
Abstract
Background:
Rectal prolapse (RP) is primarily a disease of the elderly, where treatment may be associated with significant postoperative morbidity including that related to anesthesia.
Objective:
The aim of this study was to evaluate the safety and feasibility of a novel abdominal approach to RP repair under sedation and local anesthesia and to assess short- and long-term clinical outcomes in elderly patients (>70 years).
Design Settings:
This is a prospective pilot study with 10 patients using a novel RP repair. The anesthesia type was local or epidural with sedation. Follow-up was done at 30 days, 12, and 24 months.
Patients:
Patients were men and women >70 years of age with RP.
Main Outcome Measures:
(1) Feasibility: successful completion of RP repair using the novel abdominal approach with laparoscopic assistance. (2) Safety: safety was measured by the incidence of the intraoperative complications (bowel perforation, organ injury, and bleeding requiring blood transfusion). (3) Sedation and local anesthesia feasibility: surgery was safely completed without patient intubation.
Results:
Ten female patients >70 years of age underwent RP repair using the novel abdominal approach. General anesthesia was not required in any of the 10 patients. Two patients recurred within 6 months. One of the patients with recurrence of RP subsequently underwent laparoscopic rectopexy, and the other was minimal and required no further treatment. One mortality occurred at 3 months unrelated to the procedure. No other anesthetic or surgical intraoperative and postoperative complications were observed.
Limitations:
This is a single-institution pilot study.
Conclusions:
Abdominal RP repair under sedation and regional anesthesia appears feasible and safe in elderly patients and may, in the future, provide an effective alternative to current treatment options for RP, avoiding general anesthesia. ClinicalTrial.gov registration number: NCT01980043.
Introduction/Background
Rectal prolapse (RP) is a protrusion of the rectum outside the anus, most commonly affecting the elderly population even though it can present at all ages. The overall prevalence of RP is 2.5 of 100,000 population and the prevalence is 1% in people >65 years of age.1–4 Clinical symptoms include protrusion of the rectum, rectal bleeding, incontinence, constipation, mucous discharge, rectal pain, and tenesmus.2,5 Nonsurgical approaches such as dietary change, improvement of constipation and diarrhea, and use of nonsurgical devices such as the anal plug have been proposed but do not work. 6
The treatment of full-thickness RP is surgical. There are >100 different procedures described in the literature, divided roughly into abdominal and perineal approaches.2,7,8 The choice of treatment of RP is balanced between recurrence rate and morbidity, especially in older adults with multiple comorbidities. Abdominal techniques have shown low recurrence rates (11%) and higher morbidity, whereas perineal approaches have been associated with lower morbidity but a recurrence rate of at least 20%–30%.2,5,7–9 Postsurgical morbidity, including that related to anesthesia, is a particular concern in elderly patients who are susceptible to postoperative complications due to multiple underlying comorbidities.10–12 Elderly patients increasingly seek a procedure that will avoid general anesthesia that can potentially affect their mental status postoperatively. Despite some preference for perineal resection for elderly people, since it may be done under local or regional anesthesia, abdominal surgical repair, particularly using laparoscopic methods, has shown to reduce perioperative complications in both the general population and the elderly, partially related to less surgical trauma.13,14
An anterior abdominal wall approach (fixing the rectosigmoid to the abdominal wall) has been documented in the medical literature as early as 1930.15,16 Experimental studies using endoscopic fixation of the rectum to the abdominal wall in a porcine model has shown it to be feasible and safe and suggested an alternative to current RP treatment options.1,17 A novel combined endoluminal and local repair of RP under sedation and local anesthesia offers potentially a less invasive method of treating RP by (1) eliminating the need for general anesthesia, (2) avoiding bowel resection and large abdominal incisions, and (3) possibly shortening the hospital stay and having a faster recovery.
Aims/objective
The purpose of this study is to evaluate the safety and feasibility of a novel minimally invasive abdominal approach to RP repair under sedation and local or regional anesthesia in elderly patients. The secondary objective was to evaluate the short- and long-term clinical outcomes after this novel procedure.
Materials and Methods
This study was a prospective pilot study with 10 patients undergoing combined minimally invasive and endoluminal (colonoscopic) surgery under sedation and local anesthesia for RP repair for regular care at an academic medical center. Male and female patients 70 years of age or above with body mass index (BMI) <30 kg/m2, and American Society of Anesthesiologists Score (ASA) status between 1 and 3 were invited to participate in the study after surgery for RP was recommended for standard treatment of their medical conditions. Patients with previous abdominal surgeries including abdominal wall repair with mesh were excluded from the study. The study was approved by the institutional review board.
