
Abstract
Background:
Coelomic cysts are uncommon benign cyctic lesions of the mediastinum. Complete resection of the cyst with surgical treatment is indicated depending on whether the patient is symptomatic or whether the cyst grows during follow-up, or whether the diagnosis is uncertain. Surgical treatment prevents complications, relieves symptoms, and establishes diagnosis. Video-assisted thoracoscopic surgery (VATS) is the best method for excision of these cysts. This approach is safe and effective, has low morbidity, and shortens the length of hospital stay
Objectives:
We aimed to analyze our experience with coelomic cysts through VATS, reviewing clinical, radiological, and pathological features, early and long-term results of surgical management.
Patients and Methods:
Between January 2011 and December 2018, 20 patients with coelomic cysts who underwent VATS at our clinic were included in the study.
Results:
The study included 11 female and 9 male patients with a mean age of 45.6 years. Symptoms were present in 17 patients and 3 were asymptomatic. The average cyst diameter was 5.4 cm (range 2–8 cm). Fourteen of them were right sided, the others were left sided. There were no operative mortality and complications. Postoperatively there were no complications, in all cases course was uneventful, all of them were discharged after a mean of 3 days (range 2–6 days).
Conclusions:
Considering the low complication rate and hospital stay, excision of coelomic cysts through VATS is extremely safe and comfortable, so it should be considered the primary therapeutic procedure.
Introduction
Coelomic cysts are benign cyctic lesions of the mediastinum. They account for 7% of all mediastinal masses and 33% of cysts. Posterolateral or anterolateral thorocotomy and a median-sternotomy were used for excision of these cysts. In recent years, video-assisted thoracoscopic surgery (VATS) has developed. VATS has replaced posterolateral or anterolateral thorocotomy, and a median-sternotomy as a standard procedure for most of the thoracic operations such as lobectomy, wedge resection, and coelomic cysts excision.1–3 Our study analyzes the characteristic features of coelomic cysts with their location, symptoms, and VATS results.
Patients and Methods
The Medical Expertise Training Committee has reviewed and approved this study, and all the patients signed an informed consent form from January 2011 and December 2018. In total, 20 patients underwent VATS in our clinic for coelomic cyst. All lesions, regardless of location, were explored through VATS to complete resection. Chest roentgenography and computed tomography (CT) were used in all patients. Echocardiography was used in 10 (50%) patients to evaluate the intracardiac or pericardial relationship of the lesions. Investigated criteria were age, sex, symptoms, personal history, localization and size of the coelomic cyst, the morbidity and mortality rate, complications, and hospital stay times. Patient data were collected from inpatient clinic, surgical, outpatient clinic, and pathology laboratory records. Data analysis was performed using IBM SPSS® Statistics Standard Concurrent User V25 (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.).
Results
The study population included 9 males and 11 females, mean age 45.6 years (range 23–68). A total of 14 patients with typical localized coelomic cysts were included. Of these 14 cases, 7 had symptoms of dyspnea, 3 had chest pain, 2 had cough, and the remaining 2 patients had no symptoms. In 2 asymptomatic cases, incidental diagnosis was made after direct chest roentgenography and cyst size growth was detected in the follow-up (Fig. 1a, b). Of 6 patients with atypical localization of coelomic cyst (Fig. 2a, b), 2 patients had dyspnea and 3 patients had chest pain, and 1 patient was asymptomatic. Demographic data of patients are given in Table 1.
