
Abstract
Background:
Standard treatments for nonparasitic hepatic cysts (NPHCs) include laparoscopic deroofing (LD), percutaneous aspiration, and alcohol sclerotherapy. However, these treatments have limitations. LD and alcohol sclerotherapy, for example, fail to prevent NPHC recurrences, although alcohol sclerotherapy is satisfactorily effective in treating small cysts (diameter <5 cm), which do not usually need treatment. The present study introduces a novel surgical procedure, laparoscopic enucleation with intact cyst (LEIC), which may prevent postoperative cyst recurrence.
Materials and Methods:
In this study, we enrolled 14 patients, with NPHCs larger than 9 cm in diameter, who underwent LEIC. Dissection and coagulation were performed using the harmonic shear enucleation and bipolar coagulation techniques. We attempted to completely remove the cysts intact.
Results:
For all patients, symptoms disappeared after complete elimination of the cyst capsule. No complications (hemorrhage or bile leakage) were found during the perioperative period. The mean follow-up period was 19.3 months (range 10–38 months), during which no recurrences or complications were noted.
Conclusions:
LEIC is a novel surgical approach that shows satisfactory efficacy and safety in patients with large, surficial, and symptomatic NPHCs. LEIC's main advantage is that it can efficiently prevent cyst recurrence and decrease postoperative morbidity. However, its long-term efficacy and safety require further verification, especially with huge cysts.
Introduction
Nonparasitic hepatic cysts (NPHCs) are a common condition occurring in ∼2.5%–18% of the general population. 1 NPHCs, especially large cysts (>5 cm in diameter), can cause symptoms—including abdominal pain, low appetite, and nausea—which compromise quality of life. Standard treatments for NPHCs are laparoscopic deroofing (LD, also known as laparoscopic fenestration or laparoscopic unroofing), 2 percutaneous aspiration, and alcohol sclerotherapy. 3 Although these treatments are minimally invasive and fairly effective, the problem of NPHC recurrence has been noted by clinicians. The recurrence rate after LD has been reported to range from 0% to 25%. 4 Debs et al. reported a 15.1% recurrence rate following LD in a study of 33 cases, 5 while a recent systematic review reported a 9.6% recurrence rate after LD. 1 Recurrence rates after percutaneous aspiration or alcohol sclerotherapy have been reported less frequently. Larssen et al. performed alcohol sclerotherapy in 47 NPHC patients who were followed up for 24–193 (median 56) months, during which period no recurrence was observed. 6 Hahn et al. found that alcohol sclerotherapy might be followed by transient recurrences of cysts that would disappear within several months. 7 Recurrence after percutaneous aspiration and alcohol sclerotherapy is known to be closely associated with the size of the cyst. These treatments are effective in patients with cysts smaller than 5 cm in diameter; on the other hand, such small cysts are usually asymptomatic. 8
Even though the complicated and multifold mechanisms underlying NPHC recurrence are not fully understood yet, recurrence is closely associated with the type of NPHC (e.g., polycystic liver disease is most likely to recur 1 ), cyst location, 5 and the surgeon's skill level. It has been documented that simply aspirating the cyst might result in a short-term recurrence of up to 100%. 9 Besides, the rate of recurrence is high with inadequate cyst deroofing. 10 Recurrent cysts in these cases can be attributed to the fact that the cyst capsule survives intact after both simple aspiration and inadequate deroofing. Thus, we believe that the complete removal of intact cysts will prevent recurrence. To test this hypothesis, we developed a novel procedure, laparoscopic enucleation with intact cyst (LEIC), to fully remove cysts. In the present study, we retrospectively investigated the rate of cyst recurrence in NPHC patients who underwent LEIC.
