
Abstract

Podium Abstracts
S001 OUTCOMES OF INITIAL SUBTOTAL COLECTOMY FOR PEDIATRIC INFLAMMATORY BOWEL DISEASE
Cohen Children's Medical Center at Northwell Health
Background: Subtotal colectomy with end ileostomy (STC‐I) has been well established in the adult literature as an initial surgical treatment for refractory inflammatory bowel disease (IBD) related colitis. However, in the pediatric population, the efficacy of this approach has been less well characterized; likely due to concerns regarding the advisability of leaving a diseased rectum in‐situ. Our aim was to examine the outcomes after STC‐I for refractory inflammatory bowel disease at our pediatric tertiary care center.
Methods: An IRB approved retrospective review of patients aged 5 to 21 years who underwent operative treatment with initial STC‐I for medically refractory IBD from January 2010 to August 2018 at our institution. Only complications related to the STC‐I were considered; complications subsequent to reconstruction are excluded from analysis. Early complications were defined as occurring within 60 days of STC‐I. We performed descriptive statistics using Fisher's exact test and Student's t‐test, as appropriate.
Results: Over the study period, 37 patients underwent STC‐I, with 75.7% performed laparoscopically. All open procedures were performed in the first two years of the study period. The average age of patients was 12.3 ± 4.2 years. Patients were predominately male (51.4%) and Caucasian (48.6%). Twenty‐nine (78.4%) colectomies were performed for ulcerative colitis (UC), 3 (8.1%) for Crohn's disease, and 5 (13.5%) for indeterminate colitis.
Average post‐operative length of stay was shorter in the laparoscopic group compared to those undergoing open operations (5.1 ± 2.2 vs 6.9 ± 1.6 days, P = 0.03), excluding one patient in the laparoscopic group with a post‐operative stay of 43 days secondary to complications of toxic megacolon. 30‐day readmission rate was 21.1%. Patients experiencing unplanned readmission or unplanned operations were similar between groups (22.2% vs 39.3% p = 0.3 and 22.2% vs 21.4%, p = 0.9 respectively).
Overall, 14 patients (37.8%) experienced a complication with many patients experiencing multiple complications. Early complications occurred in 9 (24.3%) patients. These included venous thromboembolism (5.4%), small bowel obstruction (5.4%), and intestinal perforation (2.7%). There were 3 patients with rectal stump dehiscence (8.1%), one resulting in mortality and one requiring emergent proctectomy. Late complications occurred in 24.3% of patients and included readmissions for dehydration (5.4%) or abdominal pain (2.7%). There were four patients (10.8%) with five admissions for bowel obstruction, two of whom required operative intervention (5.4%).
Nutritional status improved post colectomy. Albumin levels of 3.3 ± 0.8 preoperatively increased to 4.3 ± 0.47 post‐operatively (p < 0.001). Among patients for whom data was available, average time to discontinuation of IBD‐related medications was 4 weeks, with no patient requiring longer than three months of treatment (n = 14). Forty‐seven percent required rectal treatment for proctitis; no patients required oral or intravenous therapy or admission (n = 15). Patients did well long term, with twenty‐five patients (67.5%) reestablishing intestinal continuity at our institution.
Conclusions: Utilization of STC‐I as an initial procedure in the treatment of refractory inflammatory bowel disease related colitis in children is a safe and reasonable surgical approach. Implementing a laparoscopic approach to subtotal colectomy provides further benefit by reducing post‐operative length of stay.
S002 EARLY EXPERIENCE WITH VARIANT 2‐STAGE APPROACH IN SURGICAL MANAGEMENT OF INFLAMMATORY BOWEL DISEASE COLITIS IN THE PEDIATRIC POPULATION
Cohen Children's Medical Center at Northwell Health
Background: Multi‐staged surgical management of inflammatory bowel disease (IBD), culminating with an ileal pouch‐anal anastomosis (IPAA) can provide a cure for refractory IBD symptoms while maintaining fecal continence. Surgical approaches to IPAA creation have historically included a 3‐stage approach done by subtotal colectomy followed by IPAA with diversion. More recently, a variant 2‐stage approach without diversion at time of IPAA creation has become increasingly utilized, yet evidence as to the efficacy of this approach is limited. Our aim was to examine outcomes of pediatric patients undergoing variant 2‐stage approach for IPAA creation at our tertiary care children's hospital.
Methods: An IRB approved retrospective chart review of patients aged 5 to 21 years who underwent operative treatment with initial subtotal colectomy (STC), followed by a total proctocolectomy with IPAA +/‐ diversion for medically refractory IBD from January 2010 to August 2018 (n = 25). Fisher's exact test was used for statistical analysis.
Results: The average age of patients at the time of subtotal colectomy was 13.4 ± 3.4 years. Patients were predominately male (53.8%) and Caucasian (53.8%). Indication for initial STC was ulcerative colitis in 84.6% of patients, Crohn's disease in 3.8% of patients, and indeterminate colitis in 11.5% of patients.
Majority of IPAA procedures were done laparoscopically (88.5%). Thirteen patients (52%) underwent 2‐stage variant IPAA. Amongst the 12 patients undergoing conventional 3‐stage IPAA, reasons for diversion included physician preference (75%), technical considerations including tension of the anastomosis and extensive pelvic adhesions (16.7%), and 1 patient diverted for preexisting Crohn's disease. There were no significant differences in overall readmission rates (66.7% vs 53.8%, p = 0.5) or reoperation rates (50% vs 30.8%, p = 0.3) between patients undergoing 3‐stage approach and patients undergoing 2‐stage variant.
Overall, 40% of patients experienced a complication after completion proctocolectomy with IPAA. Complication rates were similar between 2‐stage and 3‐stage IPAA groups (30.7% vs 50% P = 0.33). Complications within the 2‐stage group included 1 anastomotic leak requiring IR drainage, 2 patients requiring admission for pouchitis, 1 patient with both a wound infection and anastomotic stricture, and 1 patient requiring operation for incarcerated ventral hernia at an old stoma site. Complications within the 3‐stage group included 1 readmission for bloody ostomy output, 1 readmission for dehydration secondary to intractable vomiting, 1 patient requiring dilation for anastomotic stricture, 1 patient admitted twice for small bowel obstruction, 1 patient requiring 2 diagnostic laparoscopies for pouch volvulus, and 1 patient post‐operatively diagnosed with Crohn's and formation of a pouch‐vaginal fistula. There were no mortalities in either group.
Conclusions: Treatment of refractory inflammatory bowel disease in children remains challenging to treat, but surgical treatment with subtotal colectomy followed by IPAA is an approach that provides relief of symptoms and preservation of fecal continence. Complication rates remained unchanged whether IPAA was conducted with or without diversion demonstrating that adoption of the 2‐stage variant approach is a safe and feasible surgical treatment plan that may serve to reduce subsequent anesthesia exposure and trips to the operating room.
S003 YOUTUBE AS AN EDUCATIONAL RESOURCE FOR PEDIATRIC SURGEONS ON LAPAROSCOPIC ASSISTED PULL‐THROUGH IN HIRSCHSPRUNG DISEASE
1Hospital San Juan de Dios, 2Clinica Las Condes
YouTube offers an invaluable source of information. During the last decade, videos documenting surgery procedures, patient experiences, and medical commentary have gained hundreds of millions of views and it has become a common way for surgeons to update their knowledge on surgical procedures.
This study evaluates the quality and utility of the YouTube content regarding Laparoscopic Pull‐Trough in Hirschsprung Disease (LPTHD).
Methods: Using the YouTube search feature, a search using the terms laparoscopic + pull‐through + Hirschsprung's Disease was performed. The resulting videos were analyzed to determine the content and relevance.
The exclusion criteria were videos not related to LPTHD, related to adults patients and repeated videos.
Results: The search revealed 281 videos and video playlists, and of the 254 watched videos only 38 were related to LPTHD. 7 videos had an institutional origin and 31 were private uploads. Regarding the language, English was most common, with n = 29, followed by Spanish with 5, Italian‐2 and Russian‐2. Only 10 of the videos had an audio explanation for the procedure.
Regarding the content, 3 of them show an explanation for Hirschsprung's disease and the diagnosis, 4 showed operative results and outcomes. In 15 videos laparoscopic colonic biopsy technique was showed and in 17 transanal stage was available as well. Finally, in 4 videos a comparison between the transanal and the open technique was made. No preference for country of origin was found.
Discussion: Although a popular resource for surgical study material, YouTube videos can present biased information. Most videos are private uploads without any regulation or validation. These videos can be a help when planning a surgery, but all surgeons, specially trainees, should be aware of the possible biases within the videos and be prepared to verify the information.
We believe that IPEG and IPEG's members have the opportunity and the responsibility to provide reliable audiovisual material for pediatrics surgeons and relatives of Hirschsprung's Disease patients.
S004 LAPAROSCOPIC TRANSABDOMINAL COLOPEXY FOR PROLAPSE OF A NEWBORN END COLOSTOMY
1Division of Pediatric Surgery, Hackensack Meridian School of Medicine at Seton Hall, Joseph M. Sanzari Children's Hospital, Hackensack, NJ; Department of Surgery, Boston Children's Hospital, 300 Longwood Ave, Boston, MA 02115, 2Division of Pediatric Surgery, Hackensack Meridian School of Medicine at Seton Hall, Joseph M. Sanzari Children's Hospital, Hackensack, NJ, 3Division of Pediatric Surgery, Hackensack Meridian School of Medicine at Seton Hall, Joseph M. Sanzari Children's Hospital, Hackensack, NJ; Division of Pediatric Surgery, NYU School of Medicine, Hassenfeld Children's Hospital at NYU Langone, New York, NY
Purpose: Treatment of infants with anorectal malformations may necessitate colostomy creation prior to definitive repair. Standardized placement of a newborn colostomy at the level of the distal descending colon has significantly decreased the rate of prolapse by taking advantage of the natural tether provided by the left colon attachment to the retroperitoneum. Despite this, colostomy prolapse may still occur due to normal variation in the fixation of the left colon, albeit notably less so when compared to loop colostomies.
When prolapse occurs, efforts to treat the colostomy without re‐opening the primary incision have been described. One such method involves packing the colostomy lumen with petroleum gauze to produce a palpable mass, and then utilizing transabdominal sutures to blindly pexy the colon to the anterior abdominal wall. While anecdotally successful, the approach lacks direct visualization and risks injuring or obstructing the bowel. We present a novel laparoscopic approach to treating symptomatic colostomy prolapse in infants which significantly reduces the risk of bowel injury without requiring larger incisions.
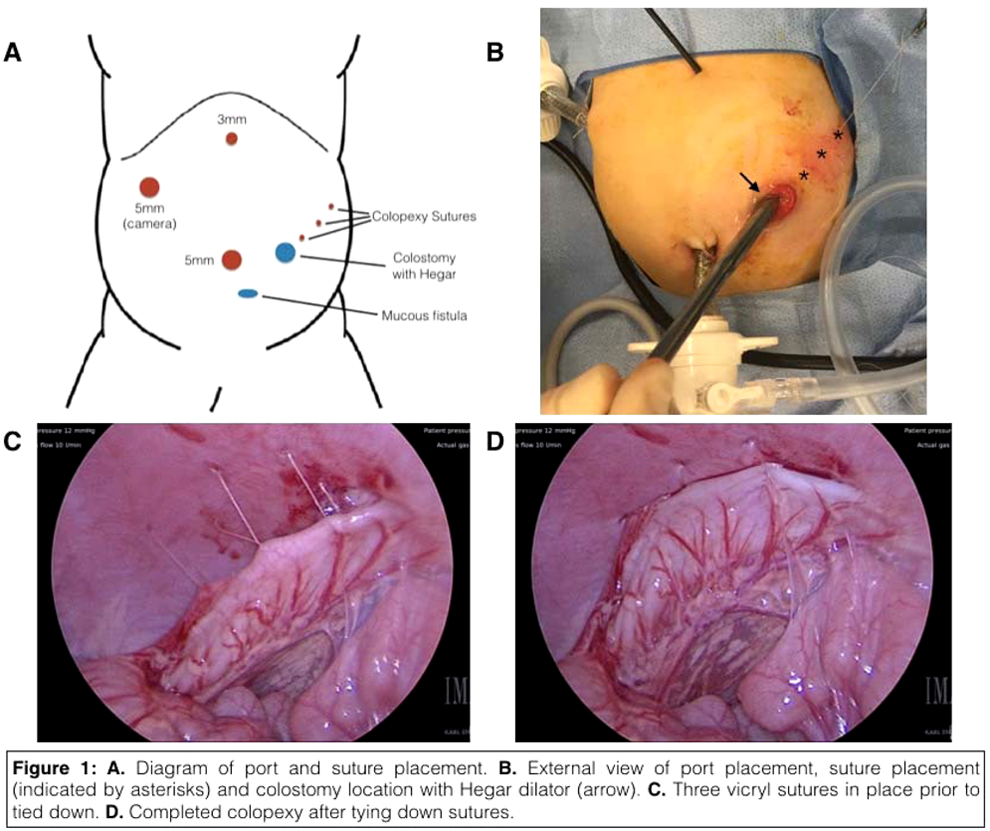
Methods: A 2 month old child presenting with recurrent episodes of obstructive prolapse was brought to the operating room for laparoscopic colopexy. Five millimeter trocars were placed at the umbilical and right upper quadrant positions, while a 3mm grasper was placed through a subxyphoid stab incision (Figure 1A). A 5mm‐30 degree camera was then placed through the right upper quadrant trocar. We observed complete lack of normal fixation of the descending colon to the retroperitoneum, an anatomic variant we hypothesize accounted for the prolapse. A #10 Hegar dilator was inserted through colostomy for manipulation of the bowel and to maintain lumenal integrity during suture colopexy. Three 4‐0 vicryl sutures were placed transabdominally through stab incisions (Figure 1B). The sutures were then grasped intraabdominally and sutured to the anti‐mesenteric border of the descending colon in three places (Figure 1C and 1D), with the sutures delivered back out through the abdominal wall using an Endoclose device. The presence of the Hegar dilator during suturing protected against inadvertent “back‐wall” suturing of the mesenteric side of the colonic wall.
Results: After tolerating the procedure well, the infant was stooling and eating normally within hours after surgery and with no further evidence of prolapse. The patient was discharged home the following day and is now five months out from surgery with no further complications in regards to his colostomy prolapse.
Conclusions: Currently, the only published data on laparoscopic colopexy in infants includes one case report involving the treatment a volvulus in a 32 month female. Therefore, to our knowledge we present the first case of a successful laparoscopic colopexy for end colostomy prolapse, modeled on a variation of the “blind” transabdominal colopexy. Addition of a Hegar dilator ensures lumenal patency and provides an added measure of safety without requiring additional incisions.
S005 USE OF MANEUVERS TO INCREASE MESENTERIC LENGTH IN CHILDREN UNDERGOING ILEAL POUCH‐ANAL ANASTOMOSIS
Mayo Clinic
Background: Operative maneuvers to increase mesenteric reach during ileal pouch‐anal anastomosis (IPAA) are well described in adults, but limited data exist on the need for their use in children.
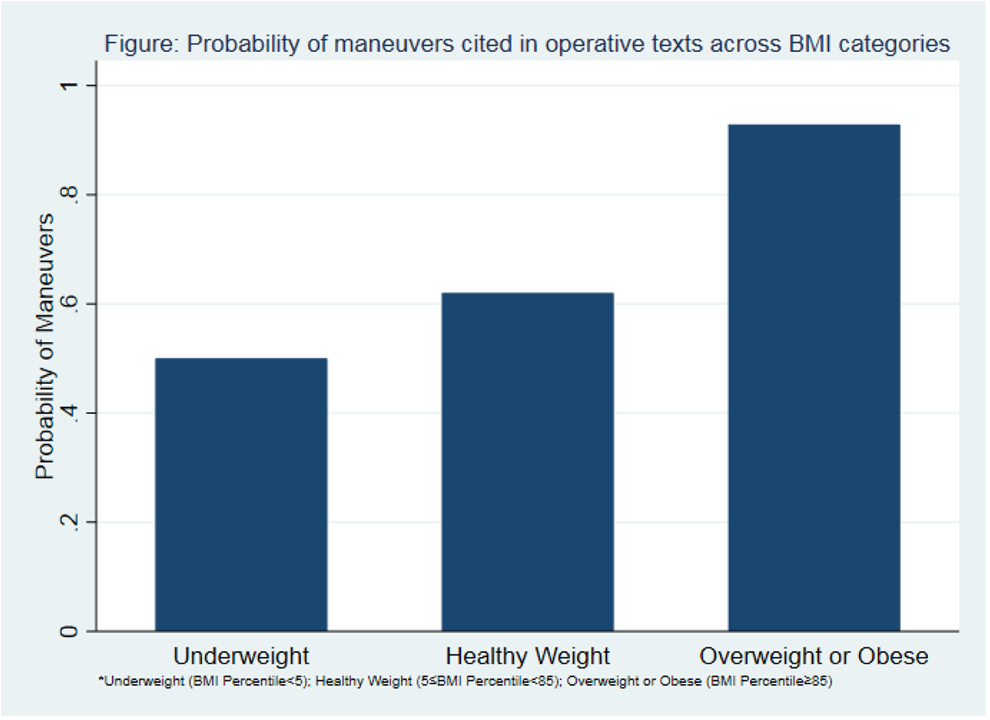
Methods: We reviewed children (age <18) considered for IPAA creation at a single tertiary referral center from 2007 to 2017. Patient factors, operative details, and thirty‐day postoperative complications were abstracted. Body mass index (BMI) was normalized to BMI percentile‐for‐age‐and‐sex and classified as underweight (BMI <5th percentile), healthy weight (5th≤BMI percentile <85th), or overweight/obese (BMI ≥85th percentile).
Maneuvers were identified from operative notes and included creation of mesenteric windows, high ligation of the ileocolic pedicle, ligation of terminal pouch vessels, and/or additional mobilization of the small bowel mesentery after a failed test of pouch length. Operative times were stratified by pediatric surgeon, group (in the case of adult colorectal surgery), and whether colectomy was performed at the same operation as the IPAA. Univariate analysis was performed to determine factors associated with the use of maneuvers. A multivariable model was built to determine independent factors affecting the need for operative maneuvers.
Patients: Of 103 patients, 52 underwent total proctocolectomy with attempted IPAA and 51 underwent subtotal colectomy, 9 did not undergo an attempt at IPAA creation (reasons included growth concerns (n = 4), ongoing medical evaluation (n = 2), patient preference (n = 2), and obesity (n = 1)).
Results: Of 94 patients who underwent attempt at initial IPAA creation, 91 (97%) had successful IPAA creation and 3 (3%) failed to reach. Failure occurred due to inability to reach in 3 patients, with specific mention of patients' obesity in 2 (BMI percentiles: 88, 98), and pouch ischemia in 1 (BMI percentile 82). In the 91 patients with successful IPAA, median age was 15 (Range: 1.5–17) and 57% were female. IPAA creation was performed as a one‐stage operation in 21 (23%), a two‐stage operation in 29 (32%), a modified two‐stage operation in 9 (10%), and as part of a three‐stage operation in 32 (35%). A laparoscopic approach was successful in 75 (82%) with 4 (4%) conversions to open, and 12 (13%) planned open procedures.
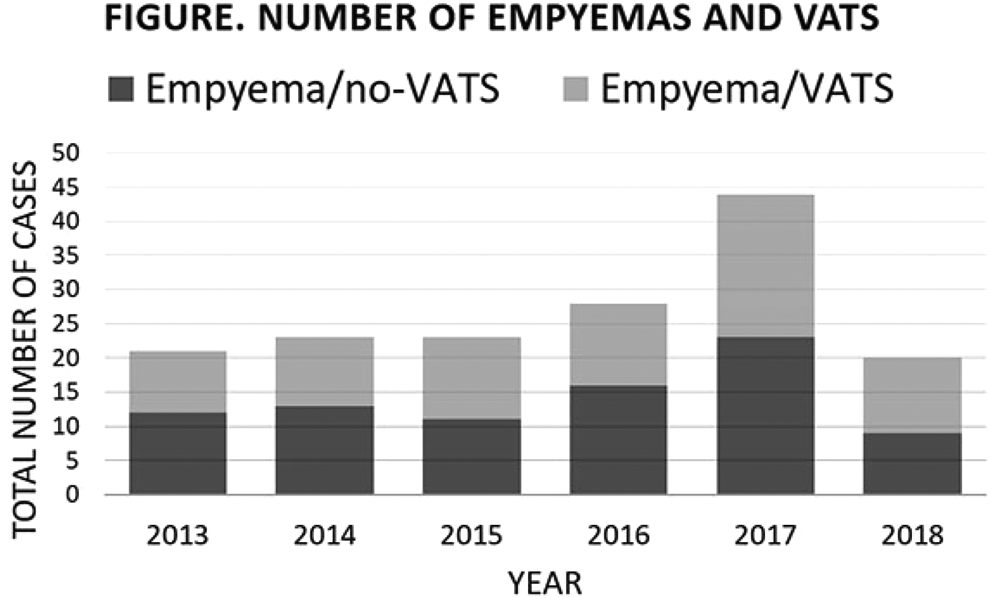
Sixty (66%) patients required maneuvers to lengthen the mesentery. On univariate analysis, overweight patients required maneuvers more often than non‐overweight patients (93% versus 61%, p = 0.03). A positive trend for requirement of maneuvers existed across increasing BMI classification (p = 0.02, FIGURE). Performing maneuvers was associated with operative times above a surgeon's median operative time in operations that required colectomy (61% versus 32%, p = 0.04), but no difference was noted in operative times for completion proctectomy operations or 30‐day maximum Clavien‐Dindo scores (both p > 0.05). Being overweight/obese remained an independent risk factor for maneuvers (OR: 9.3, 95% CI: 1.1–82.8) after adjusting for age, sex, height, operative stage, and operating surgeon.
Conclusion: Surgeons need to be prepared to perform mesenteric lengthening maneuvers when operating on overweight and obese pediatric patients in order to ensure minimal tension on IPAA. Whether these maneuvers have an impact on long‐term pouch function is undetermined.
S006 PROPHYLACTIC COLECTOMY FOR CHILDREN WITH FAMILIAL ADENOMATOUS POLYPOSIS: A COST AND OUTCOMES ANALYSIS COMPARING OPEN AND LAPAROSCOPIC SURGERY
1University of Miami, 2UT Southwestern
Background: A laparoscopic approach for the surgical management of familial adenomatous polyposis (FAP) is becoming increasingly common for pediatric patients. The purpose of this study was to evaluate the clinical outcomes and costs associated with laparoscopic compared to open surgery for elective prophylactic colectomy in children with FAP.
Methods: The Kids' Inpatient Database (2009 and 2012) was queried for all children (age ≤20 years) with a diagnosis of FAP without malignancy that underwent elective open or laparoscopic colectomy with or without proctectomy. The patient demographics, concurrent diagnoses, frequency of complications, length of stay, treating hospital characteristics, and total hospital charges were compared.
Results: Overall, we identified 216 patients with FAP that underwent elective colectomy, of which 95 cases were performed open and 121 were laparoscopic. The median age was similar (16 years) in each group. While chronic pulmonary disease was less common in the open cohort (4% vs 16%, P = 0.007), liver disease (3% vs 0%, P = 0.049) and coagulopathy (3% vs 0%, P = 0.049) were more common in the laparoscopic cohort. Complications were more common in open procedures, including accidental perforation or hemorrhage (4% vs 0%, P = 0.023), reopening of surgical site (3% vs 0%, P = 0.049), and pneumonia (3% vs 0%, P = 0.049). Diverting ostomy was performed more commonly in the open cohort (74% vs 49%, P < 0.001). There were no significant differences in the treating hospital characteristics with regard to location, bed size, teaching status, or ownership. The median length of stay was similar in the open and laparoscopic groups (7.0 vs 6.0 days, P = 0.712). Median total hospital charges were also similar ($67,334 vs $68,717, P = 0.080).
Conclusion: Our findings suggest that a laparoscopic approach to prophylactic colectomy can be safely performed for children with FAP. Laparoscopic colectomy was associated with fewer complications and a lower frequency of ostomy creation compared to an open approach. Furthermore, there was no significant difference in length of stay or cost.
S007 LAPAROSCOPIC THREE‐POINT FIXATION FOR INTRACTABLE RECTAL PROLAPSE IN CHILDREN
Alexandria University
Aim: Rectal prolapse in children is a common condition in infancy and early childhood that usually responds to conservative measures. Surgery is reserved only for refractory cases that fail to respond to conservative measures. This study was designed to evaluate the efficacy of 3‐point fixation concept (retrorectal dissection, rectopexy to presacral fascia of the sacral promontory and sigmoidopexy onto the anterior abdominal wall) in treatment of complete rectal prolapse in children using laparoscopy.
Methods: This prospective study was conducted on 18 cases with persistent complete rectal prolapse who failed to respond to adequate conservative measures from July 2015 to July 2017. The technical details of the procedure are described. Patients were followed up for at least 6 months and were assessed clinically and radiologically for continence and constipation using the appropriate scoring systems.
Results: Eighteen patients were included, 12 females and 6 males, laparoscopic rectopexy and sigmoidopexy were done for all cases. Age ranged between 6–38 months (mean 18.4) The mean duration for surgery was 58.4 min. No intraoperative complications recorded. One case (5.5%) had partial thickness recurrence and 2 cases had skin stitch sinus. Three patients had constipation requiring laxatives after surgery.
Conclusion: The laparoscopic rectopexy and sigmoidopexy is an effective approach for the treatment of refractory complete rectal prolapse in children. The 3‐point fixation proved efficient in preventing rectal prolapse in children with minimal complications.
S008 COMPARISON OF OUTCOMES FOR OPEN VS LAPAROSCOPIC SURGICAL TECHNIQUES IN PEDIATRIC ULCERATIVE COLITIS
1The University of Miami, 2UT Southwestern Medical Center
Background: Ulcerative colitis (UC) is an aggressive disease in the pediatric population and a cause of significant, lifelong morbidity. As with many other diseases, our treatment approach has been modified by the rise of minimally invasive surgical techniques. The aim of this study is to compare surgical complications in pediatric patients undergoing laparoscopic vs. open surgical treatment for UC.
Methods: We queried the triennially released Kids' Inpatient Database (KID) for all cases of UC undergoing surgical treatment in 2009 and 2012. We identified patients who received total colectomy without proctectomy (n = 413) or total proctocolectomy (n = 196). We performed univariate and multivariate analyses comparing laparoscopic vs. open procedures with regards to demographics, surgical complications, and outcomes.
Results: In UC patients undergoing total colectomy without proctectomy, median length of stay was longer in open vs. laparoscopic procedures (14 vs. 11 days, p = 0.01). Open procedures were associated with more complications than laparoscopic, including pneumonia (5% vs. 1%), coagulopathy (9% vs. 3%), neurologic disorders (8% vs. 2%), fluid and electrolyte disorders (40% vs. 28%), surgical dehiscence (6% vs. 2%), septicemia (18% vs. 2%), and gastrointestinal disorders (16% vs. 7%), all p < 0.05. Likewise, in patients with UC undergoing total proctocolectomy, there were more complications in open vs. laparoscopic technique, including increased transfusion requirements (25% vs. 7%, p = 0.001) and significantly more gastrointestinal upset (11% vs. 1%, p = 0.003). There was no difference with respect to length of stay or cost.
In a multivariate model, patients who underwent total colectomy without proctectomy demonstrated a statistically significant association to complications with open procedures (46% vs. 23%, OR 2.75) and non‐elective admissions (37% vs. 19%, OR 2.47). Similarly, patients who underwent total proctocolectomy also demonstrated statistically significant association to complications with open procedures (33% vs. 11%, OR 3.83) and non‐elective admissions (41% vs. 15%, OR 3.91), all p < 0.001. Finally, complications were also higher in the group who underwent colectomy without proctectomy regardless of surgical technique (30.5 vs 21.9%, p = <0.001) although a significantly higher proportion of these cases were also done non‐electively.
Conclusions: The rates of numerous surgical complications were significantly reduced when utilizing laparoscopic surgical techniques in the treatment of pediatric ulcerative colitis. These findings demonstrate that laparoscopic technique compares favorably to open in this disease process.
S010 ALTERING THE TRADITIONAL APPROACH TO RESTORATIVE PROCTOCOLECTOMY AFTER SUBTOTAL COLECTOMY IN PEDIATRIC PATIENTS
Mayo Clinic
Purpose: Restoration of intestinal continuity by ileal pouch‐anal anastomosis (IPAA) following subtotal colectomy may not require a temporary, protective ileostomy. We compared the outcomes of pediatric patients undergoing modified two‐stage to three‐stage IPAA after recovering from subtotal colectomy.
Methods: We reviewed children (age <18) who underwent IPAA creation for ulcerative or indeterminate colitis from January 1, 2007 to December 31, 2017. Patient characteristics, operative details, 30‐day complications, and post‐operative length of stay (LOS) were abstracted. Total LOS for the three‐stage group included both the IPAA and the ileostomy reversal operations. Univariate comparisons between patients undergoing modified two‐stage and three stage operations were performed.
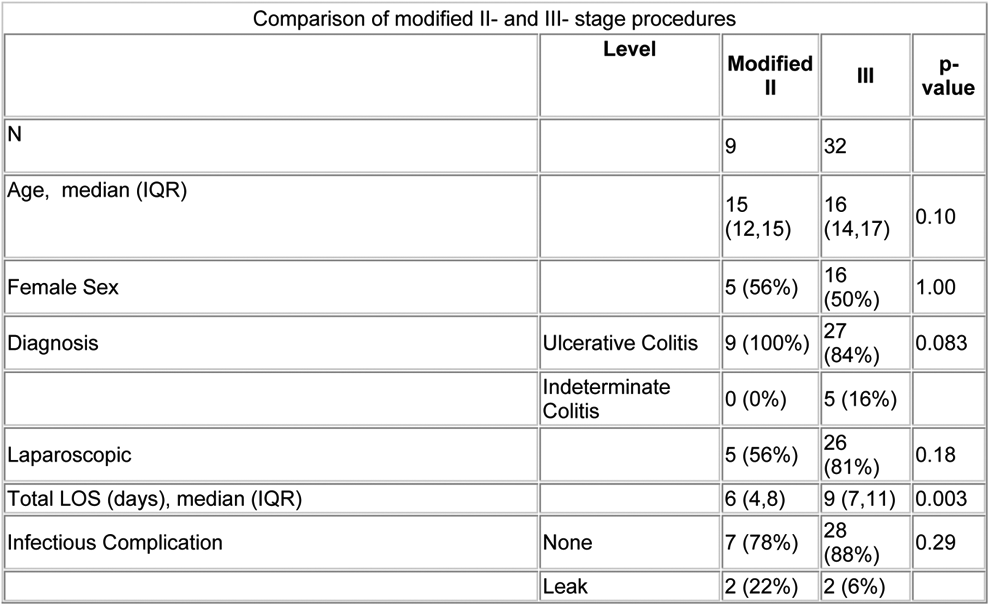
Results: A total of 41 patients underwent IPAA after subtotal colectomy; 9 (22%) underwent a modified two‐stage approach and 32 (72%) a three‐stage technique. Median age, sex, or operative approach did not differ between the groups (all p > 0.05, TABLE 1). Operative approach was laparoscopic in 31 (76%), converted to open in 1 (2%), and planned open in 10 (24%). Single‐incision technique was employed in 10 of 31 (32%) of laparoscopic cases.
Modified two‐stage procedures had shorter total median LOS (6 days versus 9 days, p = 0.003). Incidence of post‐operative leak, readmission, return to the operating room, and maximum 30‐day Clavien‐Dindo scores at the time of IPAA creation did not differ between modified‐two and three stage approaches (all p > 0.05).
Conclusion: The modified two‐stage approach to IPAA creation resulted in fewer hospital days compared to the three‐stage approach. Decisions regarding protective ileostomy after completion proctectomy with IPAA must weigh these benefits with the slight increased risk of leak.