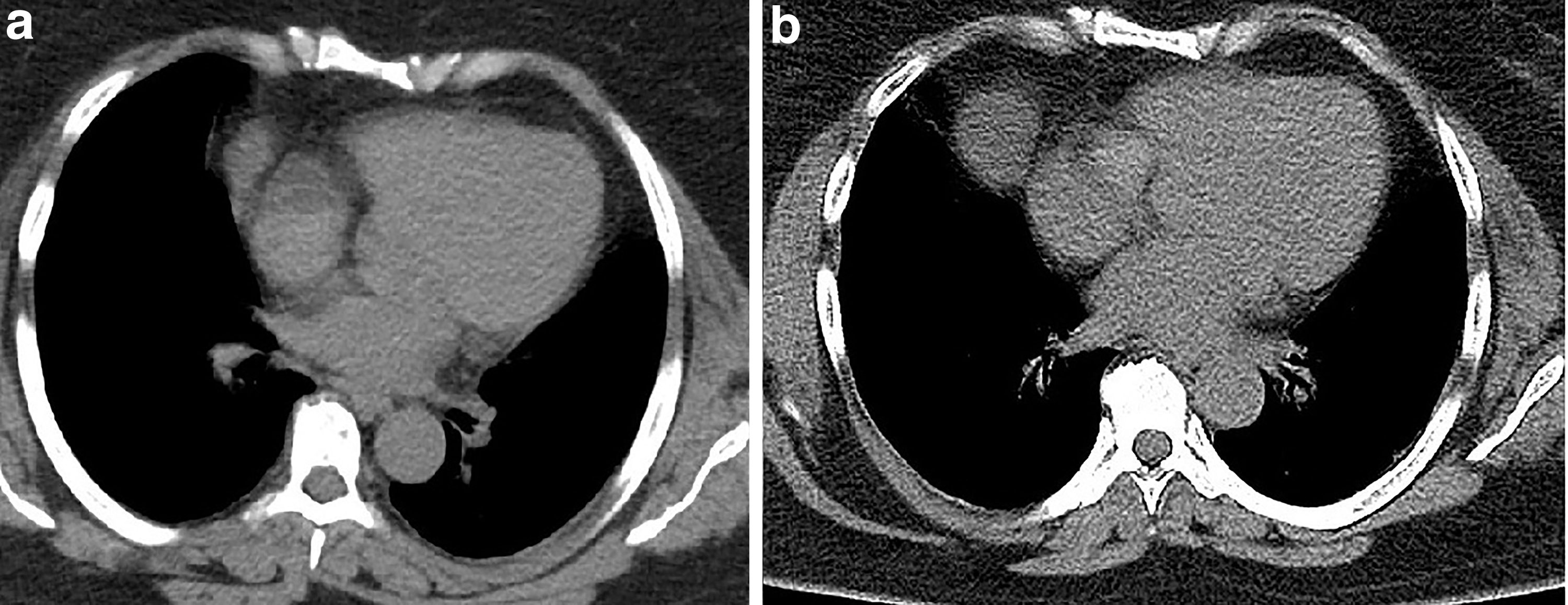
Thoracic CT shows growth of the right cardiophrenic coelomic cyst.

Thoracic CT images of atypical located coelomic cysts.
Demographics Data of Patients and Summary of Other Published Reports on Treatment of Coelomic Cysts
GA, general anesthesia; LA, local anesthesia; VAM, video-assisted mediastinoscopy; VATS, video-assisted thoracoscopic surgery.
According to chest roentgenography and CT scan, the localization of the cysts was along the right heart border in 12 (60%), the left heart border in 2 (10%), anterior–superior mediastinum in 4 (20%), paravertebral (posterior) mediastinum in 2 (10%) of the patients. The mean diameter of the cysts was 5.4 cm (range, 2–8 cm). No change was recorded in any patient after contrast injection. Resection of the cysts was decided due to the presence of symptoms in 12 patients, the diagnosis of the cyst remained uncertain in 6 patients, and increase in size during follow-up in 2 patients. Under general anesthesia, endobronchial intubation with a double-lumen tube provides single lung ventilation, the patient was turned in the lateral position: 20 patients were operated through VATS. Complete surgical excision was performed in all coelomic cysts. In 10 patients who underwent excision, the cyst contents were evacuated during dissection. In the remaining cases, the cyst content was not drained. A calcific walled cyst was completely excised without emptying the cyst content.