Surgical procedure
Under sedation in the operating room, the patient was placed in a modified lithotomy position with legs positioned in padded stirrups. The rectum was positioned for fixation against the abdominal wall using flexible or rigid sigmoidoscopy, identifying the anterior rectosigmoid wall with the scope and pushing this up against the abdominal wall with rigid scope. Then a small transverse Pfannenstiel type (3–5 cm) incision was made in the lower abdomen at the site of the scope pushing against the wall. Six to eight 2–0 polyester sutures were placed into the rectum at the fixation site, fixing it with a 3 × 6 cm piece of Gore-Tex DualMesh (GORE® DUALMESH®), Newark, DE (Fig. 1). Four size 0 polypropylene sutures were used to secure the mesh to the abdominal wall on the cephalad aspect of the Pfannenstiel incision. Before the end of the surgery, the abdomen was evaluated carefully, and subsequently the small incision was closed with size 0 Maxon interrupted sutures. The skin was closed with 4–0 Biosyn subcuticular sutures. Figure 2presents the steps of the procedure (Fig. 2). Postoperatively the patients were transported to the recovery room and admitted for an overnight stay in the hospital for postsurgical observation.

Abdominal approach of RP repair. RP, rectal prolapse. Image used with permission and created by Yuko Tonohira.
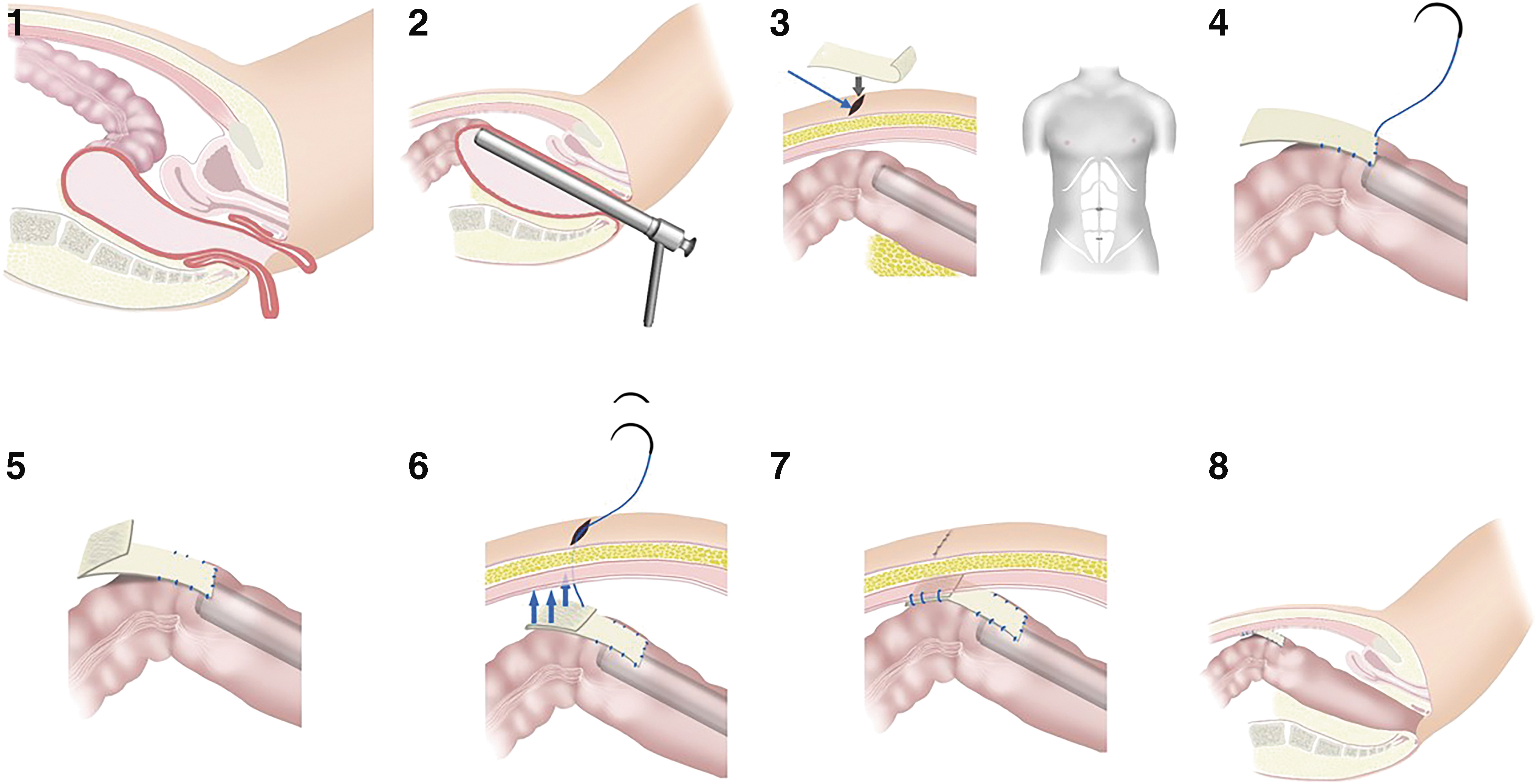
Abdominal approach of RP repair procedure steps: (1) RP; (2) using rigid scope to evaluate and push the rectum to the abdominal wall; (3) blue arrow points to the small transverse Pfannenstiel type (3–5 cm) incision in the lower abdomen below the umbilicus; (4) securing the Gore-Tex DualMesh to rectosigmoid; (5) secured mesh; (6) securing the Gore-Tex mesh to the abdominal wall using size 0 polypropylene sutures; (7) closing the skin incision; (8) completed abdominal approach of RP repair procedure. RP, rectal prolapse. Image used with permission and created by Yuko Tonohira.