S011 FOLLOW‐UP REPORT OF LAPAROSCOPIC FUNDOPLICATION IN DIFFERENT TYPES OF ESOPHAGEAL HIATAL HERNIA IN CHILDREN
Xinhua Hospital affiliated to Shanghai Jiaotong Univ. Medical School
Background: Esophageal hiatal hernia can be classified into four types (type I through IV). It has been reported that most of the complications occurred in patients with type II to IV hernia compared with type I hernia. The aim of this study was to investigate and compare the efficacy, complications and long‐time outcome after laparoscopic fundoplications between different types of esophageal hiatal hernia in children.
Methods: 110 children (ages 9 days to 6 years) underwent laparoscopic Nissen‐Rosetti fundoplication or Thal fundoplication from 2008 to 2017 in our hospital were included. A total of 81 children were followed up for an average of 47.95 months (range: 12 to 124 months.
Results: All 110 children underwent laparoscopic fundoplication (97 cases of Nissen‐Rossetti and 13 cases of Thal fundoplication) and none converted to open surgery. The mean age of the children at the time of operation was 10.42 ± 11.14 months, and the mean weight was 7.35 ± 3.33 kg. Of 110 children, type I, II, III and IV each accounted for 50.9%, 17.3%, 6.4% and 19.1%. There was no significant difference of time of operation, time to full feeding and length of hospital stay between type I and type II to IV esophageal hiatal hernia. The follow‐up information of 81 children (73.6%) were obtained. The score of postoperative symptoms were comparable between type I and type II to IV esophageal hiatal hernia. The incidence of dysphagia shortly after surgery was 12.3%, but there is only 1 patient still had severe dysphagia at the time of follow up. 9 children (11.1%) had symptoms of gastroesophageal reflux and 3 children still needed antacids. The recurrence rate was 12.3%. The difference in incidence of post‐operative dysphagia (14.6% versus 10.5%; P = .419) and gastroesophageal reflux symptoms (17.1% versus 5.3%; P = .96) and recurrence rate (12.2% versus 13.2%; P = .581) after laparoscopic fundoplication between type I and type II to IV hernia was not significant. The quality of life of three aspects improved significantly after laparoscopic fundoplication in all types of esophageal hiatal hernia children.
Conclusions: Laparoscopic Nissen‐Rosetti fundoplication was an effective approach for all types of esophageal hiatal hernia. Type II to IV hernia could obtain a comparable therapeutic effect and long‐time outcome with type I hernia despite its increased complexity of the anatomy and the required laparoscopic repair procedure.
S012 ENDOSCOPIC SLEEVE GASTROPLASTY IN CHILDREN AND ADOLESCENTS WITH OBESITY: OUTCOMES DURING THE FIRST YEAR
1Department of Surgery, King Saud University, 2Obesity Chair, Department of Surgery, King Saud University
Background: Endoscopic sleeve gastroplasty (ESG) utilizes full‐thickness endoscopic sutures that restrict the stomach to a sleeve‐like configuration. Evidence is scarce on this procedure in pediatric patients. In this paper, we report our experience with children and patients who underwent ESG as a primary procedure.
Objectives: To report weight loss, morbidity, revisions, and co‐morbidity resolution during the first year in obese children and adolescents who underwent ESG under our care.
Methods: Our prospective pediatric bariatric outcomes database was queried for data on children and adolescents who underwent ESG under our standardized care protocol and clinical pathway. ESG was offered as a day‐case procedure. Standardized case report forms (CRFs) were used to collect relevant patient data at baseline and at regular intervals after the procedure.
Results: The 60 patients in this study had a baseline body mass index (BMI) and age of 33.0 ± 5.0 and 17.3 ± 2.5 (range: 11–21) years, respectively. Fifty‐five (91.7%) were females. Mean % excess weight loss at one (n = 55), three (n = 40), six (n = 37), nine (n = 21), and twelve months (n = 10) was 46.7 ± 29.6%, 58.7 ± 39.2%, 66.0 ± 42.2%, 79.2 ± 49.5%, and 60.0 ± 48.3%, respectively. One patient (aged 19.8 years) requested removal of endoscopic stitches due to abdominal pain. During the first five post‐procedural days, 34 patients (56.7%) required oral analgesia and antispasmodics for control of abdominal pain and nausea, and 19 patients (31.7%) visited the emergency room (ER). There were no ER visits after the first five post‐procedural days, and no patient reported receiving oral analgesia at one post‐procedure year. One patient had Redo‐ESG one year after primary ESG. There were no hospital admissions, mortality, or significant morbidity.
Conclusion: ESG appears to be safe and effective in children and adolescents with obesity. Significant weight loss occurs during the first year without mortality or significant morbidity. Oral medications for abdominal pain and nausea may be required in up to half of patients during the first five post‐procedure days.
S013 A NOVEL DESIGN AND APPROACH TO THE TREATMENT OF ESOPHAGEAL ATRESIA USING A MAGNETIC COMPRESSION ANASTOMOSIS
University of California, San Francisco
Background: Magnamosis is a magnetic compression anastomotic device intended for the creation of a leak‐free bowel anastomosis between any two portions of the gastrointestinal tract. While we have successfully used these novel magnetic rings for successful anastomoses in the stomach, small bowel, and colon, there were a number of unique challenges to the use of magnetic compression for the treatment of esophageal atresia and esophageal strictures.
Esophageal atresia is a disease for which treatment is primarily surgical resection of the diseased esophagus and anastomosis, with technical success limited by post‐operative complications driven by technical factors and the natural history of the disease, including anastomotic leak and esophageal strictures.
Objective: Our goal was to utilize the lessons from our small bowel experience with Magnamosis to create a new magnetic anastomotic device designed specifically for esophageal atresia. Our new design was created with consideration for the small size of the neonatal esophagus, the friability of the tissue, and an eye towards preventing stricture formation in the future.
Given numerous considerations about the pressure and compression of the tissue, and the need for a device design small enough for the esophagus yet with the appropriate demonstration of safety and efficacy: efficacy through enough magnetic force to ensure anastomosis creation and safety by prevent slippage of the magnets once mated at the anastomotic site.
Preliminary Results: We have designed and manufactured a new magnetic compression system specifically for esophageal atresia. These magnets measure 8 mm in diameter, are crafted directly from larger magnets, and have a unique design to create a compression gradient which will create tissue necrosis in the center of the anastomosis and a more gradual anastomosis creation at the periphery, resulting in gradually formed scar tissue. Additionally, we have engineered processes and design elements to render the magnets biologically compatible and nontoxic. As many prior animal models for esophageal atresia have demonstrated significant animal morbidity and translational challenges, we have devised a new swine model for esophageal atresia with our research partners. As such, we are currently testing this device in a swine model, with successful early results, demonstrating the successful delivery and mating of the magnetic system in the esophagus.
Conclusions/Future Directions: Ongoing studies are needed to further test this new magnetic anastomotic system, with longitudinal observation to evaluate the length of time needed to routinely create and evaluate a new esophageal anastomosis. Additionally, the strength of these anastomoses need to be further evaluated. Specifically, stratifying the distance between the two magnets relative to anastomosis creation is essential, as a principal goal will be to be able to address esophageal strictures, both in prevention and their treatment.
S014 VOLUME OF IRRIGATION DOES NOT AFFECT THE DEVELOPMENT OF ABSCESS IN PERFORATED APPENDICITIS
Nationwide Children's Hospital
Background: While previous studies have evaluated whether use of irrigation decreases abscess formation (St Peter et al. 2012, Hartwich et al. 2013), these studies treated irrigation as a dichotomous variable and concluded that no irrigation resulted in a decreased abscess rate (Hartwich et al. 2013). However, a recent study found decreased rates with small aliquots to a total of 6L (LaPlant et al. 2018). We hypothesized that larger volumes of irrigation would result in a lower abscess rate.
Methods: As part of a quality improvement initiative, a post‐operative template was developed. This template included descriptors for complex appendicitis and volume of irrigation (in milliliters) utilized. We prospectively collected data from November 2014 to September 2017 while monitoring the use of this template. We queried the data for cases of complex appendicitis, which was defined as purulent fluid or a fecalith within the abdomen, presence of a well‐formed abscess, or a visible hole in the appendix. Demographic information, pre‐operative variables, and post‐operative outcomes were collected. The volumes of irrigation were categorized based on liters used. A trend analysis was performed to assess the effect of increasing volumes of irrigation; a Cochran‐Mantel‐Haenszel test was utilized.
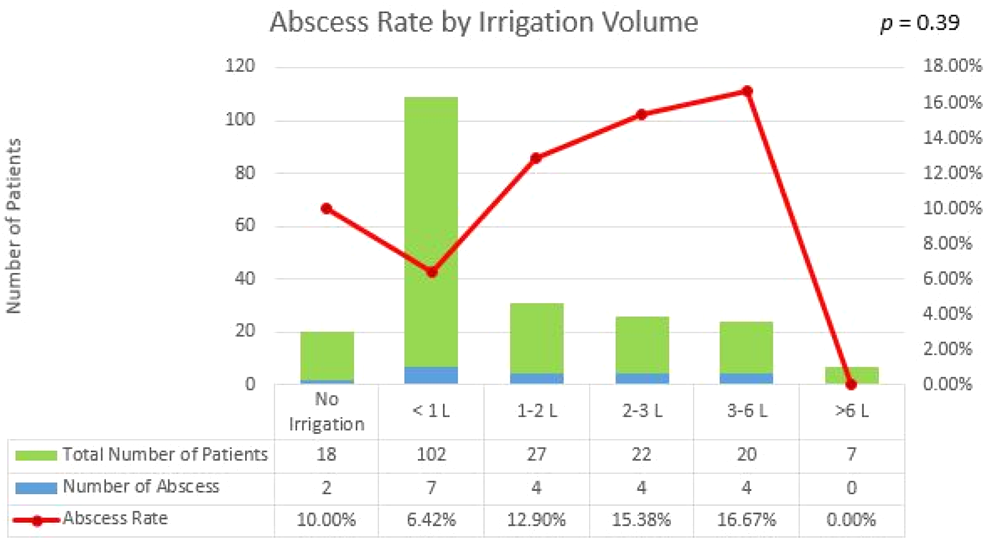
Results: The database contained 1534 appendicitis patients; 407 of these were complex appendicitis patients (26.5%). There were 217 patients with perforated appendicitis who had irrigation volumes recorded. The average age was 10.1 + 3.9 years. The overall abscess rate was 9.68%. Irrigation was commonly used (90.8% of patients). The median amount of irrigation used was 1000 mL (Interquartile range: 500 mL, 2500 mL), but ranged from 0 to 9000 mL. High risk patients (e.g. diffuse pus or well‐formed abscess) had higher volumes of irrigation used (1200 vs. 700 mL, p < 0.001). There was no overall difference in the volume of irrigation between those who did or did not develop an abscess in a bivariate analysis (p = 0.36). In a trend analysis, there was no overall difference in the rate of abscess development based on volume of irrigation (p = 0.39, see figure). Although 1L of irrigation resulted in a lower rate of abscess than no irrigation and 2–3 L of irrigation, this difference was not significant in individual comparisons (p = 0.62, p = 0.28). The volume of irrigation did not affect the size of abscesses when they developed (p = 0.6). A subset analysis of the high risk patients did not show a difference in abscess rate based on volume of irrigation.
Conclusions: The overall rate of intra‐abdominal abscess was 9.68% in patients with complex appendicitis. Although we hypothesized that the use of irrigation would result in lower abscess rates, the volume of irrigation did not appear to affect the rate of abscess formation. It is possible that patients with more severe disease received more irrigation so this analysis does not fully dismiss its value. The use of irrigation should therefore be left to the discretion of the operating surgeon.
S015 RESOLUTION OF TYPE 2 DIABETES AFTER SLEEVE GASTRECTOMY IN CHILDREN AND ADOLESCENTS: EIGHT‐YEAR RESULTS
Obesity Chair, Department of Surgery, King Saud University
Background: Bariatric surgery has proven efficacy in inducing significant weight loss and resolution of co‐morbidities, including type 2 diabetes mellitus (T2DM). However, the degree of resolution of T2DM in children and adolescents, and the maintenance of this resolution in the long‐term is yet to be demonstrated.
Objective: To report weight loss, and change in T2DM state in severely obese children and adolescents (aged 5–21 years) who underwent laparoscopic sleeve gastrectomy (LSG) under our care.
Methods: Data pertaining to all diabetic nonsyndromic children and adolescents who underwent LSG were abstracted from our prospective clinical outcomes study database. T2DM status was assessed at each follow‐up visit and was classified according to American Society for Metabolic and Bariatric Surgery outcome reporting standards.
Results: 2,019 children and adolescents underwent LSG during the study period, of whom 182 (9.0%) had T2DM at time of surgery. Baseline age and body mass index (BMI) were 13.7 ± 3.8 years and 53.2 ± 10.3, respectively, and 107 (58.8%) were boys. Fasting blood sugar (FBS), glycated hemoglobin (HbA1c) and fasting insulin for this group was 10.6 ± 5.6 mmol/L, 7.9 ± 2.1% and 46.0 ± 24.0 mIU/L at time of surgery, respectively. A total of 109 patients were on oral antidiabetics only, 45 were on oral antidiabetic + insulin, and 28 were on insulin only. All patients on oral antidiabetics, 82.2% of those on oral antidiabetics + insulin, and 67.9% of those on insulin only, achieved complete remission within the first year after surgery. All remaining patients experienced partial remission during the first year. No recurrence was observed in the subsequent years of follow‐up until the fifth year visit, when 1 patient who was on insulin experienced recurrence. Two patients previously on insulin + oral antidiabetic were restarted on oral antidiabetic at the fourth year after surgery.
Conclusion: LSG induces long‐term rapid and sustained remission of T2DM in children and adolescents.
S016 USE OF MAGNETS AS A MINIMALLY INVASIVE APPROACH FOR ANASTOMOSIS IN ESOPHAGEAL ATRESIA: LONG‐TERM OUTCOMES
1University of Chicago, 2Hospital de Niños “Sup. Sor Maria Ludovica”, 3WakeMed Physician Practices, 4Vanderbilt University, 5Mercy Children's Hospital and Clinics, 6University at Buffalo, Jacobs School of Medicine and Biomedical Science
Introduction: The majority of esophageal atresia (EA) patients undergo surgical repair with esophageal anastomosis soon after birth. However, factors due to the patient's characteristics, such as prematurity and other congenital anomalies, or anatomy issues, including a long gap between the ends of the esophagus and failed attempt of primary anastomosis initially, limit the ability to obtain esophageal continuity. A number of techniques have been described to treat these patients with “long gap” esophageal atresia, consisting of extensive mobilization, myotomies, esophageal flaps, and traction of the segments. The use of magnets is a nonsurgical alternative for esophageal anastomosis. The purpose of this study was to report long term outcomes for the use of magnets in the treatment of long gap EA.
Methods: Between 7/2001 and 12/17, 13 patients with EA underwent placement of a magnetic anastomosis catheter‐based system under fluoroscopic guidance at 6 institutions. The device promotes lengthening and approximation of the proximal and distal esophageal ends. After placement of the device, daily chest radiographs were obtained until there was union of the magnets. At this point the magnets were removed and replaced with an orogastric tube. Complications and outcomes were recorded. The average length of follow‐up was 9.3 years (range 1.42 to 17.75).
Results: 85% of the patients had type A, pure EA and 15% of the patients had a type C EA with previous ligation of the fistula. All of the patients had a gastrostomy. The average length of time to achieve anastomosis with the magnets was 6.3 days (range 3 to 13). There were no leaks in any of the patients and all had strictures requiring dilation (average number 9.8, range 3 to 22). 6 patients (46%) had esophageal stents placed for strictures and 2 patients underwent surgery. 92% of the patients were on full oral feeds at time of follow‐up.
Conclusion: The use of magnets for treatment of long gap EA is safe and feasible and accomplished good long‐term outcomes in this retrospective study. The main complication was esophageal stricture requiring dilation and stent placement and surgery in two of the patients in this cohort. A prospective, single‐arm, observational study is currently being initiated to evaluate the safety and benefit of the Flourish Device, a catheter‐based magnetic device used to lengthen the atretic esophageal ends to create an anastomosis for EA patients.
S017 DUODENAL ATRESIA REPAIR USING A MINIATURE STAPLER COMPARED TO LAPAROSCOPIC HAND‐SEWN AND OPEN TECHNIQUE
1Department of Pediatric Surgery, University Medical Center, Johannes Gutenberg University Mainz, Germany, 2Department of Pediatric Surgery, University of Leipzig, Leipzig, Germany, 3Institute of Medical Biometrics, Epidemiology and Informatics (IMBEI), Johannes Gutenberg University Mainz, Germany
Background: Laparoscopic duodenal atresia repair is a demanding procedure that requires performing a watertight anastomosis in a relatively small working space. Drawbacks of the approach have been high leakage rates and long operative times. We evaluated our initial experience with duodenal atresia repair using a miniature stapler (LA‐MS) and compared outcomes to a historic cohort of laparoscopic hand‐sewn (LA‐HS) and open repairs (OR).
Methods: A retrospective analysis of all patients who underwent surgery for duodenal atresia at our two centers between January 2010 and June 2018 was performed. Demographics, comorbidities, intra‐ and postoperative data and outcome parameters were evaluated and statistically analyzed.
Results: Duodenal atresia repair was performed in 44 patients. Ten patients underwent laparoscopic duodenal atresia repair using a miniature stapler, 21 patients laparoscopic repair with hand‐sewn anastomosis and 13 patients underwent open repair. Median age and weight at surgery was 13.5 d and 3300 g in the LA‐MS group, 4 d and 2750 g in the LA‐HS group and 4 d and 2222 g in the OS group, respectively. There were no differences concerning etiology of obstruction and comorbidities between groups. Mean operative time was significantly shorter in the laparoscopic stapled group compared to laparoscopic hand‐sewn anastomosis (145 ± 37 min (range: 97.0–217.0) vs. 201 ± 47 min (range: 119.0–275.0) p < 0.05). Duodeno‐jejunostomy (DJ) was performed more frequently in the laparoscopic stapled group compared to the hand‐sewn procedure (p = 0.007). Overall complication rate and need for re‐laparotomy were similar between groups. Time to initiation of feeds and time to full feeds were significantly shorter in the laparoscopic stapled group compared to the open approach (5 vs 11.9 d, p = 0.047 and 14.5 vs 24.4 d, p = 0.02) and similar in comparison to the laparoscopic hand‐sewn approach (5 vs 6.78 d, p = 0.1915 and 14.5 vs. 24.4 d, p = 0.2284).
Conclusion: Laparoscopic side‐to‐side repair of duodenal atresia using a miniature stapler is a novel, safe, and feasible technique that was associated with significantly shorter operating times than hand‐sewn laparoscopic duodenal atresia repair with a similar safety profile. Prospective studies are needed to confirm these findings. However, due to its simplicity, duodenal atresia repair using a miniature stapler has the potential to become the new standard of care.
S018 SLEEVE GASTRECTOMY IN 2,019 CHILDREN AND ADOLESCENTS: NINE YEARS LONG‐TERM OUTCOMES
Obesity Chair, Department of Surgery, King Saud University
Background: Bariatric surgery has proven safety and efficacy in inducing significant weight loss and co‐morbidity resolution in children and adolescents. However, long‐term evidence in this age group is yet to be reported.
Objective: To report single‐surgeon experience with long‐term weight loss and morbidity in severely obese children and adolescents (aged 5–21 years) who underwent laparoscopic sleeve gastrectomy (LSG) in our center.
Methods: Our standardized prospective outcomes research program database was queried for data pertaining to all nonsyndromic children and adolescents who underwent LSG since the inauguration of the program. Baseline and annual visit data regarding weight loss, readmissions and postoperative adverse events were analyzed for the purpose of this study.
Results: 2,019 children and adolescents underwent LSG during the study period. Baseline age and body mass index (BMI) were 15.2 ± 3.8 years and 46.4 ± 10 kg/m2. Male:Female ratio was 1:1. Mean % excess weight loss (%EWL) at one (N = 1,296), three (N = 503), five (N = 144), seven (N = 55), and nine years (N = 14) was 55.4 ± 21.5%, 79.1 ± 27.6%, 84.9 ± 39.1%, 86.3 ± 50.6%, and 71.6 ± 49.8%, respectively.
Among those who completed at least five years of follow‐up, 9.5% had occasional fatigability, and 19% had moderate‐to‐severe symptoms of gastroesophageal reflux disease (GERD). There were no bariatric‐related readmissions, significant morbidity or mortality after surgery
Conclusions: LSG induces significant, sustained long‐term weight loss without significant safety concerns, being the longest reported follow‐up to date. However, a fifth of patients developed long‐term symptoms of GERD, and a tenth reported occasional fatigability.
S019 LAPAROSCOPIC MANAGEMENT IN CHILDREN WITH CYSTIC LESIONS OF THE PANCREAS
1Sent Vladimir Children's Hospital, 2Children's Hospital named after Z.A. Bashlyaeva
Introduction: Laparoscopic surgery of the pancreas is still a relatively new field of pediatric minimally invasive surgery. The rarity of the occurrence of pathology in children, the retroperitoneal localization of the pancreas, the proximity of large vessels and the need for reconstructive interventions require pediatric surgeons to be highly skilled in minimally invasive surgery. We present our experience of laparoscopic procedures in children with cystic pancreatic lesions.
Patients and Methods: Since 2013, we performed laparoscopic operations in 63 children with various congenital and acquired diseases of the pancreas. Of these, 25 (39.7%) patients had cystic lesions of the pancreas: a posttraumatic or postnecrotic pseudocysts were present in 9, a solid pseudopapillary tumor in 8, a gastric duplication cyst with localization in the pancreas in 3, a congenital pancreatic cyst in 2, a lymphatic pancreatic cyst in 2, a hydatide cyst in 1. The following laparoscopic procedures were carried out: extirpation or enucleation of cystic mass (8), external or internal (Roux‐en‐Y cystojejunostomy) drainage of pancreatic cyst (8), spleen preserving distal pancreatectomy (4), the central pancreatectomy with distal Roux‐en‐Y pancreaticojejunostomy (3), and a pancreatic cystectomy with longitudinal pancreaticojejunostomy (2).
Results: Conversion rate was 8.0% and associated in 2 cases with large sizes of the cystic tumor or a pronounced adhesive process in abdominal cavity. In the early postoperative period, complications occurred in 2 (8.0%) patients: pancreatic fistula ‐ in 1 child and adhesive intestinal obstruction ‐ in another patient. In the long follow up, a pancreatic cyst was formed in the patient after hydatid cyst resection, which required an open Roux‐en‐Y cystojejunostomy.
Conclusions: Laparoscopy is an effective, feasible and safe method for treating children with cystic pancreatic lesions. The type of laparoscopic procedure is determined by pancreatic pathology, the age of the patients and the complications that have arisen.
S020 THORACOSCOPIC MANAGEMENT OF ESOPHAGEAL ATRESIA AND ITS RELATED COMPLICATIONS: LESSONS AFTER THE FIRST 106 CASES
1Hospital das Clinicas, 2Hospital Rebagliatti, 3Universidade Suprema
Introduction: The thoracoscopic approach for esophageal atresia (EA) repair is an important advance in pediatrics. Although authors have shown many advantages over thoracotomies, the needs for careful skills and devices for neonates have limited a more widespread use of this technique. The aim of the authors is to show experience on the first 106 cases, the lessons and useful technical hints for successful outcomes in all types of EA.
Patients and Methods: From Oct/2001 ‐ Feb/2018, 106 babies with EA were operated on thoracoscopically. The ages ranged 1 day ‐ 8 months, 66 males:50 females, weighing 1.280 – 7.400 g. The anomalies included types C (86), A (14), D (3), B (2) and E (1). The operations were performed with the patient in prone position with 30o elevation of the right shoulder, the trunk near the edge of the table, 3 miniports at the right thorax, or in many cases, a 2 or 3‐mm stab wounds with no trocars, mostly for the left‐hand instrument through the 8th intercostal space (IS). The right‐hand port was located under the right border of the scapula at the axilla, through the 3rd IS, the scope through the 5th or 6th IS. After installation of CO2, the lung was partially collapsed in most cases, but in some it was not adequate, so we developed tricks that helped better lung retraction (stiches and stylets). The azigos vein was divided only in the first 32 cases, and in some later ones when necessary. In neonates with right‐sided aorta, a right‐sided approach was also performed. In 12 type‐A cases, a thoracoscopic Foker 2‐step procedure was accomplished and a pouch flap was possible in other 2. Two had a previous open failed thoracotomy elsewhere, and the thoracoscopic anastomosis was performed thoroughly. The anastomosis were performed preferentially with extracorporeal sliding knots through the right port, 6 to 8 PDS or propylene sutures, with trans anastomotic tubes, all cases had a drain out from the scope port site.
Results: All cases were performed with no conversion, no operative deaths, there was no or minimal bleeding, mean operative time 62 minutes (40 min‐2.5 hours) for type‐C atresias. Five patients died in the week after operation due to concomitant severe anomalies, and 4 others later due to cardiac or neurologic complications. Esophageal fistula occurred in 4 of the first 50 patients, only one needed reoperation (thoracoscopic), and in 3 of the last 56, all closed spontaneously. Pathological reflux developed in 68/106 cases (64.2%), especially in long‐gap EA (21/23 – 91%). Lap fundoplication was necessary in 16 patients (23.5%). Tracheomalacia in 2 patients was treated by thoracoscopic aortopexy. Postoperative respiratory complications were minimal, there was no rib or thoracic wall complication, most of the scars tended to disappear.
Conclusions: The thoracoscopic EA repair can be safe and successful for all types and to treat complications of EA with advantages for the recovery period, in experienced hands in neonatal surgery. Comparative studies are needed to define if its better than open procedures.
S021 OUTCOME AND FACTORS AFFECTING THE POST‐OPERATIVE LENGTH OF STAY FOLLOWING VIDEO ASSISTED THORACOSCOPIC SURGERY (VATS) FOR EMPYEMA
Monash Children's Hospital
Background/Aims: VATS is indicated in children with an empyema not responding to medical treatment. However, there are several factors that could potentially affect the post‐operative length of stay (P‐LOS) that have not been fully investigated. We report on a large number of patients treated by VATS at single institution focussing on factors that could affect the P‐LOS.
Methods: A retrospective review (2013–2018) was performed on children treated with VATS and chest drain for empyema at a tertiary centre. The study was approved by the local ethics committee (RES‐18‐0000‐071Q). Statistics: results are reported as number of cases (%) and median [range] and were analysed by Mann‐Whitney U test and the Kruskal‐Wallis test. Correlation and multiple regression analysis were performed to identify factors related to prolonged P‐LOS.
Results: We identified 159 children with empyema; 75 (47%) children required VATS (Figure). Median age was 3.6 [0.4–14.5] years and there were 42 (56%) males. P‐LOS was 8 [3–47] days. Post‐operatively, chest drain was on suction in 30 (40%) patients and left in situ for a median of 3 [1–13] days. Six (8%) children required a second procedure (5 VATS, 1 thoracotomy, 1 additional chest drain). Median duration of pre‐operative symptoms before the VATS procedure was 7 [2–28] days. Presentation was: autumn 15 (20%), winter 26 (35%), spring 18 (24%) and summer 16 (21%); there was no difference in P‐LOS in different seasons (p = 0.6). Pleural fluid revealed: Streptococcus spp in 42 (56%), Other spp 6 (8%), no bacteria in 27 (36%); P‐LOS was significantly longer in the group with positive pleural fluid: 9 [4–47] vs. 6.5 [3–16] days (p = 0.02).
There was no correlation between the P‐LOS and the duration of pre‐operative symptoms (r = −0.03 [95% CI −0.3 – 0.2]; p = 0.7), the size of the empyema (r = 0.2 [95% CI −0.07 – 0.5]; p = 0.1) and the size of the chest drain (r = 0.09 [95% CI −0.14 – 0.3]; p = 0.4).
Multiple regression analysis suggested that the use of higher chest drain suction pressure post‐operatively was slightly associated with increased P‐LOS (p = 0.049).
Conclusions: In our experience, 50% of children admitted with empyema will eventually require VATS. Almost 95% of patients will be successfully treated with a single procedure with an average P‐LOS of 8 days. We identified positive culture from pleural fluid as the only factor affecting the P‐LOS. We also suggest that children post‐VATS might benefit from low or no pressure suction to the chest drain.
S023 20 YEARS' EXPERIENCE OF VATS FOR MEDIASTINAL MASS IN CHILDREN: A SINGLE‐INSTITUTION RETROSPECTIVE REPORT
Beijing Children's Hospital, Capital Medical University, National Center for Children's Health
Aim: The aim of this study was to review the clinical data of video‐assisted thoracoscopic resection of mediastinal mass in children.
Methods: This report included 1000 cases treated from January 1998 to September 2018. Reviewed the data on age, sex, histologic type, clinical manifestations, duration of surgery, blood loss, hospital stay, surgical complications and follow‐up.
Results: Of 1000 patients treated with this VATS resection, and all the surgery were successfully performed with no mortality. The median age was 3.8 years old (range, 2 weeks‐16years), and 581 for male, and 419 for female. 531 cases were on the right side of chest cavity, 451 cases on the left, 18 cases on the both side. 480(48.0%) cases of neurogenic tumors(includes neuroblastoma, ganglioneuroblastoma, ganglioneuroma, etc.). 166 (16.6%) cases of enterogenous cyst (includes bronchogenic cyst, esophageal duplication cysts, etc.). 100 (10.0%) cases of lymphoma, 73 (7.3%) cases of teratoma, 63 (6.3%) cases of lymphangioma/hemangioma. Other rare cases include primitive neurotodermal tumour, Castleman's disease, pleuropulmonary blastoma, lipoblastoma, thymoma, pericardial cyst, etc. The average tumor size was 5.4 cm in greatest dimension (range, 1.2–22 cm). The average duration of the operation was 82.2 minutes (range, 20–330 minutes). The average blood loss was 11.0 ml (0.5–500 ml). The mean hospital stay was 10.0 days (range, 4–38 days). 61 (6.1%) cases converted to open surgery, due to hemorrhea, severe adhesion, cardiac resuscitation, etc. Complication with trachea leakage, chylothorax and others. Follow‐up from 5 months to 16 years.
Conclusion: Video‐assisted thoracoscopic surgery resection of mediastinal mass in children were safe and feasible, and with minimally postoperative complications.
Keys: Mediastinal mass, VATS, children
S024 FROM THEORY TO PRACTICE: 3D RECONSTRUCTION AND PRINTING AS A VALUABLE TOOL FOR THE CHEST WALL SURGEON. IMPLEMENTATION IN A SERIES OF 105 CONSECUTIVE PATIENTS
Fundacion Hospitalaria
Objective: To assess the applicability of 3D reconstruction and printing for surgical procedures of the chest wall.
Materials and Methods: 105 consecutive patients from November 2015 to August 2018 were included and were divided into 3 groups:
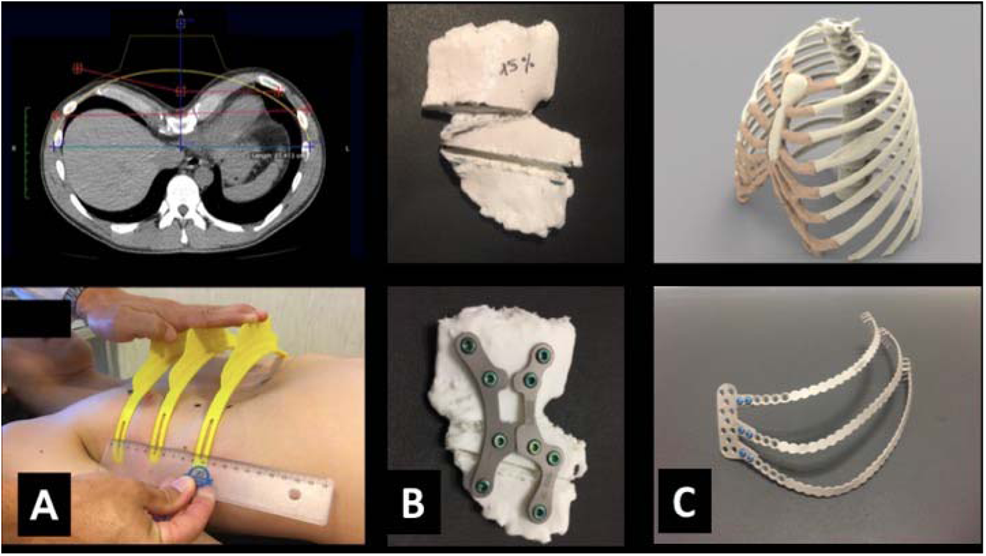
Pectus Excavatum and Carinatum: (A) a 3D printed template was generated after digital processing of 3D CT scan with a specifically designed software. Metal implants including lateral bridges were custom made for each patient following this template. (n = 99)
Poland Syndrome and Currarino‐Silverman: (B) a 3D impression of the patient's sternum was used as a model for surgical planning and manufacturing of custom made titanium sternal plates. (n = 5)
Malignant Costal Tumor: (C) a complete real size 3D printed chest was created, on which the team planned step by step the resection, reconstruction of the wall and appropriate fixation of the implants. A complex implant that included multiple ribs and sternal attachment was custom manufactured for a specific patient. (n = 1)
Results: The correction was achieved having previously planned the surgery step by step in all (100%) of the cases. There was no need to mold or modify the designed implants. The results were satisfactory in all the three groups.
Conclusion: Since November 2015 our team managed to implement (applicability) these tools (3D printing and reconstruction) in our current practice on a daily basis in all our chest wall surgical patients. We envision that in a near future these digital technologies may become available and accepted by most chest wall surgeons.
S025 BEYOND MAGNAMOSIS: A METHOD TO TEST SUTURELESS ESOPHAGEAL ANASTOMOTIC DEVICES IN LIVING PIGLETS BY CREATING AN ESOPHAGEAL BYPASS LOOP FOR NATURAL ORAL NUTRITION
1Pediatric Surgery, University Medicine of the Johannes Gutenberg University Mainz, 2Experimental Surgery, University Medicine of the Johannes Gutenberg University Mainz, 3Department of Surgery and Pediatric Device Consortium, University of California San Francisco
Background: Thoracoscopic esophageal atresia repair has become increasingly popular, but is still limited to a few expert centers and has some shortcomings. One of them is longer operation time compared to conventional thoracotomy, according to a recent meta‐analysis. The biggest challenge is suturing the anastomosis. Although magnetic anastomosis formation has been tried experimentally in seven published cases of esophageal atresia, severe stricture formation has been recorded. Since we believe that the shape and characteristics of the magnets play a fundamental role in the formation of the anastomosis and its later patency, we aimed to develop a porcine model to test magnetic anastomosis formation and at the same time allow the pig to eat in a natural way.
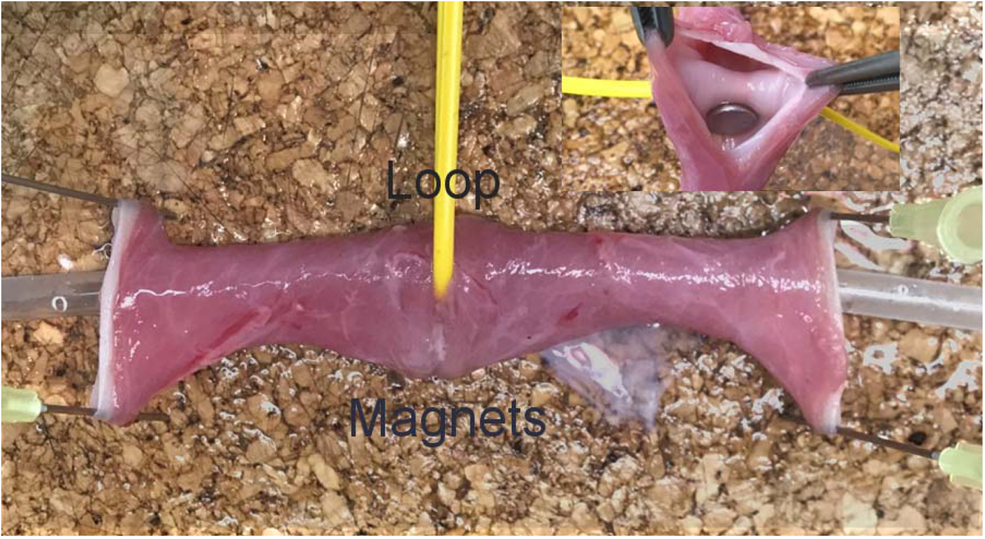
Methods: We used four Pietrain piglets aged eight weeks with a bodyweight of 15 kilograms to establish the living animal model after preceding cadaver tests. Our study was approved by the state's agency for the protection of experimental animals (permit: G‐17‐1‐033‐E1) and compliant with the directive 2010/63/EU. We performed a right‐sided thoracotomy in the fifth intercostal space, fully mobilized the esophagus to gain sufficient length to create an esophageal loop that served as a bypass for food after magnet deployment. The devices, two magnets of eight millimeters diameter, were per orally placed one after the other proximal and distal to the loop. They were separated by an elastic vessel loop to prevent slippage of the magnets into the lumen. The magnets were then approximated, forming a side‐to‐side approximation and later anastomosis. The thoracic cavity was closed in layers. Six hours later, patency of the bypass esophageal loop was assessed by passing an oro‐gastric tube, injecting Methylene blue proximally and documenting its passage into the stomach, as well as by allowing the piglets to drink after awakening from anesthesia. We also tested the device stability using the classical burst pressure test.
Results: The esophageal lumen was patent for feeding tube passed through the esophageal bypass loop into the stomach. The piglets were able to drink after recovering from anesthesia and the Methylene blue colored fluid reached the stomach without signs of obstruction. We did not observe coughing or regurgitation of fluids postoperatively. We applied burst pressures of 200,000 Pascal to the esophageal loop, but were unable to disrupt the magnets. At 6 hours after placing the magnets, we already saw subtle erosions of the esophageal mucosa indicating the beginning of anastomotic formation.
Conclusions: This animal model is useful to test different magnet designs for sutureless esophageal anastomosis. Our method allows the animals to feed post‐operatively, while the side‐to‐side anastomosis is formed. Our next step will be survival experiments in which the animals survive up to 2 weeks to characterize the evolution of the anastomosis and to assess stricture formation.
S027 OUTCOMES FOLLOWING DYNAMIC COMPRESSION BRACING FOR PECTUS CARINATUM
Children's Mercy Kansas City
Introduction: Pectus Carinatum (PC) is a chest wall deformity resulting in anterior protrusion of the chest. Some patients experience shortness of breath and chest pain, and they are particularly vulnerable to the psychosocial effects of poor body image and low self‐esteem. Non‐operative treatment of PC with orthotic bracing has been shown to be effective in PC correction. However, there are limited studies describing patient outcomes after achieving correction with bracing. We describe our experience with dynamic compression bracing (DCB) for patients who reached retainer mode and their satisfaction with bracing.
Methods: We reviewed a prospectively collected data of PC patients who underwent DCB from July 2011‐June 2018 at our institution. We included those who initiated bracing between 10 and 18 years of age and had at least four months of follow‐up. Data were analyzed for those who achieved correction and entered retainer mode, defined by a correction pressure of <1 psi. A telephone survey was conducted regarding ongoing brace use, self‐reported recurrence, limitations and motivations for brace use, whether they thought DCB was worthwhile, and overall satisfaction with the outcome of correction on a 1–10 scale.
Results: Of the 460 patients who met inclusion criteria, 144 (31%) reached retainer mode. Nine percent were female and 91% were male. Median age at bracing was 14 years (IQR 13, 15). Median carinatum height was 2 cm (IQR 1.5, 3), with a median initial correction pressure (PIC) of 3.7 psi (IQR 2.9, 4.6). Median time to retainer was 5.5 months (IQR 3, 10). 57% of patients were compliant with brace wear as instructed. There was no statistically significant relationship between median PIC or carinatum height and time to retainer mode (p = 0.08 and p = 0.10, respectively). Complications of bracing included skin erythema or acne (14%), problems with fit (14%), mechanical problems with the brace (8%), and rib flaring (5%). 63% had no complications. For compliant patients, median time to retainer mode was significantly shorter (3.5 mo. (IQR 2, 6) versus 10 mo. (IQR 6, 13), p < 0.001).
Of the patients contacted, 56 (38%) responded to the telephone survey. Median time to survey was 4.5 months (IQR 2.5, 25) after the last clinic visit. Barriers to compliance included discomfort (36%), embarrassment (13%), both (5%), and mechanical failure (2%). However, 45% reported no limitations. Motivations for compliance included appearance (59%), physiologic symptoms (14%), and parental influence (9%). All endorsed that the bracing process was worthwhile with 96% reporting a satisfaction rating of 8 or greater for the outcome of correction.
Conclusion: DCB for PC is effective in earlier achievement of correction in compliant patients compared to non‐compliant patients. Regardless of time to retainer mode, patients reported high satisfaction with bracing.
S028 THORACOSCOPIC LIGATION OF PATENT DUCTUS ARTERIOSUS IN INFANTS: MODIFICATION OF TECHNIQUES FOR CLOSURE IN NEWBORNS WEIGHING LESS THAN ONE KILOGRAM
Johns Hopkins All Children's Hospital
Background: Patent ductus arteriosus (PDA) affects approximately 39% of very low birth weight (VLBW <1500grams) infants and 61% of extremely low birth weight (ELBW <1000grams) infants. 6% of these are managed with surgical ligation in VLBW infants, rising to 13% in ELBW infants. Infants undergoing open surgical repair have a 25% risk of developing chest wall deformities, a risk that is only partially attenuated by a muscle‐sparing approach. Thoracoscopic PDA ligation has been shown to be a safe and effective alternative to open surgical approach, with the advantage of lower risk of associated chest wall deformity. Thoracoscopic difficulty often increases with decreased weight of the baby. In thoracoscopic PDA ligations in VLBW and ELBW infants, we modified our technique to increase success and safety. Currently, there is a dearth of literature and video footage detailing the technical modifications necessary to complete thoracoscopic PDA ligations in these small infants. We demonstrate a technique of thoracoscopic PDA ligation that has resulted in excellent outcomes.
Methods: Thoracoscopic PDA closure was performed by a single surgeon starting in October 2014. Echocardiogram demonstrated large left‐to‐right shunting PDA. Babies were symptomatic and unable to wean off respiratory support. Operative weights were greater than 800 grams (less than 800 grams were performed via thoracotomy). Technique of closure is as follows: setup included cuffed single lumen endotracheal tube, peripheral IVs, arterial line when possible, pulse oximetry, blood pressure cuff, decubitus position. Starting HCT >30 with blood available in the OR. Three ports were utilized (4.7mm for camera, 3.5 mm for retracting grasper, 5mm for working cautery/clip applier). Insufflation 4mmHg. Camera port was inferior to the scapula tip. Other ports were initially placed as inferiorly as possible in the thoracic cavity, with the working port posterior by the spine. Key modifications to the technique to improve visualization and safety were: moving retracting port more posterior so grasper is not in lung fissure, moving working port slightly cephalad to avoid instrument interactions, changing from a 5mm laparoscopic clip applier to a 6.6mm curved brain aneurysm clip. Pleura overlying aorta was scored with cautery and retracted medially to expose PDA and shift recurrent laryngeal nerve (RLN). Once isolated, test clamp was performed and clip applied to PDA. Chest insufflation was evacuated with no chest tubes placed. A modified “minimal dissection” technique was applied to extremely low weight babies for added safety.
Results: Thoracoscopic PDA closures during this period were completed safely and without significant complications. There were no deaths, no significant blood loss, no RLN injuries, and no great vessel injuries. Operative chest tubes were not placed because the insufflation was evacuated at the end of the operation. Follow up echocardiograms demonstrated closure of PDA. Operative time decreased with the learning curve and technique modification and is now typically 30–40 minutes.