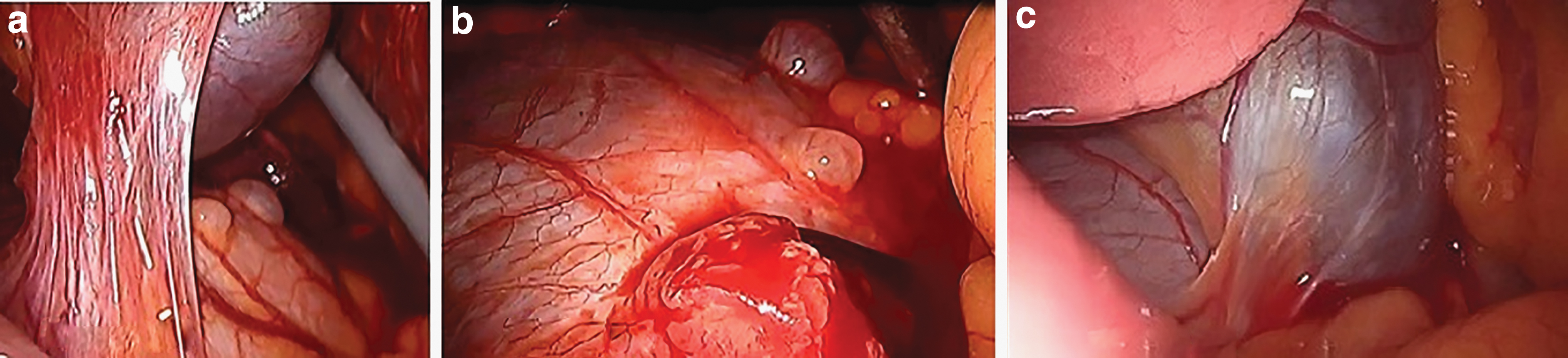
We detected multiple connection between a pericardial duplication in 1 patient through VATS (Fig. 3a–c). In 20 cases, the cyst comprised clear water-like fluid. In 1 case, the calcified walled cyst of 5 × 4 × 4 cm was filled with dark yellow material (Fig. 4a, b). All the cysts were lined with flat cuboid mesothelial cells. The mean postoperative chest tube removal time was 2 days (1–4 days). The mean hospital stay was 3 days (2–7 days). The mean observation time was 39.2 months (range 3–96). No recurrence was recorded and preoperative symptoms never recurred in any patient.
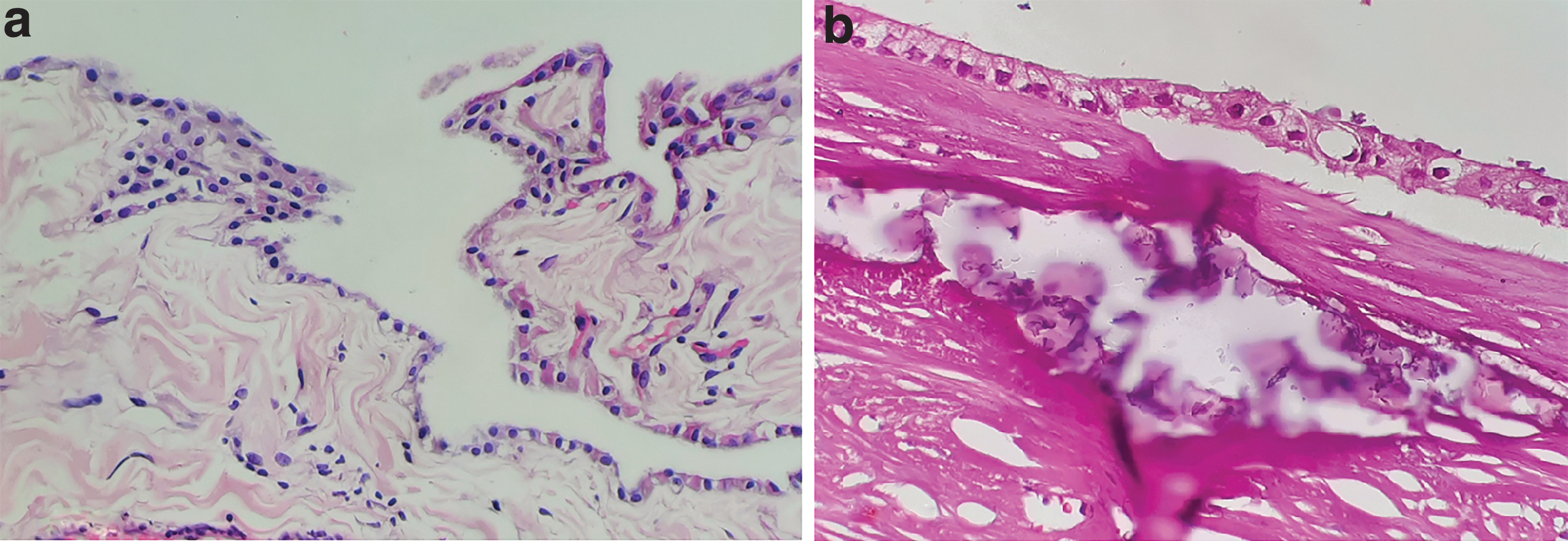
Pathological image of coelomic cysts.