Materials and Methods
Patients
We performed a retrospective study of patients with large NPHCs who underwent the LEIC surgical treatment at our hospital. Patients with polycystic liver disease were excluded. Fourteen patients with NPHCs treated between May 1, 2016, and December 31, 2018, were enrolled in this study. The inclusion criteria were simple hepatic cysts, cyst diameter ≥9 cm, and symptomatic cysts. The exclusion criteria were as follows: cyst diameter <9 cm; asymptomatic cysts; mucinous cystadenoma, cardiopulmonary dysfunction, malignant tumor, hematologic system diseases, and psychiatric disorders; age over 80 or under 14 years; or cysts coexisting with other diseases, such as hepatoma and/or cirrhosis. During surgery, the surgeon (F.Y.) checked the cysts for any possible malignancy. Immediately upon observation of any suspicious lesion, frozen section analysis was performed to identify the pathological entity. The patient characteristics are listed in Table 1.
Clinical Characteristics of Enrolled Patients
This study was designed and performed according to the World Medical Association Declaration of Helsinki (2000) and approved by the Ethics Committee of the First Affiliated Hospital of Zhejiang University (approval number 2019-644). Informed consent was obtained from each patient or their relatives after the study protocol was explained to them.
LEIC procedures
LEIC was performed by an experienced surgeon (F.Y.). Before surgery, each patient underwent a computed tomography (CT) scan to exclude those with cirrhosis, hepatoma, and parasitic hepatic cysts. The states of blood vessels, blood supply to the cyst, and the biliary duct were also assessed.
We performed LEIC using a five-port approach 11 (Fig. 1). Briefly, the patients were placed in the supine position and, after anesthesia, safely secured to the operating table at the nipple line and knee joints. If the cyst was located in the right hepatic lobe, the patient's right side was elevated by 30°. The patient's position could be changed easily at the surgeon's request. The first incision was made on the cyst surface. If the cystic fluid appeared to be clear (i.e., nonbilious), the biliary duct was deemed intact. After aspiration of the cystic fluid, the cyst capsule was removed carefully.
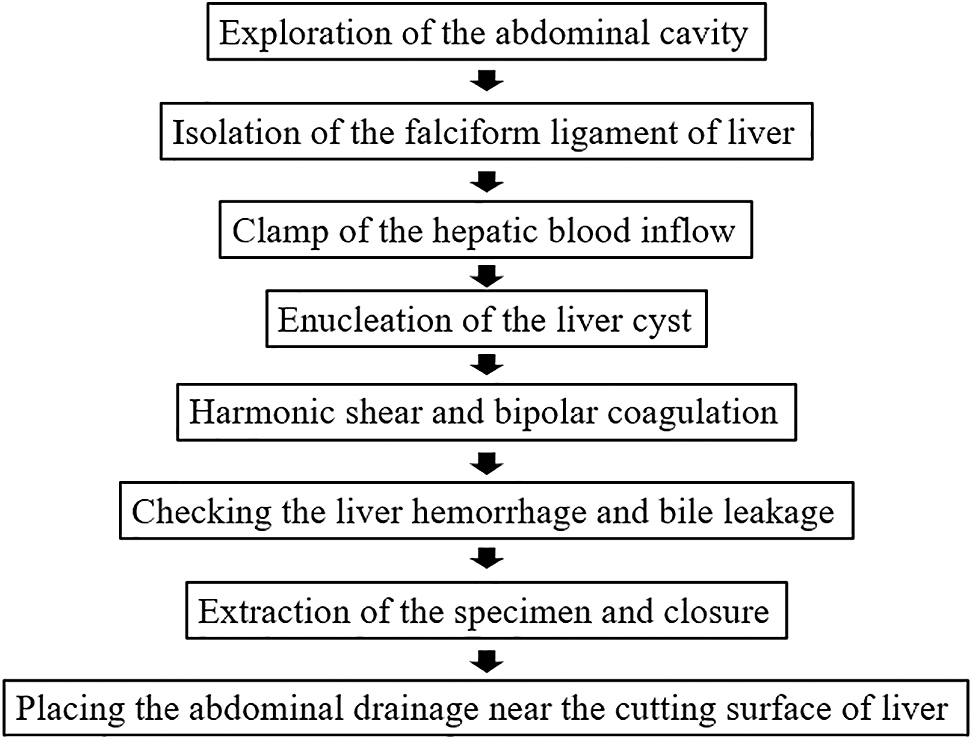
Flow chart of LEIC procedures. LEIC, laparoscopic enucleation with intact cyst.