Conclusion: Thoracoscopic PDA ligation technique presented here is effective and safe in ELBW infants. Given the known risk of chest wall deformity in infants undergoing thoracotomy, the thoracoscopic technique should be considered as an alternative to the open approach.
S029 MANAGEMENT OF PRIMARY OBSTRUCTIVE MEGAURETER IN CHILDREN AND MINIMAL INVASIVE SURGERY
1Department of Pediatric Surgery, University Hospital Arnau de Vilanova, 2Department of Pediatric Surgery and Urology, University Hospital Vall d' Hebron
Introduction: Conservative management of POM appears as the best option in patients with adequate ureteral drainage. Nevertheless, surgical intervention is indicated in POM with recurrent UTIs, deterioration of split renal function and significant obstruction. Ureteral tapering and reimplantation is an established treatment in patients with POM.
Our objective is to evaluate the efficacy, security and comunicate ours results in the treatment of Primary Obstructive Megaureter by Laparoscopic‐Assisted Extracorporeal Ureteral Tapering Repair (EUTR) and Laparoscopic Ureteral Extravesical Reimplantation (LUER) and compare with endoscopic balloon dilatation in Pediatrics patients.
Materials and Methods: Data was collected retrospectively through the reviewed of the clinical records of 26 patients diagnosed with POM between January 2011 and January 2018. All patients underwent laparoscopic ureteral reimplantation by following Lich Gregoir technique and extracorporeal ureteral tapering repair was performed according to Hendren technique in 20 patients.
Results: In 20 patients EUTR and LUER were realized and complete successfully without conversion. In 6 patients was not necessary to performed tapering because the diameter of the ureter allowed us to realize the reimplantation without difficulties. There were no major intraoperative complications. After large‐term follow‐up, all patients were asymptomatic without recurrence of POM or VUR.
Discussion: Ureteral re‐implantation with or without tapering is the gold standard treatment for progressive or persistent POM. The most significant short‐term complications are urinary leakage, and long‐term complication includes ureteral stricture and VUR. In our patients EUTR and LUER were realized and complete successfully without conversion. No patient presented urinary leakage or experienced voiding dysfunction. Only one patient presented a VUR that required a redo with excellent results postoperatively. To perform our surgical technique, age does not seem to be a limiting factor. After long‐term follow‐up, all patients were asymptomatic without recurrence of POM or VUR.
We believe that Laparoscopic‐Assisted Extravesical Ureteral Reimplantation and Extracorporeal Ureteral Tapering Repair could be selected as a first technique in the Primary Obstructive Megaureter treatment since it is minimally invasive, secure and reaching satisfactory results.
S030 LAPAROSCOPIC PYELOPLASTY FOR 44 CASES OF SEVERE HYDRONEPHROSIS IN INFANTS
Children's Hospital of the Capital Institute of Pediatrics
Objective: To compare the safety and feasibility of laparoscopic pyeloureteroplasty in infants with ureteropelvic junction obstruction between 0–6 months and 7–12 months.
Methods: We retrospectively reviewed 44 infants younger than 12 months with severe hydronephrosis who underwent laparoscopic pyeloplasty from January 2016 to June 2018. They were divided into two groups according to age: 0–6 months group (27 cases) and 7–12 months group (17 cases). The mean renal pelvis anteroposterior diameter in 0–6 months group and 7–12 months group were (3.74 ± 1.09) cm and (3.17 ± 0.66) cm, respectively. The preoperative renal cortex thickness was (1.41 ± 0.33) mm and (1.85 ± 0.46) mm, respectively. All the children were treated by laparoscopic pyeloplasty by the same Surgeon.
Results: The operation process were successfully performed in all patients. There was no conversion and intraoperative complication. There was no statistical difference in the mean operative time, intraoperative blood loss, and postoperative hospital stay between the two groups. The patients were followed up from 1 to 36 months with ultrasound. The renal parenchymal thickness were increased, the renal pelvic anteroposterior diameters were reduced and the renal functions were improved in 42 patients. The mean postoperative renal pelvis anteroposterior diameter in 0–6 months group and 7–12 months group were (1.25 ± 0.46) cm and (1.18 ± 0.48) cm, respectively. The preoperative renal cortex thickness was (3.22 ± 0.65) mm and (3.27 ± 0.72) mm, respectively. The difference in preoperative and postoperative AP values between the 0–6 month group was greater than that in the 7–12 month group, P = 0.038. One case in each group had no improvement after 1 year of operation, and was cured again by open surgery. The cure rates of the two groups were 96.3% and 94.12%, respectively.
Conclusion: Laparoscopic pyeloplasty for infants younger than 6 months with severe hydronephrosis is safe and effective. Therefore, laparoscopic pyeloplasty should be performed early in children with UPJO who have surgical indications from 0 to 6 months of age to relieve obstruction and protect kidney function.
S031 MULTICENTER STUDY OF LAPAROSCOPIC PYELOPLASTY IN CHILDREN, ANALYSIS OF 327 SURGERIES LOOKING FOR THE STANDARD
1Exequiel Gonzalez Cortés Hospital ‐ University of Chile, 2University of Chile, 3Exequiel Gonzalez Cortés Hospital, 4Great Ormond Street Hospital, 5Italian Hospital, 6Garraham Hospital
Introduction: Although the classic approach for Anderson‐Hynes (AH) pyeloplasty has been through a lumbotomy, since the 90s the minimally invasive approach has shown to have the same results as the open technique. Our objective is to analyze the experience of 4 centers where laparoscopic pyeloplasties are performed, looking for if this technique has been standardized.
Material and Method: Descriptive retrospective study of all patients undergoing laparoscopic transperitoneal AH pyeloplasty between 2009 and 2017; with at least 6 months of follow‐up at Exequiel González Cortés Hospital (Santiago, Chile), Great Ormond Street Hospital (London, England) and Italian y Garraham Hospital (Buenos Aires, Argentina). It was evaluated with ultrasound and renogram before and after surgery. Demographic data, perioperative characteristics, complications and results are described.
Results: In the 9 years, 319 patients were operated; 211 men and 116 women. Eight cases had bilateral Uretropelvic Junction (UPJ) Obstruction. Of the 327 UPJ units, 110 were right, 5/327 were duplex kidneys and 5/327 were horseshoe. With prenatal diagnosis there were 112 patients (34%). Average age at surgery was 95 months (range 1–216 m); 8.5% (n = 28) were infants under 6 months and 13.7% (n = 45) under 1 year. Average weight to surgery was 29 kg (range 4–106 k), where 8.3% (n = 17) weighed less than 7 kilos and 19.6% (n = 40) less than 10 kilos. Average skin‐to‐skin time was 133.15min. (range 60–442 m), including residents and staff. After 24 months of average follow‐up (range 6–86 months). The percentage of complications corresponds to 5%, highlighting the stenosis and leakage of anastomosis.
Conclusion: From the standardization of laparoscopic pyeloplasty the times and results progressively improve so it can be one of the first options to analyze with the parents.
S032 EVOLUTION OF MINIMALLY INVASIVE SURGERY (MIS) IN PEDIATRIC UROLOGY IN A SINGLE PEDIATRIC CENTER
Department of Pediatric Surgery and Pediatric Minimally Invasive Surgery and New Technologies, San Bortolo Hospital, Vicenza, Italy
Aim of study: to assess and evaluate the evolution of surgical MIS approaches in pediatric urology in our Centre focusing on techniques and trends of various urological procedures comparing operative time (OT), postoperative complication‐rates, outcome between MIS and Open procedures.
Methods: We analyzed surgical urological procedures in our department (2002–2017) identifying children undergoing Open and MIS procedures recording any intra‐operative/post‐operative complications. 312pts (181M,131F) were studied for congenital anomalies/urologic diseases: intrinsic/extrinsic UPJO(hydronephrosis), dysplastic kidney, vesico‐ureteral‐reflux nephropathy, kidney cystic disease, dysgenetic kidney.
Main results: 312pz; 182 presented an UPJO: 141 an intrinsic obstruction which underwent to Anderson‐Hynes pyeloplasty; 70‐Open(OP), 14‐laparoscopic(LP), 57‐retroperitoneoscopic(RP). In all patient were placed a JJ‐stent removed after 30–40 days and a perirenal drainage removed after 2 days. Equivalent intra/postoperative complication rate. As complication we recorded: 1 re‐obstruction; 2 IVU; 1leakage. OT was of 3½h. 41 patient presented an extrinsic UPJO: 36 underwent to Laparoscopic Vascular Hitch (LVH). OT was of 95'; average hospital stay 4 days; As complications we recorded 1 re‐do LP‐pieloplasty after 2 years. 61 patients underwent nephroureterectomy: 20‐OP with average age of 6 years; the OT was of 90'; 41‐were treated by RP, the average age 4.5 years, OT 140'. 69 patients underwent heminephrectomy: 30‐OP, 39‐RP with same OT (120'). Complications: 1 urinoma (conservative treatment), 2 ureteral symptomatic stumps (LP‐treatment).
Conclusions: Higher‐volume MIS centers is associated to a lower complication‐rate than lower‐volume centers. Our study shows as transition from open‐surgery to MIS requires great experience, experienced team, an adequate learning curve. MIS is associated with lower postoperative complication rate than open procedures. According us RP is preferable and suitable in patients younger 2‐years in experts' hands in performing hemi/nephrectomy or AHDP contrasting with literature which describes it as a technically demanding procedure with significantly higher complications and re‐operation rate compared to LP.
S033 LAPAROSCOPIC AND RETROGRADE INTRALUMINAL ENDOSCOPIC RENAL AND URETERAL STONE SURGERY IN CHILDREN
Eskisehir Osmangazi University, School of Medicine, Department of Pediatric Surgery, Division of Pediatric Urology
Retrograde intraluminal endoscopic renal and ureteral lithotripsy with rigid or flexible ureterorenoscopy (URS) is one of the main treatment modalities for ureter and renal stones. In case of difficulty of ureteral access and reaching to stone by URS, laparoscopy might be used to retrieve the stone. The aim of this study is to define an endoscopic management algorithm for ureteral and renal stones.
Material and Methods: Lithotripsy by rigid and flexible URS was performed in 124 children, while 7 patients needed laparoscopic stone removal (LapSR). Data and some tips and tricks to make the procedure easier were defined.
Results: The age range of the patients was between 10 months to 17 years. Retrograde laser lithotripsy with rigid URS was done for stones in ureter and renal pelvis (n: 86). Flexible URS was performed for stones in renal pelvis and lower pole calyx (n: 38). Stone size was between 5 to 17 mm. JJ Stenting was needed in 97 patients. Stone free rate after the first procedure was 74.2% and 93.5% after the second lithotripsy. The patient having nonopaque, multiple, enclaved stones with difficulty of access or associated with ureteropelvic junction (UPJ) obstruction needed LapSR. Two stones embedded in distal ureter, three stones in UPJ were removed by laparoscopy. Two renal pelvic stones were extirpated during laparoscopic pyeloplasty.
Conclusion: Age of the patient, stone type and location, difficulty of access and associated pathologies determine how we can treat the renal and ureteral stones. If there is a difficulty of performing retrograde intraluminal endoscopic procedures, LapSR could be considered as a better option to open surgery.
S034 WHEN VISION IS EVERYTHING; ANALYSIS OF A PEDIATRIC SERIES OF LAPAROSCOPIC MANAGEMENT OF RECURRENT PYELOURETERAL OBSTRUCTION
1Exequiel Gonzalez Cortés Hospital, 2University of Chile, 3Exequiel Gonzalez Cortés Hospital ‐ University of Chile
Introduction: Although the Anderson‐Haynes pyeloplasty presents a low complication rate, there are cases that require a reoperation of a recurrent obstruction. All reoperation is a complex surgery, specially because of the fibrotic tissue of the previous intervention, which in a new lumbotomy can be even more difficult. Our objective is to evaluate patients undergoing laparoscopic transperitoneal pyeloplasty with a diagnosis of recurrent pyeloureteral obstruction, analyzing whether this approach offers advantages or not.
Material and method: Retrospective descriptive study of all patients undergoing Anderson‐Hynes pyeloplasty (lumbotomy and laparoscopy) between January 2009 and December 2017. Patients who required a re‐intervention due to recurrent ureteropyelic junction obstruction (UPJO) were included. Demographic data, perioperative characteristics, complications and results are analyzed.
Results: In 9 years period there were a total of 167 performed pyeloplasties; 14 of them presented pyeloureteral obstruction again. Of those, 8/14 were resolved laparoscopically; 2 cases were initially operated open (lumbotomy) and 6 laparoscopically. Seven were males. Time for reoperation after first surgery was 24 months (range 3–120 m). Average surgery time was 159 min (range 125–220 m). In all laparoscopic cases, the ureteral junction was with considerable fibrotic tissue, where transperitoneal laparoscopic vision allowed the correct identification of the anatomy for careful dissection and allowing to perform a new pyeloureteral anastomosis in a comfortable way. After 47 months (range 19–70 m) follow up, all patients are asymptomatic and with non‐obstructive dynamic renography.
Conclusion: Any patient reoperation is a stressful event for any surgeon. That is why looking for a way that guarantees a high success rate of the new pyeloplasty is almost mandatory. This series shows that the transperitoneal laparoscopic approach provides a vision and approach to the problem allowing this complex surgery to be carried out effectively and comfortably with an excellent success rate, making it the first option in recurrent UPJO.
S035 VIDEOASSISTED MANAGEMENT OF WILMS TUMOR: A 16‐YEAR EXPERIENCE
1Hospital Araujo Jorge, 2Unifan
Introduction: The classic Wilms' treatment is currently multimodal, and preoperative chemotherapy (POC) has allowed better operations, both through an open approach and through videolaparoscopy, due to the cytoreduction of the mass, stiffening of the capsule and disappearance of lymph node nodal metastases. There are very few reports of laparoscopic treatment of nephroblastomas, being the pioneers the service of Duarte et al. in Brazil, all showing advantages of the minimally invasive access, allowing good visualization and removal of the kidney through an aesthetic and less morbid suprapubic incision. The objective of the authors is to present their 16‐year experience with laparoscopic assisted resection of nephroblastomas, presenting technical details, oncological aspects and outcomes of late follow‐up.
Patients and methods: Between march/2001 and march/2017, 38 children presented Wilms tumor at ages ranging from 1.5 to 6.6 years, clinical stages I, II and III and all were treated according to the SIOP protocol, with vincristine, actinomycin‐D, adriamycin. Preoperative tumor diameters ranged from 6.5 to 20 cm, all of which decreased with chemotherapy. The indications for video‐assisted treatment were maximum preoperative mass diameters of 6–8 cm (depending on the size of the child), predicted stages I to III. Using 3 trocars, transperitoneal approach, visceral retractions using sutures and stylets, vascular management with harmonic shears, or ligations with sutures and bipolar cautery, the tumoral kidneys were released from their original sites, and removed with adjacent peri‐renal fat and suspected peri‐aortic and peri‐cava lymphnodes and eventually an adrenal gland (tumors of the upper pole), through a Pfannenstiel incision, inside a plastic bag and without any muscular section. The kidney‐tumor boundaries were metal‐clipped (for eventual radiotherapy) and the incisions closed normally. Patients continued the postoperative chemotherapy protocol until the period of remission in our multiprofessional cancer service.
Results: All children evolved without intercurrences, no ICU admission, only one large‐mass removal required transfusion, no conversion, no complications related to video‐surgery or anesthesia, no trocar implants after a follow‐up period of 1.5 – 16 years (mean 10.3 years). The pathology confirmed nephroblastoma, the postoperative stages were [I] = 24 (63%); [II] = 10 (23.6%); [III] = 4 (13.4%). In the follow‐up period, no relapse was detected so far, even at stage III.
Conclusions: Laparoscopy is feasible and oncologically effective in the treatment of Wilms tumor up to 6–8 cm wide, using 3 ports, applying the main oncological principles, helped by hemostasis with energy devices and the multimodal treatment.
S036 LAPAROSCOPIC NEPHRON‐SPARING SURGERY FOR WILMS TUMOR: EXPERIENCE IN A HIGH COMPLEXITY MEDICAL
1Imbanaco Medical Center, 2Universidad Javeriana de Cali
Introduction: Surgical resection is the mainstay of Wilms tumor treatment. Although mortality has been reduced with a multidisciplinary management, to minimize morbidity the laparoscopic approach has been applied in patients with good results.
Objective: To describe the experience of the nephron‐sparing surgery for Wilms tumor in three patients in a high complexity medical center.
Methods: The present study describes the experience obtained from three patients with diagnosis of Wilms tumor treated with neoadjuvant therapy and underwent nephron‐sparing surgery according to the control scans. The clinical variables, the surgical technique and the outcomes are described.
Results: All three patients were taken to nephrons‐sparing surgery by intraperitoneal laparoscopic technique using 3 and 4 trocars; The tumor was dissected with Hook leaving a 3 mm margin. The extraction of the tumor was made by incision of Pfannenstiel with bag and left drain which was removed between 3–4 days. Only one patient presented postoperative urinoma which was drained by interventional radiology. The pathology report was favorable for all three patients.
Conclusions: This surgical technique is new and controversial and there is limited published literature about it. The challenge for the surgeon is to preserve the pre‐established oncological principles to prevent rupture and partial resection of the lesions. According to the experience presented we believe that if performed by experienced surgeons in a patient with adequate characteristics, this technique is feasible and will manage to reduce morbidity.
S037 LAPAROSCOPIC APPROACH FOR PEDIATRIC ADRENAL TUMORS
Hospital Italiano de Buenos Aires
Introduction: The role of laparoscopic surgery for the management of pediatric adrenal tumors has not been well defined, because of their low incidence and varied presentation. Aim: To evaluate our results in the minimally invasive approach for the diagnosis and treatment of children with adrenal tumors.
Methods: Retrospective analysis of consecutive pediatric patients with diagnosis of an adrenal tumor who were operated through a laparoscopic approach between January 2003 and August 2018. Institutional electronic records and prospective Pediatric Surgical Oncology database were reviewed. Laparoscopic approach was indicated for a tumor diameter of up to 6 cm as indicated by imaging.
Results: 28 patients were included. In 20 (71%) a complete tumor resection (R0) was performed, and in 8 a tumor biopsy was obtained (R2). There were no R1 resections in the series. 18/28 were male. Age (median): 5.2 ys (r:2 m‐18 ys). 14/28 (50%) were localized in the left side, and 2 bilateral. Clinical presentation: 16/28 (57%) incidental finding in ultrasound because of abdominal pain. Mean operating time: 109 min (45–180 min.). Mean tumor size (for resections): 4 cm. (r: 2.5–7 cm) Pathology: Neuroblastoma (n = 17), Ganglioneuroma (n = 7), Adrenocortical carcinoma (1), metastasis of Osteosarcoma (1), Pheochromocytoma (1), Venous malformation (1). Complications: Conversion to open surgery was required in 1 resection case, because of uncontrollable bleeding; jejunal perforation in 1 biopsy case. Mean hospital stay: 2.1 days (r: 1–3). Mean follow up: 43 ms (r:1–174).
Discussion: Laparoscopic adrenalectomy is feasible and safe in children with a variety of oncological diagnosis. Laparoscopic biopsy is useful for unresectable tumors when a percutaneous approach is not possible. Although advanced technical skills are required, we conclude that laparoscopic approach should be the first option for resection of adrenal tumors under 10 cm in diameter. Further collaborative research is required to warrant inclusion of this approach in oncology treatment protocols.
Keywords: laparoscopic adrenalectomy, minimally invasive surgery, neuroblastoma, adrenal tumors.
S038 SURVEY: TECHNICAL ASPECTS OF PYELOPLASTIES IN THE TREATMENT OF URETERO‐PELVIC JUNCTION OBSTRUCTION
“Queen Fabiola” University Children's Hospital Université Libre de Bruxelles (ULB)
Aim: The treatment of uretero‐pelvic junction obstruction (UPJO) is performed by different approaches: open (anterior, antero‐lateral, posterior), laparoscopic (retroperitoneal, transperitoneal), laparoscopic assisted, laparo‐endoscopic single site (LESS), robotic. We tried to have an overview of technical preferences among the members of IPEG.
Material and method: A Monkey survey containing a questionnaire with 16 items regarding the details of pyeloplaties was sent by email to the IPEG members. The data were collected anonymously.
Results: We received 101 answers. Most of the surgeons (49,50%) operate between 0–9 UPJO per year. Most of the time, 58%, were operated by a senior surgeon. Preoperative diagnostic workup includes in majority of the answers ultrasound ant scintigraphy. From the responders 84,69% operates UPJO under 1 year old. Concerning the operative technique there is a variability according to the age: 89,71% prefer open surgery below 1 year, while laparoscopic surgery (78,26%), retroperitoneoscopic surgery (83,33) and robotic (92,31)is the technique of choice for the children older than 2 years. If the obstruction is caused by a lower pole vessel and there is no ureteral intrinsic stenosis most of the surgeons prefer Hynes‐Anderson pyeloplasties. Concerning the sutures the most frequent used are running stitches with absorbable braided or monofilament. The transanastomotic stenting is performed more frequent by JJ stent usually for 4 weeks and Pippi‐Sale stent for 1 week. In open surgery 33,80% of the surgeons drain the operating site while in the other technique it is less used. The antibiotics are administered during surgery or during the hospital stay. The follow‐up is done by ultra‐sound with a preference at 3 months post‐operatively and scintigraphy at 6 months. Long‐term follow‐up is frequently until adolesce. If during the follow‐up, a patient has obstruction at scintigraphy but is asymptomatic and renal function is good, majority of the surgeons “wait and see” with regularly control (ultrasound and scintigraphy) before re‐do surgery. The subjective rate of recurrence is 0‐5%. In case of anastomotic stricture 42,71% perform an open redo‐surgery.
Conclusions: There is a great variety in technical details. Laparoscopic, retroperitoneoscopic, robotic pyeloplasties require special skills, training, learning‐curve and there are preferred in older children. Below 1 year of age open surgery is mostly used. Transanastomotic stent is performed regularly. Prospective studies and long‐term follow‐up and are necessary to have objective data.
S039 MANAGEMENT OF CYST VARIATION DURING LAPAROSCOPIC CHOLEDOCHAL CYST OPERATION
Department of Pediatric Surgery, the 2nd Affiliated Hospital of Harbin Medical University
Objective: There is a risk of canceration because of the cyst wall is repeatedly stimulated by cholangitis. Complete excision of choledochal cysts is currently regarded as the gold standard treatment. In addition to the cyst types of Todani, special types of cysts are often seen during surgery. If the cyst is not recognized, it may lead to surgery related complications.
Methods: We reviewed 126 patients who had undergone laparoscopic excision of choledochal cyst. The data was analysed for operative time, type of choledochal cyst, intraoperative problems, postoperative complications and postoperative follow up.
Results: From Jan 2009 to Dec 2017,126 patients have undergone laparoscopic surgery for choledochal cyst. Mean age was 4.5 years old (6 days – 16 y), 28 boys and 98 girls.
All patients had been recognized type I (96 spheroida dilatation and 30 spindle dilatation of common bile duct) before operation. The cyst diameter was 1.5 to 15 cm. Fourteen cases of cyst variation were found during operation, including 1 case of simple common hepatic duct (CHD) dilatation and normal common bile duct (CBD), 1 case of CBD spindle dilatation with spheroida dilatation of CHD, 2 cases of CBD cucurbit dilatation with proximal bile duct stenosis, 2 cases of CHD stenosis caused by right hepatic artery straddling, 5 cases proximal hepatic duct stenosis of choledochal cyst, and 3 cases of pseudocyst formed by wall penetrating ulcer of choledochal cyst.
All patients were treated with laparoscopic choledochal cyst resection and Roux‐en‐y hepaticodocho‐jejunostomy inludeing 2 cases with external drainage and 2 cases of cyst perforation underwent laparoscopic peritoneal drainage for the first time. Mean operative time was 240 minutes (180 – 410 minutes). Mean intraoperative blood loss was 25 ml (10–100 ml). No patients were converted to open surgery. There were no intraoperative side injuries.
Postoperative complications included: Bile leak was seen in 5 patients, four were treated conservatively and one patient required abdominal puncture drainage. Adhesive intestinal obstruction was seen in 2 girls, one was treated by redo‐laparoscopic operation in post‐operation fifth day and another was treated conservatively. Residual stone was found at distal common bile duct in perioperative period, the stone disappeared without treatment in second follow‐up months. Mean hospitalisation was 6.5 days (5 – 9 days). Follow‐up from 6 months to 7 years, two patients had cholangitis which reverted to normal after antibiotic therapy. Two boys ill with stenosis of biliary‐intestinal anastomosis were operated by redo laparoscopic hepatico‐jejunostomy in one month and three month respectively after the first operation.
Conclusions: Careful reading of various examinations before surgery combined with cholangiography during operation can effectively detect cyst variation. For patients with CHD dilatation, attention should be paid to the opening of normal and the vagal bile duct to avoid side injury caused by cyst wall excision. The distal and proximal CBD should be explored, and proximal bile duct stenosis should be found and treated.
Keywords: Choledochocyst; Laparoscopic operation; Complications; cyst variation
Acknowledgments: The research support by Supported by NSFC No.81272049 and 81572117.
S040 BILE DUCTOPLASTY FOR HILAR AND INTRAHEPATIC BILIARY DUCT STENOSIS AND COMPLETE INTRAPANCREATIC BILIARY DUCT RESECTION BY LAPAROSCOPIC CHOLEDOCHAL CYST EXCISION
Department of Pediatric Surgery, Nagoya University Graduate School of Medicine
Purpose: Intrahepatic lithiasis due to biliary duct stenosis and repeated pancreatitis due to residual intrapancreatic biliary duct are the main postoperative complications after choledochal cyst excision. We pursued complete excision of intrapancreatic biliary duct and resolution of hilar and intrahepatic biliary duct stenosis (HIBDS) by laparoscopic choledochal cyst excision. HIBDS treatment and intrapancreatic biliary duct excision has infrequently been reported in laparoscopy. We aimed to determine whether laparoscopic treatment is a feasible and safer option than open surgery for the indicated conditions.
Methods: We retrospectively reviewed the medical records of 79 patients who underwent open or laparoscopic choledochal cyst excision with hepaticojejunostomy during 2010–2018 at our institution. HIBDS was defined by a narrowing of the lumen of the bile duct compared with the more peripheral bile duct, or as the blocking of contrast medium in the intrahepatic duct, as detected by preoperative ERCP, or MRCP. During surgery, HIBDS were meticulously searched to detect HIBDS‐causing membrane or septum by cholangioscopy.
Results: Of the 79 subjects, 44 underwent laparoscopic choledochal cyst excision (Lap group) and 35 underwent open choledochal cyst excision (Open group). The operative time was significantly longer in the Lap group than in the Open group (361 versus 252 min, p < 0.05); however, the amount of blood loss was significantly smaller in the Lap group than in the Open group (46 versus 93 mL, p < 0.05). The operative bile ductoplasty for HIBDS was performed at nearly the same rate between the two groups (52% versus 63%, respectively). Postoperative complications (>Clavien–Dindo III) occurred equivalently in both groups (6.8% versus 2.9%, respectively). Postoperative magnetic resonance imaging revealed residual intrapancreatic biliary duct (>5 mm) in 0 and 3 cases after laparoscopic excision and open surgery, respectively.
Conclusion: We conclude that, in the short‐term, the treatment of HIBDS and complete intrapancreatic biliary duct excision by laparoscopic treatment is a feasible and safe option compared to open surgery.
S041 THE SHORT‐TERM OUTCOME OF REMODIFIED LAPAROSCOPIC KASAI PORTOENTEROSTOMY FOR BILIARY ATRESIA WITH 60 CASES
West China Hospital of Medicine, Sichuan University
Objectives: The aim of this study was to further improve the effects of laparoscopic Kasai portoenterostomy (LKPE) for biliary atresia (BA).
Methods: The key points of remodified of laparoscopic portoenterostomy (RLPKE) are listed as follows:
1. The hepatic duct is identified and cut off above the hepatic artery bifurcation, then the hilar fibrous cone is traced along the proximal end of the hepatic duct.
2. The hepatoduodenal ligament is not dissected, and the branches from the hepatic artery and portal vein to the hilar fibrous cone remain intact, not ligated.
3. The gallbladder is removed, but the gallbladder tube and its membrane are retained as part of the posterior wall of hepatoenteral anastomosis.
4. The level of resecting fibrous cone depends on the found of bile like juice over the fibrous stump.
5. Bleeding from the fibrous remains of portal plate is controlled by direct pressure with moist gauze without usage of any electric devices.
6. The soft tissue over the bifurcation of portal vein and hepatic artery should be preserved as much as possible.
Data of 60 patients with RLPKE from May 2005 to May 2018 were retrospectively analyzed and compared with that of 40 patients with open Kasai portoenterostomy (OKPE) during the same period, and that of 200 cases with LKPE from May 2009 to May 2012.
Results: Between May 2015 and May 2018, 60 patients (23 males, 37 females) with BA underwent RLKPE are assigned to Group B. Forty patients (17 males, 23 females) of BA received the open Kasai procedure during the same period are assigned to Group C. And 200 patients (87 males, 113 females) had LKPE during May 2009 to May 2012 are assigned to Group A. The procedure of LKPE in Group A and RLKPE in Group B were carried out by the same team, and the procedure of OKPE in Group C was performed by another team. The comparison of the operative time (P < 0.01), conversion rate (P < 0.05), postoperative hospital stay (P < 0.01), incidence of perioperative complications (P < 0.01) and cholangitis rate (P < 0.05) are significant between Group A and Group B. CJ, 1‐yr and 3‐yr SNL between Group A and Group B are not significant. The comparison of the operative time (P < 0.01), postoperative hospital stay (P < 0.01), incidence of perioperative complications (P < 0.05) are significant between Group B and Group C. CJ (P < 0.05), 1‐yr and 3‐yr SNL (P < 0.01) of Group B are much significant better than that of Group C.
Conclusions: The procedure of RLKPE is simple and feasible with less operative time and fewer complications. CJ, 1‐yr and 3‐yr SNL after RLKPE is much better than that after OKPE.
S042 EVERTING THE JEJUNAL MUCOSA ENSURES A SECURE LAPAROSCOPIC HEPATICOJEJUNOSTOMY FOR CHOLEDOCHAL CYST IN CHILDREN
Department of Pediatric Surgery, Juntendo University School of Medicine
Aim: While performing Roux‐en‐Y hepaticojejunostomy (HJ) in children with choledochal cyst (CC) laparoscopically, a secure HJ that will not leak or give rise to postoperative anastomotic stenosis may be facilitated by ensuring that both the jejunal mucosa in the Roux‐loop and the common hepatic duct mucosa are approximated and sutured. In children, the diameter at the HJ anastomosis usually ranges from around 10mm which is considered small, to less than 5mm, which is very small, irrespective of the type of CC, be it cystic, fusiform, or minimally dilated. In such cases, laparoscopic HJ (lap‐HJ) will be extremely difficult, because distinguishing between the lumen and the mucosa on the jejunal side circumferentially is tiring, tedious, and tends to be inadequate; a possible cause for the higher rates of stenosis/leakage reported in the literature for lap‐HJ compared with open HJ. We developed a technique that ensures secure HJ anastomosis by everting the mucosa of the Roux‐loop jejunum circumferentially (eversion technique; ET) to facilitate suturing and prevent complications.
a: The jejunum is incised.
b: Bleeding points are coagulated with bipolar diathermy.
c: The edge of the jejunal incision is everted.
d: The mucosa is everted circumferentially.
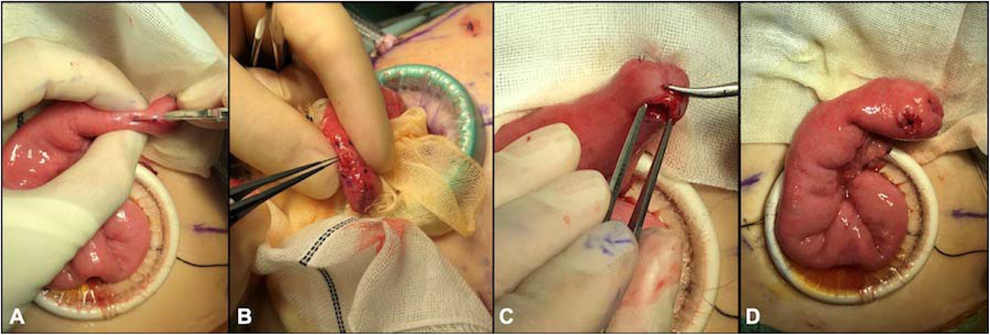
Methods: We used ET during laparoscopic HJ (lap‐HJ) in 16 consecutive children with CC performed between 2016 and 2018; mean age at surgery was 4.2 years‐old. After transumbilical, extracorporeal Roux loop‐plasty, the closed end of the jejunum is incised with a scalpel (Fig 1) and bleeding points coagulated with bipolar diathermy (Fig 1). Then, the mucosa at the incision is everted circumferentially using 7/0 absorbable sutures (Fig 1). By doing this, the mucosa of the ET jejunum is readily identifiable and can be anastomosed securely to the common hepatic duct using 5/0 or 6/0 absorbable sutures during lap‐HJ.
Results: The diameter of the anastomosis during lap‐HJ was less than 5 mm in 4 cases, 5 to 9 mm in 10 cases, and more than 9 mm in 2 cases. Even during lap‐HJ when the diameter at the anastomosis was less than 5 mm, the lumen at the incision in the Roux loop jejunum was easily visible, the mucosa in the incision of the jejunum easily identified because of ET, and the mucosa could be sutured readily, more efficiently than when ET was not used. After routine follow‐up of a mean of 1.3 years (range: 0.6–2.5 years), there have been no cases of anastomotic leakage nor anastomotic stenosis reported.
Conclusions: ET greatly facilitates secure anastomosis during lap‐HJ, even when the diameter at the anastomosis is less than 5 mm. The safety and efficiency of lap‐HJ in children for CC would be improved by this simple maneuver.
S043 THE KEY TECHNIQUE OF COMPLETE MOBILIZATION OF PORTAL VEIN IN LAPAROSCOPIC KASAI OPERATION
1Department of Pediatric Surgery, Huai'an Women and Children's Hospital, 104 Renmin Road South, Jiangsu, 223002, P. R. China, 2Department of Pediatric Surgery, Huai'an Women and Children's Hospital, Huai'an, Jianshu, 223002, P. R. China
Purpose: Mobilization of the left and right portal veins is the key technique of laparoscopic Kasai portoenterostomy (LKPE) in the treatment of type III biliary atresia (BA). The aim of this study is to discuss the technical details on complete mobilization of the left and right portal veins in laparoscopic Kasai portoenterostomy.
Methods: We have performed a new modification of the laparoscopic Kasai operation on a series of patients by thoroughly mobilizing the left and right portal veins, two rubber bands putting around the portal veins and hepatic arteries, the portal hepatis was exposed by stretching laterally the two elastic rubber bands. The fibro cord was then removed and laparoscopic portoenterostomy was accomplished easier.
Results: During the period January 2016 to Jun 2018, fifteen patients were available for review of their clinical results to evaluate our new modification. Age of the cases by LKPE was 30 ∼ 129 d, 14 of the cases were between 30 ∼ 80 d, and one case was 129 d. Time of laparoscopic procedure varied from 194 ∼ 260 min(mean 218. 5 ± 15.8 min), time of thoroughly mobilizing the left and right portal veins was 113 ∼ 132 min(mean 114 ± 12.5 min), time of Kasai portoenterostomy was 28 ∼ 42 min(mean 35 ± 4.5 min). All the cases survived the surgery without any intraoperative complications. Blood loss during operation was minimal, without necessity for blood transfusion. The case aged 129 d died of respiratory failure a week after surgery. Follow‐up after discharge was from 3–29 months (mean 16.6 months) and revealed that 12 patients (90.9%) were completely and continuously free of jaundice, without living‐related liver transplantation or reoperation, with an additional 2 patients showing a significant overall drop post‐surgery.
Conclusion: Our new laparoscopic Kasai operations of complete mobilization left and right portal veins to expose porta hepatis to freeing the biliary remnants and facilitating enteric anastomosis is effective for persistent and complete disappearance of jaundice, and decreases the need for liver transplantation or reoperation.
S044 LESSONS LEARNED AFTER MORE THAN 100 CASES OF SINGLE SITE UMBILICAL INCISION MAGNETIC ASSISTED CHOLECYSTECTOMIES IN CHILDREN: MAGNACHOLE
Fundacion Hospitalaria
Introduction: In the last 10 years we have done over 180 single site umbilical incision magnetic assisted surgeries in pediatric patients at our institution. In the cholecystectomy development, our choice has been the magnetic assisted minimally invasive one.
Objective: report the largest series ever reported and describe our gold standard technique.
Methods: Retrospective case series of consecutive pediatric patients who underwent magnetic assisted minimally invasive cholecystectomy between 2008 and 2018 at our center. 103 patients were operated (71 females) by 8 different surgeons. The mean age was 15 yo, (10 under 5 yo, 18 from 5 to 10, 52 from 10 to 15 and 22 over 15). The average body weight was 51,94 kg (r = 0,5‐123), 10 patients weighted 80 kg or more.
Technique: a 13 mm umbilical incision is done for an 11 mm 0° scope with a working channel. An internal alligator attached to a 5 mm magnet is introduced into the abdomen. At the beginning, we utilized more than 1 internal magnet but due to interaction between them in the following 98 patients we used only one magnet. 45 cm non magnetic instruments are used. We attach the alligator to the gallbladder fundus with a grasper and the internal magnet interacts with a large external magnet attached to an articulated arm. A non articulated curved grasper (Storz) is introduced through the umbilicus, 1 cm lateral to the trocar, directly through the fascia, and it is used to expose the Callot triangle. The following steps are similar to the laparoscopic approach with cauterization and clipping as necessary.
Results: The mean operative time was 120 minutes in the first 5 years, and 60 in the last 5 years. There were no complications during or after surgery. Mean length of stay was 24 hours.
Discussion: Single site transumbilical conveys many disadvantages compared to conventional laparoscopy. These include lack of maneuverability, stability, reach and torque, multiple instruments in a small surface that tend to collide, visual disorientation, umbilical ports too large for children and a new learning curve is required.
We have overcome some of these issues with the magnetic assisted transumbilical technique. The critical view achieved with the traction of the cystic duct by the magnet, allows the surgeon to emulate conventional cholecystectomy as in expected operative time, length of stay and complications.
On the other hand, this technique requires a learning curve and the availability of special materials such as a clamp attached to the intracorporeal magnet, a curved grasper and an articulated arm to hold the external magnet.
Conclusions: The fusion of magnets and single site umbilical incision magnetic assisted cholecystectomies has become a safe, ergonomic, effective technique in children that we named MAGNACHOLE and has become our gold standard.
S045 LAPAROSCOPIC TREATMENT IN SPECIAL CHOLEDOCHAL CYST
1Pediatric Surgery, 2Pediatric General Surgery Department
Objective: To investigate and analyze the treatment of Biliointestinal reconstruction in special cases during laparoscopic choledochal cyst.
Methods: The clinical data of 378 cases of congenital choledochal cyst treated by laparoscopic procedure from March 2012 to October 2018 were analyzed retrospectively. Among them, there were 76 males and 302 females, 325 cases of cyst type and 53 cases of spindle shape.
Results: 376 patients completed operation successfully under laparoscopic procedure, and 2 cases were converted to laparotomy. In 376 cases of laparoscopic choledochojejunostomy, Roux‐Y anastomosis was performed in 369 cases. The size of the anastomosis was 0.6‐2.5 cm. In the remaining 7 cases, 1 case had a common hepatic duct diameter about 3 mm due to the high position of cyst opening, and the reconstruction was performed with 6 needles of intermittence suture during choledochojejunostomy; two cases underwent cholecystoneck ligation and Roux‐Y choledochojejunostomy due to the diameter of common hepatic duct about 3 mm. The diameter of the anastomosis was about 1.0 cm; Three patients with accessory hepatic duct diameter of about 3 mm underwent accessory hepatic duct plasty and common hepatic duct jejunum Roux‐Y anastomosis; The diameter of accessory hepatic duct was about 1.5 mm in 1 cases. The accessory hepatic duct was ligated and the jejunal Roux‐Y anastomosis was performed. All 7 cases were followed up for 6 months‐28 months without complications such as biliary stricture, biliary tract infection and so on.
Conclusion: Laparoscopic choledochal cyst resection with Roux‐en‐Y hepatojejunostomy is a complicated operation. In some special cases, choledochal cyst and Biliointestinal management need rich experience, accurate judgment and appropriate treatment.
Keywords: choledochal cyst; Laparoscopy; Biliary intestinal reconstruction
S046 A MANEUVER FOR OVERCOMING THE LACK OF TACTILE SENSATION WITH DA VINCI‐ASSISTED HEPATICOJEJUNOSTOMY FOR CHOLEDOCHAL CYST IN CHILDREN
Department of Pediatric Surgery, Juntendo University School of Medicine
Aim: In children with choledochal cyst (CC), the diameter at the hepaticojejunostomy (HJ) anastomosis is normally smaller than 10mm. While the da Vinci® surgical system (dV) has been successfully used for treating CC in children, there is a lack of tactile sensation that can hinder suturing at times. We developed a maneuver to overcome this during dV‐assisted HJ (dV‐HJ).

Methods: We applied our maneuver during dV‐HJ for 6 consecutive children with CC performed during a recent one‐year period; mean age at surgery: 4.3 years (range: 1.2 to 11.2 years); mean weight at surgery: 17.3 kg (range: 9.8 to 35.6 kg). When closing the anterior wall during HJ, we place the final three 5/0 or 6/0 absorbable sutures between the incision in the Roux‐loop jejunum and the common hepatic duct but do not tie any of them (Figure 1). The anterior wall of the HJ is thus left open, and the sutures are then tied in turn. The last two sutures between the Roux‐loop jejunum and the common hepatic duct can be placed easily in the jejunum and the common hepatic duct, respectively, because both the lumens of the jejunum and common hepatic duct are left open and the surgeon can see where to place them; on the contrary, if one of the 3 sutures is tied before the remaining 2 sutures are placed, it will be extremely difficult for the surgeon to place the remaining sutures. During open surgery, the surgeon uses tactile feedback to determine the details of suturing, but this is lost during dV‐assisted surgery. Our maneuver replaces tactile feedback with visual cues to overcome this. By leaving the sutures untied until all have been placed, the surgeon can see rather than “feel” where they should be, thus allowing even the smallest of HJ anastomoses to be completed confidently.
Results: The diameters of the HJ anastomoses in this series were (cases 1 to 6: 4 mm, 13 mm, 5 mm, 13 mm, 9 mm, and 5 mm, respectively). dV‐assisted HJ was performed safely using our maneuver in all cases without difficulty. There have been no reports of anastomotic leakage or anastomotic stenosis after a mean follow‐up of 10 months (range: 7 to 15 months).
Conclusions: Our maneuver assists the surgeon by using visual cues to overcome lost tactile feedback. Thus, for dV‐HJ where there is no tactile feedback, our maneuver allows the HJ anastomosis to be completely safely and efficiently even when the anastomosis is extremely small in children with CC.
S047 LAPAROSCOPIC SPLEEN PRESERVING DISTAL PANCREATECTOMY FOR SOLID PSEUDOPAPILLARY NEOPLASM IN ADOLESCENTS
1Johns Hopkins Children's Center, 2Ann & Robert Lurie Children's Hospital of Chicago
Introduction: Solid pseudopapillary neoplasm (SPN) is the most commonly encountered pancreatic tumor in adolescents. Due to their malignant potential, the current recommendation for management is complete surgical resection; however, there is no broad consensus on the operation of choice to accomplish this. While open distal pancreatectomy with splenectomy has been the conventional approach for pancreatic tail lesions, minimally invasive and spleen preserving operations offer several advantages. Herein, we describe three consecutive laparoscopic spleen preserving distal pancreatectomies for SPN in adolescents.
Methods: Our cohort included all patients <18 years of age treated at our institution from 2015‐2018 who underwent surgical resection of an SPN. Patient data was extracted from the medical record and included demographics, clinical presentation, diagnostic evaluation, surgical treatment, postoperative course, pathology, and follow up.
Results: Three patients with an age range of 13‐16 years were identified. Two of the patients were male and one was female. The presenting symptoms were vomiting in one patient and abdominal pain in the others. The diagnostic evaluation began with cross sectional imaging that suggested SPN in all three patients, and histologic confirmation was obtained preoperatively in two patients (endoscopic ultrasound/fine needle aspiration and laparoscopic core needle biopsy, respectively). All three patients underwent laparoscopic distal pancreatectomy with preservation of the main splenic artery and vein. Mean estimated blood loss was 116cc. No patients suffered from postoperative pancreatic fistula. Median length of stay was five days. One patient who presented with preoperative acute gastric outlet obstruction had prolonged postoperative feeding intolerance requiring temporary parenteral nutrition, which lengthened his hospital stay to 10 days. Final histology revealed SPN in all three cases, with tumor size ranging from 2cm to 10cm in greatest dimension. All margins were negative for tumor. All three patients have been followed (mean 13 months) with surveillance ultrasound demonstrating a normal remnant pancreas and normal splenic perfusion.
Conclusions: Laparoscopic spleen preserving distal pancreatectomy is a safe and effective treatment for solid pseudopapillary neoplasms of the body and tail of the pancreas in adolescents. This approach achieves the margin negative resection that is appropriate for the disease without subjecting children to the risk of post‐splenectomy sepsis or the need for antibiotic prophylaxis. Furthermore, splenic preservation is associated with a reduction in perioperative morbidity when compared to conventional distal pancreatectomy with splenectomy in adults. Therefore, laparoscopic distal pancreatectomy with splenic preservation is our preferred operation in adolescents presenting with SPN.
S048 ASSESSING SURGICAL SKILLS USING DEEP CONVOLUTIONAL NEURAL NETWORKS
1Monash University, Department of Mechanical & Aerospace Engineering, 2Department of Paediatric Surgery, Urology & Surgical Simulation, Monash Children's Hospital
Purpose: Current surgical skills assessment primarily relies on a subjective assessment by a competent surgeon. These include the use of work‐based assessments, which may become time‐consuming and also potentially subjective with intra‐observer differences. An automated system that can objectively differentiate skill levels of junior surgeons is highly desirable and had not been currently established. Our study aims to develop a more accurate automated surgical skill evaluation system that may be used in a clinical surgical environment.
Methods: We utilised a motion capture system based on wearable inertial measurement unit sensors (WIMUS) and recruited 15 participants ranging from novice medical students to senior surgeons to perform core surgical skills tasks. A deep convolutional neural network was developed to analyse the hand motion data and automatically identify the skill level of the participants. Validation was achieved with correlation with JIGSAW an established robot based surgical training device.
Results: Our model achieved an average competitive accuracy of 97% for the open surgery dataset in differentiating the participants underlying surgical skill base: 3 sensor configurations of 100%, 100% and 92%. When the participant scores from their performance on the JIGSAWS machine was compared to the scores obtained with WIMUS, its correlation validated the performance of our neural network. We obtained outperformed accuracy compared to some existing datasets; 100%, 100% and 96% for Suturing, Needle‐Passing, and Knot‐tying respectively.
Conclusions: Our study demonstrate the feasibility of this method of WIMUS to automatically assess surgical skills in both open surgery and Robot‐assisted minimally invasive surgery.
Keywords: Surgical skill assessment, simulation‐based medial education, deep neural network
S049 FETOSCOPIC CLOSURE OF SPINA BIFIDA WITH A 3‐PORT TECHNIQUE
1Universidad Autónoma de Nuevo León, 2Medicina Perinatal Alta Especialidad‐Hospital Christus Muguerza
Introduction: The worldwide incidence of neural tube defects (NTD) ranges from 1.0 to 10.0 per 1000 births. The most frequent NTD is open spina bifida (OSB), which includes myelomeningocele (MMC) and myeloschisis (MS). The objective of this report is to describe a case series of OSB fetoscopic closure with a 3‐port technique.
Material and methods: in a 12‐monthperiod, 7 pregnant mothers were included in the protocol approved by the local IRB. Mean age of the mothers was 27.7 (19‐40) years; and were operated at a mean of 26.3 (25.7‐28) weeks of gestation (WG). There were 5 (71.41%) MMC and 2 MS (28.57%), 7 (100%) with Arnold Chiari, and 6 (85.7%) withventricular dilatation. Surgical technique: Using general anesthesia, the intervention was divided into 3 stages. In the first stage, midline laparotomy, exposure of the uterus, uterine ultrasound to evaluate position and fetal hemodynamic status and it was injected for sedation and relaxation (vecuronium and fentanyl). In the second stage 3 ports were placed in the uterus, amniotic fluid was drained, and CO2 insufflation was performed. Three mm instruments was carried out for OSB closure according to presentation (MMC or MS) with polyglactin 5‐0; finally, restitution of intrauterine fluid and closure of the uterine orifices. The third stage began with reintroduction of the uterus into the abdomen and laparotomy closure.
Results: In all patients, the OSB was closed up to the skin, except 1 (14.28%) MS in which only muscle closure was achieved; Durepair™ regeneration matrix was used in two patients. Surgical time for OSB closure was a mean of 133 minutes (MMC: 54, MS: 237); total surgical time was a mean of 300 minutes. The mean WG at birth was 35.3 (34‐37.4) in 4 neonates; mean weight was 2260 (2035 ‐ 2455) g, with two pregnancies in evolution. Complications: a fistula of cerebrospinal fluid requiring postnatal closure, a fetal death 2 week after surgery at 27.8 WG due to a previously unknown immune pathology of the mother, and 1 neonatal death due to necrotizing enterocolitis and septic shock. Regarding follow‐up in the integrated multidisciplinary clinic of the 3 patients so far at 1 year, 8, and 6 months, respectively, a functional injury level exits at L4‐L5, L5‐S1, and S1‐S2, respectively.
Discussion: We report the first series in Mexico of OSB closure by fetoscopic surgery. The use of 3 ports improved dissection of the OSB components and improved intracorporeal suture. These two factors reduce the surgical time associated with the learning curve of the team. Antenatal treatment of these defects must be carried out by a multidisciplinary team where each of those involved contributes with the best of their skills to achieve the best results with a pathology that usually has a poor functional prognosis.
S050 “OPTIMIZING SURGICAL TRAYS FOR LAPAROSCOPIC APPENDECTOMIES AT AN ACADEMIC CHILDREN'S
1UT Southwestern Department of Surgery, 2Dallas Children's Hospital Department of Surgery
Introduction: Approximately 20% of America's gross domestic product is spent on healthcare each year. Over 50 million operations and procedures are performed annually in the United States. Recent studies have shown that an estimated 56% of perioperative costs are materials and supplies. Cost savings can be realized in many ways, such as eliminating excess instrumentation and creating more streamlined perioperative processes. Current data suggests that during a given procedure, between 33‐87% of surgical instruments are never used. Moreover, storage, sterilization, and maintenance of surgical equipment has been estimated to cost about $0.41 per instrument. We hypothesize that the optimization of surgical trays for common surgical procedures is an opportunity to improve cost effectiveness and also surgical throughput.
Methods: Over a period of three months (April – June 2018), an observational study identifying the utilization of instruments during laparoscopic appendectomy was performed at a high volume free standing children's hospital. All instruments within the tray were identified and all instruments actually used by the surgeons registered. The trays used prior to this study were identified as Tray A. A “thinned out” tray was created based on surgical tech input (Tray B). Data on instrument use, processing time and cost were determined.
Results: Tray A contained 67 instruments and Tray B contained 78. The number of instruments used per case ranged between 7 and 15 with a mean of 9.6. There was no statistically significant variation between the surgeons with regards to number of instruments used (p = 0.41). The time of processing of Tray A is 94.7 minutes and Tray B is 81 minutes. The most widely used instrument was the Adson forcep, used in all 31 cases. The least used instruments from the survey, aside from those that were never used, included the Ligasure device (1 use) and the 5mm 0‐degree camera (2 uses).
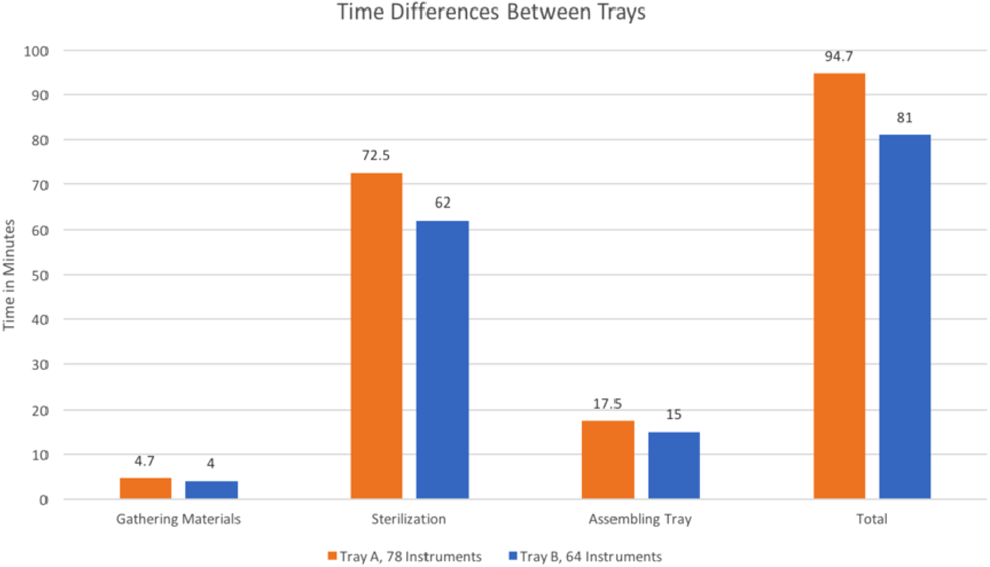
Conclusion: Studying the use patterns of faculty surgeons during common cases allows for optimization of surgical trays. The data suggests a baseline time saving of nearly 14 minutes per case between Tray A and B (Table 1). This extrapolates to over 20,000 minutes of peri‐operative time and cost savings at a high‐volume institution on an annual basis. Saving the overhead cost of the unused instruments as well as the processing time is a step in the right direction for providing cost‐effective care. Moreover, operating room efficiency increases as set‐up and sterilization times decrease. Future studies will investigate both further optimization of the appendectomy kit as well as expanding this process to other operations.
S052 IS TECHNICAL EXPERTISE NECESSARY TO ASSESS TECHNICAL EXPERTISE? LET'S ASK THE KIDS
1Christchurch Hospital, 2University of Otago
Simulation can be used to assess minimal access surgery (MAS) technical skills. Validated tools such as the Objective Structured Assessment of Technical Skills (OSATS) have been used. The rating of videoed simulated attempts by consultants can be time‐consuming and a potential barrier to simulation‐based training. This study tests the hypothesis that assessors with technical expertise are necessary to objectively score a technical task. We used experienced paediatric surgical consultants and children to test this hypothesis.
Methods: A single task was performed using a synthetic thoracoscopic simulator for oesophageal atresia and tracheo‐oesophageal fistula, specifically to cut an opening in the upper pouch of the oesophagus in an oesophageal atresia model. Each attempt was videoed and the training level of the subject was recorded. The overall global OSATS score was used to mark the attempt rated from 1 (novice) – 5 (expert). Assessors included 3 paediatric surgeons and 3 children aged 9‐13 years. They were blinded to the seniority and identity of the subject. The children were shown a demonstration video of an expert completing the task as a baseline prior to marking the videoed attempts. None of the children had had previous surgical training!
Results: There were 27 subjects, 5 consultant surgeons (2 paediatric surgeons, 3 upper gastrointestinal adult surgeons with MAS skills), 5 surgical registrars and 17 house surgeons and trainee interns with no MAS training who were videoed performing the task. The task took a median of 48 seconds (range 12 – 143). There was a strong positive correlation (0.8714 p < 0.0001) between the average of the children's and consultants' scores. When adjusted for the covariates, seniority of subjects and operating time, there was still a strong positive correlation (0.7071, p < 0.0001). A Shapiro‐Wilk normality test indicated a normal distribution of both ratings. A paired t‐test identified the mean (SD) of the differences between children's average ratings and consultants' average ratings to be −0.25 (0.52) (p = 0.0201) identifying a poor agreement. Consultants tended to give higher scores than the children. The intraclass correlation coefficient for consultants and children was 0.304 and 0.476 respectively, both indicating a poor inter‐rater reliability.

Conclusions: Unskilled assessors, without specific expertise in the technical skill being evaluated, appear to be as reliable as assessors skilled in the technique being observed. This may have implications for who can be chosen to judge technical expertise. The variability between assessors (inter‐observer reliability) means that multiple assessors should be used to increase the reliability for high stakes assessments of competence: this too has implications for summative assessments using simulation if a high level of reliability is desirable.
S053 THE CONTINUOUS SKILL TRAINING USING THE DISEASE SPECIFIC ENDOSCOPIC SURGICAL SIMULATOR PROMOTE YOUNG PEDIATRIC SURGEONS: LEARNING CURVE FOR TRAINEES
1Department of Pediatric Surgery, Graduate School of Medical Sciences, Kyushu University, 2Department of Pediatric Surgery, Reproductive and Developmental Medicine, Faculty of Medical Sciences, Kyushu University, 3Department of Pediatric Surgery, Faculty of Medicine, University of Tsukuba
Background and aims: Pediatric surgeons are required to learn highly advanced skills in endoscopic surgery because of a wide variety of operative procedures, however the experience of young pediatric surgeons is limited. Therefore, we developed the laparoscopic fundoplication simulator with an objective endoscopic surgical skill evaluation system. The present study was performed to evaluate the effectiveness of continuous training with the disease‐specific endoscopic surgical simulator for young pediatric surgeons.
Methods: Nine pediatric surgeons who had performed fewer than five laparoscopic fundoplication procedures participated as trainees in this study. The participants watched expert videos upon starting training and trained with the laparoscopic fundoplication simulator for 1 hour every 10 days. At the start of each training session, we used the surgical skill evaluation system to assess the participants' surgical techniques with five factors: 1) the task time, 2) the right and left balance of suturing in three ligatures, 3) the suturing interval between the three ligatures, 4) the total path length of the forceps, and 5) the velocities of both forceps. The path length and the velocity of the forceps were measured using the AURORA system. We examined the learning effect of each training and compared with the expert's results. The expert pediatric surgeon group comprised 10 pediatric surgeons who were either certified by the ESSQS or had an equivalent skill level. Statistical analysis was performed and p < 0.05 was considered statistically significant.
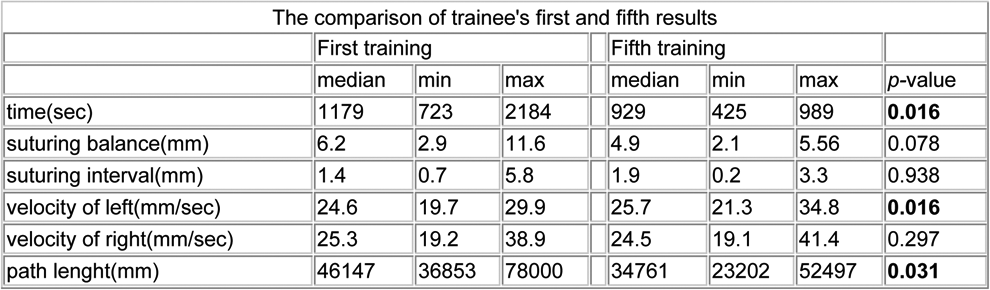

Results: Seven of the nine participants were able to continue the prescribed training. Comparison of the trainees' first and fifth results showed that the total task time was significantly shorter in the early stage of training (p = 0.016). There was no significant change in the velocity of the right forceps (p = 0.297), however, the velocity of the left forceps significantly increased (p = 0.016). The total path length of both forceps was significantly shortened (p < 0.05). The right and left balance and the interval between the three ligatures tended to improve (figure 3 and 4).
Conclusion: Our study showed that significant training effects can be confirmed from the early stage.
S054 A RETROSPECTIVE REVIEW OF REOPERATION AFTER LAPAROSCOPIC INGUINAL HERNIA REPAIR IN CHILDREN
Saitama Children's Medical Center
Background: Inguinal hernia repair is one of the most common procedures in pediatric surgery, and laparoscopic repair is increasingly widely accepted. However, the risks of recurrence remain unknown. The present study summarized our single‐center experience with recurrences after laparoscopic inguinal hernia repair in children.
Methods: Laparoscopic percutaneous extraperitoneal closure (LPEC) and single‐incision LPEC (SILPEC) were introduced in our hospital in 2007 and 2009, respectively. We retrospectively reviewed the cases between 2000 and 2018 and searched for cases in which hernia repair was performed ≥2 times as reoperation cases. We evaluated the medical records and surgical videos of those cases wherein the first hernia repair was performed laparoscopically.
Results: During the study period, 2112 patients (44.6%) underwent LPEC or SILPEC in our hospital. Twenty‐two cases (1.0%) were judged as reoperation cases: 14 (recurrence ratio = 0.7%) had recurrences after treatment for preoperative symptomatic side and 8 (incidence ratio = 0.4%) had contralateral metachronous inguinal hernia (CMIH), which was not treated during the first hernia repair. After treatment, recurrence for contralateral patent processus vaginalis (cPPV) was not found. The male/female ratio was 15/7 (68.2%/31.8%), the median age during the first repair was 24.5 (2–143) months, and the median period from the first repair to recurrence was 12.5 (1–72) months. Of the 14 recurrence cases, 13 (92.9%) were of inguinal hernias and 1 (7.1%) showed hydrocele as first symptoms. The median period from the first repair to recurrence was 6.5 (1–19) months. With regard to the etiology of the recurrence, loosened ligation and torn peritoneum were found in 6 cases and 1 case at the first repair, respectively (Fig. 1). With regard to CMIH, at least four cases were suspected of having insufficient checks of cPPV.