Depending on age, gender, and size, there was no significant difference in terms of length of postoperative chest tube removal time and length of hospital stay.
Discussion
Benign masses representing 33% of all mediastinal cysts are coelomic cysts located in the mediastinum. 2 It is most commonly located in the right mediastinum (51%–80%) or left cardiophrenic angle (15%–38%), and sometimes occurs in other mediastinal areas (8%–11%) not associated with the diaphragm.4–8 Mediastinal coelomic cysts are seen in the third or fourth decade.4–8 In our data, the patients' mean age was 45.6 (23–68 years) and 55% were women. The average cyst diameter was 5.4 cm (range 2–8 cm) and 14 of them were right sided, the others were left sided. In our results, we found that most of the coelomic cysts (14/20; 70%) were in the visceral mediastinum near the heart. Coelomic cysts are mostly asymptomatic.9,10 In contrast, symptoms such as dyspnea, chest pain, and cough can be seen by pushing adjacent organs such as cardiovascular system and main bronchus.11,12 In our series, 9 patients admitted with dyspnea, 6 patients with chest pain, 2 patients with cough, and the others were asymptomatic. Also with the recent increase in the use of imaging procedures such as thoracic CT, the diagnosis of these lesions has further increased. There is no admitted consensus on the treatment of coelomic cysts. Many authors have maintained that even in asymptomatic patients, complete excision of the cyst is preferred because of the potential for complications such as enlargement of the cyst, spontaneous rupture, risk of torsion, and the possibility of inflammation.11,12 In the 2 cases, we observed growth of cyst. In 10 cases, intraoperative cyst was aspirated. In 1 case, postoperative pathology reported as calcified coelomic cyst. Thoracoscopic first coelomic cyst excision was performed in 1934 by Pickhardt. 13 In recent years, thoracoscopic surgery has been the most preferred method, with less muscle incision, less pain, and less hospital stay.14,15 All of our patients underwent VATS. In the surgical technique, the patients were placed in the lateral decubitus position after intubation with a double lumen tube. The first trocar incision for the camera was opened at the seventh or eighth intercostal distances in the anterior axillary line, and the other one or two trocars were placed in the best management position after visualization of the cyst. Cysts detected by thoracoscopy were excised by careful dissection with the help of thoracoscopic energy devices for hemostasis. During the dissection, we took care on keeping the cysts intact because it makes dissection easier, but in some cases we aspirated the cystic fluid. One of the most important point we took care was removal of the cystic mucosa lining completely during the dissection to prevent recurrence. And till today, all patients were free from recurrence. There was no operative mortality complications observed. Our prognosis after complete excision was excellent. No postoperative complications were observed. The mean duration of hospitalization in the postoperative period was 3 days (range 2–7 days).
Table 1 summarizes the other published reports on treatment of coelomic cysts.
In conclusion, in cases with typical localized coelomic cysts, if there is symptom, or if there is an increase in cyst size during follow-up, complete surgical resection is indicated and VATS is the best method. Excision with VATS should be performed in all cases with atypical coelomic cyst for diagnostic purposes. In recent years, complete resection of the coelomic cyst can be carried out successfully with VATS. So VATS should be indispensable in the treatment of coelomic cyst with low morbidity and mortality rates without any recurrence.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.