In a few cases, some portions of the cyst capsule had adhered to the tough Glisson's sheath, which made excision difficult. In such cases, hemostasis was achieved first, using bipolar coagulation, and clips were placed on the adhesion sites between the cyst wall and Glisson's sheath to prevent hemorrhage and bile leakage. Then, the cyst was dissected and coagulated with harmonic shears. Bearing in mind that the presence of bile in the cystic fluid indicated bile leakage, we used sterile gauze to check the biliary duct and anastomoses for bile leaks after performing the above procedures. Once detected, bile leaks were controlled and repaired with Prolene sutures (5-0 or 6-0 according to the size and location of the leak). Next, the removed cyst was sent to pathology for quick frozen section examination to confirm NPHC diagnosis. Finally, an abdominal drain was placed to observe whether bleeding and bile leakage occurred after the operation. Detailed procedures are shown in a Supplementary Video S1.
Patient follow-up
All patients were followed up at 1, 3, and 6 months after surgery. Liver function and cyst recurrence were assessed using a strengthened CT scan. Every 6 months, ultrasonography was performed to explore cyst recurrence.
Results
Patient characteristics
The enrolled patients' clinical characteristics are listed in Table 1. The subjects were mostly female (10 versus 4), average age 59.28 ± 10.85 years, and symptomatic, with a mean cyst diameter of 10.87 ± 2.16 cm. Before surgery, 9 patients suffered from abdominal pain, 9 complained of abdominal distension, and 4 had other complaints. The comorbidities observed in the studied population included cholecystic polypus, adiposis hepatica, cholelithiasis, cholecystitis, and hepatic hemangioma. Twelve cases (4 males and 8 females) had one cystic lesion, while two cases (females) appeared to have two cystic lesions.
Surgery
Laparoscopic enucleation was successfully completed with no intraoperative complications. The median operation time and the average postoperative hospital stay were 80 ± 25 minutes and 6.5 ± 1.4 days, respectively. Figure 2 shows a removed cyst with its capsule preserved intact. Representative CT images of two patients who underwent laparoscopic enucleation are shown in Figure 3. The cyst was removed successfully, and consequently, blood flow in the hepatic veins was ameliorated. Diagrams of the oppressed hepatic vascular show enlarged veins (Fig. 3.).