Conclusion: We summarized our experience with recurrences after laparoscopic inguinal hernia repair in children. Loosened ligation, torn peritoneum, or insufficient checks of cPPV were found in some cases.
S055 ENDOSCOPIC NAVIGATION SURGERY WITH INDOCYANINE GREEN FLUORESCENCE IN PEDIATRIC PATIENTS
Nagoya University Graduate School of Medicine
Introduction: Navigation with indocyanine green (ICG) fluorescence has been recently applied in pediatric endoscopic surgery. However, the uniqueness of each pediatric surgery due to variations in body size (body weight ranging from 500 g to 50 kg) and pediatric‐specific techniques (e.g., portoenterostomy for biliary atresia) [A1] makes it difficult to standardize the protocol for endoscopic surgery with ICG fluorescence. We have been applying ICG fluorescence in pediatric endoscopic surgery for the treatment of various diseases, and we report here our newly standardized protocol as well as outcomes.
Subjects and Methods: We obtained approval for this study from our institutional ethics board and consent from patients or their parents. The study subjects were patients under the age of 15 years who underwent endoscopic surgery with navigation using ICG fluorescence at our hospital from January 2015 through August 2018. Patients without consent and those with allergy to iodine were excluded from this study. To visualize the biliary tract, intestinal blood flow, lymphatic vessels, or tumor, ICG was administered intravenously or subcutaneously at a dose of 0.01–0.1 mg/kg depending on the target site. ICG was also used to visualize defective anastomotic sites during hepaticojejunostomy or leakage sites in the thoracic cavity of patients undergoing peritoneal dialysis. Endoscopic surgery was performed using an ICG/near‐infrared[A2] (NIR) imaging system under observation with NIR fluorescence laparoscopy. We evaluated the applied dose of ICG, timing of ICG administration, ICG visualization status, and ICG‐related complications.
Results: We performed endoscopic surgery with navigation using ICG fluorescence in 89 patients. No event of complications occurred. The distribution of cases was as follows: 29congenital choledochal cyst, 19 biliary atresia,10 metastatic lung tumor, 11 esophageal atresia, 5 chylothorax, 2 cholelithiasis, 5 cholestasis, 3 hepatoblastoma, 3 anorectal malformation, 1 Hirschsprung's disease,1 plueroperitoneal communication, and 1 varicocele.
ICG fluorescence enabled confirming critical events and sites during surgery, including bile leakage in hepaticojejunostomy involving the the common bile duct, the thoracic duct in lymphangiography, chylous leakage, blood flow in the anastomotic site in anorectal malformation and Hirschsprung's disease, lesion in pleuroperitoneal communication, and vasculature (lymphatic, arterial, and venous) in varicocele surgery. A 10‐mm laparoscope had initially been used; however, a 5‐mm laparoscope has been used since April 2016. The 5‐mm laparoscope provided sufficient visualization.
The use of ICG fluorescence in 40 metastases in 10 cases with metastatic lung tumor resulted in 2 false‐positive masses, and the fluorescence observations were not consistent across biliary atresia cases.
Conclusion: Our results encouragethe application of endoscopic navigation surgery with ICG fluorescence in various pediatric diseases. The ideal dose and timing of ICG administration should be further investigated for each disease.
S056 DEVELOPMENT OF AN INFANTILE THORACOSCOPIC LOBECTOMY MODEL THAT IS TAILORED TO EACH PATIENT'S SPECIFIC ANATOMY FOR PREOPERATIVE SIMULATION
1Graduate School of Medicine and Faculty of Medicine, The University of Tokyo, 2Department of Pediatric Surgery, Saitama Children's Medical Center, 3Department of Pediatric Surgery, Gunma Children's Medical Center
Background: In congenital pulmonary airway malformation (CPAM), the pulmonary lobar arteries, veins and bronchi are sometimes greatly displaced because of a large cystic lesion. Therefore, during infantile thoracoscopic lobectomy for the treatment of CPAM, highly advanced surgical skills are required and the risk of operative complications is high. Operative navigation techniques based on the patient's imaging data such as computed tomography (CT) and a three‐dimensional (3‐D) lung model constructed using a 3‐D printer were recently developed. However, it is difficult to preoperatively image the operative complications that the surgeon may face. We aimed to develop a 3‐D lung model that replicates the patient's specific anatomy in which the textures of the organs in the model resemble those in patients, and that would be useful for practicing endoscopic surgical procedures preoperatively.
Methods: Stereolithography data of a patient's lung consisting of a pulmonary lobe, bronchi, pulmonary arteries and veins, were extracted from CT data of a one‐year‐old CPAM patient. A 3‐D lung model was created with super‐soft resin using the vacuum injection method (Fig.a). This material is so soft that surgeons can perform endoscopic surgical manipulations on this model. This lung model was placed in a rapid‐prototyped pediatric chest model that had been developed using CT data of a one‐year‐old infant. The size and texture of each artificial organ such as the bronchus, artery and vein were evaluated by five pediatric surgeons certified by the pediatric Endoscopic Surgical Skill Qualification (ESSQ) system developed by the Japan Society for Endoscopic Surgery. Two examinees performed thoracoscopic lobectomy on this model; one examinee performed lobectomy on this model before the operation in the patient and the other performed the simulation after the operation. The examinee who performed surgical procedures on the simulator was the same as the main operator who performed thoracoscopic lobectomy in the patient. The simulations on this model were video‐recorded (Fig.b) and compared with the video recording of thoracoscopic lobectomy in the patient (Fig.c). A questionnaire was conducted in which the examinees were asked to rate the simulator.
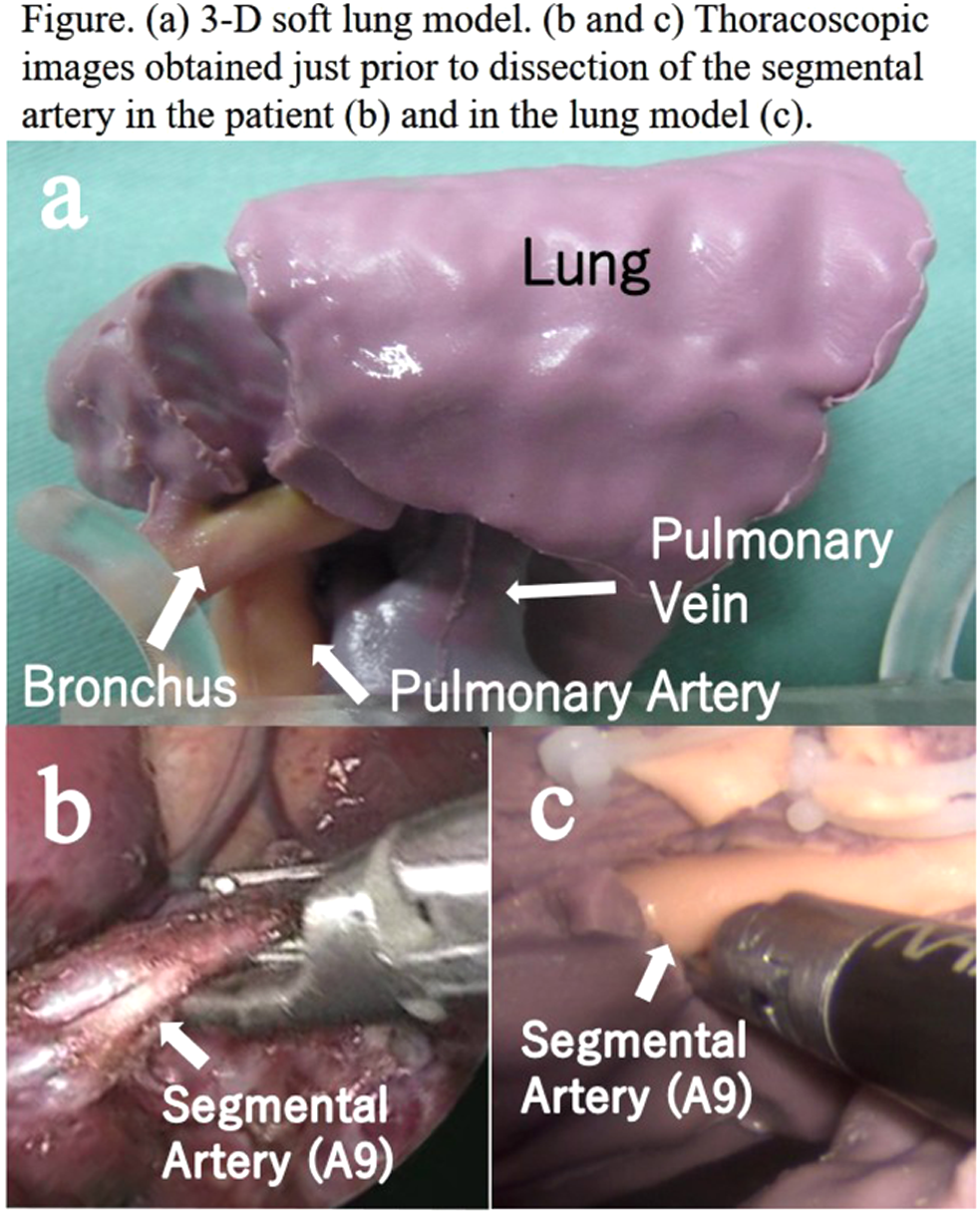
Results: In the lung model, after dissecting the interlobar fissure, some branches of the bronchi, pulmonary arteries and pulmonary veins were exposed, and the surgeon performed ligation, clipping, and cutting. When comparing the recorded videos, the anatomical details of these artificial organs were almost the same as those of the organs seen during thoracoscopic lobectomy in the patient. The questionnaire results showed that our 3‐D lung simulator well replicated the clinical situation, and the usefulness of the model for preoperative simulation was rated as high. However, examinees rated that the materials used to make each organ need improvement.
Conclusion: Our 3‐D lung model is made according to each patient's specific anatomy, and endoscopic surgical manipulations can be performed on the model. When examinees perform the simulation according to the operative procedures, all staff can share images of the simulated thoracoscopic lobectomy on every patient. This model will be useful for education of residents and fellows. Future work will be to add a troubleshooting function.
S057 ANALYSIS OF FORCES IN LAPAROSCOPY: THE DECONSTRUCTION OF AN INTRACORPOREAL SUTURING TASK
University of Toronto
Background: An intracorporeal suturing task simulator has been developed that can measure forces in real time during the performance of the task. These forces have been described and have been shown to be greater in larger size simulators. We analyze the forces on deconstructed task segments to allow for targeted assessment and teaching.
Methods: Participants, majority of whom were recruited at a previous IPEG meeting, performed a defined intracorporal suturing task on a pediatric (PLS) simulator. Expertise level was assigned based on number of laparoscopic cases. Real‐time force and torque data were collected in 3 degrees of freedom using a custom‐designed force sensing platform. The task was deconstructed into four segments: loading needle/pull‐through, double‐throw knot, first single‐throw knot, and second single‐throw knot. Force analysis parameters (FAPs) were calculated for each of the segments. FAPs included maximum, mean, and number of extreme force events. Outcomes were analyzed using one‐way ANOVAs and paired sample t‐tests (p < 0.05).
Results: One‐hundred two participants were recorded (20 experts, 52 intermediates, 30 novices). The largest differences were seen in the “double‐throw knot segment”. In this segment, significant differences were identified between expert and novices in mean forces exerted in the “side‐to‐side” direction. Experts exerted a mean force to the right whereas novices exerted a mean force to the left. Congruently, differences were also seen in this segment between novices, intermediates, and experts in the torque applied in the “side‐to‐side axis”. Experts applied significantly more torque towards the right than novices and intermediates. Similar differences were not found in other segments. In the “first single throw segment”, the novices had a significantly larger number of extreme force events in the “up‐and‐down” direction. Analyzing maximum forces did not demonstrate any significant differences between the groups in any segment.
Conclusions: We demonstrate an ability to detect real‐time assessment of forces during the performance of an intracorporeal suturing task. Deconstruction of the task into segments allows us to gain insight into the specific forces applied which distinguish expertise level. Further studies on forces applied during specific laparoscopic maneuvers may reveal greater insights that distinguish experts and allow for teaching in a more focused and effective manner.
Quickshot Abstracts
QS001 LAPAROSCOPIC TREATMENT FOR BLADDER GIANTS STONES AFTER ENTEROCYSTOPLASTY IN CHILDREN
Department of Pediatric Surgery. Urology and Laparoscopic Surgery Child. Municipal Children's Hospital. Hospital Pediátrico del Niño Jesús Chair of Pediatric Surgery. Universidad Nacional de Córdoba. Córdoba. Argentina.
Objective: Bladder stones are one of the most frequent complications in the long term in patients with previous surgery of enlarged bladder and neck plastic. Its high lithogenic index is due to chronic bacteriuria, a major waste discharge and post production of mucus. The incidence of calculi in augmented bladders with intestinal patch has a range of 10 to 50% (regardless of whether small or large bowel), whose composition is almost exclusively of struvite and calcium phosphate.
Material and methods: In the period between March 2007 and January 2017 were included in the study eight patients (five female and three male) with previous bladder surgery, enterocystoplasty and bladder neck plastic (7 patients had stoma Mitrofanoff continent). Seven with neurogenic bladder conditioned by myelomeningocele, and one with previous cystectomy with Kock pouch and continent stoma for bladder exstrophy. All patients had radiographic and sonographic diagnosis of multiple giant bladder stone, two of them also with stones in the ureter and pelvis. Two patients had previous surgery for stone extraction by open surgery with recurrence of stones.
Were included, patients without the possibility of alternative treatment, except for stone removal by open surgery.
Results: We performed in all cases, a laparoscopic approach transperitoneal with three working channels, with good immediate postoperative result. There were no intraoperative complications. Mean operative time was 74 min (r: 50‐100). Bladder catheter was left for a period of seven days, and a suction drain the surgical site for 24 hours. The hospitalization time was 48 hours in all patients with early feeding (at 6 hours). None presented urinary leakage from the suture site relevant or digestive symptoms. The need for analgesics was minimal, and all were discharged from the hospital indicated antibiotic prophylaxis and anticholinergic medication. Monitoring bladder ultrasonography was performed with no recurrences so far.
Conclusions: The principle of management of bladder stones in patients with previous surgery of it, involves the use of less invasive technique that allows the removal of calculus in one piece to avoid recurrence while avoiding injury of the urinary tract or adjacent structures. So far have been described as technically feasible endoscopically (in patients without previous neck surgery), percutaneous suprapubic and conventional open surgery, with risks already described for each of these procedures. It is proposed in this initial experience, a transperitoneal laparoscopic approach with minimal bladder opening for extracting multiple urinary calculi in patients with neurogenic bladder, previous surgery of enlarged bladder and neck plastic, without therapeutic alternatives than open surgery. Initial results show this technique as safe and effective with minimal morbidity and short hospital stay, without intraoperative or postoperative complications, which allows the extraction of multiple stones and large size without fragmenting.
QS002 ESOPHAGOJEJUNAL ANASTOMOSIS BY CIRCULAR STAPLER IN PEDIATRIC PATIENTS: SIZE MINIMA DEFINED BY EXPERIENCE AND GEOMETRY
1Phoenix Children's Hospital, 2Children's Hospital of Milwaukee
Background: Esophagojejunostomy is facilitated by use of a circular stapler, particularly when performed laparoscopically. The minimum patient size which will allow use of circular staplers in the small intestine is unknown.
Methods: Retrospective review of esophagogastric dissociations performed at a single tertiary care institution over a 4 year interval.
Results: From the seven cases identified, patients weighing >16 kg easily accommodated the 21mm stapler. There was a narrow fit in the patient weighing 13.6 kg, and the 6 kg patient was too small for the circular stapler.
Conclusions: Through a combination of clinical observation and physical reasoning, circular stapler applicability in small intestine is predicted by patient weight or intestinal measurement. Patients weighing greater than 16 kg will accept the stapler whereas patients less than 13 kg are likely too small. Alternately, on the basis of a geometric derivation, if the width of the flattened intestine is greater than 1.6 times the device diameter, the device will fit.
QS003 THE USE OF CRYOANALGESIA IN THE NUSS PROCEDURE – LESSONS LEARNED
Phoenix Children's Hospital
Introduction: Minimally invasive repair for pectus excavatum has evolved over the years since it was first described by Nuss et al. in 1998. Even with an evolving technique, pain control remains a challenge and patients often require significant amount of perioperative opioids. Therapeutic options to manage this pain have included epidural analgesia, multimodal anesthesia, intercostal nerve blocks, elastomeric pain pumps, and more recently, cryoanalgesia. Cryoanalgesia, previously described in thoracotomies in the 1980s, has recently been applied to the Nuss procedure and has the reported benefit of prolonged postoperative chest wall anesthesia that may result in shorter hospital length of stay and quicker recovery. However, there is scant reported data on the complications associated with the use of cryoanalgesia in the Nuss procedure. One potential complication of this therapy includes thermal injury to surrounding tissue. When our institution initially incorporated cryoanalgesia in our multimodality pain management for our patients undergoing minimally invasive pectus repair, we encountered a higher rate of pneumothorax. This drove us to investigate the impact and safety of the use of cryoanalgesia in the Nuss procedure.
Methods: We performed a single institution retrospective review of pediatric patients undergoing the Nuss procedure with and without cryoanalgesia from June 2017 to July 2018. Multimodal anesthesia was used in every patient, and most patients additionally received either cryoanalgesia or elastomeric pain pump therapy. Clinical and demographic data were collected. Primary outcome was actionable pneumothorax. For the purpose of the study, actionable pneumothorax was defined as those that required additional intervention such as a thoracostomy tube placement. Secondary outcomes included hospital length of stay, operative times, pain scores at discharge and re‐intervention.
Results: A total of 101 patients underwent minimally invasive repair of pectus excavatum; 45 had cryoanalgesia and 56 had other modalities of intraoperative pain control. Mean Haller Index (HI) was 5.04 for the non‐cryoanalgesia group and 5.07 for the cryoanalgesia group. In the cryoanalgesia group, we encountered actionable pneumothorax in four cases versus one case in the non‐cryoanalgesia group (p = 0.139). Delayed pneumothorax (>24 hours after surgery) was slightly higher in the cryoanalgesia group (48% vs 16%). Length of stay was comparable (median of 3 days versus 4 days). Pain scores at discharge were similar in both groups (mean visual analogue scale score 2 vs 2.65). Operating time was similar in‐between two groups (mean time 1:59 vs 2:06). Mean follow up was 7 weeks for the cryoanalgesia group and 22 weeks in the non‐cryoanalgesia group. No re‐interventions were required.
Conclusion: Cryoanalgesia seems to be a feasible and effective technique for pain control after minimally invasive pectus repair. In our experience, slightly increased rate of pneumothorax was encountered during the initial adoption of cryoanalgesia therapy. This prompted us to develop techniques to decrease the risk of thermal injury to the lung during cryotherapy and to develop an algorithm to address potentially actionable pneumothorax. Larger and prospective studies are needed to assess the long term impact and complications of cryoanalgesia applied to the Nuss procedure.
Keywords: Nuss procedure, Minimally Invasive Pectus Excavatum Repair, Cryoanalgesia, Postoperative Analgesia.
Level of Evidence: Level III, Retrospective
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not‐for‐profit sectors.
Abbreviations: Haller Index (HI)
QS004 THE EVALUATION OF EFFECT OF THE TREATMENT FOR INTRA‐ABDOMINAL CRYPTORCHIDISM OF CHILDREN WITH TRANSUMBILICAL SINGLE‐SITE LAPAROSCOPIC SINGLE STAGE FOWLER‐STEPHENS ORCHIOPEXY
Children's Hospital of the Capital Institute of Pediatrics
Objective: To evaluate the clinical effect of the treatment for intra‐abdominal cryptorchidism of children with transumbilical single‐site laparoscopic single stage Fowler‐Stephens orchiopexy (FS0).
Methods: Retrospectively reviewed the case records of the intra‐abdominal cryptorchidism of children who had undergone transumbilical single‐site laparoscopic single stage FSO between January 2011 and January 2017, set for observation group (OG), whoes age was from 1 to 8 years and average age was 1.5 years, with 22 unilateral and 8 bilateral, 38 testis in total. 31 children of intra‐abdominal cryptorchidism who had undergone laparoscopic two stage FSO were set for control group (CG), whose age was from 11 months to 9 years and median 20 months, with 23 unilateral and 8 bilateral,39 testis in total. Postoperative follow up was conducted with the evaluation index included the testical position and whether or not atrophy. To observe the procedure effect and postoperative complication, evaluate the difference between two operation methods.
Results: All operations were successful in both groups without intraoperative Complication. 38 testis of OG were operated with single stage FSO, 39 testis of CG were operated with two stage FSO. Postoperative complications included scrotum wound infection 1 case and scrotum hematoma 1 case among OG, abdominal wall emphysema 1 case, intestinal obstruction 1 case and umbilicus infection 1 case among CG. Follow up ranged from 6 months to 6 years, median 24 months. All of testical were in the scrotum, each group had one case of testical atrophy. The difference of postoperative complication and effect between two groups had no statistical significance (P > 0.05).
Conclusions: Outcomes between single stage and two stage FSO are similar. The transumbilical single‐site laparoscopic FSO not only has the satisfactory effect, but also make some patients avoid the reoperation and secondary anaesthesia, but the indications and contraindications of this procedure should be brought to attention.
QS005 OUTCOME FOR GUBERNACULUM SPARING LAPAROSCOPIC ASSISTED ORCHIDOPEXY FOR BILATERAL INTRA‐ABDOMINAL TESTICLES
King Faisal Specialist Hospital and Research Centre, Jeddah
Background: Controversy still exists over the optimal laparoscopic technique to mobilise intra‐abdominal testes. The gubernaculum sparing, laparoscopic assisted, staged Fowler Stephens (FS) approach, has been shown to be highly effective in restoring testicles into the scrotum. Crucial to the success of this procedure is the preservation of an adequate arterial supply to the testes.
Aim: To assess the outcome of the above technique for bilateral intra‐abdominal testes.
Method: Over a 12 year period (2005‐17), 30 cases of impalpable testes subjected to laparoscopy under a single surgeons care were prospectively recoded on an Excel spreadsheet. Five cases with bilateral intra‐abdominal testicles were the focus of this study. Demographic details, operative findings, details of intervention and outcome were recorded. Follow up was for a period of at least 2 years.
Technique: A 3 stage procedure was undertaken; a first stage laparoscopic FS on the right followed 6 months later by 2nd stage laparoscopic assisted FS on the right and a 1st stage FS on the left. Finally, 6 months later, following confirmation of an adequate result on the right, the left side was subjected to a 2nd stage, laparoscopic assisted FS.
The 2nd stage, laparoscopic assisted FS involved internal mobilisation of the testicle on the pedicle of the vas deferens, exposure of the inguinal canal via groin incision, traction on the gubernaculum to draw the mobilised intra‐abdominal testes into the canal and finally its fixation in a Dartos pouch. Paramount to outcome is preservation of the gubernacular vessels in situ.
Results: Five cases of mean age 4.3 years (range 1.1‐10) underwent bilateral orchidopexy. Two cases had significant underlying comorbidities and were late referrals. All interventions were day procedures and there were no complications. At 2 year follow up all patients had a successful outcome with palpable testicles evident in the scrotum bilaterally.
Conclusion: This study confirms the effectiveness of a staged gubernaculum sparing, laparoscopic assisted FS procedure for bilateral intra‐abdominal testicles. The results match those of unilateral intra‐abdominal testicles subjected to the same procedure. Preservation of collaterals in a gubernaculum‐sparing approach may explain the excellent results seen in this and prior series.
QS006 THE EXPERIENCES OF PREOPERATIVE SIMULATION USING COMPREHENSIVE PEDIATRIC PNEUMOPERITONEUM SIMULATOR
1Tsuchiura Kyodo General Hospital, University of Tsukuba Hospital, 2Tsuchiura Kyodo General Hospital, 3University of Tsukuba Hospital
Purpose: Pediatric surgeons must have dexterous manipulation of surgical instruments in order to handle fragile tissues in a small workspace, the size of which varies according to the age of the child. Despite the need for advanced surgical skills in order to avoid complications, opportunities for pediatric surgeons to simulate the appropriate port location are limited. We developed and already reported a laparoscopic pneumoperitoneum simulator for pediatric surgeons with a surgical skill validation system. We newly developed a renal pelvis and ureter and have used this simulator for the preoperative simulation of advanced surgery for pyeloplasty and total nephroureterectomy. We herein report the experiences of preoperative simulation using our pediatric pneumoperitoneum simulator.
Methods: We developed a pyeloplasty model, consisting of a kidney, dilated renal pelvis and ureter. The renal pelvis and ureter were made of styrene materials (C6H5CH = CH2), and the physical proportions of the organs were derived from three‐dimensional imaging of a computed tomography scan of a patient. These artificial organs were placed in the pneumoperitoneum simulator, which has already been reported as a comprehensive pediatric simulator. We performed preoperative simulation using this new simulator as follows: Case 1, a 15‐year‐old patient diagnosed with intermittent hydronephrosis with crossing vessels underwent laparoscopic pyeloplasty; Case 2, a 6‐year‐old patient diagnosed with hypoplastic kidney induced by multicystic dysplastic kidney with an ectopic urethral opening underwent laparoscopic total nephroureterectomy. Each procedure was performed laparoscopically, and there were no intra‐ or postoperative complications.
Results and Discussions: We could performed and smoothly introduced these urogenital advanced surgery. We have already reported that the most appropriate approach, especially the port location, differs among attending surgeons. On examining individual experiences, it is apparent that problems are most likely to occur during the first five procedures performed by a surgeon. As such, preoperative simulation is essential for preparation in order to ensure the best possible operative outcome and avoid complications. With this approach, we were able to determine whether or not a port location was suitable for laparoscopic advanced surgery. this may help reduce the risk of complications and stress on trainees, even those who are new to a given procedure.
Conclusion: We newly developed a pyeloplasty model, including a kidney, dilated renal pelvis and ureter, for preoperative simulation. Preoperative port simulation in advanced surgery using our artificial simulator is feasible and may help improve the outcome of minimally invasive surgery in children.
QS007 MINIMALLY INVASIVE TECHNIQUE IN THE SURGICAL TREATMENT OF DIGESTIVE TRACT DUPLICATIONS IN CHILDREN.
1Clinic “OBERIG”, 2Bogomolets National Medical University
Aim: to evaluate the safety, applicability and benefits of laparoscopic and thoracoscopic approach for treatment of digestive tract duplications in children.
Materials and methods: starting on 2011 and continuing through inclusive 2018 there were 15 patients with digestive tract duplications that underwent surgery with the use of MIS technique. The average age of the children was 6 years 4 months. 8 (53.3%) patients didn't have any significant clinical signs and the digestive tube duplication was an incidental finding while annual well‐care visits with ultrasound scan. 5 (33.3%) children sought medical attention for abdominal pain, and 2 (13.3%) of them had intestinal obstruction. Assessment of the surgical patients included: blood test, Doppler ultrasonography, X‐ray contrast study of the digestive tract with barium, CT or MR scan. 5 (33.3%) children presented with esophageal duplication, 4 (26.6%) with gastric duplication, two (13.3%) with duplication of ileocecal region, and 1 (6.6%) with duplication of terminal ileum. In all cases cystic duplications were in evidence. For surgical procedure 5 mm camera in transumbilical position and 3/5 mm working ports at the flanks were used.
Results: Thoracoscopic excision was performed in two cases of esophageal duplication in middle third. In three cases of abdominal part of esophagus duplication laparoscopic excision with Nissen fundoplication (either Dor fundoplication in one case) was performed.
Laparoscopic excision was performed in four cases of gastric duplication with intracorporeal closure of a stomach incisional wound.
In 4 cases laparoscopy was performed with anastomosis carried out extracorporeal through the transumbilical approach. Duplication enucleation was performed in 2 cases without enterotomy with following serous‐muscular lining suture.
There were no intraoperative complications. The NG tube was removed within 12 hours after procedure in all children and with following liquid intake and enteral nutrition feeding in 24 hours post‐op. On the 5th day after procedure all the patients were discharged. None of the children required narcotic analgesics and administered NSAIDS in a short‐term of two days.
Conclusion: We consider MIS technique to be safe and effective for the treatment of digestive tract duplications in children. It gives the best visualization of the whole digestive tube, reduces the postoperative pain syndrome and ensures fast recovery.
QS008 LAPAROSCOPIC SUTURE RECTOPEXY FOR RECURRENT RECTAL PROLAPSE IN CHILDREN
Section of Pediatric Surgery, Faculty of Medicine, Tanta University, Egypt
Introduction: Laparoscopic rectopexy for recurrent rectal prolapse became more widely used nowadays. Strict indications are needed to get the proper outcomes. The advantages rely on the careful dissection of peritoneal sac and fixation of rectum. One of the theories of recurrent rectal prolapse is the hernia like in front of rectum.
Aim: The aim of this presentation is to present our experience of laparoscopic suture rectopexy (LSR) in indicated cases of recurrent rectal prolapse in children.
Patients and Methods: Fourteen patients were included with recurrent rectal prolapse where all were subjected to LSR procedure after exclusion of other probable causes. Dissection of peritoneal sac anterior to the rectum was carried out followed by closure of deep pouch by non‐absorbable sutures then fixation of the right side of rectum and sigmoid to the lateral wall of areolar tissue. Fixation to sacral promontory is done by Ethibond or Prolene sutures when redundancy is obvious.
Results: We have 10 girls and 4 boys with age ranged between 3 and 10 years in the last 4 years. Nine cases were treated earlier with injection therapy and 5 following Thiersh procedure after failure of conservative treatment for 6 months. Operative time ranged between 40 and 80 minutes. Follow up period ranged between 6 and 36 months with mean of 15 months. Post‐operative mucosal prolapse reported in one case 6 months post surgery.
Conclusions: LSR is efficient technique in well selected cases of recurrent rectal prolapse and could reverse this underlying pathology. Longer follow up and evidence are needed to standardize the technique.
QS009 ENDOSCOPIC REPAIR AS PRIMARY TREATMENT FOR H‐TYPE TRACHEOESOPHAGEAL FISTULA
University of Wisconsin School of Medicine and Public Health
Tracheoesophageal fistula (TEF) without atresia, also known as isolated or H‐type TEF, is an uncommon congenital esophageal malformation representing approximately 4% of all TEFs1. Diagnosis may be delayed as presentation can be indolent, often after workup for recurrent episodes of aspiration pneumonia or choking during feeding. Management of H‐type TEF has typically been surgical repair via cervical incision. However, this technique is associated with significant morbidity such as high rate of recurrent laryngeal nerve injury2. Others have attempted repair via thoracoscopy, although most H‐type TEFs are not amendable to thoracoscopic repair due to its high location in the neck3. There have been reports of successful endoscopic intervention for both recurrent and primary H‐type TEFs4. Most reports described endoscopic de‐epithelialization of the fistula tract followed by injection of a sealant such as fibrin glue5. Here, we reported two patients (18 months old and 13 days old) who were diagnosed with H‐type TEF and underwent successful repair using endoscopic technique with injection of injectable gel. The first patient was found to have an isolated H‐type TEF at 17 months of age after having persistent cough with liquid intake. The fistula was confirmed on rigid bronchoscopy with a large fistula and short track which was de‐epithelialized using a Bugbee cautery. Hyaluronic acid gel was injected around the fistula to oppose the track's surface. He had significant improvement of symptoms (with exception of mild cough with liquids) but still had a small fistula on esophagram. After the second endoscopic procedure, he remained asymptomatic after 22 months. The second patient was found to have an H‐type TEF during rigid bronchoscopy workup for right lung aplasia. Her fistula track was short and narrow. She underwent endoscopic repair using Bugbee cauterization of the track and injection of a long‐lasting injectable gel around the fistula. She had no evidence of recurrence at 16 months of age. Neither patient experienced any complications. The mechanism of closing H‐type fistula in these two patients is thought to be due de‐epithelization of fistula track followed by opposing the track wall concentrically. Large fistulas with short track might require more than one treatment. These outcomes suggest that endoscopic closure should be considered as primary treatment for H‐type fistula.
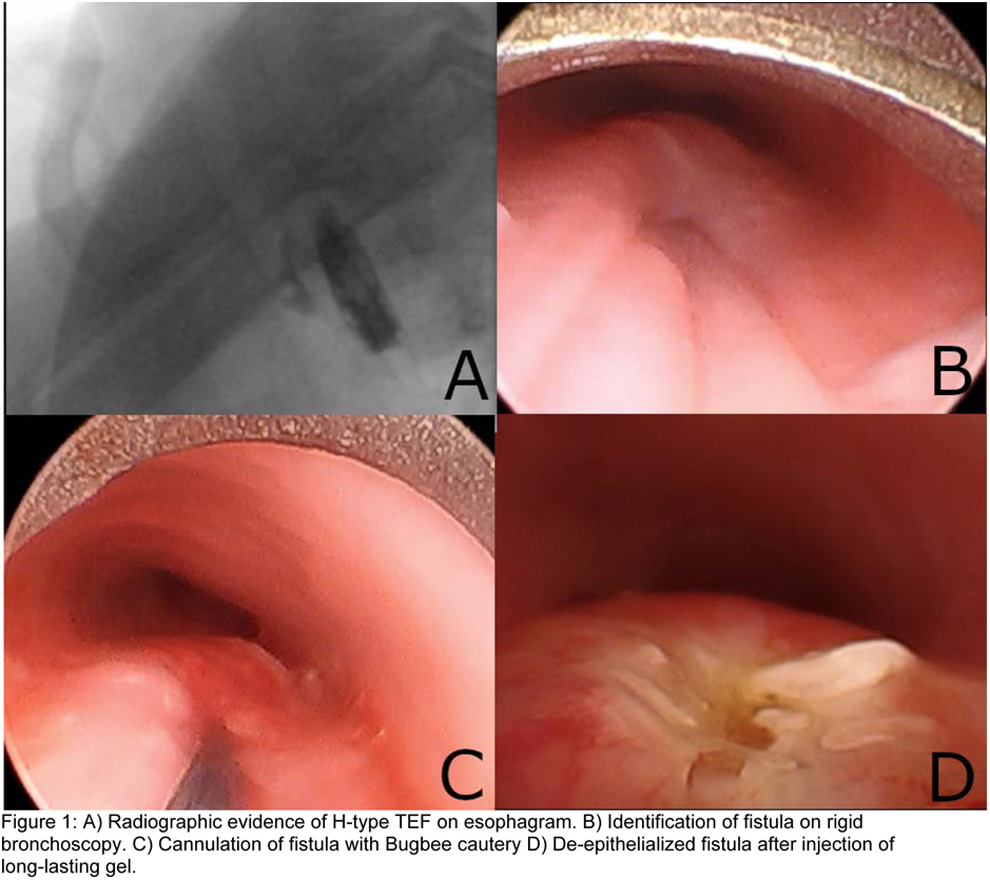
References:
Kappelman MM, Dorst J, Haller AJ, Stambler A. H‐Type Tracheo‐Esophageal Fistula. American Journal of Diseases of Children 1969;118:568. DOI:10.1001/archpedi.1969.02100040570005.
Fallon SC, Langer JC, Peter SDS, Tsao K, Kellagher CM, Lal DR, et al. Congenital H‐type tracheoesophageal fistula: A multicenter review of outcomes in a rare disease. Journal of Pediatric Surgery 2017;52:1711–4. doi:10.1016/j.jpedsurg.2017.05.002.
Allal H, Montes‐Tapia F, Andina G, Bigorre M, Lopez M, Galifer R. Thoracoscopic repair of H‐type tracheoesophageal fistula in the newborn: A technical case report. Journal of Pediatric Surgery 2004;39:1568–70. doi:10.1016/j.jpedsurg.2004.06.030.
Tzifa K, Maxwell E, Chait P, James A, Forte V, Ein S, et al. Endoscopic treatment of congenital H‐Type and recurrent tracheoesophageal fistula with electrocautery and histoacryl glue. International Journal of Pediatric Otorhinolaryngology 2006;70:925–30. doi:10.1016/j.ijporl.2005.10.017.
Meier JD, Sulman CG, Almond PS, Holinger LD. Endoscopic management of recurrent congenital tracheoesophageal fistula: A review of techniques and results. International Journal of Pediatric Otorhinolaryngology 2007;71:691–7. doi:10.1016/j.ijporl.2007.02.022.
QS010 PRELIMINARY RESULTS OF LAPAROSCOPIC STAPLED DUODENO‐DUODENOSTOMY FOR DUODENAL ATRESIA
1Robert Debre Children University Hospital, 2Lucerne Children's Hospital, 3Rocky Mountains Children's Hospital
Background: Duodenal atresia (DA) is ideally repaired laparoscopically. Complications have been previously reported such as anastomosis leakage and stenosis. We report here the first results of laparoscopic stapled anastomosis for duodenal atresia
Patients and method: All patients operated for DA in 3 international pediatric surgical centers were reviewed retrospectively. A 4‐5 mm 30° angle camera and two 3 mm operative port were used. One was switched for a 5 mm to be able to use a 5 mm stapler (Just Right Surgical, Boulder, Colorado, USA). Once the mobilisation of the distal part of the duodenum below the atresia was completed, the proximal and the distal duodenal part were approximated and the anastomosis was then performed using the stapler.
Results: 11 patients were operated on, 6 boys. Two presented with associated anomalies (Malrotation, Down's syndrome and AV canal). Median weight at surgery was 2800 g [2200‐3800]. Median time for the procedure was 60 min [25‐118]. There were no peri‐ or postoperative complications. Median time to 1st feed was 4 days [2‐8] and median time to reach full enteral feed was 8 days [7‐16]. Median discharge day was on day 8 [8‐18].
Conclusion: Laparoscopic DA repair with stapled anastomosis allowed to perform a wide anastomosis without any complication in this series. Full feed could be obtained rapidly. These results need to be compared prospectively with laparoscopic hand‐sewed anastomosis.
QS012 LAPAROSCOPIC RETROPARITONEAL APPENDICOSTOMY FOR ACE PROCEDURE
1Laparoscopy research center, Shiraz University of Medical Sciences, 2Marburg University Germany
Background: Laparoscopic creation of ACE‐Stoma (antegrade colonic enema) for fecal incontinence is an effective and accepted procedure. Two major complications could occur after the operation, internal bowel herniation around the appendix and fecal leakage from the appendix. To prevent these complications a new procedure is presented as a primary report here.
Material and Methods: Two 5 mm ports (one through the umbilicus, second in left lower quadrant) are inserted. The peritoneum just above the appendix is marked and incised. The position of telescope ischanged from umbilicus to the left lower quadrant port for better exploration. At first with a clamp the peritoneum near the umbilicus is dissected award the peritoneal incision over the cecum. And dissection is continued with a Maryland until to the primary peritoneal incision above the cecum. The preperitoneal space is dissected through the umbilicus orifice to allow space for the underlay the appendix. Now the appendix is grasped and pulled through the preperitoneum (space between peritoneum and fascia) into the umbilicus. The course of the appendix and cecum is evaluated and the tip of appendix is sutured into the umbilicus and a catheter is inserted into the appendix.
Result:
Conclusion: Using this new innovation, the chance of internal hernia around the appendix is decreased and also due to prepritonealizing the appendix and some angulation, the chance of leakage through the appendix is decreased. The procedure is secure, simple and safe and is effective in decreasing the complications after ACE procedure.
QS013 GIANT CONGENITAL BLADDER DIVERTICULA. LAPAROSCOPIC RESECTION
Department of Pediatric Surgery. Division of Pediatric Urology and Laparoscopic Surgery. Municipal Children's Hospital. Hospital Pediátrico del Niño Jesús Chair of Pediatric Surgery. Universidad Nacional de Córdoba. Córdoba. Argentina
Objective: The bladder diverticula are herniations of the bladder mucosa between detrusor muscle fibers by a deficiency caused by a weaknesss in the detrusor musculature, to be more common in males and they are usually located cephalic and lateral to the ureteral orifice with an incidence of 1.7%. They can be congenital (solitary, by an inherent weakness in the detrusor muscle) or acquired (multiple and they are the result of bladder outlet obstruction or infectious or iatrogenic)
Material and methods: 5 patients (3) male (3 months, and 2 .6 and 7 years old), respectively, all of them diagnosed with congenital single giant bladder diverticulum, and treated by laparoscopic resection by transperitoneal approach were included in this report, excluding those patients with secondary bladder diverticula and congenital diverticula treated with surgery conventional surgery.
Results: from august 2007 to January 2010 five patients (3 male) respectively, presented the first, prenatal diagnosis of bilateral hydronephrosis, and the remaining two by recurrent episodes of urinary infection. All diagnosed with congenital single giant bladder diverticulum, with absent outlet bladder obstruction. Ultrasonography, voiding cystourethrography, scintigraphy and dynamic renography study were performed. One presented association with vesicoureteral reflux, while in three months old patient bilateral ureterohydronephrosis due to bilateral primary obstructive megaureter was found. all underwent to laparoscopic transabdominal resection of the diverticulum, with low bilateral ureterostomy in the youngest patient with obstructive megaureter. The seromuscular layer was approximated over the small defect. The bladder was drained for 24 hours. All patients were discharged 36 hours after the procedure without complications and followed with renal ultrasonography a week after and voiding cystourethrography 3 months postoperatively with successfully remission of symptoms as well as dilation of the urinary tree.
Conclusion: management of giant bladder diverticulum depends on the patient's symptoms, such as infection, obstruction or reflux. In the absence of these often do not need treatment. However, surgical resection is recommended when episodes of recurrent infection, bladder or ureteral obstruction or persistent reflux are present. Resection of the giant congenital diverticula can be done by open technique, endoscopic or laparoscopic. In our initial experience laparoscopic resection proved to be a feasible and safe technique especially in those cases in which the only treatment required is resection of the lesion without ureteral reimplantation with surgical results close to the open technique also with less morbidity, short convalescence period and hospital stay, with minimally invasive fashion and it should be consider a good alternative for this procedure.
QS014 THE PERFORMANCE OF TWO DIFFERENT TYPES OF GASTROSTOMIES PLACED AT THE TIME OF LAPAROSCOPIC FUNDOPLICATION
King Faisal Specialist Hospital and Research Centre, Jeddah
Aim: To assess the performance of gastrostomy placement at the time of laparoscopic fundoplication.
Method: A retrospective review of a prospectively compiled database of fundoplications undertaken by a single surgeon over 2 decades was undertaken. A cohort having either an endoscopic assisted FRECA gastrostomy or a primary MIC‐KEY Button device at the time of surgery was further evaluated. Demographic, operative and short term performance measures were analyzed.
Technique: The fundoplication was performed utilizing a 4 port approach assisted by a Nathanson retractor for liver retraction. Patients with prior gastrostomy (12) had these taken down laparoscopically before commencement of fundoplication. Gastrostomy placement followed fundoplication and the FRECA device (9 or 15F calibre) was drawn through the newly created wrap under endoscopic guidance. The MIC‐KEY buttons (12 or 14F calibre) were placed using a Stamm technique with the antrum drawn to the anterior abdominal wall via an additional 5mm port placed in the epigastrium.
Result: Forty gastrostomies with mean age 3.6 years (range 0.5–16) were placed in a series of 104 fundoplications. Patients were predominantly female (ratio 1.66:1) with a mean weight of 12.6 kgs (range 3.3 – 31.1). Ninety percent (36) were significantly neurologically compromised with the remainder, failure to thrive (2) and with chronic lung disease (2).
FRECA PEGS were placed in 80% (32) cases with 20%, having MIC‐KEY buttons. All of the latter were significantly neurologically compromised and had full wraps. There were no conversions in this series nor intra‐operative complications related to gastrostomy placement. Mean operative time inclusive of gastrostomy creation was 126 mins and the majority (55%) underwent an anterior partial wrap of the Watson type. Tube feeding was started the day following on surgery.
Three patients with FRECA devices experienced leakage, one lasting 10 days before settling. None of the MIC‐KEY devices leaked but 1 was deflated by PICU staff on the eve of surgery and replaced into the peritoneal space requiring re‐siting in the OR the next day. There were no instances of bleeding.
Patients stayed a median of 4 days (range 2–27).
Conclusion: A significant number of patients (38%) undergoing fundoplication will require a gastrostomy, the majority with neurological compromise. Prior gastrostomy did not prove to be an impediment to deconstruction and replacement. Both PEG devices and primary MIC‐KEY buttons can be placed without difficulty and without any compromise to the wrap. Early gastrostomy leakage was seen in the former group and may prolong in hospital stay. Button devices require close surveillance and instruction to avoid inadvertent removal. Over the medium term, change of PEG to button type device requires general anaesthetic posing further risk to compromised patients.
QS016 LEFT THORACOSCOPIC SYMPATHETIC DENERVATION FOR THE TREATMENT OF “MALIGNANT ARRYTHMIAS” (LONG QT SYNDROME): INITIAL EXPERIENCE
1Hospital Luis Calvo MacKenna, 2Clínica Las Condes
Introduction: Long QT syndrome (LQTS) is a well‐known malignant arrythmia. It is a type of genetic channelopathy and is potentially lethal. It can appear as ventricular tachycardia (VT) or fibrillation (VF). There are 12 related genes. Most common mutations are related to potassium channels genes (KCNQ1, KCNH2) or sodium channels (SCN5A). Medical treatment includes beta‐blocker pharmacotherapy, as well as the use of implantable cardioverter defibrillators (ICDs). Left Cardiac Sympathetic Denervation (LCSD) became popular recently. It has an anti‐fibrillatory potential and could avoid the use of ICDs. Our objective is to show our initial experience with LCSD in five pediatric patients.
Materials and Method: Retrospective study of a case series of five pediatric patients, diagnosed with LQTS and treated with LCSD between 2015 and 2018. Variables analyzed were: Age, sex, presence of genetic diagnosis, symptoms, medical treatment, indication for surgery, length of stay after surgery, surgical complications and follow‐up. Surgical technique: Right decubitus. Three thoracic trocars are placed. Identification of the sympathetic chain. Pleura is opened. Stellate ganglion is localized. Resection from T1 to T4 is performed.
Results: Five patients were diagnosed with malignant arrythmia. Four were LQTS and one was refractory VT. The median age of diagnosis was 6 months (0:120). Genetic diagnosis was confirmed in the four LQTS patients: One was type 1 (KCNQ1), two were type 2 (KCNH2), and only one was type 3 (SCN5A). There was only one patient with family history: father with the same genetic mutation. Symptoms were variable: in two older patients the most common symptom was syncope. One patient was diagnosed antenatally during a fetal monitoring. One patient with family history and the electrocardiograph (ECG) alteration was asymptomatic. ECG showed long QT in the four LQTS patients. One patient presented refractory VT after cardiac surgery. Three patients had ICDs before surgery. Indications for surgery were primary prevention of cardiovascular events in two of the patients, and secondary prevention in the others. No surgical complications were found and no post‐operative Claude‐Bernard‐Horner Syndrome either. Median time of discharge after surgery was 2 days (1:4). Follow‐up was 7 months (1:36). One patient had arrythmia after surgery.
Conclusion: Thoracoscopic LCSD is a well‐known technique used as prevention of cardiovascular events in patients with LQTS. It can be easily reproduced by surgeons with practice in thoracoscopic surgery. In our experience it was a very useful technique without morbidity.
QS018 ADOPTING SINGLE INCISION LAPAROSCOPIC APPENDECTOMY IN CHILDREN—IS IT SAFE DURING THE LEARNING CURVE?
1University of Illinois College of Medicine at Peoria Department of Surgery, 2Children's Hospital of Illinois at OSF St. Francis Medical Center, 3Jump Trading and Simulation
Introduction: Minimally invasive surgery is widespread in training and practice. Laparoscopic appendectomy is the gold standard for treatment of acute appendicitis. Single incision laparoscopy is an alternative approach and has gained widespread acceptance. However, there is minimal data on the outcomes during the adoption of this technique in the era of wide laparoscopic experience in training and practice. Studies have shown a learning curve does exists when transitioning to single incision surgery. This study evaluates the learning curve of contemporarily trained surgeons adopting SILS appendectomy, and more specifically, the safety of the operation during the early phase of this learning curve.
Methods: A retrospective review of 974 consecutive pediatric patients under 18 years of age, who underwent an appendectomy at the Children's Hospital of Illinois from 2005 to 2018 was performed. Acute non‐perforated and perforated appendicitis cases were included. A subgroup analysis was then performed for the technique of single incision laparoscopy. Specifically, the SILS approach utilized a commercially available multiport trocar. The adoption of this technique by new partners in the group was evaluated. Variables collected included age, gender, height, weight, diagnostic modality, antibiotic usage, operative technique, and operative duration. Outcomes measured included length of operation, length of anesthesia time, and complication rate, including surgical site infection. These numbers were compared using a log logistics and a Loess smoothing model.
Results: A total of 438 single incision laparoscopic appendectomies were reviewed. Surgeons performed between 1 and 142 single site appendectomies. A trend towards faster operative times was observed for all surgeons as case numbers increased. Using a statistical modeling for operative time, the odds of still being operated on decreased by 0.997 for each additional case. Based on a 95% confidence band using a Loess smoothing method and this experienced time as the standard, we expect adopting surgeons to reach this experienced level after 51 cases. During the early SILS appendectomy learning curve, there was no significant difference in complication rate when compared to conventional multi‐port laparoscopy (Table 1).