Anesthesia procedure
Anesthesia was carried out as per standard of care using one of the three following anesthetic options. First, patients were offered spinal or epidural anesthesia using 0.75% bupivacaine (spinal) and 2% lidocaine (epidural) or intravenous sedation accompanied by local anesthesia administered by the surgeon at the abdominal site. If these two options were not medically or technically feasible, general anesthesia with endotracheal intubation was considered.
Outcomes
Primary outcomes definitions (Table 1)
Feasibility: successful completion of RP repair using the novel abdominal approach with laparoscopic assistance
Safety: measured by the incidence of the intraoperative complications (bowel perforation, organ injury, and bleeding requiring blood transfusion)
Sedation and local anesthesia feasibility: surgery completed without patient intubation
Clinical outcomes: RP recurrence within 30 days, length of hospital stay, and postsurgical complications; pain score before and after surgery on the scale from 0 to 10, 0 being no pain, 10 maximum pain
Long-term clinical outcomes: RP recurrence.
Data collection
Data were collected before, during, and after surgery by trained personnel. Demographic information (age, gender, BMI, and ASA), information about preoperative comorbidities, and previous abdominal surgeries were collected before the surgery. During surgery, data about the surgical procedure, operation time, estimated blood loss (mL), and intraoperative complications (bowel perforation, other organ injuries, and bleeding requiring a blood transfusion) were collected. The anesthetic evaluation included information about the type of anesthesia, intubation needed, breathing problems, and oxygen (O2) saturation <96% for >5 minutes. Pain score was evaluated before and after surgery on the scale from 0 to 10, 0 being no pain and 10 maximum pain. Postsurgical data collection included information about morbidity (wound infection, abdominal abscess, bleeding, intestinal obstruction, and bowel perforation) and mortality. Length of stay in hospital was measured from admission to date of discharge, and the postsurgical stay was measured from date of surgery to the discharge date. RP recurrence was evaluated at 30 days, 12, and 24 months. RP recurrence was defined as a protrusion of the rectum through the anus and verified by clinical examination.
Statistical analyses
Descriptive analyses were used to present the data. The results are reported in number and percentages. Measures of central tendency and dispersion were reported appropriately.
Results
Ten consecutive female patients were enrolled in the study. The results are listed in Table 2. The median age of the patients was 82 years old, with a range of 75–96 years. General anesthesia was not required in any of the 10 patients during surgery. No mental status changes were observed postoperatively. Two patients recurred with RP within 12 months after surgery. One of the patients subsequently underwent laparoscopic rectopexy for rectal relapse repair at 12 months after surgery. The second patient's prolapse was minor and has been tolerated well by the patient since then. One mortality occurred in the first 6 months unrelated to the procedure. No other anesthetic or surgical intraoperative and postoperative complications were observed.
Definitions of Outcomes
RP, rectal prolapse.
Results
ASA, American Society of Anesthesiologists Score; BMI, body mass index; MAC, monitored anesthesia care.
Discussion
This study evaluated a novel abdominal approach to RP repair, avoiding general anesthesia and using local or regional anesthesia with sedation. Although this is a pilot study, the results are promising as the procedure itself was feasible, without postsurgical complications. Our focus was surgical and anesthetic feasibility and safety. All patients had successful completion of RP repair using this novel abdominal surgical approach.
