal retraction which may stretch and injure the sphincter. We found that such injuries were transient and insignificant in our series. Out of 10 patients followed up for 1–2 years, only 4 had occasional soiling (<3 times/week), and 1 had frequent soiling for more than 3 times/week. The risk of fecal soiling is comparable with those who underwent PSARP procedure.10,25
Patients suspected to have CS require a thorough work-up to exclude a potential neural tube anomaly. Some reports advocated repair of the meningocele before correcting the anorectal anomalies to reduce the risk of meningitis. 26 Some authors described a single-stage procedure for repair of the meningocele and anorectal anomaly at the same sitting.11,12 We advocate a multidisciplinary consultation before operation and a combined surgery with a neurosurgeon for a single-stage procedure under protective stoma. Furthermore, tethered cord without meningocele should be treated in a staged manner in patients with CS.
Our study demonstrated that LAARP is a safe and effective method to treat CS especially for redo cases. However, this study is limited by its retrospective nature and a relatively short follow-up period. Furthermore, this study lacks objective measurements such as a clinical score or manometry for evaluation of functional outcomes. In the future, a prospective study with objective functional outcome measurements would be needed to support the findings of this study.
Footnotes
Acknowledgments
The author would like to thank Dr. Lin Yeachi and Dr. Chen Yong from KK Women's and Children Hospital, Singapore for constructive criticism and diligent proofreading of the article.
Ethics Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional Research Committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the National Natural Science Foundation of China (81700451).