Conclusion: As expected, the more single incision cases performed, the shorter the operative times. More importantly, there was no increase in complication rate during the learning stage of single incision appendectomies in either perforated or non‐perforated appendicitis. When compared to a surgeon specifically trained in SILS appendectomy, the learning curve eventually reaches an inflection point and plateau when a surgeon has reached the experienced level. We conclude that the adoption of SILS appendectomies is safe throughout the brief learning curve among contemporary surgeons with minimally invasive surgical training.
QS019 IT'S A WRAP! OR IS IT? ‐ THE ROLE OF FUNDOPLICATION IN INFANT FEEDING INTOLERANCE
1Cincinnati Children's Hospital, 2Akron Children's Hospital, 3University at Buffalo Jacobs School of Medicine & Biomedical Sciences / John R. Oishei Children's Hospital / Kaleida Health
Purpose: Fundoplication in infants with gastroesophageal reflux and feeding intolerance is one of the most common procedures performed by pediatric surgeons. No consensus exists in the management of these patients, with multiple institutions now opting for medical therapy over surgical treatment. The APSA Outcomes and Evidence‐based Practice Committee released a systematic review concluding that evidence was insufficient to formulate recommendations. The purpose of this study is to analyze the current practices of pediatric surgeons participating in the Case Debates and Controversies session at APSA 2018.
Methods: A case‐based survey was administered during the session, and audience responses were collected through an electronic polling system. The root clinical vignette described a two‐month‐old former premature infant with reflux, normal upper gastrointestinal series, and persistent vomiting after adjusted feeds and prokinetic therapy. The variables adjusted were presence or absence of failure to thrive (FTT), neurological impairment, and complex cardiopathy. One additional question included cough and syncope in the cardiac patient. Polls were presented in a best next step format.
Results: Surgeons selected fundoplication in 14 to 74% of cases. The odds ratio (OR) for fundoplication in the presence of failure to thrive was 1.82 (CI 0.99–3.32, p = 0.05) overall, achieving significance in subgroup analysis for cardiopathy (OR 3.46, CI 1.72–6.94, p = 0.0005) and neurological impairment (OR 1.77, CI 1.01–3.12, p = 0.04), but not in the absence of comorbidities (OR 1.05, CI 0.57–1.94, p = 0.88). The OR for fundoplication in the presence of neurological impairment was 1.97 (CI 1.3–2.99, p = 0.001) and cardiopathy was 1.77 (CI 1.2–2.6, p = 0.0036), independent of FTT status. In subgroup analysis, the greatest predictors for fundoplication were neurological impairment with FTT (OR 2.55, CI 1.42–4.57, p = 0.001) and complex cardiopathy with FTT and cough/syncope (OR 6.97, CI 3.75–12.97, p < 0.0001). Surprisingly, presence of cardiopathy with absence of FTT had the overall lowest odds of fundoplication (OR 0.42, CI 0.21–4.57, p = 0.01).

Conclusion: There is a tendency towards fundoplication in the presence of failure to thrive and comorbidities, particularly in cases where these variables are concurrent. Respiratory symptoms seem to be a strong predictor for fundoplication, although objective analyses cannot be performed due to the absence of this variable in other groups. Further studies are needed to define the role of fundoplication in the management of infant reflux and feeding intolerance.
QS020 FEASIBILITY OF LAPAROSCOPIC PYELOPLASTY IN CHILDREN UNDER 1 YEAR OF AGE: A MULTICENTER STUDY
1Exequiel Gonzalez Cortés Hospital, 2University of Chile, 3Great Ormond Street Hospital, 4Exequiel Gonzalez Cortés Hospital ‐ University of Chile, 5Italian Hospital, 6Garraham Hospital
Introduction: Anderson‐Hynes pyeloplasty is the technique of choice for the treatment of ureteropyelic junction obstruction (UPJO) with a good success rate. Classically, the approach was through lumbotomy. Although the minimally invasive approach has shown to have the same results as the open technique, its diffusion in young children has not been totally approved. The aim of this study is to analyze the experience of 4 centers where laparoscopic pyeloplasties are frequently performed, including children under 1 year of age, evaluating their feasibility and complications.
Material and Method: Descriptive retrospective study of all infants under one year of age who underwent laparoscopic pyeloplasty between 2009 and 2017 at Exequiel González Cortés Hospital (Santiago, Chile), Great Ormond Street Hospital (London, England) and Italian and Garraham Hospital (Buenos Aires, Argentina). Patients were evaluated with ultrasound and renogram before and after surgery. Demographic data, perioperative characteristics, complications and results are described.
Results: In 9 years, of a total of 327 transperitoneal laparoscopic pyeloplasties, 42 laparoscopic Anderson‐Hynes pyeloplasty were performed in patinents under 1 year of age; 35 males and 7 females. Two cases had bilateral UPJO. Out of 44 renal units, 12 were right‐sided. Prenatal diagnosis was present in 31 cases (70%). Average age at surgery was 6 months (range 1–12m); 64% (n = 27) were infants under 6 months. Average weight at surgery was 8 kg (range 5‐10k), where 31% (n = 13) weighed less than 7 kg. Average skin‐to‐skin time was 145, min. (range 75–230 m). After an average follow up of 22.5 months (range 4–75 months), 2 (4.5%) patients progressed with complications, one of them with recurrence of UPJO, which required new laparoscopic pyeloplasty in one and nephrectomy in the other as progressive deterioration of renal function was demonstrated.
Conclusion: Laparoscopic AH pyeoloplasty in children under 1 year old is easily and with simil results than in older children, as well as with the open approach. Once experience has been achieved in laparoscopic pyeloplasty, the factor of age and weight has ceased to be a limiting factor, gaining strength and popularity in all pediatric age groups with comparable results as classical AH pyeloplasty.
QS021 THORACOSCOPIC HARVEST OF THE PHRENIC NERVE FOR NERVE TRANSFER IN A PEDIATRIC CASE OF VIRALLY‐INDUCED UPPER EXTREMITY PARALYSIS
Children's Hospital Los Angeles
Acute flaccid myelitis (AFM) is a rare complication of common respiratory viral illnesses that results in the sudden onset of partial or total paralysis of the extremities. The upper extremities are most frequently involved and only half of those affected recover spontaneously. In partial paralysis, nerves from the uninjured portion of the brachial plexus, or nearby nervous system, can be used as donors to transfer functioning axons to the injured nerves. However, in total palsies, very few donor nerve options exist. Two‐thirds of those affected by acute flaccid myelitis also have paralysis of the spinal accessory nerve, one of the most commonly used donor nerves. In these cases, alternative extraplexal donor nerves with sufficient power and length to reach the target(s) must be sought. Here, we describe the thoracoscopic harvest of one such alternative donor source, the phrenic nerve, for transfer to the posterior interosseous nerve and nerve to the long head of the triceps to power elbow, wrist, and hand extension.
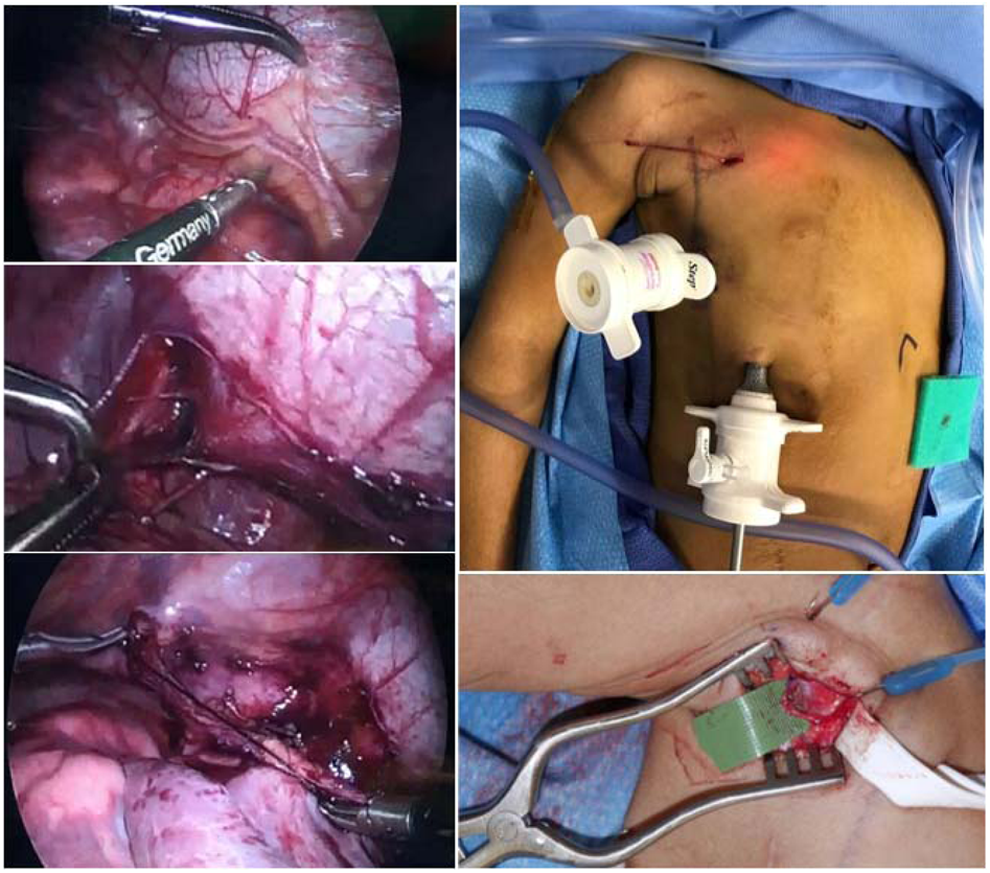
Our patient is a 3‐year‐old, formerly right‐hand‐dominant, girl who developed acute flaccid myelitis after an episode of enterovirus‐induced respiratory illness. All of the muscles of the right upper extremity were paralyzed with the exception of the supinator muscle. She had previously undergone coaptation of several intercostal nerves to the musculocutaneous nerve to power elbow flexion and the median nerve to restore wrist and finger flexion. To drive elbow, wrist, and digit extension, another donor nerve was needed. After phrenic nerve studies demonstrated normal and symmetric excursion of the diaphragm on both sides, we proceeded with phrenic nerve harvest. A 5 mm port was inserted into the right second intercostal space under single lung ventilation followed by subsequent placement of two additional 5 mm trocars into the right thorax under direct thoracoscopic visualization. The phrenic nerve was carefully dissected proximally from the superior vena cava and pericardium and distally to the level of the diaphragm where the nerve was clipped and cut to obtain maximal length (5 cm in this case). The distal end of the phrenic nerve was then delivered out through the superior trocar site and tunneled subcutaneously to reach nerve targets in the posterior axillary space.
One year later, our patient has adapted well after undergoing physical and biofeedback therapy to relearn how to control her once paralyzed arm. Now, she coughs to flex her right elbow and breathes deeply to extend her arm. She is able to perform complex multi‐functional tasks, such as manipulating a door handle. Typically, great care is taken to spare the phrenic nerve. However, we present a scenario where the phrenic nerve can be safely harvested for nerve coaptation in a select population suffering from total upper extremity paralysis.
QS022 SIMULATION IN PEDIATRIC VIDEO SURGERY ‐ PROPOSAL OF TRAINING WITH MODELS OF SIMPLE AND REPRODUCIBLE EXERCISES ELABORATED BY RESIDENTS
Hospital Pequeno Príncipe
Introduction: The increase in the use of minimally invasive surgery in all fields of surgical speciaties, has made the trainig of specific habilitites in videosurgery essential for the surgeons training these days. In terms of Pediatric Surgery, for the most part, the residents do not have a specific simulation training program, including classes and supervised activities in minimally invasive surgery, during their residencies. Most of the time the learning process occurs in vivo or in short courses.
Objectives: To describe and evaluate a set of low cost and easily executed exercices, created by the residentes for the training and practcing of basic skills.
Methods: Seven exercices were elaborated with materials of daily use in the hospital, aiming to simulate maneuvers representative of the main surgeries performed The residents were guided by a written and video description showing the execution of the exercises. They performed the exercices and answered to a previosly elaborated questionaire which included the impression they had about the exercices, the degree of dificulty and their importance. The same activity was repeated three weeks later to evaluate the results after a period of individual training.
Results: Most of the nine residents questioned received in vivo training during theirs general surgery residency programs. Only 33.4% of them received supervised training. Some of the reported alternatives for the learning process were telemedicine, unsupervised training or other types of courses. The participants considered the exercices to be representative of the actual skills needed in videosurgey. Exercises 2‐knot, 3‐sliding knot and 4‐extracorporeal sliding knot were considered the most representatives of them all (100%). The exercices that most required skill for execution were 5‐sutures, 7‐incision with scissors and the 2‐knot, in this order of dificulty. In the 2‐knot exercise one participant acquired this ability during the training period, and in the 7‐incision scissors exercise two participants acquired this ability. There was no difficulty in finding the materials or assembling them for the training before the second part of the study. About 77% of the participants planned to dedicate up to 30 minutes per week of exercise training, 2 or 3 times a week with the intent to repeat the same program after 3 weeks. No resident what was planned in relation to the training, and the main reasons listed were the great amount of activities of the residence, no specific training period, no suppervision during the training and the abscence of na appropriate place for the training. On average, participants spent one day a week for 3 weeks, less than 30 minutes for training.
Conclusion: It is clear the importance of the simulation in video surgery during the formation of the pediatric surgeon. A simple set of exercises can be developed by residents themselves and make simulated training doable even without the availability of specific and expensive materials and programs. However, the presence of a tutor and the scheduling of exclusive training schedules is necessary for these to occur satisfactorily. A study with a larger number of participants, and a longer follow‐up period, is necessary to evaluate if there was improvement of the skills in video‐surgery, as well as to compare it with other simulation exercises already reported in the literature.
Key words: videosurgery, simulation, surgery training
QS023 THE IMPACT OF A TRAINING PROGRAM IN CMI WITH BIOLOGICAL MODEL
Centro Experimental ‐ Instituto Nacional De Salud Del Niño San Borja
During the last decades, minimally invasive surgery has become a common practice in all types of surgical disciplines, in Pediatric Surgery the minimally invasive approach is recommended as the treatment of choice for multiple abdominal and thoracic pathologies, in our local environment not there is a specialty training program; for this reason a program of basic and intermediate education was implemented, and models with biological material (Humid) of the most frequent pathologies were created: esophageal atresia, biliodigestive derivation, Diaphragmatic hernia in space and scale of newborns
Objective: To evaluate the development of skills that surgeons in pediatricians and doctors in Surgery training, in laparoscopic surgery, through our learning models, with short‐term practical courses and obtain their assessment.
There were 56 participants, 24 in a first basic course (28 hrs), with obtaining basic skills, and 32 in a second phase: intermediate course (24 hrs), applying the specific training models. The evaluation of skills was carried out based on the experience, the participants of the intermediate course had as requirement to have realized a certified basic course. Both the simulator exercises and the surgical techniques practiced were evaluated objectively using the OSATS global evaluation scale, the evaluation was complemented with a list of specific tasks for intracorporeal suture and another for the models created with biological tissue; The execution times of the exercises were recorded at the beginning and at the end of the course, both in the simulator and in application of the specific models, as well as an evaluation survey of the training program with a Likert scale of 5 points.
Results: the grade averages were significantly higher after completing the workshop. The greatest difference was observed in operative knowledge (0.27 before the workshop versus 0.55 after the workshop, p < 0.05). All participants who completed the course applauded the realism and efficiency of this type of training. The feedback of the force and manipulation allowed in the specific models and their capacity of repetition and reproduction allows to develop skills in spaces very close to surgery in small cavities (similar proportion to neonates).
Conclusion: The program of training in training and considering the biological models created (real simulation in size and proportion to neonates), allows the acquisition of surgical skills in a meaningful way to the training of our pediatric surgeons and local doctors in training, not described before.
QS024 FEASIBILITY STUDY OF THORACOSCOPIC SURGERY OF SEVERE CONGENITAL DIAPHRAGMATIC HERNIA IN NEONATES AND RESOLUTION OF SURGICAL DIFFICULTIES
Capital Institutes of Pediatrics
Objective: The aim of this report is to explore the feasibility of thoracoscopic surgery of severe congenital diaphragmatic hernia in neonates and analyze the difficulties during the surgery.
Methods: The clinical data of 14 cases of neonatal severe diaphragmatic hernia (≤28 days) treated by thoracoscopic surgery in our hospital from April 2014 to June 2018 were retrospectively analyzed, including 8 cases of male and 6 cases of female. All the children were diagnosed by imaging examination (ultrasound, MRI) and confirmed as CDH after surgery. Severe CDH was diagnosed if at least one of the following conditions was met: gestational age of prenatal diagnosis ≤25w; hepatic herniation; LHR <1.0; SNAP‐score >28; Brindle score ≥3.
Results: All of the 14 children completed thoracoscopic diaphragm repair without transfer. 13 children were diagnosed with CDH by ultrasonography prenatal and 1 was diagnosed by chest X‐ray after birth because of respiratory distress. In 13 cases, tracheal intubation was performed immediately after birth, and 1 case 2 hours after birth. 13 cases were left diaphragm hernia and 1 case were right. Average gestational age of prenatal diagnosis was (28.6 ± 5.9) w, the average SNAP‐value was (22.6 ± 6.7), Brindle value was 1 (0, 3); The average gestational age at birth was (37.5 ± 2.1) w, and the average birth weight was (2.9 ± 0.6) kg. The average age of surgery was 1.5 (0.8, 2.1) d, and the average time of surgery was 180 (120, 200) min. The mean length of hospital stay was 17 (12, 28) d and the mean postoperative ventilator usage was (4 ± 1.3) d. Among the surviving children, the minimum birth weight was 1.84kg, the minimum prenatal diagnosis age was 18 weeks, and the minimum birth age was 31w.1 case used patch by thoracoscopic repair the giant diaphragm defect, then cured and discharged .2 cases complicated postoperative pleural effusion, which were cured after 7 ∼ 30 days conservative treatment. Of the 14 cases, 11 survived and 3 died which including 2 due to postoperative respiratory failure and 1 due to renal failure. All the children were followed up for 1 month to 4 years, and 1 patient using patch experienced recurrence. After the second thoracoscopic patch repair, the patient recovered. And the remaining children had normal growth and development without related complications.
Conclusions: Thoracoscopic surgery for neonatal severe CDH is safe and feasible, with advantages of small trauma and rapid postoperative recovery, etc. When the operator has abundant endoscopic experience and the vital signs of the child are stable, thoracoscopic surgery can be given priority. It is possible to repair the defect of diaphragm by patch under thoracoscope.
QS025 OPEN VERSUS LAPAROSCOPIC SPLENECTOMIES: COMPARATIVE STUDY PERFORMED AT PUBLIC HOSPITAL IN BRAZIL
Pediatric Surgery department, Federal University of Paraná
Introduction: Splenectomy is a very old surgical procedure, which in childhood is usually indicated for benign hematologic diseases or traumatic rupture. In 1991, the first laparoscopic splenectomy was reported, since then the laparoscopic approach is becoming more popular than the open one. In most public hospitals in Brazil, where harmonic scalpel or other vessel sealing devices are not available, open splenectomy may be the preferred method of most surgeons to guarantee intraoperative safety.
Objectives: To compare open and laparoscopic splenectomy in children in a public hospital in Brazil.
Methods: Retrospective study conducted between January 2010 to June 2018. Pediatric patients (0 to 14 years old) that were submitted to open or laparoscopic splenectomy at the University Hospital of Federal University of Paraná were included. Clinical, laboratory, imaging and surgical data were collected prospectively.
Results: In 8 years, 35 patients were submitted to splenectomy, mean age of 4 years old (1‐13 years old) and 54% (19/35) were female. 69% (24/35) had sickle cell anemia and 23% (8/35) spherocytosis, and indication for surgery was a previous episode of splenic sequestration. Mean pre‐op hemoglobin was 9.3. 37% (13/35) of the surgeries were performed laparoscopically, all without harmonic scalpel or other vessel sealing devices, only with hook, bipolar and manual vessel ligation. All open splenectomies (22/35) were operated by a left subcostal incision. Only 2 intraoperative complications were reported: one bleeding in the laparoscopy group with no need for transfusion, and one prolonged surgical time due to technical problems with the video equipment. Mean operative time on laparoscopy group was significantly higher than in open group (186 vs 66 min). Postoperatively there were 2 wound infections on the open group, and no re‐operations. One child died on 1m post‐op probably due to sepsis.
Conclusion: Performing laparoscopic splenectomy without harmonic scalpel or other vessel sealing devices is feasible but it implicates in a significantly higher surgical time.
QS026 MICKEY VS MINI: A RANDOMIZED CROSS‐OVER TRIAL FOR PARENT PREFERENCE
Children's Mercy Kansas City
Introduction: Laparoscopic gastrostomy with primary button placement is one of the most common operations in pediatric surgery. Data around parental preference for the 2 main low‐profile balloon gastrostomy buttons are lacking.
Methods: We conducted a prospective, randomized crossover trial to evaluate parental preference. We included children age 0‐5 years requiring a gastrostomy with a tube length of 0.8‐1.0 cm. Patients were randomized to MIC‐KEY or MiniONE button at placement. At the 2 month initial change, the patients were given the opposite button of randomization. At the 4 month follow‐up, parents were asked which one they wanted to keep.
Results: 343 patients were screened for eligibility, of which 123 did not meet inclusion criteria and 61 declined to participate. 158 subjects were randomized, 79 each to receive MiniONE or MIC‐KEY button first. There were no differences in age, weight or gender distribution. 60 with MiniONE and 68 with MIC‐KEY completed their first follow‐up. 18 with MiniONE and 3 with Mickey did not cross over at this stage, wanting to keep their first button. 43 with initial MiniONE and 65 with initial MIC‐KEY completed crossover, 69% of whom preferred the MiniONE button. (McNemar's p < 0.001). Including those who preferred their first button and declined to switch buttons at 2 months, 92 of 128 (72%) kept the MiniONE.
Conclusion: In a randomized crossover trial of the two of the most common low‐profile gastrostomy tubes in children, parents demonstrated a strong preference for the MiniONE button.
QS027 LAPAROSCOPIC TREATMENT OF CONGENITAL NONPARASITIC LIVER CYSTS IN NEWBORNS
1Pediatric Hospital Irkutsk, 2Pediatric Hospital Kemerovo
Introduction: Congenital nonparasitic liver cysts in newborns are rare. Thanks to the achievements in antenatal diagnostics, this anomaly began to be diagnosed much earlier. Surgical excision of these formations is necessary to prevent complications. Reports of laparoscopic treatment of simple liver cysts in children are rare. We present a series of endosurgical treatment of patients, numbering 5 children and coming from a single surgical center.
Material and methods: Data of 5 patients with nonparasitic liver cysts were collected at the Center for Neonatal Surgery, beginning in 2014. The laparoscopic technique of the operation was an enucleation of the cyst. After the inspection of the abdominal cavity and the location of the cysts in relation to the surrounding tissues, puncture and evacuation of the cyst were performed. With the help of monopolar coagulation, complete resection of the cysts was performed. At the conclusion of the operation, plasma coagulation was carried out in the argon gas atmosphere of liver tissue in the region of the cyst bed. The analysis of the patient's demographic data and parameters of hepatic cysts (location, histological structure) is performed. Early and long‐term results of laparoscopic operations were studied.
Results: All patients were newborns. Of these, 3 girls and 2 boys. The primary diagnosis was established during prenatal ultrasound examination. The laparoscopic approach was used in all patients, with the use of which a complete resection of pathological liver formations was performed. Histological examination revealed a benign single nonparasitic liver cyst lined with a cylindrical or flat linear epithelium. The early postoperative period was not accompanied by the development of complications. In the long‐term follow‐up period, there were no recurrences of the disease.
Conclusion: The study presents one of the largest series of laparoscopic excision of nonparasitic liver cysts in newborns. It was found that laparoscopy is a safe and effective method of treating of congenital hepatic cysts.
QS028 IS THE LAPAROSCOPIC VASCULAR HITCH PROCEDURE WORTH TAKING INTO ACCOUNT IN CHILDREN WITH URETEROPELVIC JUNCTION OBSTRUCTION CAUSED BY POLAR VESSELS
Gdansk Medical University
Purpose: Pediatric ureteropelvic junction obstruction (UPJO) is a common problem which may be rarely caused by extrinsic compression from crossing vessels (CV). The transposition of lower pole crossing vessels (vascular hitch‐VH) has been reported as an alternative technique to dismembered pyeloplasty for the treatment of UPJO. We report a prospective study of laparoscopic VH in children with intermediate follow‐up.
Methods: Prospective analysis of 12 consecutive children treated by laparoscopic transposition of crossing vessels at our institution and age matching 28 children treated by laparoscopic dismembered pyeloplasty. Patients were selected on the basis of clinical history, renal ultrasonography, preoperative MAG‐3 renal scan, and or magnetic resonnance urography. Selection criteria for VH procedure included presence of lower pole crossing vessels with moderate hydronephrosis and poor renal drainage. Extrinsic compression by CV was usually presented symptomatically in older children with recurrent abdominal/flank pain and haematuria. All patients presented in ultrasound intermittent hydronephrosis. During operation diuretic test (DT) was performed in all patients before and after the vessels transpositions confirming the extrinsic UPJO and normal ureter with UPJ peristalsis. In the cases of negative DT‐ laparoscopic dismembered pyeloplasty was performed. All children were followed clinically with renal ultrasonography and postoperative MAG‐3 renal scan. Success was defined by symptoms resolution with improvement in hydronephrosis and drainage.
Results: 12 children (4 boys, 8 girls) presenting with flank pain, hydronephrosis SFU grade 2 or 3, impaired drainage on MAG‐3 and lower‐pole crossing vessels at a mean age of 8.5 years (range 4.75‐16) were selected for vascular hitch. Operations were performed through transperitoneal laparoscopy. The DT was negative in 3 cases. The mean operative time of vascular hitch was 96 min. (40‐130), and length of hospital stay was 3 days (1‐5). No ureteral stents or urethral catheters were placed intraoperatively. With a mean follow‐up of 18 months (11‐36), outcome was successful in all patients, with resolution of symptoms, improved hydronephrosis and better drainage on MAG‐3. Two children have shown improvment of hydronephrosis and symptoms, but still show impaired drainage on MAG‐3 renal scan. There was no significant difference in success rate between consecutive VH and laparoscopic dismembered pyeloplasty patients.
Conclusions: At intermediate follow‐up the laparoscopic vascular hitch procedure, has been successful in treating a selected group of children with obstructive CV, and represents a safe and reliable alternative to standard dismembered pyeloplasty in the management of symptomatic children where CV is considered the only etiology. In our opinion VH is less technically demanding than laparoscopic pyeloplasty, resulting in a lower complication rate and a significantly reduced hospitalization. VH is not an alternative corrective surgery of UPJO, but a complementary way to repair hydronephrosis in very selected cases. The necessary conditions for success are careful patient selection based on preoperative clinical and radiologic findings that are diagnostic of extrinsic UPJO, combined with intraoperative DT to confirm the appropriate selection of corrective procedure.
QS029 VIDEO‐ASSISTED THORACOSCOPIC LOBECTOMY IN CHILDREN: A RETROSPECTIVE SINGLE‐CENTER STUDY WITH 490 CONSECUTIVE CASES
Department of Thoracic Surgery, Beijing Children's Hospital, Capital Medical University, National Center for Children's Health
Objective: To evaluate the safety and efficacy of video‐assisted thoracoscopy for lung diseases in infants and children.
Methods: From September 2014 to June 2018, a retrospective review was conducted for 490 consecutive patients undergoing video‐assisted thoracoscopy. Clinical data, surgical procedures, surgical findings and postoperative pathological examinations were analyzed.
Results: All procedures were successfully completed. There was no single case of severe complication and re‐operation. There were 300 boys and 190 girls. The mean age was (19.2 + 50.5)(2‐211) months, mean operative duration (60.0 + 42.0)(10‐300) minutes and mean blood loss (2.0 + 3)(1‐400) ml. There were conversions into open thoracotomy (n = 24, 4.9%). Postoperative pathological examinations revealed lung cystic adenomatiod malformations, i.e. congenital pulmonary airway abnormalities (CPAM, n = 255), pulmonary sequestrations (n = 160), lung tumor (n = 23), emphysema (n = 18), bullous lung disease (n = 12), pulmonary cyst (n = 3), pulmonary interstitial lesions (n = 4), bronchitis (n = 2), bronchogenic cyst (n = 2), congenital pulmonary airway dysplasia (n = 1), bronchiectasis (n = 1), bronchial atresia (n = 2), pulmonary vascular lymphatic malformation (n = 1), pulmonary arteriovenous fistula (n = 1), pulmonary parasites granuloma (n = 1), diffuse alveolar hemorrhagic syndrome (n = 1), pulmonary fungal infection (n = 1), langerhans histiocytosis (n = 1), empyema (n = 1).
Conclusions: Safe and effective for pulmonary resection, video‐assisted thoracoscopy is indicated for treating lung diseases in infants and children. This mini‐invasive approach offers less surgical trauma, minor postoperative pains and shorter hospitalization. In addition, operative scar is smaller and cosmetic outcomes are better.
QS030 CURRENT MINIMALLY INVASIVE APPROACH FOR MEDIASTINAL NEUROBLASTOMA: RESULTS FROM A NATIONWIDE SURVEY IN JAPAN
1Kagoshima University, 2Kyushu University, 3National Center for Child Health and Development, 4Niigata University, 5Kyoto Prefectural University of Medicine, 6Osaka Medical Centre, 7Hyogo College of Medicine, 8Keio University School of Medicine, 9Nihon University School of Medicine, 10Hiroshima University Hospital, 11Tohoku University, 12Kumamoto Rosai Hospital
Background: Recent advances in minimally invasive surgery (MIS) have brought many advantages, including less operative scarring, an earlier recovery, and an improved cosmetic appearance in both adult and pediatric patients. Neuroblastoma (NB) is suitable for an MIS approach, but its indications and technical feasibility are unclear. Our study assessed the present status of the MIS approach for NB in Japan after mass screening of NB, focusing on mediastinal NB.
Methods: Preliminary questionnaires requesting the numbers of NB patients who underwent surgery via the MIS approach from 2004 to 2016 were sent to 159 major institutes of pediatric surgery in Japan. Secondary questionnaires were then sent to the institutions in which NB patients were treated via the MIS approach to collect detailed data.
Results: We received replies from 133 institutes (83.6%). Of these 133 institutes, 82 (61.6%) reported operating on NB patients(total number of operative cases:1435). The MIS approach was applied in 174 cases (12.1%). Of these 174 cases, the completed forms of 139 (79.9%) patients were sent back, and 39 had mediastinal NB while 100 had abdominal NB. Regarding mediastinal NB, a detailed analysis was performed based on the secondary questionnaires. The male/female ratio was 28 (71.8%)/11 (28.2%). The mean age was 3.2 years old (range: 1 month to 12 years old). Associated anomalies were recognized in three cases (cerebral ataxia, cleft palate, and undescended testis in one each). The clinical stages were as follows: 1 in 14 (35.9%), 2 in 6 (15.4%), 3 in 7 (17.9%), 4 in 8 (20.5%), 4S in 1 (2.6%), and unknown in 1 (2.6%). Therapeutic summaries of the MIS approach for mediastinal NB are shown in Figure 1. Fourteen cases (35.9%) underwent a laparoscopic biopsy, and none were converted to thoracotomy. The mean tumor size at the thoracoscopic biopsy was 6.7 ± 3.7cm (range:3.2–15 cm). The only monopolar energy devices were used. Twenty‐eight cases (71.8%) underwent MIS for radical resection, and none were converted to thoracotomy. Primary thoracoscopic radical resection was performed in 21 cases (53.8%). The mean tumor size for thoracoscopic radical resection was 5.2 ± 2.4 cm (range:2.6–7.6 cm). The mean operative time was 162.7 ± 41.4 min. The maximum blood loss was 150 ml. The operative procedures of radical resection were as follows: total resection in 18, subtotal resection in 9, and partial resection in 1. The number of trocars used in radical resection was 3 in 26 cases and 4 in 2 cases. The energy devices used were monopolar, bipolar, vessel sealing system, ultrasonically activated device, and combinations of these devices. Postoperative complications of radical resection were recognized in one case (Horner's syndrome). The obtained pathological diagnoses were as follows: undifferentiated in 2(5.1%), poorly differentiated in 14(35.9%), ganglioneuroblastoma‐intermixed in 8(20.5%), ganglioneuroma in 10(25.6%), ganglioneuroblastoma in 1(2.6%), unknown in 3(7.7%), and other in 1(2.6%). Eleven cases (28.2%) were treated by thoracotomy and conservative therapy.
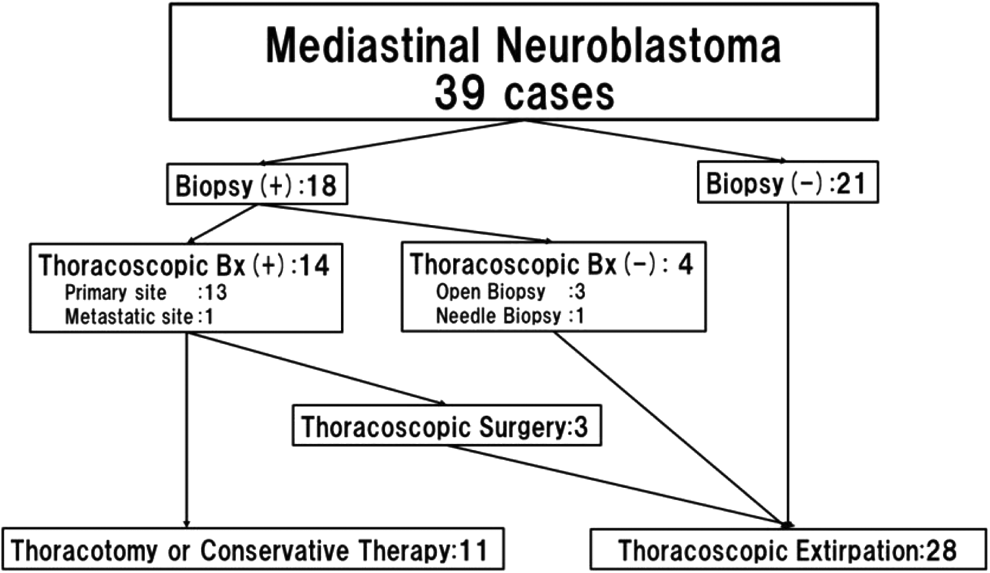
Conclusions: The MIS approach was performed in limited cases of mediastinal NB. No severe complications were noted, but the indications were determined based on each institution's experiences and surgeons' oncological therapeutic strategies. The indications and technical standardization of the MIS approach for mediastinal NB should be determined through prospective randomized trials.
QS031 LAPAROSCOPIC PYELOPLASTY – COMPARING OUTCOMES BETWEEN CHILDREN UNDER AND OVER 1 YEAR‐OLD IN A SINGLE CENTER
1Department of Pediatric Surgery, Centro Materno Infantil do Norte, Centro Hospitalar Universitário do Porto, Porto, Portugal, 2Department of Pediatric Surgery, Hospital de Braga, Braga, Portugal, 3Department of Pediatric Surgery, Hospital de Braga, Braga, Portugal; Life and Health Sciences Research Institute (ICVS), School of Medicine, University of Minho, Braga, Portugal; ICVS/3B's – PT, Government Associate Laboratory, Braga/Guimarães, Portugal
Introduction: Minimally invasive pyeloplasty is becoming the gold standard for ureteropelvic junction obstruction management in children. The laparoscopic approach demands complex technical expertise, usually being disfavored in infants under 1 year old.
Methods: A prospective analysis of all patients submitted to laparoscopic dismembered pyeloplasty between March 2016 and August 2018 in a single institution was performed. Demographic data were collected, as well as operative details such as operative technique, operative time, type of urinary diversion, intra and post‐operative complications and length of hospital stay. Comparative analysis concerning surgical outcomes was performed between subjects younger than 1 year and older using Mann‐Whitney U test with a significance level p < 0.005.
Results: A total of 14 laparoscopic pyeloplasties were performed, 8 of which in infants under 1 year old. Study population included 13 children, 57,1% being male. Median age at time of surgery was 8.35 months (min:max 3,0: 192,9) and median weight was 8,57kg (4,6: 64). 4 children (28,6%) presented preoperatively with urinary tract infection. All procedures were performed transperitoneally, using a 5mm umbilical port (for a 30° scope) plus two 3 mm working ports. Trans‐anastomotic stenting was applied in all patients, and no abdominal drains were used. Mean operative time was 175 minutes(110:240), the longest procedure being a conversion due to intraoperative bleeding. No other intra or post‐operative complications occurred. Median length of hospital stay was 2.5 days. Reduction of hydronephrosis was documented by US in all cases with follow‐up longer than 6 months (n = 11). No significant differences between infants younger than 1 year and older children regarding operative time, complications and length of hospital stay were found (p > 0.05).
Conclusion: Laparoscopic pyeloplasty is a safe and effective approach for children of all ages, including infants under one year of age without intraoperative time lengthening or added intra or postoperative complications.
QS032 THE VERY VERMIFORM APPENDIX‐OPERATIVE MANAGEMENT
1Memorial Hermann Hospital, Houston, TX, 2Morgan Stanley Children's Hospital NYP
Background: Laparoscopic appendectomy techniques typically include delivering the appendix via the umbilicus. Minimizing wound contamination when removing the appendix reduces wound infection. Protection with a retrieval bag may be limited by the size of the port used, particularly in small children.
Objective: Factors may preclude use of a standard endoscopic retrieval bag to limit wound contamination in laparoscopic appendectomy. We describe a technique to allow use of bag when small ports are used.
Methods & Materials: A 7 year‐old boy presented to the emergency department with a 2 month history of right lower abdominal pain. His abdomen was soft with mild lower abdominal tenderness. Abdominal imaging revealed a normal appendix with a large fecal load. Bowel prep was carried out. One week later his pain was worse. Exam again revealed right lower abdominal tenderness without guarding. Ultrasound did not identify the appendix. MRI showed mild dilation of the appendix with wall enhancement, felt to represent resolving appendicitis. Following a discussion with the patient his parents, we agreed to perform laparoscopic appendectomy because of his ongoing pain.
Three 5 mm ports were used. The appendix was found lateral to the cecum without gross inflammation. The blood supply was divided and the skeletonized appendix was secured with endoscopic loop ties. Upon dividing the appendix, soft fecal material freely protruded from the cut edge of the specimen. On close inspection, pinworms were identified. The umbilical port was removed. A 10 mm endoscopic retrieval bag was extended 2cm beyond the end of its housing. The umbilical wound was probed with a clamp and the fascia was gently widened. The bag ring was introduced into the abdomen under direct vision. The ring and bag were deployed. The appendix was inserted into the bag; the bag was sealed and removed without fecal material contacting the wound.
Results: The patient recovered uneventfully. Albendazole was given and repeated at 2 weeks. On follow‐up at 1 month his abdominal pain had resolved.
Conclusions: Using a 5mm port does not preclude use of a 10mm retrieval bag to remove dirty material during laparoscopic appendectomy.
QS033 IS THE LAPAROSCOPIC APPROACH SAFE FOR INGUINAL HERNIA REPAIR IN PRETERMS?
1Hospital Álvaro Cunqueiro, 2Hospital Universitario 12 de Octubre
Introduction: Although laparoscopic inguinal hernia repair in children has gained popularity in the last decades, this approach remains uncommon in preterm infants. The aim of this study was to compare the characteristics and the outcomes of indirect inguinal hernias in term and preterm infants.
Material and methods: From January 2002 to November 2015, all charts of the pediatric patients who underwent laparoscopic indirect inguinal hernia repair in one single institution within the first 6 months of life were revised. The data of 156 patients were analyzed retrospectively. Patients were divided in two groups: group I including the term patients and group II including the preterm patients. Prematurity was defined as less than 37 weeks of gestation at birth. A p value of less than 0.05 was considered statistically significant.