Some of the challenges of working with elderly people with RP are the surgical complications, avoidance of recurrence, and managing mental status changes related to surgical procedure and anesthesia. Using our approach, there was no postsurgical complication such as abscess, bowel obstruction, issues with the Gore-Tex mesh, or any other complications within 30 days. The low complication rate may be explained by a simple surgical procedure that avoids the need to work deep inside the abdominal/pelvic cavity. RP recurrence using abdominal approach has been quoted 8.2%–30%.18–20 Ricciardi et al. evaluated all patients who underwent surgical treatment for RP from the trackable California inpatient database and found that the risk of reoperation is substantial for both transabdominal (11%) and transperineal (11%) approaches. 21
Both recurrences in this pilot group occurred within 6 months. One patient subsequently underwent successful surgical repair of the recurrent RP using laparoscopic techniques. The reoperative laparoscopic rectopexy surgery was performed without intraoperative challenges or complications. There were no challenges during the port placement, as at the original surgery a small transverse Pfannenstiel type (3–5 cm) incision was made in the lower abdomen, which is anatomically away from the umbilicus (Fig. 2). Pneumoperitoneum was cautiously administered and abdominal cavity evaluated. Minimal adhesions were seen and the Gore-Tex mesh had become detached from the rectosigmoid, likely the cause for the recurrence of the prolapse. Indeed, in this case we were aware of a previous surgical technique, but with this novel approach of abdominal wall RP repair, we recommend the operating surgeon explain the procedure to the patient and the possible implications for future surgery. The other patient had a minor recurrence of RP that has been tolerated well without need for further treatment. Even though we used mesh in our approach, it is not clear from this pilot study whether the mesh plays a significant role in the support and the recurrence. Our study does not report any complication related to the mesh. Both recurrence patients are well at 24 months postprocedure.
An attractive aspect of the procedure was the avoidance of general anesthesia and endotracheal intubation. There are a number of studies demonstrating the negative effect of general anesthesia in elderly patients. A study on 406 patients showed that elderly patients >80 years undergoing abdominal surgery with general anesthesia had decreased survival after surgery. 22 Chung et al. reported that patients >80 years of age undergoing surgery with general anesthesia were at higher risk for postoperative respiratory complications compared with regional anesthesia. 23 Our study did not have any intraoperative anesthetic complications or postoperative complication related to anesthesia, suggesting that this is a safe approach for elderly patients undergoing RP repair.
General anesthesia may negatively impact cognition and independence in the elderly population. 24 It has been suggested that monitoring oxygenation and maintaining O2 saturation ≥96% during anesthesia reduces the cognitive decline after surgery.24,25 In our studies, patients were monitored continuously for O2 saturation and none had <96% for >5 minutes during surgery. All subjects reported zero pain during and after surgery, and the activities of daily living were restored within 2 days. As the elderly population usually has more comorbidities than younger patients, avoidance of general anesthesia with endotracheal intubation may help avoid postoperative complications.
The hospital length of stay compared with that in other studies was shorter. Patients were discharged from the hospital with a median length of stay in the hospital of 3 days, which is shorter than that in RP repair with general anesthesia with a median length of stay of 6 days.26,27 One patient stayed in the hospital for 10 days due to complex medical conditions before the surgery. Ultimately, less complications and faster discharge from the hospital will not only increase the quality of the care but also decrease the cost of hospitalization.
At 12 and 24 months, participating subjects reported 100% restoration of their usual daily activities and a high level of satisfaction (with an average of 9 on a 10 point satisfaction scale, 1 being the worst and 10 the best). Discussing the current alternatives of surgical repair of RP, several authors have reported that all techniques are associated with significant recurrence rates and comorbidities.18–21 The novel approach in this study offers a viable alternative with a low complication rate, acceptable recurrence rate, avoidance of general anesthesia, and relatively rapid discharge. Our research study has limitations, as it is only a single-institution pilot study. A larger sample study would provide more conclusive results related to the recurrence rate. Another limitation is that follow-up in our study was only 2 years, and longer follow-up (5 years) would provide additional information about the effectiveness of the procedure.
In conclusion, an abdominal RP repair under sedation and local or regional anesthesia, fixing the rectosigmoid to the abdominal wall appears feasible and safe in elderly patients. This approach may combine the higher success rate of an abdominal repair with the advantages of avoiding general anesthesia. Further research with powered studies is warranted.
Footnotes
Acknowledgment
The authors thank the medical illustrator Yuko Tonohira for drawing the procedure illustration.
Authors' Contributions
Conception and design were carried out by J.W.M., K.T., F.G., S.A., and K.A.G.; acquisition of data was by J.W.M., K.T., F.G., S.A., and K.A.G.; analysis and interpretation of data were performed by K.T., J.W.M., K.A.G., F.G., and S.A.; drafting the article or revising it critically for important intellectual content was done by K.T., J.W.M., F.G., S.A., and K.A.G.; and final approval of the version to be published was by J.W.M., K.T., F.G., S.A., and K.A.G.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by research grant from Olympus.