A removed cyst with its capsule preserved intact.
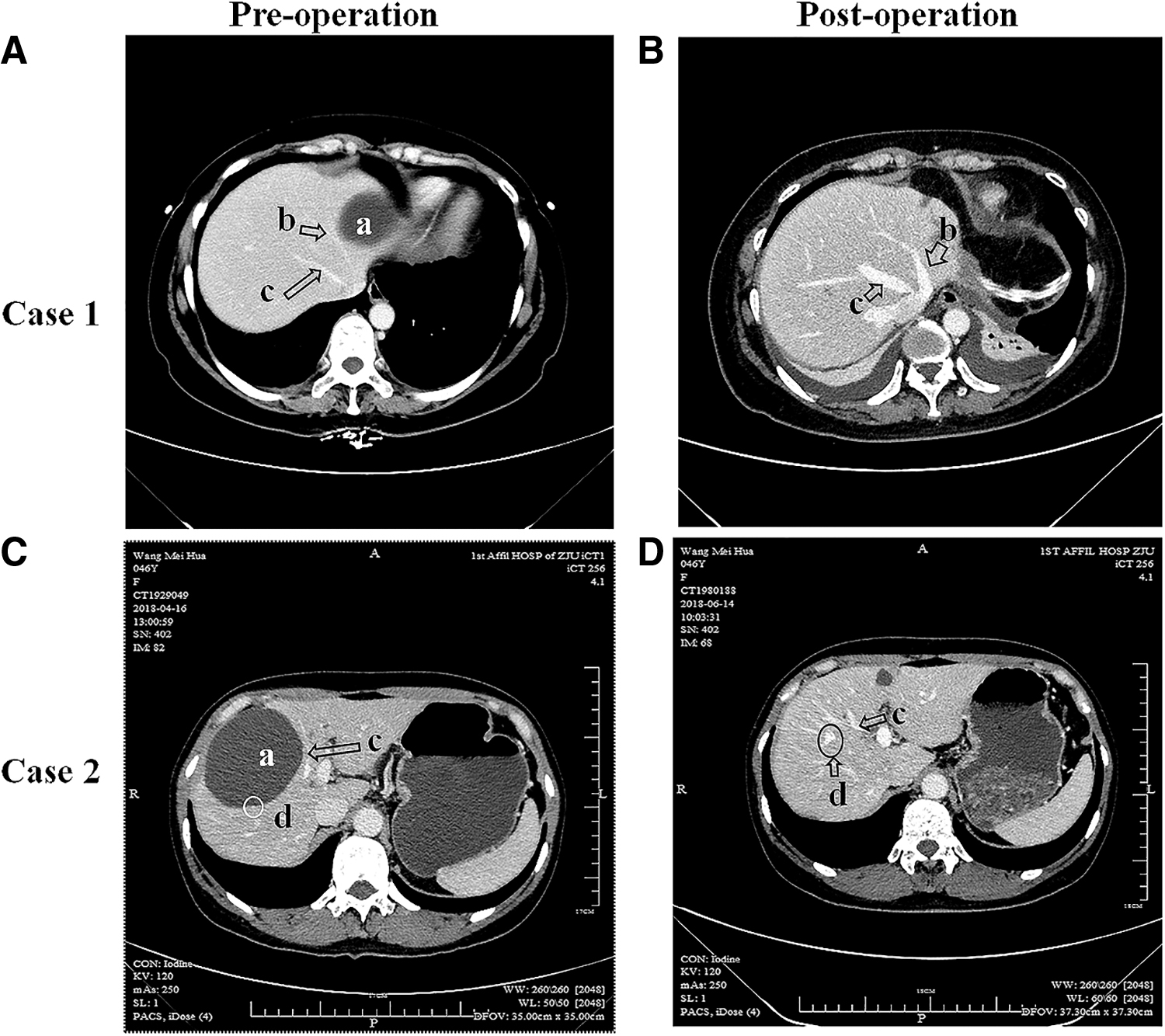
Representative CT images for two patients with liver cysts who underwent LEIC.
Follow-up
During follow-up (average 19.3 months, range 10–38 months), no recurrence of the cyst, complications, or death was reported (Table 1). All patients needed only medication to prevent complications, and the Clavien–Dindo classification was grade II. 12 The symptoms of all patients were relieved after surgery, confirmed at the outpatient clinic. No patient required a secondary surgery.
Discussion
In the present study, we introduced LEIC as a novel approach to treating NPHCs through complete removal of the cyst. To the best of our knowledge, this is the first study to describe a surgical procedure for eliminating an intact cyst. During follow-up, no cyst recurrence was found in the enrolled patients. This result suggests that dissecting and coagulating the cyst may help decrease cyst recurrence, whereas complete removal of the cyst will completely prevent recurrence.
In this study, we selected symptomatic patients with NPHCs over 9 cm in diameter for the following reasons: (1) all these patients were symptomatic and (2) in patients with NPHCs greater than 10 cm in diameter, the cyst protruded from the liver surface and therefore could be approached easily; besides, in those with NPHCs between 9.0 and 10 cm in diameter, the cyst was observed only 0.78 ± 0.24 cm deep within the liver tissue and thus considered superficial. We did not include patients with NPHCs <9.0 cm. Obviously, if the cyst is located deep in the liver, excising it intact might be risky. According to the present study results as well as our clinical experience, we speculate that a depth of ≤1 cm from the liver surface is safe because the cyst at this location is easy to approach and the injury to the liver parenchyma is slight. Nonetheless, the safe depth for LEIC requires further investigation in the future.
Similar to a previous report by Debs et al., 5 we followed up 14 patients for an average period of 19.3 months (range: 10–38 months). The present study, however, achieved better outcomes than the previous study (recurrence: 0 versus 5). 5 Furthermore, no postoperative hemorrhage or bile leakage was observed in our 14 patients. Our data suggest that LEIC is an effective and safe procedure for patients with NPHCs.