Results: A total of 90 term infants and 66 preterm infants were included. In the group I, preoperative diagnosis was right‐sided inguinal hernia in 20% of patients, left‐sided in 22.2% and bilateral in 57.5%; while in the group II, preoperative diagnosis was right‐sided inguinal hernia in 42.4% of infants, left‐sided in 15.2% and bilateral in 42.4% (p = 0.01). In group I intraoperative diagnosis was right‐sided inguinal hernia in 10% of patients, left‐sided in 16.7% and bilateral in 73.3%; while in the group II, intraoperative diagnosis was right‐sided inguinal hernia in 25.8% of infants, left‐sided in 12.1%, bilateral in 60.6% and there was no hernia in 1 patient (p = 0.02). However, there was no statistically significant difference in the correct intraoperative diagnosis between both groups (p = 0.59%). A comparison of postoperative complications in both groups is shown in Table. No statistical significance was observed between the two groups regarding postoperative complications.
Conclusions: Bilateral inguinal hernia is more frequent in preterm infants as compared to term infants, whereas the incidence of right‐sided inguinal hernia is higher in term patients. Laparoscopic inguinal hernia repair in preterm infants is safe and it is not associated with higher rate of postoperative complications.
QS034 UNIVATS MODIFIED TECHNIQUE FOR LARGE PULMONARY MALFORMATIONS IN SMALL BABIES
Nuestra Señora de Candelaria University Hospital, Santa Cruz de Tenerife, Spain.
Introduction: Performing a thoracoscopy in a small pediatric patient can be challenging at times. We present two clinical cases where an UNIVATS modified technique was used to perform the resection of a right pulmonary sequestration in one case and a lower left lobectomy in the other one.
Clinical Cases: Two patients, nine and eleven months old, were taken to the operating room for a resection of a right inferior extralobar pumonary sequestration and a lower left lobectomy, respectively.
The patients were placed in corresponding lateral decubitus position, with the arm ipsilateral to the lesion placed above the head and at 90° of flexion.
Surgical technique: First, a three cm mini‐thoracotomy is performed just below the scapula, at the level of the fifth intercostal space, between the anterior and medial axillary lines. Once inside the thoracic cavity, a 5 mm trocar was placed at the level of the seventh intercostal space, medial axillary line, for the 5 mm 30° telescope.
The patient is placed faced to the surgeon and the monitor behind the patient. The scrub nurse stands next to the monitor.
An extra small wound retraction ring is inserted into the minithoracotomy and the 5 mm 30° optic through the port. We began to perform the resection of the right pulmonary sequestration and the left inferior lobectomy through the minithoracotomy. In both cases, 3 mm thoracoscopic and a 10 mm stappler instruments were introduce by mini‐thoracotomy and the procedure was performed as usually, with both, direct and thoracoscopic vision.
Once the surgery is finished, the piece is easily removed through the mini‐thoracotomy and the trocar orifice is used to leave a thoracic drain in both cases.
Conclusion: The UNIVATS modified technique, is a feasible and reproductible technique.
The mini‐thoracotomy allows the use of whole stapplers range, without addicional wounds under thoracoscopic control and permits an easy removal of the specimen, being the size of the incision similar to that used in thoracoscopy. We are able to feel the tissue, being this an advantage in other thoracic procedures. The postoperative period is much more bearable, with less pain and more comfort for the patient if we compare it with traditional thoracotomy.
QS035 SINGLE INCISION PEDIATRIC ENDSURGERY (SIPES) CHOLYCYSTECTOMY FOR HEMATOLOGICAL DISEASE DONE BY TRAINEES
QS036 LAPAROSCOPIC HIGH LIGATION OF THE HERNIAL SAC IN RECURRENT PEDIATRIC INGUINAL HERNIAS
1Children's Hospital of Fudan University, 2The Hospital for Sick Children
Background/Purpose: To review our hospital's experience with laparoscopic treatment of recurrent inguinal hernia repairs in children and to assess their outcomes.
Methods: We retrospectively reviewed all children with primary inguinal hernia repairs in our hospital from 2016 to 2017 and analyzed the outcomes of laparoscopic recurrent inguinal hernia repairs.
Results: There were 1703 children who had an inguinal hernia repair: 1549 were laparoscopic (91.0%) and 154 open (9.0%). 35 (2.1%) of these children had recurrent inguinal hernia with no difference in prevalence between laparoscopic and open (P = 0.24). One case was bilateral. Simple patency of the peritoneal vaginal duct was found in all recurrent cases. Laparoscopic ligation of the hernial sac at the internal inguinal ring was performed successfully in all children with recurrent inguinal hernias. There were no intra or post‐operative complications in any of the recurrent cases. No children had inguinal hernia recurrence at follow‐up (8 months – 2 years).
Conclusions: Laparoscopic high ligation of the hernia sac is a simple, effective and safe technique for the treatment of recurrent inguinal hernia in children.
QS037 URGENT THORACOSCOPIC REPAIR OF A SEVERELY PERFORATED SUBCLAVIAN VEIN DUE TO HEMODIALYSIS CATHETER IMPLANTATION CAUSING HEMOTHORAX IN A CHILD
QS038 CONGENITAL CYSTIC LUNG MALFORMATIONS: DOES TIMING OF RESECTION AFFECT SURGICAL OUTCOMES?
Morgan Stanley Children's Hospital Columbia University Medical Center
Background: Optimal timing for resection of congenital cystic lung malformations remains somewhat poorly understood. Historically, a non‐operative approach to asymptomatic patients was recommended, but with no consensus on the frequency, type and length of clinical follow‐up or radiological review. More recently, a best practices review advocated for resection of asymptomatic lung lesions to prevent future infections and cardiopulmonary manifestations. The aim of this study was to define optimal timing for surgical intervention of patients with congenital cystic lung lesions. Furthermore, we sought to define clinical variables that would affect surgical outcomes.
Methods: An IRB‐approved retrospective chart review was conducted for pediatric patients with congenital lung lesions who underwent surgery at our institution. Subjects were divided into cohorts based on timing of operative intervention. Early intervention (EI) was defined as surgery within 4 months of birth; intermediate intervention (IMI) was defined as surgery between 4 to 6 months of age; and late intervention (LI) was defined as surgery after 6 months of age. Clinical characteristics including sex, gestational age, birth weight, cyst volume ratio (CVR) and medical comorbidities were collected and correlated with surgical outcomes including estimated intraoperative blood loss (EBL), surgical time, post‐operative pneumothorax, and hospital length of stay. Groups were compared using Fisher's exact test or Chi‐ squared test for categorical variables; one‐way analysis of variance test was used for continuous variables.
Results: A total of 75 patients with congenital cystic lung malformations were studied. There were no significant differences in sex, gestational age, birth weight, prenatal complications, intensive care unit admissions, or other medical comorbidities. Additionally, there were no significant differences in lesion characteristics, size, lung lobe affected, or pre‐operative weight. Pre‐malignant cellular pathology was identified in 2 patients. Timing of surgery did not significantly affect outcomes. Specifically, there were no differences in operative time, EBL, postoperative pneumothorax, or length of hospital stay among the early, intermediate, and late intervention groups. Furthermore, controlling for CVR did not significantly affect these same post‐operative outcome variables.
Conclusions: Surgical outcomes for resection of congenital cystic pulmonary malformations are not significantly affected by timing of surgery. Further studies are required to determine whether long term outcomes are affected by timing of resection and repair. As we found no significant difference in outcomes between early, intermediate and late intervention groups, we nevertheless advocate for early repair to decrease the incidence of pre‐operative lung infection and to contribute to an extended period of compensatory lung growth.
QS039 RECURRENT TRACHEOESOPHAGEAL FISTULA AND TRACHEAL DIVERTICULUM; TRACHEOSCOPIC ABLATION WITH TCA
1University Hospital Vall d'Hebron España, 2Clinica Los Condes Chile, 3University Hospital Dr Pedro Elizalde Argentina, 4Department of Pediátric surgery, university hospital Arnau de Vilanova
Objective: to report the experience of three centers in the treatment of recurrent tracheoesophageal fistula (RTEF), bronchial‐esophageal fistula (BEF) trachea‐ colonic fistula (TCF) and tracheal diverticulum (TD) by tracheoscopic ablation with trichloroacetic acid. The treatment of these complications usually involve open surgery with high morbidity and mortality. Many minimally invasive techniques have been developed since the past decades by thoracoscopy or bronchoscopy; nevertheless, optimal treatment is still not determined because of the few number of patients, short term of follow‐up, and different procedures.
Materials and methods: from 2009 to 2017, twenty six patients with RTEF, BEF, TCF, and TD were selected for endoscopic management in three centers. Twenty patients had RTEF after prymary repair of EA/TEF by thoracotomy approach and five patiens had another kind of fistula. In all cases the diagnosis was confirmed by clinical evaluation, esophagram and bronchoscopy. Under general anesthesia, a rigid pediatric bronchoscope with a 0° rod lens telescope tele monitoring was used to localize and refresh the fistula with a small endoscopy brush. Cotton soaked with 50% TCA was applied on the fistula for 30 seconds. The procedure has to be repeated three times.
Results: The fistula closed in twenty‐five patients, including the TD. It was confirmed by esophagram or bronchoscopy after 2 months of the procedure. It remains completely obliterated and the patients are asynmptomatic. There was only a patient that also had a cervical fistula as a finding and was operated. The mean number of procedures in each patient was 1.7. Median follow up was 57 months. The postoperative complications were a bacterial pneumonia and bronchospasm.
Conclusion: we considere tracheoscopic ablation of recurrent fistulas and TD with the use of 50% TCA is a minimally invasive, safe and effective technique. It has few complications and avoids the morbidity of open surgery.
QS040 IS STERNAL ROTATION A RELEVANT FACTOR OF CARDIAC COMPRESSION IN PATIENTS WITH PECTUS EXCAVATUM? (PROSPECTIVE STUDY IN 120 PATIENTS)
1Fundacion Hospitalaria, 2Diagnostico Maipu
Objective: The relationship between Sternal Rotation (SR) and cardiac compression (CC) has never been described in detail. We aim to determine if SR is related to CC in patients diagnosed with Pectus Excavatum (PE).
Materials and methods: Prospective study including 120 consecutive patients with PE. All patients were assessed with Chest Computed Tomography (CCT) and Cardiac MRI (CMRI). SR angle (SRA) and orientation (SRO) were evaluated in the axial plane of CCT while CC was assessed with CMRI in the horizontal long axis plane.
Results: A total of 120 patients were included, 85.8% were male and the mean age was 19.7 ± 6.5 years. CCT assessment revealed that the most frequent side of SR was to the right observed in 61 (50,8%), followed by left side in 37 patients (30,8%). CMRI analysis denoted that a total of 100 patients (83,3%) presented cardiac compression. Detailed evaluation of CC revealed that left side SRO was related to compression of the free wall of the right ventricle, in addition patients with right side SRO also presented atrioventricular (AV) groove compression (p = 0,005). The analyses of the SRA revealed that, at higher angles (17,9° −26,7°) greater CC towards the AV groove were observed (p = 0,001).
A: Right side SRO presents compression of the free wall of the right ventricle (RV) and the AV groove.
B: Left side SRO is related to a punctual compression of the free wall of the RV
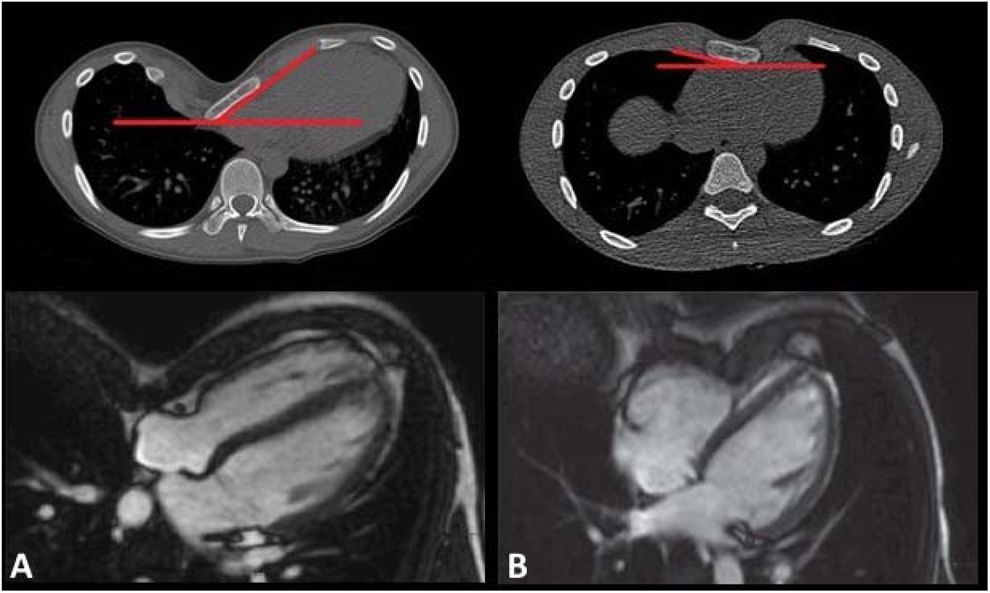
Conclusion: SRA and SRO are related not only to an asymmetric or complex malformation but also to cardiac compression morphology and severity in patients with Pectus Excavatum. We concluded that sternal rotation is a relevant factor of cardiac compression in these patients.
QS041 COMPARATIVE ASSESSMENT OF UPJO PATIENTS UNDERGOING OPEN AND LAPAROSCOPIC PYELOPLASTY USING RENAL DRAINAGE INDEX: A NEW QUANTITATIVE ASSESSMENT TOOL
PGIMER
Aim: outcome of UPJO after pyeloplasty is measured on various parameters. We present a unified assessment scheme for evaluating outcomes of UPJO. This eliminates heterogeneity in assessment.
Patients & Methods: Patients diagnosed with UPJO were evaluated retrospectively and divided into 2 groups. Group A for Open pyeloplasty and Group B for Laparoscopic pyeloplasty. Pre‐op evaluation with IVP and diuretic renal scan was done. Three key parameters on Drainage on EC, Percentage Function on EC, IVP appearance were given a score ranging from 1‐3,1‐4 and 3‐6 respectively. The findings in contralateral normal kidney was also scored and taken as control. After pyeloplasty score was calculated at 6 months. A two‐way evaluation was done with intra group and inter group comparison of scores was done.
Results: Sixty one patients were studied. NA = 30 & NB = 31. Mean age was 2.74 yrs. Mean RDI score for A & B in pre‐op was 8.5 & 8.6 and for post op 11 & 10.55 respectively proving significant improvement. RDI score were significantly higher within the group and across the group.
Conclusion: quantitative scoring of renal improvement after surgical intervention is made easy with the use of the proposed scoring system. There was significant improvement in the RDI of operated kidney in the 2 groups and the improvement in laparoscopic group was comparable to the open group.
QS042 THORACOSCOPY IN CHILDREN FROM “STATE OF THE ART” TO STANDARD OF CARE
Hospital Infantil Privado
Introduction: The first report in children was published by Rodgers and Tlbert in 1976, they performed pulmonary biopsies to diagnose pulmonary lesions and regional decortications. Nevertheless, the real application of this technique was not until 1990 with reports of isolated cases. Nowadays, almost every case of pediatric thoracic pathology can be treated by minimally invasive approaches in an efficient and secure way, avoiding the morbility associated with the open chest/thorax approaches.
The aim of this work is to show the development in the application of thoracoscopy, from the simpler procedures occasionally practiced to the more complex ones performed routinely.
Methods: A retrospective and descriptive study. Patients operated by thoracoscopy in the period from January 1, 2000 to July 31, 2018 were included. They were divided in two groups: the first one from 2000 to 2009 and the second from 2010 to 2018. According to the type of operation, they were arranged in diagnostics and therapeutic procedures. The age, weight, diagnosis, complications, conversions and surgical times of each group were analyzed.
Results: During the period evaluated, 262 thoracoscopies were performed in 261 children. Group I consisted of 75 patients and group 2 of 186 patients. The average age of group was 9.2 years for Group 1 and 2.7 years for Group 2. The diagnostic procedures for both groups were pulmonary and mediastinal biopsies. The frequency was 26.66% for Group 1 and was 8.07% for Group 2. The therapeutic procedures were debridement of empyema, sympathectomy, diaphragmatic plasty, esophageal plasty, aortopexy, thoracic duct ligation, pericardial window, pulmonary lobectomy, resection of esophageal duplication, Nuss surgery and closure of bronchial fistula. In group I it represented 73.33% of surgeries and in group 2 91.93% of patients. The average surgical time in group I was of 122.30 min and in group 2 of 95.62 min. Empyema drainage was performed in 43.63% of group 1 and in 36.8% of the second group. Complex surgery (lobectomy, diaphragmatic plasty and esophageal plasty) in 14 patients of group 1 and 41 of group 2. The patients with pleural fistula required a second operation. The frequency of conversion in group 1 was of 9.3% and in group 2 of 2.2%, in both groups in patients with diaphragmatic plasty, lobectomy or esophageal atresia. In group I, an average of 8.3 thoracoscopies per year were performed and 20.66 in group 2. No complications, no mortality attributable to the procedure.
Discussion: The treatment of pediatric thoracic disease by minimal invasion has evolved from being performed sporadically, (mainly for diagnostic purposes) to being performed daily for more complex procedures each time in smaller patients. This allows the solution of complex pediatric pathologies together with the advantages already known of these approaches. This development has been possible thanks to advances in pediatric anesthesia, endo‐surgical equipment, pulmonary retraction techniques and the development of dissection and suture skills in small spaces. Altogether, these advances have made the thoracoscopic approach to be currently considered the first choice in pediatric thoracic pathology.
QS043 A SINGLE CENTER'S EARLY EXPERIENCE WITH DYNAMIC COMPRESSION BRACING FOR PECTUS CARINATUM
1Texas Children's Hospital, 2Baylor College of Medicine
Background: Dynamic compression braces have an innovative pressure measuring system with adjustment devices that are able to estimate treatment duration, adjust treatment pressures, and increase compliance for correction of pectus carinatum. We initiated the use of dynamic compression bracing in October 2016. The objective of this study was to review our experience with dynamic compression bracing for the treatment of pectus carinatum.
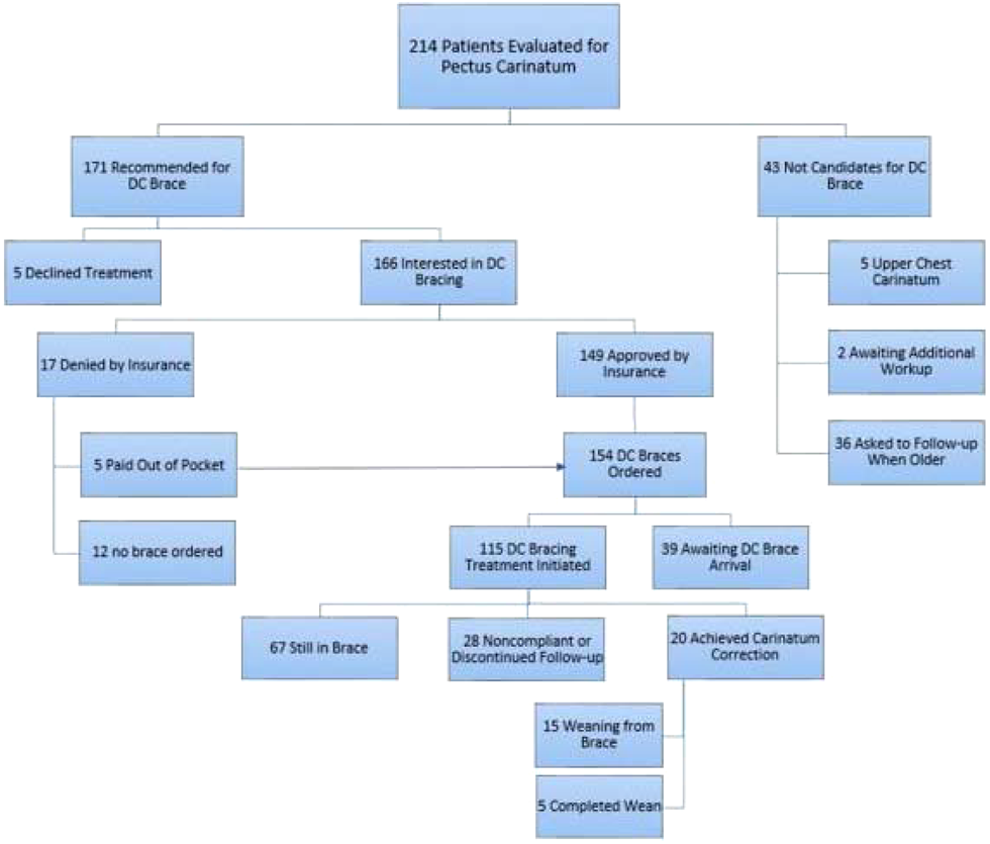
Methods: A retrospective study was performed of all children with pectus carinatum from October 2016 to August 2018 at a tertiary‐care children's hospital. Data collected included demographics, insurance type, presenting symptoms, carinatum height, location and pressure of correction, physical and subjective complaints while wearing the brace, mechanical issues with the brace and median duration of treatment.
Results: A total of 214 patients presented for evaluation of pectus carinatum during the study period. Dynamic compression bracing was not offered to 43 patients due to being too young (N = 36), having an upper chest carinatum that was too high for bracing (N = 5), or needing further workup (N = 2). The remaining 171 patients were recommended for dynamic compression bracing; however, 5 patients (3%) declined treatment. Of the 166 patients interested in bracing 17 patients (10%) were denied insurance coverage, and 5 of these patients proceeded to pay out of pocket for bracing. This resulted in 154 total patients proceeding with dynamic compression bracing. Currently 39 patients are awaiting brace fitting, while the remaining 115 have begun treatment with the dynamic compression brace.
The median age at the time of the initial brace fitting was 14 years and 85% of patients were male. The median carinatum elevation was 2.5cm with a median pressure of correction of 4.2psi. 52% of carinatums were located on the right side of the chest, 24% on the left, 20% on the center, and 4% had an overlapping location. The most common presenting complaint was disliking the physical appearance of their chest (44%). Other complaints included a combination of chest pain, exercise intolerance, and shortness of breath. During treatment with the brace, 15 patients (13%) complained of complications including back pain, arm numbness or skin breakdown. Nine patients (8%) had mechanical problems with the brace which included a lost strap, broken hinge or stripped screws. Thus far, 20 patients have achieved complete chest correction with a mean duration of treatment of 5 months. Five of these patients have also completed their additional 3 month brace weaning period. A total of 28 patients were noncompliant with the brace or discontinued follow‐up (missing >2 months of adjustments).
Conclusion: Dynamic compression bracing is an innovative and effective way to treat pectus carinatum with minimal complications. Patients who are compliant with the bracing have excellent outcomes and a short duration of treatment.
QS044 LAPAROSCOPIC TREATMENT OF INTESTINAL MALROTATION IN CHILDREN: EXPERIENCE WITH 30 PATIENTS
1ho chi minh city Children hospital Number 2, 2University of Medicine and Pharmacy, Ho Chi Minh City,
Objective: The aim of this study was to examine the feasibility, safety, and short‐term outcome of laparoscopic treatment of intestinal malrotation in children.
Method: A retrospective analysis of all patients undergoing laparoscopic treatment of intestinal malrotation from February 2015 to January 2018 was performed.
Results: Thirty patients underwent the laparoscopic treatment of intestinal malrotation. Twenty‐one patients were operated within the first month of life. The average total operative time was 74 minutes. The rate of conversion to open was 6.7%. The median number of days to achieving full feeds was 5 days. The average length of postoperative hospitalization was 12 days. Median follow‐up was 15 months. The rate of recurrence was 3.8%, adhesive bowel obstruction was 7.7%.
Conclusions: Laparoscopic Ladd's procedure in children can be safely and successfully performed with good short‐term outcome.
QS045 THORACOSCOPIC INTERCOSTAL TO PHRENIC NERVE TRANSPOSITION TO ACHIEVE VENTILATOR INDEPENDENCE IN CHILDREN WITH DIAPHRAGMATIC PARALYSIS
1St. Christopher's Hospital for Children, 2Shriner's Hospital for Children
Introduction: Patients with diaphragmatic paralysis face a number of challenges, one of the foremost being ventilator dependence. The associated mortality and morbidity is high in these cases due to respiratory complications which require persistent vigilance to avoid. Treatment that results in successful weaning from the ventilator is known to result in improvement in quality of life. In lower motor neuron injuries, however, direct pacing is not possible because the phrenic nerve distal to the injury has undergone Wallerian degeneration and has lost the ability to conduct an electrical signal. Instead, viable axons from a nerve with intact lower motor neurons need to be transferred to the phrenic nerve to restore the phrenic nerve's conductive properties. We describe a series of patients that underwent novel use of thoracoscopic intercostal to phrenic nerve transfer with concomitant phrenic nerve pacing for reanimation of the diaphragm.
Methods: A retrospective review was conducted of all patients who underwent thoracoscopic intercostal to phrenic nerve transposition. Preoperative testing was performed to confirm the presence of a lower motor neuron injury leading to phrenic nerve dysfunction by using nerve conduction studies and electromyography in conjunction with ultrasound to monitor contractions of the diaphragm. Surgical repair was performed while in the lateral decubitus position with placement of four 5 mm trocars in the intercostal spaces. The phrenic nerve was dissected off the pericardium and the 10th intercostal nerve off the chest wall after nerve stimulator testing found physiologic response to stimulation. The intercostal nerve and attached electrode were then transferred to the left phrenic nerve and coaptation was secured with sealant. Chart review was conducted for hospital course, patient demographics and outcome.
Results: Three patients were identified in which thoracoscopic intercostal to phrenic nerve transfer was performed. The mean age was 4.8 years (range 3.5–7) and there were 2 females. Follow‐up ranged from 6 months – 6 years, with a mean of 2.5 years. Etiology of diaphragmatic paralysis was due to traumatic paraplegia (2) and acute flaccid myelitis (AFM) (1). Due to the nature of the injury, the AFM patient did not require pacing and had spontaneous reanimation of the diaphragm by 6 months post‐operative. Both traumatic patients did have pacing initiated at follow‐up appointments and then were slowly weaned off of the ventilator as tolerating. Currently, 1 patient has been completely weaned off of the ventilator and the other is still weaning as tolerated.

Conclusion: This novel approach of thoracoscopic nerve mobilization and phrenic to intercostal nerve transposition to be both safe and effective for restoring innervation of the diaphragm. This minimally invasive technique decreases the morbidity in comparison to an open thoracotomy approach, and we recommend this as the preferred approach to reanimate the diaphragm.
QS046 FACILITATING PULMONARY LOBECTOMY IN CHILDREN WITH CONGENITAL CYSTIC LUNG DISEASE. ADVANTAGES OF AN EXTRA TROCAR IN THE LOWER THORAX
Department of Pediatric Surgey, Juntendo University School of Medicine
Purpose: To describe how an additional trocar enhances the safety and efficiency of thoracoscopic pulmonary lobectomy (TPL) in children with congenital cystic lung disease.
Methods: The additional trocar (AT) was inserted in the10th intercostal space (IS) in the posterior axillary line after trocars were placed conventionally in the 6th, 4th, and 8th IS in the anterior axillary line, for a 5mm 30o scope, and the surgeon's left and right hands, respectively for a lower lobe TPL (LTPL) and in the 5th, 3rd, and 7th IS for an upper TPL (UTPL), with the AT in the 9th IS. Switching between trocars (8th ↔6th for the scope, 6th ↔4th for left‐hand instruments, and 10th ↔8th for right‐hand instruments during an LTPL and 7th ↔5th, 5th ↔3rd, and 9th ↔7th during an UTPL, respectively) adds another dimension by allowing vital structures such as the pulmonary veins, bronchi, and feeding artery(s) to be viewed posteriorly. Blood loss, operative time, duration of chest tube insertion, post‐operative analgesia, intra‐/post‐operative complications were compared between TPL+AT (n = 28) and TPL‐AT (n = 27).
Results: AT greatly facilitated dissection of the posterior aspect of the pulmonary vein and bronchus. In TPL+AT, mean intraoperative blood loss (5.5 vs. 10.4 mL), operative time (3.9 vs. 5.4 hours), and chest tube insertion (2.0 vs. 3.3 days) were all significantly decreased (p < .05, respectively). In TPL‐AT, 1 case required conversion to mini‐thoracotomy for bronchial artery bleeding. Differences in complications and post‐operative analgesia were not significant.
Conclusions: An additional trocar significantly improved the safety of TPL in children with congenital cystic lung disease.
QS047 A PATENTED INTRALUMINAL FIXATION MECHANISM TO DELIVER MEHCANOTRASDUCTIVE FORCES TO SMALL BOWEL
1University of MIchigan, 2Case Western Reserve, 3Cleveland Clinic
Short bowel syndrome (SBS) represents a loss of sufficient intestinal length, which compromises absorption of nutrients required to sustain life. SBS predominately affects infants and children, and although patients may be maintained on parenteral nutrition, the associated morbidity and mortality can be devastating. Eighteen years of research and development has culminated in a patented attachment mechanism that is mounted on a flexible catheter device similar to a double balloon enteroscopy concept. A specific configuration has been designed to allow safe application of distractive forces between two attachment points in small bowel in continuity. The challenge lies in creating a system that will not damage the precious and limited intestinal tissue in SBS patients while achieving the mechantransductive forces required to induce cell turn over and tissue growth. The attachments are specially designed to easily slide through intestinal lumen when deflated yet possess the ability to safely grip the mucosal surface when inflated. A mesh coated balloon allows for the appropriate grip strength. When deflated, a series of silastic struts creates a fenestrated decoupling shroud that covers the majority of the balloon's textured mesh surface allowing the device to slide smoothly across the mucosa. When insufflated, the struts are spread by the radial expansion of the balloon and enough of the balloon surface area makes contact with the mucosa to create adequate grip. The decoupling and timed cycling of the device allows for passage of succus without creating intestinal obstruction. The device has been tested in non‐GLP large animals, however, plans are to overcome regulatory hurdles to allow human use in the near future. This could provide an alternative treatment for children with SBS.
QS048 SUTURELESS LAPAROSCOPIC INGUINAL HERNIOPLASTY: STANDARIZED PROSPECTIVE PROTOCOL ANALYSIS
Hospital Exequiel González Cortés
Multiples laparoscopic inguinal hernioplasty techniques have been described for the pediatric population. In Chile 2010 Dr. Jorge Godoy described a simple and minimally invasive surgery for inguinal hernias in girls, called BURNIA (BURN‐HERNIA). In the last decade some case series have been published, demonstrating BURNIA effectiveness; allowing to establish it as a valid technique given its cosmetic advantages and excellent postoperative outcomes. Our aim is to analyse a standarized follow‐up results and to contribute to this technique validation.
Method: Prospective study that included girls who underwent BURNIA during june 2016‐june 2018.
The standarized protocol consist of clinical and ultrasound follow up to 18 months. Demographic, surgical and complication data were collected, as postoperative analgesia, hospital stay and clinical or ultrasound recurrence.
Results: 53 BURNIA hernioplasty were included, 19 bilateral, 8 left and 7 right hernias. Average age was 4 years (range 2 months ‐ 10 years), average weight 16kg (range 1.87 Kg – 60 Kg). Operative time 31 minutes (range 15 to 70 minutes). 85% underwent BURNIA according the original technique (Single incision laparoscopic surgery), 15% an additional access was used. None complication or recurrence was registered. 2 patients with recurrence, who previously have open technique hernioplasty, underwent BURNIA. Only 1 patient with bilateral inguinal hernia required unilateral conversion due to a hernia sac larger than 3cm wide.
Conclusions: Burnia is a surgical alternative that is simple, safe and easy to reproduce that could expand its indication to wider age ranges and management of recurrences to offer them the cosmetic advantages in an effective and safe way.
QS049 THORACOSCOPIC POSTERIOR TRACHEOPEXY IS A FEASIBLE AND EFFECTIVE TREATMENT FOR TRACHEOMALACIA
1University of Colorado, Department of Surgery, 2Children's Hospital Colorado
Background: Posterior tracheomalacia is characterized by collapsibility of the posterior trachea and is often present in patients with congenital esophageal atresia with or without trachea‐esophageal fistula. It can lead to a variety of symptoms from mild expiratory stridor and difficulties clearing secretions to severe respiratory distress, especially in the setting of infectious respiratory illness. Depending on the severity of symptoms, treatment ranges from medical therapy with nebulizers and steroids to surgical treatment in the form of posterior tracheopexy. The purpose of this study is to review our institution's experience with posterior tracheopexy.
Methods: A retrospective review was conducted from 2017‐2018 at a free standing, quaternary care children's hospital. Statistical analysis included descriptive measures (median, range, and proportions).
Results: The current analysis included 6 patients. The median age at surgery was 6 (range 3–8) years and 4/6 (57%) of cohort were male. The majority of patients (5/6, 83%) had a history of prior esophageal atresia and tracheoesophageal fistula repair and 3/5 (60%) had associated VACTERL anomalies. All patients demonstrated severe tracheomalacia on preoperative bronchoscopy with collapse of the posterior membrane. In regard to surgical approach, the most recent cases (4/6, 66%) underwent thoracoscopic repair. The median operative time was 248 (277 thoracoscopic, 218 open) minutes. The median length of stay was 3 days, and 2/6 (33%) of patients had a post‐operative complication of chylothorax (1 thoracoscopic, 1 open), which resolved without invasive intervention. The current median length of follow up is 7.5 months, and all patients reported symptomatic improvement. Only one patient who had symptomatic improvement initially has regressed to baseline symptoms, and follow up bronchoscopy demonstrated tracheomalacia recurrence.
Conclusion: Posterior tracheopexy is a safe and effective treatment option for symptoms associated with tracheomalacia. The thoracoscopic approach is feasible in experienced hands.
QS050 ISOLATED VATS APPROACH FOR THE MANAGEMENT OF CERVICOTHORACIC JUNCTION TUMOR IN CHILDREN
Beijing Children's Hospital, Capital Medical University, National Center for Children's Health
Background: The tumors that located in cervicothoracic junction area were very difficult for achieving complete resection. Previous literature reported that the tumors in this area usually need combined cervical and thoracic surgical approach like “supraclavicular incision‐sternotomy‐anterior thoracotomy.” This study aims to explore the feasibility and safety with isolated VATS approach for the tumor in cervicothoracic junction in children.
Methods: We retrospectively reviewed our patients with tumor of cervicothoracic junction from January 2014 to September 2018. There were 55 patients received isolated VATS approach for removing the tumor located in the cervicothoracic junction area. We reviewed the data on tumor characteristics, completeness of resection, duration of surgery, blood loss, hospital stay, surgical complications and follow‐up.
Results: Of 55 patients treated with this isolated VATS approach and all the surgery were successfully performed with no mortality. The average age was 3.9 years old (range, 4 months–14.4 years), and 28 patients were male, and 27 were female. 35 cases were on the left side, 20 cases on the right. The average tumor size was 5.0 cm in greatest dimension (range, 2.0–16.0cm). 27 cases of ganglioneuroblastoma, 19 cases of neuroblastoma, 5 cases of ganglioneuroma, 2 cases of neurilemmoma, 1 case of lipoblastoma and 1 case of lymphangioma. The average duration of the operation was 93.2 minutes (range, 30–260 minutes). The average blood loss was 6.0ml (1‐50ml). The mean hospital stay was 6.6 days(range, 5–13 days). No severe complication occurred during the surgery.
Conclusion: In several situations, isolated video‐assisted thoracoscopic surgery resection for cervicothoracic junction tumor in children were safe and feasible, and with minimally postoperative complications.
Keys: Mediastinal mass, VATS, children
QS051 OPTIMAL VIEWING DIRECTION OF THE OBLIQUE LAPAROSCOPE IN SINGLE INCISION LAPAROSCOPIC PERCUTANEOUS EXTRAPERITONEAL CLOSURE FOR INGUINAL HERNIA
Department of Pediatric Surgery, Gunma Children's Medical Center
Purpose: It is difficult for young surgeons to perform single incision laparoscopic surgery (SILS) because collisions between the forceps and laparoscope often occur. The oblique laparoscope is usually used for SILS, but manipulation of this laparoscope requires special skills that are difficult to teach verbally. We studied the viewing direction of the oblique laparoscope in single incision laparoscopic percutaneous extraperitoneal closure (SILPEC) for inguinal hernia, and assessed the optimal manipulation to avoid collisions.
Methods: A retrospective chart review was performed on patients who underwent SILPEC at a single children's hospital between April 2016 and April 2017. The viewing direction of the 30‐degree oblique laparoscope was measured by the field stop pointer which is a function of the laparoscope made by Striker Corporation (Figure 1). Three ranges of viewing direction were defined: the Inside viewing direction was from −90 to −11 degrees, Upward viewing direction was from −10 to 10 degrees, and Outside viewing direction was from 11 to 90 degrees. The patients were divided into 3 groups according to the viewing direction at the beginning of the procedure. The percentage of cases in which there was a change in category of viewing direction during the procedure was compared.
Demographic data are expressed as mean ‐ standard deviation, and analyzed using ANOVA or Fisher's exact test.
*statistically significant.
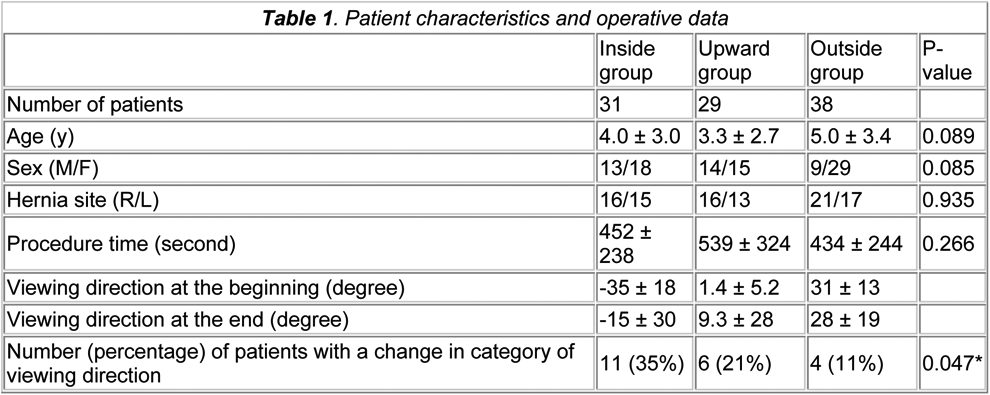

Results: Table 1 shows the patient characteristics, procedure time and viewing direction. The percentage of patients with a change in category of viewing range was significantly lower in the Outside group than in the Inside group.
Conclusions: These results show that setting the initial viewing direction to the outside can reduce correction of the viewing direction during SILPEC. Because the intersection angle between the outside‐viewing‐laparoscope and forceps is close to a right angle, this might reduce collisions.
QS053 5‐YEARS FOLLOW‐UP AFTER 17 LAPAROSCOPIC TRANSHIATAL ESOPHAGECTOMY AND GASTRIC PULL‐UP (TEGPUL)
Fundación LaparoKids, Caracas ‐ Venezuela
Background: Survival in patients with EA has improved due to advances in: neonatal intensive care, anesthesia, mechanical ventilation, nutrition, antibiotic therapy and surgery, among others. However, in Venezuela, there has been a detriment of these factors, which is why morbidity and mortality rebounded due to EA. That is why we created the LaparoKids Foundation and replicated the Spitz technique of open gastric pull‐up laparoscopically. In the present study we show our experience.
Materials and Methods: Between 2011 and 2015 we performed 17 TEGPUL in 8 girls and 9 boys, with a mean age 34 months (range 8‐99 months). All born with EA 65% (11) was acquired long‐gap (EA Type III, those where a primary anastomosis was initially achieved and then lost because of complications and re‐do surgeries) and 35% (6) congenital long‐gap (EA Type I and II). Immediate, mediate and late complications were recorded. They were contacted by email, Facebook, instagram and whatsapp. WHO charts was use for nutritional diagnosis.
Results: Mean operating time 5.5 hours (3.5 ‐ 8 hours), mean days of mechanical ventilation 4.5 (2 ‐ 8 days), mean days of hospitalization 18 (9 ‐ 40 days), mean time of oral feeding 12.5 days (3 ‐ 30 days). We contacted 92% of the living patients. Immediate complications (first 14 post‐operative days): 3 (18%) patients were reoperated (2 acute gastric obstruction and 1 incidental colon perforation); 3 (18%) patients had perioperative cardiac arrest (2 in‐OR and 1 out‐OR) all left but one, with neurological sequelae, died on the 12th postoperative day; 8 patients (47%) had a leak of the esophagogastric anastomosis, all health spontaneously in an average of 15 days and high blood pressure in 10 (59%) patients, unknow etiology. Mediate complications (from 15 post‐operative days to 3 months): gastric emptying delay 3 (18%), GER 5 (29%) and recurrente lower respiratory infections 9 (53%). Late complicacions (from 3 months to 5 years): malnutrition 2 (18%), risk of malnutrition 3 (27%), diaphragmatic hernia 1 (9%). Postoperative parents satisfaction 100%.
Conclusion: TEGPUL is a safe and reproducible esophageal replacement technique in patients with long‐range AE, but have a long learning‐curve. However, more long‐term and larger follow‐up studies are needed, for which we recommend grouping these patients in a national reference center.
QS054 DUODENO‐GASTRIC BILE REFLUX AFTER LAPAROSCOPIC HEPATICO‐DUODENOSTOMY FOR CHOLEDOCHAL CYST: EVIDENCE BASED COHORT STUDY
PGIMER Chandigarh
Background: Duodeno‐Gastric bile reflux (DGBR) after laparoscopic Hepatico‐Duodenostomy (LHD) for Choledochal cyst (CDC) is a concern in literature. There is insufficient data to support that LHD causes problems in early and late follow up.
Aim: To analyze LHD patients operated at our institute for clinically significant DGBR
Patients & Methods: Bidirectional study in clinically proven CDC patients operated by single surgeon. Six months follow up was mandatory. They underwent LHD either laparoscopically or by Robotic surgery. D2 anastomosis was done. Follow up at 3 months was done by clinical and biochemical evaluation, HIDA scan and Endoscopy for antral biopsy and gastric juice aspirate for bile pigments.
Results: Mean age of 56 patients (66.1% females) was 5.19 ± 3.2mths. Mean follow up duration was 22.17 ± 2.16 months. On HIDA scan 66% patient showed no evidence of DGBR. Antral biopsy showed mild gastritis in 85.1% patients. Bile was seen in antrum in 80.90% patients. Gastric aspirate showed absence of bile pigments in 68% patients. 19% patients had evidence of DGBR on all 4 parameters of evaluation. Only 4% of patients were clinically symptomatic.
Conclusion 19% of patients have DGBR with LHD. They have very mild symptoms and can be easily managed conservatively.
QS055 PERITONEAL ASPIRATION WITH DRAINAGE VS. PERITONEAL LAVAGE WITH DRAINAGE DURING LAPAROSCOPIC APPENDECTOMY IN CHILDREN WITH PERFORATED APPENDICITIS
QS056 LAPAROSCOPIC COMPLETE EXCISION OF BENIGN OVARIAN TERATOMA WITH OVARIAN TISSUE PRESERVATION IN CHILDREN: CASE SERIES
1Section of Pediatric Surgery, Faculty of Medicine, Tanta University, Egypt, 2Section of Surgical Oncology, Surgery Department, Faculty of Medicine, Tanta University, Egypt, 3Section of Pediatric Surgery, Faculty of Medicine, Alexandria University, Egypt
Introduction: Although teratomas are the most common histologic subtype of childhood ovarian germ cell tumors, their appropriate treatment in this age group still remains unclear. Paucity of research dedicated exclusively to both mature and immature teratomas of the ovary, contribute to decision making difficulties.
Aim: To present our experience of complete excision of a benign ovarian teratoma in children. In addition, combine the benefits of laparoscopy with ovary preservation in children.
Patients and Methods: The medical records of elven patients along 6 years (mean age of 5.6 years with range of 1–14 years) who had undergone laparoscopic ovary‐sparing surgery for teratoma were analyzed retrospectively. Mean duration for follow‐up was 26.5 months with range of 6–50 months.
Results: Five patients suffered from chronic abdominal pain; two had acute colicky abdominal pain. In four patients, there was no presenting clinical symptom. One patient was operated on emergency basis due to symptoms related with acute abdomen. On the other hand, ten were operated electively. Ultrasonography was performed in all patients. Additionally, CT or/and MRI were performed in all except one. Main radiologic findings consisted of heterogenous cystic and solid ovarian masses predictive of teratoma. The definitive diagnosis in emergency cases were as follows: torsion of the ovarian mass with teratoma [1]. The final diagnosis in electively treated 10 patients were: unilateral ovarian teratoma [9] and bilateral ovarian teratoma [1]. The operations were performed by laparoscopy in all with one conversion. The procedures were ovary‐sparing surgery in 10 ovaries and detorsion of ovary in 1 patient. The main indication for ovary‐sparing surgery was the “existence of a perfect dissection plane between the tumor margins and healthy ovarian tissue”. The remaining ovarian tissue was evaluated macroscopically for residual lesions. The pathologic diagnosis was: mature cystic teratoma in 10 and necrotic cyst in 1 case. The postoperative outcome and follow‐up was uneventful.
Conclusion: Heterogenous ovary mass containing solid and cystic portions with echogenic areas on ultrasound imaging is highly suggestive of ovarian teratomas. Based on imaging modalities findings, ovary‐sparing surgery can be safely performed laparoscopically if the preoperative diagnosis is teratoma and there is always a plane of dissection between the normal ovary and cyst wall. Magnification of laparoscope with energy devices are excellent tools in complete excision with ovarian tissue preservation.
QS057 INCIDENTAL FINDINGS OF GYNECOLOGICAL ANOMALIES DURING LAPAROSCOPIC PROCEDURES
1Department of Pediatric Surgery, Hospital de Braga, Braga, Portugal; Life and Health Sciences Research Institute (ICVS), School of Medicine, University of Minho, Braga, Portugal; ICVS/3B's – PT; Government Associate Laboratory, Braga/Guimarães, Portugal., 2Department of Pediatric Surgery, Hospital de Braga, Braga, Portugal
Background: Laparoscopy is becoming the standard of care for most abdominal and pelvic pediatric surgeries. Besides the known advantages, minimally invasive surgery enables better visualization of the whole abdominal cavity regardless of the surgical site. There are several reports of incidental findings during elective procedures in adult and pediatric patients, namely for gynecological anomalies. Our aim was to characterize gynecological incidental findings in female children at our department in order to propose a standardized inspection during elective and emergent procedures.
Materials and Methods: We reviewed all elective and emergent laparoscopic procedures performed at our department in 2016‐17 in females. All cases where visualization of the pelvis was possible were included, namely exploratory laparoscopy, appendectomy, cholecystectomy, inguinal hernia repair, pyeloplasty, ureteric reimplantation, nefro‐ureterectomy, adrenalectomy, colo‐anal pull‐through and colon resection. Incidental findings regarding the reproductive system were assessed. We collected data regarding age of the patient, type of surgery, intraoperative findings and definitive diagnosis.
Results: From january 2016 to december 2017, 98 female children underwent laparoscopy at our department. Four had incidental findings of gynecological anomalies. We present in the table our detailed results.
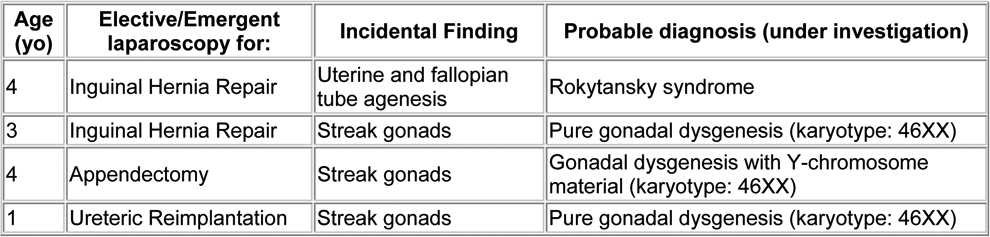
Conclusions: Routine pelvic inspection should be implemented during all laparoscopic procedures in females once a significant number of gynecological anomalies could be identified as occurred in our series.
QS058 DISTAL URETER PRESERVATION FOR CLEAN INTERMITTENT CATHETERIZATION DURING LAPAROSCOPIC NEPHRECTOMY
“Queen Fabiola” University Children's Hospital Université Libre de Bruxelles (ULB)
Aim: Mitrofanoff principle of bladder intermittent catheterization improved renal outcome and quality of life in many patients. We present our experience with continent catheterisable conduit created from distal ureter after nephrectomy.
Case 1: Boy aged 2 years, born with posterior urethral valves and bilateral reflux (grade V right and IV left) presented several episodes of UTI and urine retention. The cystography showed a massively right refluxing kidney that appeared barely functioning (<10%) on isotopic scan. A right nephrectomy was proposed and clean intermittent catheterization (CIC). Unfortunately, CIC by urethra failed due to absent child compliance. Laparoscopic right nephrectomy was performed and the distal ureter preserved. The distal ureter was exteriorized by the port orifice in the right iliac fossa and a modelage according to the Kalicinski technique performed. The distal ureter was then reimplanted laparoscopically according to Lich‐Gregoire and externalized through the umbilicus as a continent easy to catheterize stoma. Two years follow up: there is no leakage, no stenosis and a very good cosmetic result. CIC is performed smoothly and the left reflux nearly disappeared.
Case 2: Girl aged 4 years with a neurogenic bladder secondary to a myelomeningocele was referred to our department. At the age of one year, a Cohen procedure was performed for a right uretero‐vesical reflux. The evolution was marked by persistent UTIs despite CIC, a non‐functioning right kidney and progressive renal function deterioration Laparoscopic right nephrectomy was performed with distal ureter conservation. The latter was sectioned at the level of the iliac vessels crossing and brought out to the right iliac fossa trocar site in a way to obtain a continent catheterisable conduit. One year follow‐up shows easy CIC without any complication.
Conclusions: The distal ureter presents an ideal anatomical structure for catheterisable channels. Uretero‐vesical junction preservation offers continence (with or without reimplantation) with a minimal conduit blood supply risk. Furthermore, the ureter as a conduit offers a predictable behavior in terms of long term contact with urine.
QS059 LAPAROSCOPIC ADHESIOLYSIS FOR SMALL BOWEL OBSTRUCTION: THE LARGEST UK SINGLE‐CENTRE SERIES
Great Ormond Street Hospital for Children
Aim: Laparoscopy for adhesiolysis in the management of small bowel obstruction has shown to be feasible and is being increasingly utilised, with varying rates of success. In this study we aim to describe our experience of laparoscopic adhesiolysis for small bowel obstruction.
Methods: A five‐year retrospective casenote review was performed, of all children aged 18 years and below, undergoing laparoscopic adhesiolysis for small bowel obstruction between August 2013 ‐ August 2018 at our specialised neonatal and paediatric surgical centre. Institutional audit approval was gained. Data collected included demographics, previous surgeries, operative details, conversion to laparotomy and complications, including recurrence of obstruction.
Results: A total of 32 patients were identified in our study that underwent 35 initial laparoscopic operations for adhesive bowel obstruction (male = 21, mean age = 7.9 years, range = 2 months‐18 years) with a mean follow‐up of 13 months (range = 1‐47 months). All patients had presented with their first episode of adhesional bowel obstruction. 30/32 patients had a history of previous abdominal surgery, with approximately one third of our patients having had an appendicectomy (see Table 1). Median time to presentation was 145 days (range = 4 days ‐ 13.5 years). 19/35 (54%) operations were successfully completed laparoscopically, with the remaining requiring conversion to laparotomy. Reasons for conversion included: presence of ischaemic bowel (5/16), limited working space or vision (4/16), failure to release adhesions (3/16), repair of serosal tears (2/16), unknown (1/16) and 1 patient required conversion to open due to iatrogenic enterotomy. 4/32 (13%) patients had a recurrence of adhesional bowel obstruction requiring surgical management. Three of these patients had had an initial laparoscopic adhesiolysis, with the other requiring conversion to open. There were no mortalities.
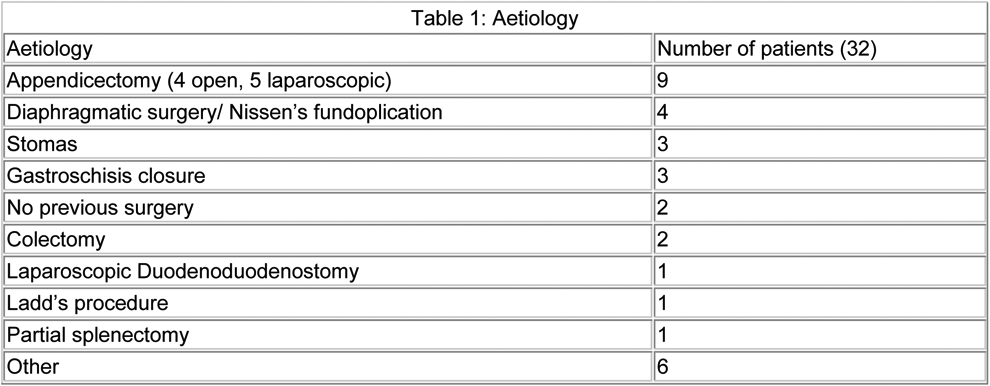
Conclusion: We present one of the largest single‐centre studies on paediatric laparoscopic adhesiolysis for small bowel obstruction. More than 50% of our patients were successfully managed laparoscopically Laparoscopic adhesiolysis can be successfully and safely utilised in the paediatric population.
QS060 A SIMPLE AND EFFECTIVE LAPAROSCOPIC TECHNIQUE FOR ANTEGRADE ENEMAS
Medical College of Wisconsin
Introduction: Constipation is a frequent problem in children and many patients require enemas for bowel management. Surgical interventions to access the colon and facilitate antegrade colonic washouts are frequently performed. We describe a surgical approach that simplifies other well‐established techniques for antegrade enemas.
Methods: We performed a single‐institution retrospective review of patients that underwent a standardized technique of laparoscopic appendicocecostomy. Patients that had another procedure during same event were excluded. The technique consists of identifying the appendix laparoscopically, dissecting its mesentery, and extracting it through a right lower quadrant incision. The appendix is then near‐completely transected, the mucosa is exposed and sutured to the dermis such that the mucosa is buried beneath the level of the skin. The stoma is accessed with a button appliance for administration of antegrade enemas.
Results: A total of 92 laparoscopic appendicocecostomy procedures that fulfilled criteria have been performed at our institution from 2008 to 2018. Seven patients were excluded due to sigmoidectomy or other interventions during the same OR event. Patients had a mean age of 9.1 years (SD 3.8, range 3–18 years) and the mean postoperative length of stay was 1.7 days (SD 1.8, median 1, IQR 1‐2). Mean operative time was 61 minutes (SD 21). No intraoperative complications were seen and 12 patients (14%) required a return to the OR, mainly for tube exchange and cauterization of granulation tissue.
Conclusions: Laparoscopic appendicocecostomy is a safe and relatively quick procedure that simplifies other techniques to establish access for antegrade enemas. A long‐standing tube may increase compliance while decreasing leakage and avoiding stenosis of the tract. An ongoing review of our experience will yield more granular data that will inform surgeons about the benefits of the present approach.
QS061 COMPARISON OF THREE‐DIMENSIONAL AND TWO‐DIMENSIONAL LAPAROSCOPY IN THE PEDIATRIC NISSEN FUNDOPLICATION
Saitama Children's Medical Center
Aim: Three‐dimensional (3D) vision in laparoscopy facilitates improved depth perception and more precise recognition of anatomical structures, thus making it easier to perform complex procedures in narrow spaces. The advantages of 3D vision compared to two‐dimensional (2D) vision in laparoscopy include shorter operative times and a reduction in technical errors. However, implementation of 3D laparoscopy has not been widespread, and clinical research on the usefulness of 3D vision in pediatric laparoscopic surgery remains scarce. The aim of this study was to evaluate the usefulness of 3D vision compared to conventional 2D vision in pediatric laparoscopic Nissen fundoplication procedures.
Methods: Our hospital introduced 3D laparoscopy in January 2017. The medical records of patients 18 years old or younger who underwent laparoscopic Nissen fundoplication at a single institution between January 2015 and August 2018 were retrospectively reviewed. Videos of each procedure were also reviewed. The total pneumoperitoneum and wrapping times (duration of wrapping from insertion of the first suture to cut of the last suture) were measured. A questionnaire was provided to each surgeon that performed the 3D procedure.
Results: Twenty‐seven and 19 patients underwent laparoscopic Nissen fundoplication with the surgeons operating under 2D and 3D vision, respectively. The median (range) age and weight at the time of surgery in the 2D group and the 3D group were 31 months (5–212 months) vs. 29 months (3–170 months) and 9.9 kg (4.6–45.1 kg) vs. 9.3 kg (3.8–22.9 kg), respectively. There were no significant differences in either parameter. The median (range) pneumoperitoneum and wrapping times in the 2D and 3D groups were 190 min (120–362 min) vs. 192.5 min (130–335 min) and 1411 sec (936–2217 sec) vs. 1455 sec (960–2132 sec), respectively. There were no significant differences between the two procedures with regard to these parameters either. On the questionnaires, all 8 surgeons acknowledged the merits of 3D laparoscope, but they hoped to see a decrease in the size (diameter) of the scope and the visual field range (in the current system, only two directions, looking upward and downward, are available). Four surgeons (50%) experienced eyestrain and one experienced double‐vision. Six surgeons' (75%) responses indicated that they preferred 2D to 3D vision.
Conclusions: This study showed that there was no reduction in surgical time with the use of 3D scope compared to that with the 2D scope. Decreasing the size of the scope diameter and adding functions, such as multidirectional visions, are needed for the 3D scope to gain more widespread approval and use in pediatric surgery.
QS062 LAPAROSCOPIC INGUINAL HERNIA REPAIR RECURRENCE AT A LARGE TERTIARY CARE CENTER
Texas Children's Hospital
Purpose: Laparoscopic inguinal hernia repair in children is increasingly gaining acceptance among pediatric surgeons. However, there continues to be variation in technique and experience with the procedure. The objective of this study was to identify the rate of inguinal hernia recurrence for surgeons of mixed experience with laparoscopic inguinal hernia repair at a tertiary‐care academic children's hospital.
Methods: A retrospective review of children ages 0‐18 years who underwent outpatient laparoscopic inguinal hernia repair between January 2015 and December 2017 was performed. Patients were identified by CPT code, and those that had a prior inguinal hernia repair were excluded. Data collected through chart review included demographics, operative details, and complications. In addition, a telephone survey was performed to identify prolonged post‐operative symptoms, inguinal hernia recurrence, and additional inguinal surgeries. Descriptive statistics were performed and are expressed as median and interquartile range.
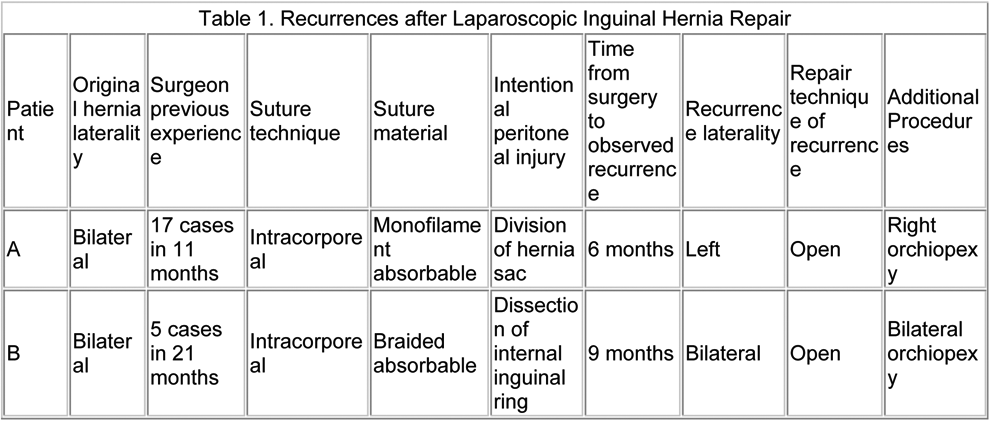
Results: Of the 206 children identified, 71% were male, the median age was 4 [1‐8] years, weight was 17.1 [10.5‐27.0] kg, and BMI was 16.6 [15.4‐18.3]. All cases were performed by twelve surgeons with a median case load of 8 [2‐28] patients during the study period. Hernias were most commonly identified on the right (40%) with 37% being bilateral. Operative technique varied with 82% of cases undergoing extracorporeal suturing and 67% having intentional injury of the peritoneal surface at the internal ring. The most common type of suture used was non‐absorbable braided (82%) followed by absorbable braided (16%) and absorbable monofilament (2%). Follow‐up telephone surveys were attempted for all patients with a response rate of 44% (n = 90). Of the non‐responders, 106 (51%) could not be reached, 8 (4%) did not have a working number, and 2 (1%) declined to participate. The recurrence rate after laparoscopic inguinal hernia repair was 1% (n = 2) based on chart review and completed telephone surveys (Table 1). Two additional postoperative complications were identified. One patient had a stitch abscess and the other required subsequent orchiopexy. The median time from operation to study follow‐up was 18 [13–24] months.
Conclusion: Laparoscopic inguinal hernia repair in children has a low recurrence rate even amongst surgeons with varied experience using different techniques at a single institution.
QS063 REDO LAPAROSCOPIC FUNDOPLICATION IN PEDIATRICS IN 10 YEARS‐ A SINGLE CENTER STUDY IN CHINA
Pediatric surgery department, Capital institute of pediatrics
Background: Hiatal hernia is a common cause of vomiting in pediatrics, which is surgically correctable. Though the laparoscopic technique for this disease is becoming a popular option, the safety and efficacy of redo laparoscopic correction of hiatal hernia is seldom investigated.
Objective: In this study, we assess the feasibility and safety of redo laparoscopic fundoplication for paediatrics from single center for last ten years.
Methods: 14 patients (aged 6 monthto 8 years) between Jan 2008 and Jun 2018, presenting with vomiting or dysphagia after primary fundoplication (either open or minimal invasive surgery) were treated with redo laparoscopic fundoplication. Indication for redo‐operation were the severity of symptom and results of upper gastrointestinal (GI) radiography. Follow‐up evaluation was conducted by GI radiography and questionnaire.
Results: 9 out of 14 patients were done with open fundoplication for the primary operation. Among all the redo laparoscopic cases, one case was converted to open procedure due to severe adhesion and blood loss. Mean recurrent time from primary operation was 8.5 month (range 0.33–30). Mean operating time was 180 minutes (range, 80–300). All patients were discharged from surgery unit and returned to their regular physical activity within mean 6 days after surgery. Upon clinical follow up at 3 months to 10 years, 5 out of 14 (36%) patients present vomiting or dysphagia, and only 3 of them showed evidence of oesophageal stenosis upon upper GI radiography, however none of above cases needed re‐operation.
Conclusions: Redo laparoscopic fundoplicationis feasible and effective in pediatrics. This technique is suitable for cases even though the primary operation is under open procedure. However, sufficient laparoscopic skills are required to master this technique.
QS064 UPPER ENDOSCOPY AND COLONOSCOPY FOR EVALUATION OF HOST VS GRAFT DISEASE AFTER HAEMATOPOIETIC STEM CELL TRANSPLANTATION. EXPERIENCE IN A PEDIATRIC HOSPITAL
Universidad Nacional de Colombia
Haematopoietic stem cell transplantation is a therapeutic option in life threatening diseases in children, gaining more indication during the past decade. It has been estimated that 20% to 50% of patients can develop host vs graft disease (GvHD) as complication, being gastrointestinal (GI) tract one of the most frequent places of presentation. Histologic confirmation and severity are primordial in the adjustment of management, but literature is scare in children regarding interventions for the diagnosis of gastrointestinal compromise.
Materials and methods: Clinical charts of all patients that were taken to upper endoscopy or colonoscopy after bone marrow transplant were reviewed in a single pediatric institution, since January 2015 to December 2016. Pathology and outcome were evaluated as well.
Results: There were 55 procedures in 29 patients. Of those 29 corresponded to upper endoscopy and 26 colonoscopy. GI GvHD was the indication for 27 patient taken for the procedures, and in the other 2 were upper GI bleeding. During upper endoscopy gastric biopsy were positive for GvHD in 11 patients, of 16 esophageal biopsies, 3 were positive and there were only 6 duodenal biopsies of witch 4 were positive for GvHD. Of the 26 colonoscopies, 16 patients were positive, with rectal biopsies only. There were evidence of higher severity of GvHD in rectal biopsies compared with de upper gastrointestinal biopsies. Regarding follow up, mortality was present in 14 patients, being 3 related to severe GI GvHD. 15 patients were controlled until 2018, of which 11 are free of disease and 4 had relapse.
Conclusions: GI GvHD is a common complication after stem cell transplantation in children, that need pathology confirmation for therapy directions. In the present study only 40–60% of clinical suspected GI compromise were confirmed by histology, being rectal biopsy the more reliable, in concordance with the literature reported in adults. Additionally this patients frequently have severe thrombocytopenia and neutropenia that limit the extension of procedures. For example it is not our routine practice to take duodenal biopsies, due to the risk of duodenal hematomas in severe thrombocitpenic patients, that may be in conflict with some recommendations in other papers. Regarding colonoscopy, only rectal biopsies are taken and no preparation or extension above de sigmoid colon are performed, with low risk of related complication and the best histologic accuracy. There is need for more studies in children that can unify the best procedure recommendations and places for histologic confirmation, with the lowest risk for patients.
QS065 LAPAROSCOPIC RECTOPEXY IN A 2 MONTH OLD BOY WITH MASSIVE RECTAL PROLAPSE
Department of Pediatric Surgery University Hospital Erlangen
Introduction: Rectal prolapse frequently occurs in childhood and adolescence and usually responds well to conservative treatment, whereas in the literature nothing has been researched about the rare, resistant cases in infants.
Presentation of Case: We present the case of a 10 week old boy weighing 2700 grams. Pre‐existing conditions include lumbar spina bifida, open meningomyelocele, Chiari‐II‐malformation, hydrocephalus internus and vesicoureteral reflux III°. On his second day of life a Rickham‐Capsule was implanted and the open spine was covered. On his 9th day of life a right ventricular peritoneal shunt (VP‐shunt, Codman‐Hakim valve, pressure level 140 mmH2O) was implanted. The boy was presented to us with a complete (full‐thickness) rectal prolapse, which had progressed under conservative therapy. The boy suffered from frequent abdominal pain, but had regular, non‐bloody bowel movements, and was well nourished. Clinically, there were a severe external rectal prolapse with erosive mucosal lesions and a lax pelvic floor with a dilated anal canal.
Management and Outcome: Due to the implanted VP‐shunt the patient received intravenous, antibacterial prophylaxis (cefotaxim and vancomycin), started one day preoperatively and continued for five days postoperatively. Laparoscopic rectopexy was performed using 4 trocars (2 and 3 mm). The patient was positioned by overstretching the pelvis slightly. The rectum was pulled back into the peritoneal cave laparoscopically and held in position via a loop brought through a window of the mesorectum. The fixation of the rectum to the exposed promontory was performed under moderate tension with a continuous, transmural, resorbable suture (Covidien V‐Loc™ wound closure device) without mesh implantation. Time of operation was 113 minutes. The pressure of abdominal gas insufflation was 6 mmHg. No intraoperative or postoperative complications occurred, particularly no shunt infection. Nutrition could be started on the day of operation. The patient was discharged on the 6th postoperative day. There was no recurrence of a rectal prolapse, the patient showed up free of symptoms in the follow‐ups.
Conclusion: Laparoscopic rectopexy can be performed well with appropriate instruments even in infancy. Since there are no valid data about advantages and disadvantages of different surgical techniques for rectal prolapse in infancy, it's advisable to proceed as restrictively as possible and to adapt the procedures due to the success of the therapy. If sclerotherapy or cerclage are not indicated due to the severity of the case, laparoscopic rectopexy offers a good surgical option. Using a mesh should be considered cautiously, as the risks of intestinal obstruction or perforation might be much higher because of the significantly smaller anatomical conditions compared to children or adolescents. In our case of a 2 month old boy with a continuous, transmural, resorbable suture (Covidien V‐Loc™ wound closure device) the outcome was successful.
QS066 THORACOSCOPIC REPAIR OF H‐TYPE TRACHEOESOPHAGEAL FISTULA IN NEWBORN: A TECHNICAL AND OUTCOME PERSPECTIVES
QS067 ROLE OF MINIMALLY INVASIVE SURGERY AFTER NEOADJUVANT CHEMOTHERAPY IN PEDIATRIC AGE: PRELIMINARY EXPERIENCE
1Buzzi Children's Hospital, Milan, Italy, 2Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy
Background and aims: In pediatric oncology secondary surgery is performed, depending on the protocols, after neoadjuvant chemotherapy, mainly in unresectable or metastatic tumors in order to perform a radical ablation of the residual mass. The characteristics of tissues after chemotherapy, with tight adhesions to main vessels and vital structures, make this surgery difficult, thus the traditional open approach is routinely adopted. Nevertheless in some cases of metastatic tumor the opportunity to perform a minimally invasive surgery (MIS) may represent a big advantage for the patient. Aim of our study is to present our preliminary experience of pediatric patients submitted to secondary surgery with a minimally invasive approach.
Methods: We retrospectively analyzed our oncological patients submitted to minimally‐invasive secondary surgery, in a period between July 2012 and June 2018. Following data were analyzed: demographics, tumor characteristics, timing of surgery, preliminary biopsy, operative details, operative time, intra‐ and postoperative complications, hospital stay, recurrence at follow‐up.
Results: A total of 25 oncologic patients were treated through a minimally‐invasive approach in the period of study. Of these, 4 had previously been subjected to chemotherapy according to the protocols related to the specific neoplasm. The patients, all males, had a median age at diagnosis of 17 months (range 10–168) while the median age at operation was 23 months (range 20–175). Types of tumors were: 3 stage IV adrenal neuroblastoma (NB) (2 right, 1 left); 1 metastatic sacrococcygeal germinal (yolk sac) tumour (YST). Of the 3 patient with NB, one had undergone a tru‐cut biopsy of the primitive lesion, one an open transoral biopsy of a jaw metastasis and one a bone marrow biopsy; the YST patient had undergone a biopsy of the sacrococcygeal mass in another centre. Median preoperative size of tumor mass was 4.6 cm (range 4.2–7.5). The procedures were all performed by the same operator, experienced in MIS and oncologic surgery. The MIS approach to the mass was entirely laparoscopic in the 3 NB cases, while the YST was excised though a combined laparoscopic and perineal approach in order to resect the coccyx. Median operative time was 279' (range 118 – 380). All the masses were extracted inside an endobag. No intraoperative nor postoperative complications occurred. Median postoperative stay was 6.5 days (range 3 – 19). No recurrences were observed at a median follow‐up of 18.5 months (range 12 – 74).
Discussion and conclusions: While presenting considerable technical difficulties, secondary surgery of pediatric tumors after neoadjuvant chemotherapy can be performed with minimally invasive technique in highly selected cases. It offers to this group of patients, affected by high grade or metastatic disease, all the advantages of MIS compared to traditional surgery: less pain, shorter recovery times, earlier chemotherapy, less surgical complications like intestinal adhesions and incisional hernias. However, patients should be carefully selected by a multidisciplinary team comprising at least surgeon, pediatric oncologist and radiologist, always according to the treatment protocols, and the surgical act must strictly adhere to the principles of oncologic surgery and be entrusted to expert hands.
QS068 DURATION OF FEVER AND AGE AT PRESENTATION AS KEY PROGNOSTIC FACTORS FOR SUCCESSFUL NONOPERATIVE MANAGEMENT OF UNCOMPLICATED APPENDICITIS IN CHILDREN
1Juntendo University School of Medicine, Pediatric General & Urogenital Surgery, 2Juntendo University School of Medicine, Clinical Research and Trial Center
Aim: To assess nonoperative management (NOM) for uncomplicated appendicitis (UC‐appy) in children.
Methods: All UC‐Appy cases presenting before the age of 16 years between 2014 and 2018 who had NOM (one dose of intravenous analgesia, intravenous piperacillin‐tazobactam (TAZ) 112.5mg/kg 8 hourly) and were followed‐up for more than 3 months after treatment (n = 146) were prospectively reviewed. An integral feature of our NOM protocol are criteria for evaluating effectiveness. They were: 1. Abdominal pain (assessed every 12 hours using a numeric rating scale where 5 was the level of pain at presentation); 2. Body temperature (assessed every 12 hours); and 3. Laboratory data (white cell count, assessed every 24 hours).
Results: NOM was successful (S‐NOM) in 48.6% (n = 71) and failed (F‐NOM) in 51.4% (n = 75). Gender ratios (S‐NOM vs F‐NOM: 62.0% male vs 56.0% male), mean maximum body temperature (38.1o vs 38.1o), presence of rebound tenderness (69.0% vs 73.3%), WBC (14.4 vs 15.1x103/uL), CRP (5.7 vs 6.0mg/dL), size of the appendix (9.4 vs 9.6mm), presence of an appendecolith (40.8% vs 40.0%), and duration of pain (1.9 vs 1.8 days) were similar for both groups, but differences in mean age at presentation and duration of fever preadmission were statistically significant; 10.4 years old (S‐NOM) versus 9.1 years (F‐NOM) and 1.3 days (S‐NOM) versus 1.8 days (F‐NOM), (p = .021 and p = .018, respectively). Receiver operator characteristic curve analysis showed that 7.0 years old (32% sensitivity, 7% specificity) and 1.0 days (95% sensitivity, 75% specificity) were the optimal cut off values for age at presentation and preadmission fever duration, respectively. NOM was abandoned according to a protocol determining failure at 12 hours (n = 20/75; 26.7%), 24 hours (n = 31/75; 41.3%), 36 hours (n = 14/75; 18.7%), 48 hours (n = 2/75; 2.7%), 60 hours (n = 4/75; 5.3%), and 72 hours (n = 4/75; 5.3%). All F‐NOM required laparoscopic appendectomy (LA). Of these, 14/75 (18.7%) were perforated at LA. Post‐LA sequelae arising within 3 months were: residual abscess (n = 7/75; 9.3%) and transient ileus (n = 1/75; 1.3%). Two residual abscess required CT‐guided percutaneous drainage; the rest resolved spontaneously. Results of a review of the English language literature for studies evaluating NOM for UC‐appy in children are shown (Figure‐1).
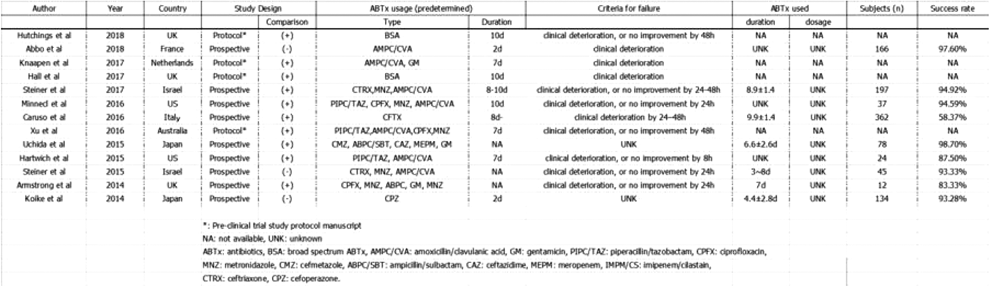
Conclusion: Our data suggest that UC‐appy patients 6 years old or younger and febrile for at least 2 days before presentation may benefit from elective surgery rather than NOM.
QS069 RETROPERITONEAL APPROACH NEPHRECTOMY AS GOLD STANDARD IN PEDIATRIC END STAGE RENAL DISEASE: 16 CASES GUATEMALA CITY
Roosevelt Hospital
Introduction: In Pediatric population there are multiple urinary tract diseases, congenital or adquired, that need total nephrectomy or heminephrectomy. For a surgical procedure to become a gold standard approach it needs the following variables: Applicable in multiple surgery indications and in different age patients, reproducible, safe and low morbidity. Pediatric patients with end stage renal disease (ESRD) require renal replacement therapy like peritoneal dialysis, haemodialysis or kidney transplant. In children, the peritoneal dialysis is the first choice for renal replacement therapy so when an urological surgery is needed the retroperitoneal approach is the best option. Refractory arterial hypertension is the most frequent indication for nephrectomy in pediatric patients with ESRD. However, massive proteinuria, kidneys trasplant protocol, urinary tract sepsis, severe hydronephrosis are other surgical indications for retroperitoneal or transperitoneal approach nephrectomy.
Methods and Materials: Prospective Descriptive Longitudinal Study that include 16 pediatric nephrectomies with retroperitoneal approach operated in Pediatric Surgery Department of Roosevelt Hospital, Guatemala City, between November 2012 ‐ November 2017.
Results: There are 16 nephrectomies with retroperitoneal approach in 14 patients (02 bilateral nephrectomies). The average age was 9.7 years old (1.5 ‐ 15), average weight 23 Kg (10 ‐ 30.6). Ten patients were Male and six patient were Female. Left nephrectomy was done in 10 cases (62.5%) and right nephrectomy on 06 cases (35%). Indications for surgery were: refractory arterial hypertension 12 patients (75%), severe hydronephrosis and renal exclusión 02 patients (12.5%) and vesicoureteral reflux nephropathy/sepsis 02 patients (12.5%). Twelve patients (75%) were in renal replacement therapy (peritoneal dialysis or haemodialysis). All patients h0ad Renal ultrasound (US) and Voiding uretrocistogram (VCUG). Only 03 patients (18.75%) had CAT Scan or renal Gammagraphy. Penrose drain was used in 04 patients (25%). Average surgical time was 131 minutes (77 ‐ 203). Complication rate was 02 patients (12.5%), hospital stay 7.1 days (3 ‐ 15), conversion and mortality rate was 0%.
Conclusion: Retroperitoneal approach nephrectomy should be the gold standard in pediatric ESRD.
QS070 EVALUATION OF LAPAROSCOPY IN THE TREATMENT OF INTESTINAL OBSTRUCTTION IN CHILDREN
Department of Pediatric Surgery, the 2nd Affiliated Hospital of Harbin Medical University
Objective: Because of abdominal distention, the patients with intestinal obstruction have limited operation space in abdominal cavity, which has once become a contraindication of laparoscopic operation. This article evaluates the value of minimally invasive laparoscopic techniques in the diagnosis and treatment of pediatric intestinal obstructive diseases.
Methods: Retrospective analysis was made on the cases of intestinal obstruction treated by laparoscopy from 2007 to 2017. Included the child's age, gender, diagnosis, surgical methods, prognosis and so on.
Results: 129 children diagnosed with intestinal obstruction underwent laparoscopic surgery, including 97 males and 32 females, with an average age of 4 years (3 days ‐ 14 years). The types of disease included 18 cases of intestinal atresia (There were 8 cases of intestinal obstruction, 5 cases of small intestine atresia, 5 cases of anal atresia), 12 cases of intestinal malrotation, 7 cases of Meckel's diverticulum, 2 cases of congenital cord, 15 cases of incarcerated hernia, and 7 cases of intussusception (5 Cases of acute 2 cases of chronic), 57 cases of adhesive intestinal obstruction (There were 42 cases of previous operation history, 15 cases of acute and chronic abdominal infection inflammatory mass), 5 cases of fecal ileus obstruction, 3 cases of intestinal obstruction caused by swallowing magnetic foreign body, 3 cases of abdominal hernia. Surgical methods include: laparoscopic direct intestinal anastomosis, extracorporeal anastomosis, sling removal, adhesion loosening, intussusception reduction, incarcerated iliac crest, high ligature ligation, and diverticulum resection. Among them, 11 cases were converted to open surgery and 2 cases were reoperation with second laparoscopic surgery. There were no deaths and no serious complications. After a follow‐up of 6 months to 2 years, the prognosis was good.
Conclusion: Minimally invasive laparoscopic technique has its advantages in the diagnosis and treatment of intestinal obstructive diseases in children, with less trauma, sufficient exploration and quick recovery. However, the timing of surgery needs to be masteredproperly, excessive abdominal distension will affect the operating space, and intraoperative intestinal decompression can be carefully selected. Timely conversion to open surgery can avoid serious complications.
QS071 CHILEANS ARE THE CHAMPIONS: VERY‐HIGH INCIDENCE OF LAPAROSCOPIC CHOLECYSTECTOMY IN A RETROSPECTIVE SINGLE‐CENTER PEDIATRIC POPULATION
1Pediatric Surgery Department. Hospital Carlos Van Buren, Valparaíso, Chile. Universidad de Valparaíso, Chile., 2Pathology Department. Hospital Carlos Van Buren, Valparaíso, Chile. Universidad de Valparaíso, Chile., 3Centro Interdisciplinario de Estudios en Salud, CIESAL. Universidad de Valparaíso, Chile.
Introduction: Recent series report incidence of pediatric cholecystectomy to be 0.8 to 13.0/100,000. The Chilean adult population is characterized by a very‐high prevalence of gallstones disease and gallbladder cancer. However, the incidence of cholecystectomy in the Chilean pediatric population has not been estimated. The aim of our study was to determine the demographics and clinical features of our pediatric population submitted to laparoscopic cholecystectomy.
Methods: A retrospective single‐center review of children 0‐15 years during 2011‐2018 was performed. Clinical data were obtained from medical records. The incidence rate was estimated in the base of population data.
Results: In an 8‐year period 65 patients with gallbladder diseases were identified. Four patients were excluded by congenital malformations of the biliary tract. Laparoscopic cholecystectomy was indicated in 61 patients. Three patients had an identifiable cause of gallstones, two by use of parenteral nutrition and one due to hereditary spherocytosis. Another patient was diagnosed with biliary dyskinesia. The remaining 57 patients presented unrelated cholelithiasis, with only one asymptomatic patient. For patients with surgical indication, 19 (31.1%) had complicated gallstones disease (acute cholecystitis, choledocholithiasis, jaundice and biliary pancreatitis). Three of them were managed in another center by the need of ERCP. A total of 58 patients were submitted to laparoscopic cholecystectomy in our hospital. The mean age was 12.8 ± 2.6 years and 46 (79.3%) were females. None of the patients were identified as Mapuche Indigenous. Nutritional status was overweight in 7 (12.1%) and obesity in 23 (39.7%). Fatty liver was presented in 8 (13.8%). Operative time was 78.6 ± 23.1 minutes. Intraoperative cholangiography was not performed in our patients. No conversions, major complications or bile duct injuries were noted. The length of stay was 1.88 ± 0.62 days. At histological examination, 54 (93.1%) patients showed chronic inflammatory changes. Analysis of stones was performed in 45 patients, with cholesterol in 27 (60%), mixed in 14 (31.2%), and both pigmented and sludge in 2 each (4.4%). The estimated incidence of laparoscopic cholecystectomy for this cohort was 23.42/100,000.
Discussion: Our Chilean pediatric population exhibits distinctive features compared to previous studies in children: a very‐high incidence of laparoscopic cholecystectomy, a high number of symptomatic patients, lower rates of biliary dyskinesia and hematological disorders as indications of surgery, and a high proportion of cholesterol stones. The high chronic histologic changes observed in our patients and the good surgical outcomes suggests that laparoscopic cholecystectomy must be the treatment option in Chilean pediatric patients with gallstones disease.
QS072 “BURNIA” TECHNIQUE FOR THE TREATMENT OF INGUINAL HERNIAS IN GIRLS
Nuestra Señora de Candelaria University Hospital, Santa Cruz de Tenerife, Spain.
Introduction: Minimally invasive surgical techniques are increasingly applicable in pediatric patients. We present our initial experience in the use of “BURNIA” technique (cauterization of the deep inguinal ring) in girls.
Methods: Retrospective review of girls with diagnosis of inguinal hernia, operated according to “BURNIA” technique between January 2017 and September 2018.
Surgical procedure: The procedure is performed under direct vision with 5mm‐0 degrees pleuroscope with 3 mm working channel introduced by umbilical port. A 3mm Maryland dissector is introduced by the working channel and is used to burn the inguinal hernias and patent processus vaginalis. In the case of contralateral patent peritoneovaginal duct, it was repaired by BURNIA technique in the same surgical act, even in the absence of symptoms.
Results: 26 BURNIA procedures were performed in 16 girls on an outpatient basis. Mean age was 5 years (4 months‐13 years). 10 cases were unilateral and 8 were bilateral cases. In 4 patiens the preoperative diagnosis was unilateral, nevertheless cotralateral defect side was diagnosed and treated. 12 cases had concomitant umbilical hernia and were resolved in the same surgical act. Mean operative time was 12 minutes (6‐25 minutes) and 17 minutes (12‐32 minutes) in unilateral and bilateral cases respectively. At the beginning of our learning curve we had 1 conversion to open herniorrhaphy. Mean follow‐up was 12 months (1 ‐ 20 months).
Conclusion: BURNIA is a feasible technique. It allows intraoperative diagnosis and repair of contralateral defects, and the concomitant treatment of others procedures in the same surgical act. Under our initial experience, the learning curve is fast and has good functional and aesthetic results, without visible scars.
QS073 COMPARISON OF THE EFFECTIVENESS BETWEEN THREE DIFFERENT ENDOSCOPIC SURGICAL SKILL TRAININGS FOR MEDICAL STUDENTS USING THE INFANT LAPAROSCOPIC FUNDOPLICATION SIMULATOR
Pediatric Surgery, Kagoshima University
Background and Aim: Trainings on the acquisition of laparoscopic suturing skills are range to dry‐box training to virtual simulator training. There are advantages and disadvantages with each training method, however, it is not revealed which training is best for medical students and young surgeon. The aim of this study is comparing the proficiency of medical students in acquiring laparoscopic suturing skills after short‐term trainings: a video, an expert teacher or a virtual simulator.
Materials and methods: Eighteen medical students (6th grade in medical school in Japan) were registered and divided into three groups; 1) a group received personal training while watching training video (video group), 2) a group received training under the guidance of an expert (teaching group) and 3) a group received personal training with a virtual simulator (virtual group). They practiced laparoscopic suture and tie skills for one hour. Following their training, they performed the evaluation task of three sutures and ties using the laparoscopic fundoplication simulator (Fig. 1). We developed a 1‐year‐old infant body model (body weight 10 kg) based on computed tomography (CT) data and reproduced a pneumoperitoneum body model based on the clinical situation. The liver and spleen were made of urethane, and the stomach was made of styrene. The pneumoperitoneum model was covered with synthetic skin. A 30° scope 5 mm in diameter was fixed using an arm. We measured the time required to complete the task, the path length of both forceps tips, average velocities of both forceps tips, suturing balance of the right and left side in making 3 ligatures and suturing interval between 3 ligatures in wrap construction. To further analyze the spatial trace of the tips of the forceps, TrackSTAR (Northern Digital Inc., Ontario, Canada) was used as the three‐dimensional position measuring instrument and placed on the thoracic side of the model to trace the tips of the needle driver and forceps. The needle driver and assistant forceps had sensors mounted on the tips, and their paths were traced on a computer with an electromagnetic tracking system. All data are expressed as the mean ± standard deviation. Two‐tailed paired and unpaired Student's t‐tests and analyses of variance were conducted for comparisons using the JMP® 11.0 statistical software program (SAS Institute Inc., Cary, NC, USA). All data were defined as being statistically significant at p values <0.05.
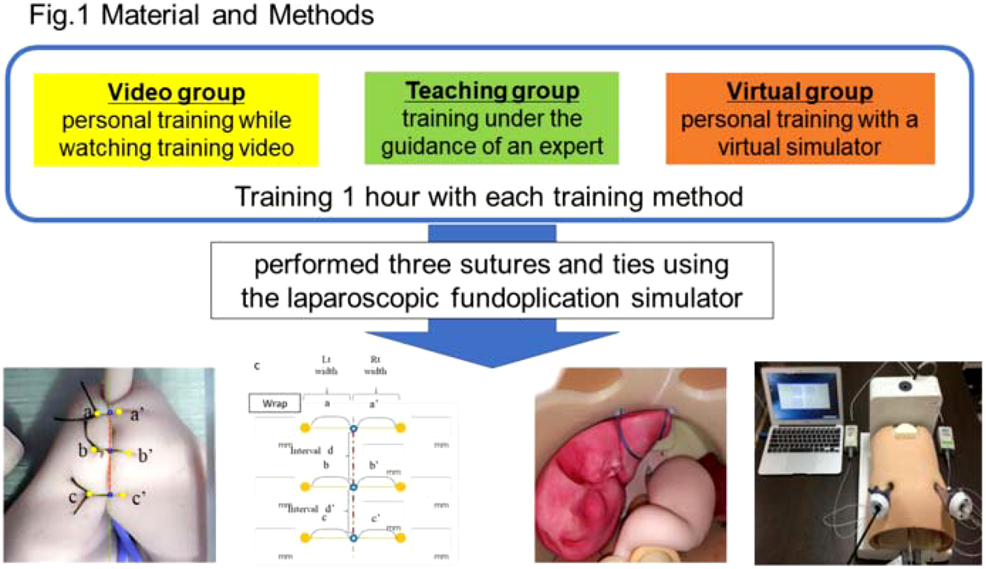

Results: The obtained results are shown in Table 1. The path length of assistant forceps in virtual group is longer than other two groups, but there is no significance (video group 4230.72 ± 4157.36, teaching group: 2805.93 ± 966.33, virtual group: 7925.54 ± 6379.83, p = 0.06). There are no significant outcome in other evaluation parameters.
Conclusion: Varies of short‐term training in this study did not affect the acquisition of laparoscopic suturing skill in medical students. Long‐term training with each method may affect the acquisition of laparoscopic suturing skills. Long‐term and combination training study should be done in order to develop the best training method for medical students and unexperienced young surgeons.
QS074 LAPAROSCOPIC INTERVENTION IN PEDIATRIC BLUNT LIVER AND SPLEEN INJURY A USEFUL APPROACH TO AVOID LAPAROTOMY
1Phoenix Children's Hospital, 2Akron Children's Hospital, 3Arkansas Children's Hospital, 4Dell Children's Medical Center, 5Children's Healthcare of Atlanta, 6Children's Mercy Hospital, 7Children's Medical Center part of Children's Health (SM), 8Le Bonheur Children's Hospital, 9The Children's Hospital at OU Medical Center
Background: Several series have reported the use of diagnostic laparoscopy in pediatric trauma, however there has been little reported about the use of laparoscopy as a treatment modality in this population. We queried the data from a large multicenter trial focused on contemporary management of blunt liver or spleen injury (BLSI) in children to ascertain the incidence and extent of laparoscopy utilization.