As early as 1996, Gigot reported that 23% of patients undergoing insufficient LD had symptomatic recurrence and 37% had radiographic recurrence during an average 9-month follow-up. 13 Thus, a period of 9 months seems sufficient to observe recurrence. By the same token, the follow-up period in our study (average 19.3 months) proves to be reliable.
Petri et al. reported that inadequate removal of the cyst capsule resulted in a 38.8% recurrence rate. 10 If the cyst capsule is not fully removed, the remaining capsule will recover and grow, causing cyst recurrence. LEIC involves complete dissection and coagulation of the cyst capsule, which fundamentally eradicates the source of recurrence. In cases where the capsule is difficult to remove, dissection and coagulation can be performed using bipolar coagulation, Hem-o-lok clips, and harmonic shears. In this way, most capsules can be completely dissected. Bipolar coagulation can obliterate any potential remaining tissue at the Glisson's sheath. However, this procedure can be technically difficult—especially for cysts located in S7, where the liver lobes need to be completely isolated. The cyst causes chronic compression and, consequently, atrophy of the hepatic tissue in the liver capsule whose wall may concurrently be changed by chronic inflammation. Any prominent ridge protruding from the cyst capsule wall could be a branch of the hepatic vessels or biliary ducts. Inappropriate surgical techniques, such as coagulation or scratching of the capsule wall, could result in complications such as hemorrhage and bile leakage. 14 Thus, this surgery must be performed by an experienced surgeon who is familiar with NPHC anatomy and pathology. In this study, 8 patients had cysts in the right hepatic lobe. To ensure complete removal of the cyst capsule, particularly for cysts located in unapproachable areas of the liver—such as S7 (n = 4) and S8 (n = 2), the liver was isolated by laparoscopic instruments and the right hepatic lobe was clearly exposed.
Although our findings indicate that LEIC is an effective and safe procedure for NPHCs, they were limited by the small sample size and lack of long-term observations. (1) Huge hepatic cysts usually compress the surrounding hepatic parenchyma, making it atrophic. Moreover, the cystic wall often abuts large vessels (e.g., Glissonean branches and/or hepatic veins). Hence, to avoid the risk of damaging adjacent vessels, surgeons do not touch the portion of the cyst wall adjoining the liver parenchyma. Although no complications after LEIC were observed in the present study, injury to vessels must always be considered a potential risk and avoided in future operations. Depending on the cyst location, structures in the Glisson's sheath (e.g., portal vein, hepatic artery, and bile duct) and the hepatic veins might be slightly or seriously injured as a result of touching the cyst wall, which needs to be treated carefully. (2) LEIC might be a much more invasive procedure than the traditional LD, particularly with huge cysts. (3) Huge cysts usually undergo fibrotic changes due to inflammation in the cystic wall, making it difficult for surgeons to separate only the cysts from the surrounding liver parenchyma. (4) In addition, in the case of huge cysts that cause jaundice, Glissonean trunks near the hepatic hilum are usually compressed. Thus, separating the cystic wall from the liver parenchyma may entail the risk of damaging a thick Glissonean branch, thereby creating a large ischemic area. Thus, the safety and long-term efficacy of LEIC, especially for huge cysts, require further study.
Conclusions
In this study, we verified LEIC's efficacy and safety for treating NPHCs. Since LEIC achieves complete cyst excision (Table 2), it can prevent cyst recurrence more effectively than conventional LD and alcohol sclerotherapy and thus proves to be a promising new procedure, particularly for patients with large (diameter ≥9 cm), surficial (depth from the liver surface ≤1 cm), and systematic NPHCs. However, further studies are needed to evaluate the safety and long-term efficacy of LEIC, especially for huge cysts.
Strengths and Weaknesses of the Existing Surgical Procedures for Treating Nonparasitic Hepatic Cysts
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was partly supported by grants from the Japan Society for the Promotion of Science (Grant-in-Aid for Young Scientists, Type B, No. 20791025, and Grant-in-Aid for Scientific Research C, General, Nos. 24592157, 15k10358, and 18K08991).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.