Methods: Prospective data was collected on all children age ≤18 years with BLSI presenting to one of 10 Pediatric Trauma Centers. Patients who required laparoscopy were identified and demographic and clinical data were collected in order to determine the role of laparoscopy in the care of the trauma patient.
Results: Of 1008 children with BLSI, 58 patients required laparotomy, 10 required a laparoscopic procedure and one patient underwent a laparotomy followed by laparoscopy one day later. In 2 patients the laparoscopic procedure was converted to a laparotomy. Median age of patients undergoing laparoscopic procedure was older than the laparotomy group (11.5 [IQR: 5.8, 16.4] vs 10.2 [IQR: 5.3, 15.0]). Laparoscopy was performed at 7 of the 10 centers. Median time to surgery was statistically longer in the laparoscopic group compared to the laparotomy group (42 hours [IQR: 8, 96] vs 3.2 hours [IQR: 2, 5] (p < 0.05)). Laparoscopy was performed in six patients with liver injury, 4 had spleen injury and 1 with both. Procedures and frequencies performed are presented in table 1.
Conclusions: The use of laparoscopy in pediatric BSLI is uncommon (∼1%) and is utilized much later in the clinical course than laparotomy. Despite these findings, laparoscopy is successful in over 80% of patients as a diagnostic and treatment modality, and has a role in clinically stable pediatric BSLI trauma patients.
QS075 EARLY MANAGEMENT OF ESOPHAGEAL LEAK IN ESOPHAGEAL ATRESIA. CHANGING PARADIGMS
Clínica Las Condes
Introduction: One of the most fear complication in Esophageal Atresia (EA) repair is the leak of the anastomosis. It occurs in 10 to 20% of the cases, regardless the type of approach. Thoracoscopic repair is trans‐pleural, with the potential development of an empyema if a leak occurs. Traditional treatment has always been observation, drainage and antibiotics. The reason to avoid a re‐do anastomosis is to suture fragile esophageal tissue, resulting in high‐risk of stenosis or a new major leaking. Our objective is to show that an early thoracoscopic re‐do anastomosis management is safe and feasible.
Materials and Method: Retrospective study of a case series of four pediatric patients, diagnosed with EA and treated with thoracoscopic approach between 2013 and 2018. Variables analyzed were: Age, weight, type of EA, day of leaking, surgical approach, time to start feeding, surgical complications and follow‐up.
Results: Four patients were included in this study. They were all born at term. Mean weight was 2,7 kg. Three patients were type III EA, and 1 was type I EA. The three type III EA patients were operated with thoracoscopic approach within the first two days of life. The patient with type I EA underwent a gastrostomy and six weeks later the thoracoscopic anastomosis was done. Leaking was found the second day post‐op in one patient, the third day in two patients, and the fifth day in the last one. It was diagnosed with the observation of saliva in the drainage, chest X‐ray and esophagogram in all of them. All the patients were operated in the first 24 hours after diagnosis of the leak by a thoracoscopic approach. The site of leaking was found and a re‐do anastomosis was performed. Patients started feeding between the third and fourth day through the trans‐anastomotic tube and started oral feeding at the seventh day after showing an esophagogram without leak. No complications were found after the re‐do anastomosis. Mean time to discharge: 10 days. One patient needed two dilatations, another one needed four dilatations and a Nissen fundoplication. The other two patients did not need any other procedures or dilatations. Mean time of follow‐up: 33 months.
Conclusion: Early thoracoscopic leak repair can be considered as an alternative to the traditional management. The re‐do esophageal anastomosis is a change of paradigm because it potentially avoids an empyema and its complications. Also offers the benefit of preservation of the native esophagus, the patients can resume enteral feedings earlier and shorten the length of hospitalization.
QS077 LAPAROSCOPIC REPAIR OF PEDIATRIC INGUINAL HERNIA: DISCONNECTION OF THE HERNIAL SAC VERSUS DISCONNECTION AND PERITONEAL CLOSURE
Tanta Faculty of Medicine
Background/Purpose: Several techniques were described for laparoscopic treatment of pediatric inguinal hernia (PIH). Some authors emphasized the importance of disconnecting the sac, to create a scar, and to close the peritoneum to mimic the open approach. Others stated that peritoneal disconnection alone is enough for treatment of PIH regardless the size of the internal ring. In this study we compare the short term results of laparoscopic disconnection of PIH sac versus disconnection and peritoneal closure as regards feasibility, operative details, postoperative complications and recurrence rate.
Patients and Methods: This prospective randomized clinical study was carried out in Pediatric Surgery Unit, Tanta University Hospitals, during the period from March 2016 to March 2017, on 33 patients with 40 pediatric inguinal hernias, with age from 1‐ 24 months; patients were randomly divided into 2 groups. Group A: subjected to laparoscopic disconnection of the hernia sac without closure of peritoneum over internal ring. Group B: subjected to laparoscopic disconnection of the hernia the sac with closure of peritoneum over internal ring. Both groups were compared regarding the operative details, including complications and conversion, postoperative complications and recurrence.
Results: Group A included 20 hernias in 15 patients, while Group B included 20 hernias in 19 patients. The age ranged from 1‐21 months. The male: female ratio was 7.5:1. In Group A, the mean operative time was 34.6 ± SD 3.71 min and 39.4 ± SD 4.39 min for unilateral and bilateral case respectively, while in Group B, it was 45.1 ± SD 4.87 min for unilateral cases and 65 min. for 1 bilateral case. The operative time was significantly shorter in group A than group B for unilateral cases (P < 0.01). There was no conversion and no intraoperative complications. No recurrences occurred in Group A while 3 recurrences were encountered in Group B. All recurrences occurred in hernia with internal ring diameter >10 mm. However the difference was statistically insignificant between the two groups.
Conclusion: Laparoscopic treatment of PIH can be done safely with both techniques. Laparoscopy offers many advantages specially visualization of both sides, magnification and minimal manipulation of cord structures. Both laparoscopic sac disconnection with internal ring closure and sac disconnection only are effective for treatment of PIH however the latter technique is not recommended for cases with internal ring diameter >10 mm. larger numbers from different centers are needed to validate these results.
Keywords: laparoscopic, Pediatric, hernia repair, sac disconnection.
QS079 LAPAROSCOPIC LATERO‐LATERAL URETERO‐BLADDER ANASTOMOSIS WITH EXTRAVESICAL URETERAL REIMPLANTATION FOR THE URETEROVESICAL JUNCTION OBSTRUCTION CORRECTION
1Municipal Children's Hospital. Hospital Pediátrico del Niño Jesús Chair of Pediatric Surgery. Universidad Nacional de Córdoba. Córdoba. Argentina., 2Municipal Children's Hospital, Chair of Pediatric Surgery. Universidad Nacional de Córdoba. Córdoba. Argentina, 3Chair of Pediatric Surgery. Universidad Nacional de Córdoba. Córdoba. Argentina
Objectives: Surgical management of megaureters is one of the most difficult problems in urologic surgery in neonates and infants. We describe laparoscopic latero‐lateral uretero‐bladder anastomosis with extravesical ureteral reimplantation technique for the ureterovesical junction obstruction UVJO correction.
Material and Methods: Five children (3 male, aged 6 months to 5 years 2 right side) underwent laparoscopic latero‐lateral uretero‐bladder anastomosis with extravesical ureteral reimplantation. Two with antenatally obstructive megaureter were detected. Three had recurrent urinary infection.
Preoperative examination consisted on: laboratory test, renal sonography (intermitent moderate hydronephrosis with no caliceal dilatation and a well preserved cortex) voiding cystourethrography, 99m Tc DTPA diuretic renal scan and uroresonancy and nephrotomography in older patients. Reimplantation indication was marked as progression of hydroureteronephrosis on ultrasound, delayed excretion on D.T.P.A. One patient had concurrent ureteropelvic and ureterovesical junction obstruction; one had contralateral vesicoureteral grade 3 reflux. The postoperative follow up included abdomino‐pelvic ultrasound at three months after surgery, and a voiding cystourethrography at six month after initial surgery.
Technique: laparoscopic detrusor‐tunnelling, extravesical ureteroneocystostomy with previous latero‐lateral uretero‐bladder anastomosis without section of the native ureter technique, even for the treatment of very wide ureters. The bladder is mobilized to gain sufficient lenght of the submucosal tunnel and proper ureteral direction. The ureter wich passes through the sub mucosal tunnel, is first mobilized with blunt dissection, not transected; at the level of stenosis, a hitch stitch is placed from the internal side of the ureter to the external lateral wall of the bladder. Then is opened in its internal wall, and anastomosed to the neo hiatus in the bladder. Vesical mucosa is opened and latero‐lateral ureterovesical anastomosis is performed, a double J stent is placed. The ureter is then installed into the detrusor cavity and the tunnel is closed.
Results: The drain was removed after 24 hours and all the patiens were discharged home in the first 36 hours with Foley catheter. In one patient with concurrent ureteropelvic junction obstruction we perform at the same time laparoscopic dismembered pyeloplasty, in other patient with contralateral reflux, endoscopic injection of bulky agent was performed at the same time of the major surgery. A 3 month follow‐up ultrasound showed considerable improvement of the hydronephrosis vesicoureteral. The patients do not required oral opioids once they are discharged from the hospital.
Conclusions: several surgical techniques are proposed for the treatment of UVJO, consisting of an intravesical approach or a combined intravesical‐extravesical approach. The most popular is ureteroneoystostomy technique with tailoring of ureters, especially when they are very wide. prenatal detected ureterovesical junction obstruction (UVJO) rarely undergoes surgical intervention today, but those with extreme dilation and reduce function are likely to benefit from surgical therapy. Surgical management of megaureters is one of the most difficult problems in urologic surgery, particularly in neonates and infants.
QS080 MINIMALLY INVASIVE SURGERY IN PEDIATRIC DIAPHRAGMATIC DISEASE: 51 CASES IN ROOSEVELT HOSPITAL GUATEMALA CITY
Roosevelt Hospital
Introduction: Diaphragmatic diseases are common in pediatrics. The surgical treatment has shifted to the Minimally Invasive Surgery. The main disadvantages of MIS is the 7% hernia recurrent rate and the longer surgery time when compared to open surgery.
Materials and Methods: Prospective Descriptive Longitudinal Study that includes 51 pediatric patients with diaphragmatic diseases (congenital diaphragmatic hernia, diaphragmatic eventration) born or transfered to the Roosevelt Hospital that required a surgical treatment by Video Assisted Thoracic Surgery (VATS) between October 2012 and 2018 (6 years).
The patients were divided by age in three groups: Group #1 Neonates (1 – 30 days), Group #2 Infants (1 month – 2 years) and Group #3 Pre‐School (2 years and older).
Results: The results can be seen in TABLE 1. and show epidemiologic and surgical variables as well as global and group integrated results.
Conclusions: Minimally Invasive Surgery is a great technique for the treatment of Diaphragmatic Diseases in Childrens with low morbidity and mortality.
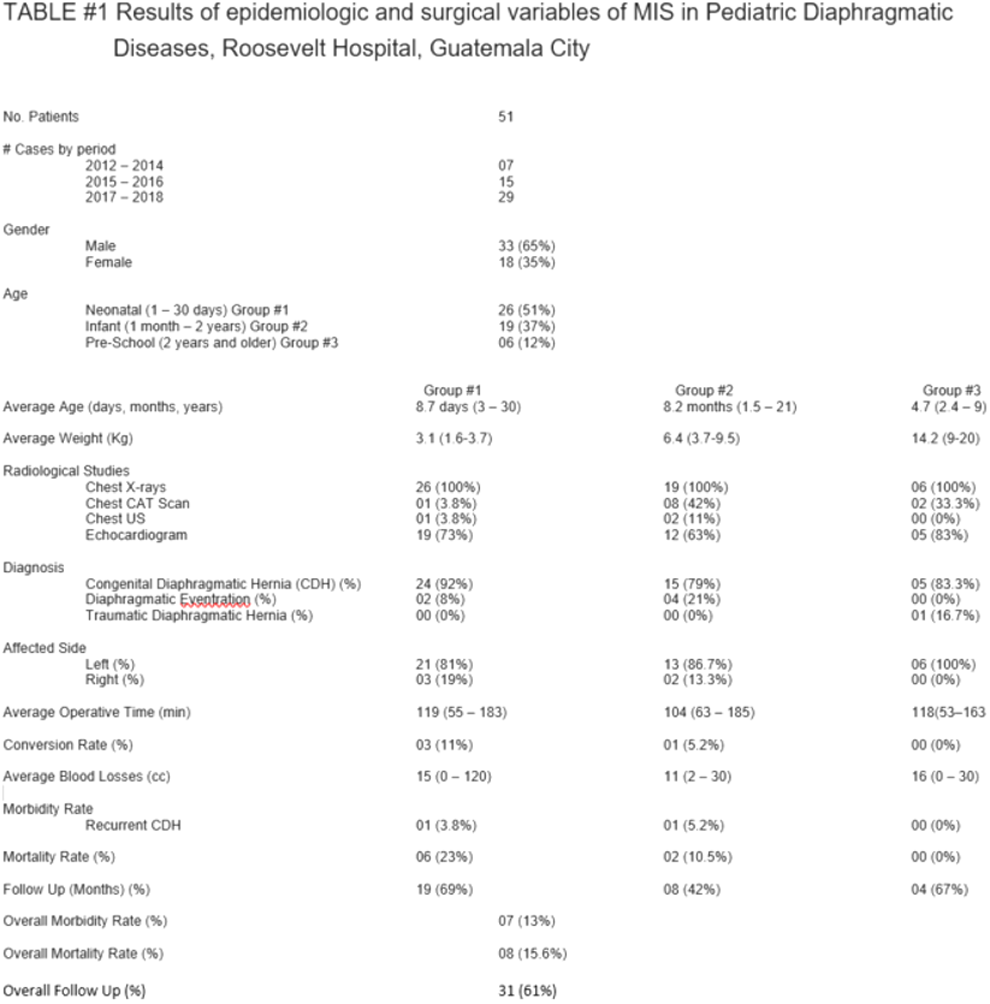
QS081 LAPAROSCOPIC TREATMENT OF SPLENIC BENIGN LESIONS (SBL) IN THE PEDIATRIC POPULATION: AN ITALIAN MULTICENTER EXPERIENCE
1Pediatric Surgery Unit, Ospedale dei Bambini “v. Buzzi”, Milano, Italy AND Pediatric Surgery Unit, University Hospital of Padova, Padova, Italy, 2Pediatric Surgery Unit, University Hospital of Padova, Padova, Italy, 3Pediatric Surgery Unit, Ca' Foncello Hospital, Treviso, Italy, 4Pediatric Surgery Unit, Ospedale dei Bambini “v. Buzzi”, Milano, Italy
Aims: The advantage of spleen preservation in children with splenic benign lesions (SBL) is to maintain as longer as possible the splenic immune function. The laparoscopic partial splenectomy (LPS) is widely accepted for hemoglobinopathies whereas in the literature there are few data about the laparoscopic treatment of SBL.
We aimed to have a large multicenter series in order to assess the feasibility of LPS for in children with SBL.
Methods: Data of patients laparoscopically approached for SBL since January 2007 to September 2018 from three Italian Centers were retrospectively reviewed.
Results: 18 patients (10 Centre 1, 7 Centre 2, 1 Centre 3) with SBL were laparoscopically approached. 10 were males and 8 females; the mean age at surgery was 12,6 years (range between 5,9 to 17,3 years). In all patients the LPS was pre‐operatory planned on the basis of a high definition imaging of the ilar vessels (angio‐MRI or CTscan).
15 (83%) underwent to partial splenectomy and 3 (17%) to cystic drain and unroofing. In all patients the splenic parenchyma was sectioned by Ligasure® or Stapler in order to obtain a better section of the healthy splenic tissue and the resected spleen was removed within an endo‐Catch through the umbilical access. None patient needed a conversion to laparotomy neither a blood transfusion.
The mean operative time was 202 minutes. Final diagnosis showed a cystic lesion in 15, Lymphangioma in 2, Amartoma in 1. In all patients the postoperative course was uneventful and the mean length of stay was 5,8 days. At long‐term follow‐up 4 patients (22%) presented recurrence of the cyst: two out of four were been previously treated with unroofing and two with LPS. In three a redo surgery with total splenectomy was required, while one patient with a mild cyst underwent an alcoolization.
Conclusions: In literature there are limited data about LPS in children with SBL, nevertheless this technique may be considered a suitable option and, likely, the treatment of choice only in Centres with a high level of laparoscopic skills. In our opinion LPS with Stapler or Ligasure® has a lower risk of recurrence of the cysts compared with the unroofing, however larger series with more homogeneous data are necessary to confirm this opinion.
QS082 GASTRIC PULL‐UP IN ESOPHAGEAL ATRESIA: MODIFIED LAPAROSCOPIC APPROACH
1Departament of Pediatric Surgery, University Hospital Arnau de Vilanova, 2Departament of Pediatric Surgery, University Hospital Vall d'Hebron
Aim: To describe a modified surgical technique and the initial outcomes for esophageal replacement through laparoscopic gastric pull‐up by posterior mediastinal pathway in esophageal atresia patients.
Material and Methods: Descriptive study of four patients had EA type I undergoing laparoscopic esophageal replacement between January 2016 and December 2017. After pyloric forced dilation with balloon through the gastrostomy, the stomach was dissected preserving the right gastroepiploic artery. The gastrostomy was disassembled and the stomach was exteriorized to be tubulized. Then laparoscopic trans‐hiatal blunt dissection was realized. Cervical esophagogastric anastomosis was done by gastric pull‐up using the posterior mediastinal pathway.
Results: The surgical procedure was successfuly completed in all children. One patient had a punctiform tracheal perforation that was resolved immediately though tracheal suture. All patients were fed through transpyloric tube at 24 hours. Oral feeding began once the absence of leaks was confirmed. One patient presented an anastomotic leak that was treated non‐surgicaly. A pyloric dilation was realized 3 months after surgery.
Conclusion: Laparoscopic approach in esophageal replacement is secure and has few complications. Slight modifications of the technique such as pyloric dilation and gastric extracorporeal tubulization descend laparoscopic surgical time.
QS083 MORBIDITY IN THE THORACOSCOPIC TREATMENT OF ESOPHAGEAL ATRESIA WITH TRACHEOESOPHAGEAL FISTULA. A VIEW TO THE PAST 10 YEARS IN THE HOSPITAL DE EMERGENCIAS PEDIATRICAS‐ LIMA‐PERU
Hospital de emergencias pediatricas
Introduction: Esophageal atresia is a congenital pathology that happens 1 in every 4,500 live births. The advances in the last decades in surgical practice, as well as neonatal intensive care, have contributed to the reduction of mortality and morbidity rates.
With the introduction of minimally invasive surgery, the results and prognosis have improved as the learning curve evolves. ?This report aims to show the results in the last decade of the patients treated in our institution. We focus on common and serious postoperative complications after repair of esophageal atresia, such as the appearance of anastomotic leaks, stenosis and recurrent fistula.
Objectives: Establish the main complications in cases from the last 10 years in the thoracoscopic management of esophageal atresia with tracheoesophageal fistula in the Hospital de Emergencias Pediátricas.
Method: A retrospective review of the medical records of patients treated from 2008 to 2018 was performed and the following criteria were reviewed: Surgical age, associated congenital diseases, operative time, anastomotic leak, stenosis, esophageal dilatation and recurrent fistula.
Results: We reviewed the medical records of 77 patients with esophageal atresia operated by thoracoscopy excluding patients with esophageal atresia type I and type V, resulting in a total group study of 58 cases. The average surgical age was 12 days. The associated congenital diseases were: 9 patients with heart disease, 2 with VATERL, 1 with trifurcation of the trachea, 1 with Goldenhar's syndrome, 5 with tracheomalacia, 1 with DiGeorge syndrome, 2 with renal pathology, 5 with MAR, 1 with Down síndrome and 2 with polydactyly.
The average surgical time was 150 minutes (380‐60 minutes), considering that the longest procedures were during the first years. When dividing the total of patients into 2 equal groups, it was found that the averages decreased from 187 minutes (90‐380) for the first group to 109 minutes (60‐180) for the most recent group. In 1 patient, conversion to thoracotomy due to desaturation and bradycardia was decided. Anastomotic leak was found in 9 patients (16%) with spontaneous resolution in all cases. Stenosis was observed in 24 patients (41%), which when compared in a similar way to the operative time, ranged from 61% (16 patients) to 30% (8 patients). The average dilatations were 2 (1‐5) with intervals of one week in severe cases and one month for moderate cases. There was recurrence of esophageal‐tracheal fistula in 4 patients (7%); One of them was resolved with a second intervention by thoracotomy, the other three underwent chemical closure with trichloroacetic acid.
Conclusions: Thoracoscopy is an effective procedure for the treatment of esophageal atresia, feasible to reproduce with equal or better results than the conventional thoracotomy procedure. Although the procedure is not free of complications, the results improve in relation directly proportional to the experience of the surgical group, as demonstrated by the present review.
QS084 THORACOSCOPIC LOBECTOMY: WHAT TO LEARN FROM EARLY EXPERIENCE
Hospital Exequiel González Cortés
Introduction: Thoracoscopic lobectomy has become a safe technique for congenital lung lesions in the peadiatric patients with all the major advantages of minimally invasive surgery. Our aim is to evaluate the results and assess its safety and efficacy as it is becoming the gold standard.
Method: Retrospective study from December 2012 and June 2018. Children who underwent a thoracoscopic lobectomy where included. Demographic data collected were age at surgery, weight and gender. Clinical presentation were:prenatal diagnosis, incidental finding, respiratory symptoms and lung infections. Imaging diagnostic exams were analyzed: prenatal ultrasonography, fetal magnetic resonance and Thorax Computed Tomography. For assessing surgical procedures, we registered operating time, number of ports, intraoperative difficulties, conversion rate, lobe resected and biopsy report. Immediate postoperative outcomes as hospital stay, days with pleural drainage and mechanical ventilation, critical care unit stay and complications where recorded. Long term follow up symptoms were registered.
Results: 22 children had athoracoscopic lobectomy. Average age was 22 months (range 3days‐11years), average weight 14Kg (range 3‐44Kg.). 16/22 patients were asymptomatic: 1 postnatal incidental finding and 15 prenatal diagnosis (13 ultra sonographic diagnosis only and 3 had fetal magnetic resonance available). Most frequent symptomatic presentations where infection 5/22 pneumonia. Respiratory distress of the newborn was present in one patient with congenital lobar emphysema. The lobectomy was performed with 3 ports in 86% patients, 4 ports in 4,5% and 9% with 3 ports and a percutaneous access. Operative time was average 166 min(range 65‐290 min). The conversion rate was 18%(4/22,), due to intraoperative difficulties like lung fibrosis, vascular variants and a finding of an esophageal bronchus. The most frequently resected lobe was the lower left(63%), the upper right(18%), lower right(14%) and the middle lobe(5%). Biopsy results were 17 CPAM(77%), 1 congenital lobar emphysema (4,5%) and 4 lung sequestration (18%, 3 extralobar and 1 intralobar). Mean hospital stay was 6,3 day(range 3‐22), days in the critical care unit were average 2,7(range 1‐6), days with mechanical ventilation were average 0,5(range 0‐2). Pleural drainage time was average 4,8 days(range 1‐22). Postoperative complications were 1 quilothorax, 1 massive hemothorax, 1 fistula and 1 infected pleural effusion. Only 2 major complications underwent reoperation: massive hemothorax required a thoracotomy approach for quick hemostasis and the patient with quilothorax required 3 changes of pleural drainage that were performed in the operating room. Long term follow up range from 4months to 6years. 21/22 patients are asymptomatic and 1 is been treated for asthma but with major improvement of his respiratory symptoms.
Conclusions: Thoracoscopic lung resection approach has a high technical demand. Early resection is important to avoid potential infection and fibrosis that would difficult the procedure with higher intraoperative difficulty. Due to long term efficacy and excellent clinical response especially in functional outcomes, nowadays we consider it the gold standard.
QS085 PRELIMINARY EXPERIENCE OF ROBOTIC SURGERY FOR PEDIATRIC CHOLEDOCHAL CYST COMPARED WITH OPEN AND LAPAROSCOPIC PROCEDURES
Department of Pediatric Surgery, West China Hospital, Sichuan University
Objectives: We reported our preliminary experience on indication, feasibility, safety and complications of treatments of pediatric choledochal cyst using robotic surgery. Surgical outcomes of resection of cyst and biliary reconstruction were compared with both open and Laparoscopic procedures.
Methodology: Patients receiving surgical treatments for choledochal cysts from Jan, 2017 to June,2018 at our institution had been divided into three groups: open surgery, Laparoscopic surgery and robotic surgery. Following parameters were recorded and analyzed: Baseline information including age, weight, diameter of the cyst and degree of inflammation. Clinical characteristics including operation time, bleeding, biliary leakage and strictures and hospital length of stays. Cosmetic effects of children.
Results: A total of 154 patients had been involved in this study including 104 of open group, 38 of Laparoscopic group and 12 of robotic group. The youngest age and lowest weight of robotic group were 6 months and 7.2Kg which were older than the other two groups. Open surgeries had obvious advantages in complicated cases especially in those with inflammation and diameter of common bile duct less than 1.5cm. Mean operative time were: 1.65 hours for open group, 3.7 hours for Laparoscopic group (with four cases of conversions to open surgery) and 3.4 hours for robotic group. Blood loss ranged from 10 to 30 ml in open group and did not differ significantly among three groups. For both open and robotic surgical groups, no biliary leakages or strictures were noted during follow‐ups. There were 11 cases of leakage after Laparoscopic surgeries and 2 case had biliary strictures which needed open re‐operation for corrections. Most of the complications were found in cases with severe inflammation or with diameter of common bile duct less than 1.5cm. Mean lengths of incisions were 4.0 cm in open group, 5 mm in Laparoscopic group and 8 mm in robotic group. Average lengths of hospital stays were 6.3, 5.1 and 5.2 days respectively in open, Laparoscopic and robotic groups.
Conclusions: Open surgeries for treatment of pediatric choledochal cyst were safe and had lower technique demands with little rates of surgical complications. But they had poor cosmetic effects. Laparoscopic surgeries were the most technique‐demanding but had the best cosmetic effects. Rates of surgical complication of laparoscopy were higher but acceptable. Robotic surgery had reduced the technical difficulties of conventional Laparoscopic surgeries and had close precision with open surgical procedures. It was safe and had good cosmetic effects. But medical costs of robotic surgery were high.
QS086 IMPACT OF PNEUMOPERITONEUM WITH CARBON DIOXIDE ON THE KIDNEY BLOOD FLOW IN RABBIT MODEL USING [99MTC] DTPA SCINTIGRAPHY
Campinas State University
Background/Purpose: Increased intra‐abdominal pressure resulting from pneumoperitoneum can cause renal physiological changes, such as oliguria and anuria, in mammals. Although videolaparoscopic surgeries are usual, the occurrence of renal lesions due to these procedures has not been precisely documented in the literature. The aim of this study was to evaluate the impact of pneumoperitoneum on renal flow in an experimental model of rabbits using renal scintigraphy with [99mTc] DTPA (technetium‐labeled diethylene triamine pentaacetic acid).
Materials and Methods: Six healthy New Zealand male rabbits weighing 3 kilograms, previously anesthetized and mechanically ventilated through a tracheostomy tube, underwent to pneumoperitoneum by peritoneal puncture and gas insuflation. Intra‐abdominal pressure was maintained at 15mmHg for 2 hours. Each animal was its own control and analyzed in two different moments: [99mTc] DTPA renal blood flow without pneumoperitoneum (control ‐ 1) and with pneumoperitoneum (2). The animals remained throughout the study under respiratory monitoring by capnography, oximetry and arterial pressure median, followed by euthanasia at the end of the procedure. This study was approved by Ethics Committee on Animal Use of Campinas State University, and the ethical principles for the use of laboratory animals were followed, prepared by SBCAL‐Brazilian Society of Science in Laboratory Animals‐and fully applied their requirements during the validity of this Protocol.
Results: The results were obtained through the scintigraphic images of renal capture and renal clearance of the radiopharmaceutical at the two moments, with the construction of flow images, quantitative and qualitative analysis of the images, evidencing a pattern suggestive of reduced renal arterial flow through determination of [99mTc] DTPA during pneumoperitoneum. Compared to basal condition, all animals presented reduction of renal blood flow (minimum 18% and maximum 84%). The mean [±standard deviation] of renal flow reduction after pneumoperitoneum was 48[±25%].
Conclusions: Pneumoperitoneum induces a significant reduction of the renal blood flow, as determined in this experimental method in rabbits. These data are in agreement with literature, but non‐invasive methods are scarcely used. It is necessary to continue this study, in order to identify precisely at what time and conditions the pneumoperitoneum directly affects, so that this influence can be analyzed quantitatively.
QS087 SHORT TERM OUTCOME OF LAPAROSCOPIC DUODENAL ATRESIA: A MULTICENTER STUDY
1Cairo University, 2San Bortolo Hospital Vicenza, 3Wroclaw Medical University
Background: Laparoscopic Duodenal Atresia has evolved over the past years after primarily reported by Steve Rothenberg in 2002. Studies have shown comparable results to open surgery with lower morbidity and shorter recovery time and hospital stay and superior cosmesis.
The purpose of the study is to compare the outcomes of patients with Duodenal Atresia across the three Neonatal MIS centers with different level of expertise.
Methods: Retrospective study of cases collected from 3 Neonatal MIS centers performing Laparoscopic Duodeno‐duodenostomy. Data included demographic, operative and postoperative to discharge.
Results: Thirty two cases (n = 9,12,11) were included in the study with subgroup analysis of each center. There were zero mortalities. Patients were followed for at least 6 months postoperatively. Mean gestational age: 36.14 weeks, mean weight on admission: 2306.5g, 48% males and 72.4% full‐term cases. Mean operative time:154.3 minutes, 3 conversions to open surgery and no operative complications. Median time to start oral feeds was 5 days postoperatively and 17.2 days to complete discharge.
Conclusion: Laparoscopic Duodeno‐duodenostomy for Duodenal Atresia operative and postoperative results are comparable between centers of Neonatal MIS with different experience.
QS088 RADIOLOGIC IMAGE GUIDED TUBE STOMA INSERTION IN NEONATAL SHORT BOWEL SYNDROME: FIRST CASE IN THE LITERATURE
Sidra Medicine
Surgical short bowel syndrome(SBS) in neonate is the most common cause of intestinal failure which is defined as a significant reduction in the functional gut mass below a critical threshold necessary to maintain growth, hydration and/or electrolyte balance. Necrotizing enterocolitis (NEC) is the most common cause of SBS in neonates followed by gastroschisis, intestinal atresia and intestinal malrotation/volvulus. The management of SBS patients is complex and needs a multidisciplinary approach. Advances in medical management and liver salvageable total parenteral nutrition (TPN) have significantly improved the outcome of these patients. In addition to, enhancement in bowel expansion and length via different surgical techniques which have been integrated with medical management to provide promising approach to such kind of vulnerable patients. Controlled tissue expansion programe (CTE) is applied for patient with short bowel in order to increase the length and circumferential diameter of the bowel over a period of time. This makes a new and greater surface area for absorption and more tissue for lengthening and tailoring. CTE is done via clamping tube stoma which is created surgically via inserting either malecot catheter or later on once the tract becomes mature a Foley catheter into proximal and distal stoma sites. These tubes associated with frequent risk of dislodgement and exposing patients for further surgical procedure with risk of losing more bowel length. So in this paper we describe a new technique used in CTE to avoid and manage such a compilation of these catheters via less invasive approach of image guided procedure.
QS090 RECURRENCE OF CONGENITAL DIAPHRAGMATIC HERNIA AS A POST SURGICAL COMPLICATION
National institute of children health
Purpose: Operative approach in the repair of congenital diaphragmatic hernia (CDH) is variable, including open thoracic or abdominal approach, thoracoscopic and laparoscopic approach. Post operatory complications such as recurrent hernia in the short term and long term are described. We evaluated the recurrence of infants with CDH as a post‐surgical complication with different approach and the associated factors.
Methods: Cross‐sectional study collected data from infants with CDH were analyzed from January 2015 to August 2018. Recurrent hernia was defined as reoperations during initial hospitalization or posterior. Operative approaches included abdominal, thoracic, laparoscopic, and thoracoscopic techniques. Complications included short‐term recurrent hernia.
Results: Of the 35 patients identified with CDH, 28 met the inclusion criteria. 15 patients were female and 13 male. The most frequent age group was found between the month of life and 2 years. 14 patients (50%) underwent minimally invasive techniques (MIS) repairs with 4 reported recurrences, of them, the thoracoscopy approach had more recurrence (37.5%) than laparoscopy (12.5%), compared with 4 for open techniques, which included the approach by laparotomy and thoracotomy, each with 25%. Finding whit these data an association between the type of approach and the risk of recurrence (p < 0.00). Emergency surgeries reported more recurrences (62.5%) compared with elective surgeries (37.5%). Patients with associated heart disease had a higher recurrence rate (62.5%) than those who lack associated heart disease (37.5%).
Conclusion: Recurrence was the most common complication after CDH repair. The thoracoscopic approach had a higher recurrence rate; probably associated with the learning curve of surgeons who use this technique, the condition of the patient in underdeveloped countries where the patient's nutrition is an important factor, the association with other comorbidities also influence the surgical results. Likewise, a greater recurrence was determined in emergency surgery, and in patients with associated cardiac pathology. A study with a larger sample is required to extrapolate the data obtained in this study and be able to perform interventions to reduce the risk of recurrence in the postoperative period of these patients.
Keywords: Congenital diaphragmatic hernia, minimally invasive surgery, thoracoscopy, thoracotomy, laparoscopy, laparotomy and recurrence
QS091 OUTCOME OF ROBOTIC‐ASSISTED REDO‐SURGERY AFTER FAILED FUNDOPLICATION IN CHILDREN AND ADOLESCENTS
1Department of Pediatric Surgery, University Medical Center of the Johannes Gutenberg Universtiy Mainz, Germany, 2Department of Surgery, University Medical Center of the Johannes Gutenberg Universtiy Mainz, Germany
Background: Failed fundoplication is not unusual in pediatric population, especially when the Fundoplication was performed in very young age, as the tissues may wear and stretch with time and patient growth. Redo‐surgery in such cases can be challenging due to adhesion formation and altered anatomy. This may justifies the need for more advanced equipment such as robotic assistance using a telemanipulator. However, data on the outcome of such redo surgery in children are scarce Purpose: To describe our experience with robotic‐assisted redo‐surgery after failed fundoplication in children and adolescents.
Methods: All patients over 10 years of age with failed previous fundoplication were operated using a telemanipulator system (Da Vinci Xi robotic system Intuitive, Sunnyvale, CA, USA). Preoperative workup for included a contrast swallow study, and pH‐probe with or without esophageal manometry. Intra‐ and postoperative complications were recorded, and the patients were followed up for resolution of symptoms.
Results and Discussion: Three patients underwent redo‐surgery using robotic‐assisted technique. Adhesiolysis was performed in all cases, followed by complete Nissen re‐fundoplication in two. In one patient, a re‐hiatoplasty was performed without a re‐fundoplication. No intraoperative complications were reported. Mean operative time was 158 minutes, full oral diet was achieved within 24h, and the mean length of stay was 2 days. At 3 months follow up, 2 patients had still dysphagia and one patient suffered from a esophageal ulcer. All patients with symptoms at follow‐up received a contrast swallow study that showed intact fundoplication.
Conclusion: Robotic assisted redo surgery after failed fundoplication is an alternative to the conventional laparoscopic procedure that adds 3‐dimensional vision and increased instrument range‐of‐motion. Our limited patient collective experienced a relatively high rate of postoperative dysphagia not seen in our previous conventional laparoscopic experience. These findings should be critically appraised in prospective studies before robotic re‐fundoplication can be universally recommended in pediatric patients. These postoperative results may not depend on the surgical laparoscopic technic per se, but may result from preexisting pathology and long‐term alterations of lower esophageal physiology. On the other hand, the lack of haptic feedback and early learning curve may explain the findings in our patients.
QS092 QUALITY OF LIFE IN PATIENTS WITH ESOPHAGEAL ATRESIA MANAGEMENT UNDER THORACOSCOPIC APPROACH
1Hospital San Juan de Dios, 2Clinica Las Condes
Since the introduction of thoracoscopy in pediatric surgery, the classic surgical technique for esophageal atresia (EA) was adapted, resulting in less postoperative pain and superior cosmetic result. We evaluate the outcomes and the quality of life (QOL) of patients with EA under procedures with minimally invasive surgery (MIS).
Methods: All cases from a single general institution which underwent MIS over a 6 year period were reviewed. Operative details and complications were examined. PedsQL TM (Pediatric Quality of Life Inventory) was applied to the patients parents.
Results: 14 patients were included. 13 of them had a distal fistula and 1 was without fistula.
In 11 patients fistula ligation and primary esophageal anastomosis was performed, in 1, due the low weight (900 g) and the severe condition of the patient, only a fistula ligation and gastrostomy was performed. The 2 patients with a long gap (the first with distal fistula and the second without fistula) were managed with initial pouch alignment with thoracoscopic stich and a delayed esophageal anastomosis.
The mean gestational age was 35 weeks (28‐41), birth weight 2459 grams (900‐4015). Only 4 of them had antenatal diagnosis. Regarding the morbidity, 6 had VACTER Association, 2 had central nervous system malformations, 2 had any trisomy (Down syndrome, Edwards Syndrome) and 1 had bronchopulmonary dysplasia.
The mean operative time was 2,7 hours (2‐4) and all of the patients used a pleural tube. They were fed after 12 days (4‐29).
No cases required conversion. In this series, only the patient with Edward Syndrome passed away.
In the early outcomes, 1 patient required a reoperation, due an anastomotic leak. 3 developed pneumothorax and 2 chylothorax, and needed management under thoracic tube. In the medium and long outcomes, 7 patients developed stenosis and required endoscopic dilatations (mean 4, 1 up to 12). In 2 patients Nissen procedure was performed. One of them had an Hiatal Hernia and the other had gastroesophageal reflux.
The patients have been followed from 1 year up to 6 years. They were contacted and 57% reported no troubles with feeding by mouth, 29% some difficulties and in 2 patients (Down Syndrome and broncopulmonary dysplasia) were being fed by gastrostomy tube.
Regarding the quality of life measure, the mean score for PedsQL TM was 76 (PedsQLTM Score 0‐100; where higher score indicates better quality of life). The lowest score (17) belongs to a patient with a severe pulmonary dysplasia, who requires permanent ventilation support.
Conclusion: The thoracoscopic approach is a safe alternative in patients with EA, with excellent exposure and visibility of anatomic landmarks and little associated morbidity.
This group has a good QOL, except for the patient who has an associated condition. In this case the QOL is influenced by the patient's morbidity.
Further collaborative studies are needed to know if the surgical aproach has any influence on the QOL of the patients with this condition.
QS093 THE EFFECT OF 3D VERSUS 2D VISION ON TECHNICAL PERFORMANCE IN A VIRTUAL ROBOTIC SURGERY SIMULATOR CURRICULUM
Pediatric Surgery, Johannes Gutenberg University of Mainz
Background: Three‐dimensional (3D) vision has been the standard for robotic‐assisted surgery since its introduction. Recently, 3D optics have been becoming increasingly available for laparoscopic and thoracoscopic surgery as well. While metaanalyses of clinical studies have shown advantages in terms of shorter operative times and less blood loss [1,2], the underlying advantages for the surgeon have not been analyzed in detail. Some visual adverse symptoms, such as focusing were actually more prevalent with 3D vision [3].
Purpose: This study quantitatively compares the effects of 3D to conventional two‐dimensional (2D) laparoscopic vision during standardized exercises on a virtual robotic simulator, focusing on technical performance and manual dexterity.
Methods: A cohort of 25 advanced medical students interested in surgery performed standardized exercises (Pick and Place (Figure 1), Ring Walk, Stacking Challenge) on a robotic simulator (dV Trainer, Mimic Technologies, Seattle, WA, USA). In order to account for the learning curve, the exercises were performed with six repetitions, alternating between 3D and 2D optics three times. The participants were randomized to start either with 3D optics or 2D technique. The system gave a detailed report card on performance after each exercise, including time to completion (seconds), economy of motion (centimeters), master workspace range (centimeters), and other factors, all integrating into an overall score. Parameters were statistically compared between 2D and 3D vision.
Results: Overall, exercises were performed faster, with less instrument collisions and episodes of instruments out of view, as well as a better manual performance when 3D vision was employed. The Overall Score was also significantly higher with 3D optics than with 2D for all exercises (Pick and Place p = 0.0023, Ring Walk p = 0.00052, Stacking Challenge p = 0.0008).
Conclusions: This study shows that 3D vision leads to faster completion of tasks, better manual dexterity, less errors, and improved overall performance on a virtual robotic simulator. These effects may translate into more efficient surgical performance and less complications in the clinical setting. Therefore, 3D endoscopic surgery should become the standard in the future. Medical device companies should particularly focus on developing miniature systems of 5mm diameter and smaller for pediatric surgery.

Literature:
1. Liang H, Liang W, Lei Z, Liu Z et al. Three‐Dimensional Versus Two‐Dimensional Video‐Assisted Endoscopic Surgery: A Meta‐analysis of Clinical Data. World J Surg 2018 [Epub ahead of print].
2. Dirie NI, Wang Q, Wang S. Two‐Dimensional Versus Three‐Dimensional Laparoscopic Systems in Urology: A Systematic Review and Meta‐Analysis. J Endourol 2018;32:781‐790.
3. El Boghdady M, Ramakrishnan G, Alijani A. A study of the visual symptoms in two‐dimensional versus three‐dimensional laparoscopy. Am J Surg 2018 [Epub ahead of print].
QS094 TRACHEOESOPHAGEAL FISTULA REPAIR IN PATIENT WITH COMPLEX CONGENITAL ANOMALIES
Morgan Stanley Children's Hospital‐Columbia University
Background: We report a case of right sided thoracoscopic repair of esophageal atresia and distal tracheoesophageal fistula (EA/TEF) in a baby with multiple congenital anomalies including vascular ring and choanal atresia. The ideal timing and strategy for repair of these simultaneous entities remains unclear; no reported cases in the literature have specifically address timing of repair. Two prior reports of synchronous choanal atresia and EA/TEF describe repair of both anomalies in the same operation shortly after birth.
Case Presentation: On prenatal evaluation the fetus was found to have polyhydramnios and concern for vascular ring on fetal echocardiogram. The patient was born at 35 5/7 weeks via cesarean section in the setting of maternal chorioamnionitis. At delivery, the patient developed respiratory distress and was orally intubated after failure of passage of the endotracheal tube through the nares. In addition, a nasogastric tube was unable to be advanced beyond 11cm. Cross sectional imaging with angiography demonstrated a vascular ring comprised of a right sided aortic arch, aberrant left subclavian artery, and a large patent ductus arteriosus. Esophageal atresia was also demonstrated. Otolaryngology evaluation confirmed the diagnosis of choanal atresia. We repaired the EA/TEF on day of life three via right thoracoscopy (despite right sided arch) to preserve the left thorax for the possibility of subsequent ligation of large PDA. Because choanal atresia repair requires manipulation and extension of the neck intraoperatively and subsequent deep suctioning postoperatively, we elected to postpone the repair of the choanal atresia until the esophageal anastomosis had healed. On postoperative day six we performed an esophagram that confirmed no leak from the anastomosis. The choanal atresia repair was performed on postoperative day eight. The patient failed to wean from mechanical ventilation post operatively and eventually developed hemodynamic instability secondary to shunting across the large PDA. One week after her choanal atresia repair she underwent left thoracotomy and ligation of her PDA along with aortopexy. The patient recovered from these surgeries well and was tolerating full enteral feeds on room air by one month of age.

Conclusion: We propose this staged approach to repair of the patient's synchronous, complex anomalies, as a strategy to minimize complications.
QS095 MASTERY LEARNING SERIES™: EVALUATION OF BASELINE INTRACORPOREAL SUTURING SKILLS AND SUMMATIVE PROCEDURE‐SPECIFIC PERFORMANCE
1Ann and Robert H Lurie Children's Hospital of Chicago, Chicago, Illinois, USA, 2University of Cincinnati, Cincinnati, Ohio, USA, 3Hospital Garrahan, Buenos Aries, Argentina, 4Medical University of Graz, Graz, Austria, 5Emory University, Atlanta, Georgia, USA, 6University of Texas, Southwestern, Dallas, Texas, USA, 7Kinderspital Luzern, Luzern, Switzerland
Background: Mastery Learning (ML) is a rigorous method of competency‐based education whereby all learners are expected to acquire cognitive, technical and professional skills, without regard to the time in which these achievements take. ML was first implemented in 2017 at the IPEG Annual Congress, and these data represent the second iteration of this advanced simulation‐based course. The purposes of this study were to 1) define participants' baseline intracorporeal suturing skills, and 2) report summative procedure‐specific scores for thoracoscopic pulmonary lobectomy (tLobe) and tracheoesophageal fistula repair (tTEF), as simulated during the Mastery Learning Series™.
Methods: After IRB exemption, 30 participants attended a ML course for tLobe and tTEF at the 2018 IPEG Annual Congress. Participants were evaluated for baseline laparoscopic suturing skills, as well as summative performance metrics for tLobe and tTEF. The 9‐hour course included both didactic and hands‐on simulation sessions. Participants were evaluated for baseline intracorporeal suturing skills, followed by intensive didactic and hands‐on training in tLobe and tTEF. After completing the course, faculty assessed each participant for global and procedure‐specific performance measures, and debriefed these data with each participant. Descriptive statistics are reported as means with standard deviation (range, minimum – maximum possible scores).
Results: The average score for the baseline suturing assessment was 22 ± 4.6 (range 14–32, min 6 – max 34). Of the 30 participants, 77% (23/30) were able to complete the first square knot without gaps and 63% (19/30) were able to complete two square knots without gaps. For tLobe the average global skills score was 24 ± 5.2 (range 12–34, min 12 – 36) and the procedure‐specific summative performance score was 31 ± 6.9 (range 15–45, min 9 – max 45). For tTEF the average global skills score was 21 ± 4.5 (range 12–27, min 8 – max 32) and the procedure‐specific summative performance score was 20 ± 4.3 (range 12–29, min 6 – 30).
Conclusion: The majority of participants were able to perform portions of each of the procedure‐specific tasks, however at varying degrees of proficiency, as indicated by the variability in summative procedure‐specific scores. These data serve as a benchmark for participants to better understand their current knowledge, skills and attitudes that are necessary to successfully implement these procedures within the clinical environment. As the curriculum continues to mature, and as participants return to advance further in their performance, we seek to ultimately develop the knowledge, skills and attitudes so that these participating surgeons can safely implement advanced surgical procedures within their home clinical environments.
QS096 FACTORS AND CAUSES RELATED TO CONVERSION OF MINIMALLY INVASIVE SURGERY IN A PEDIATRIC HOSPITAL
uniVERSIDAD NACIONAL DE COLOMBIA
Introduction: The use of minimally invasive techniques in pediatric surgery has increased dramatically in recent years and is now the standard of care for various surgical conditions. Some of the advantages are the development of fewer adhesions and scar tissue, lesser postoperative pain and better aesthetic results. In our institution we have seen an increase in minimally invasive procedures in the last years, with some of the procedures requiring intraoperative conversion to open surgery.
Objective: To characterize the preoperative factors, intraoperative causes and outcomes in pediatric patients taken to a minimally invasive procedure converted to open surgery in our institution.
Materials and Methods: This study was carried out as a single‐ institution retrospective chart analysis of all patients who underwent minimally invasive surgery between 2009 and 2017 requiring conversion to open surgery. Preoperative factors, time of evolution of the disease, cause of conversion, rate of conversion and postoperative outcomes were recorded.
Results: We included one hundred and fifty‐four patients in this eight‐year study, 89.6% were laparoscopic and 10.34% were thoracoscopic procedures. The mean age was 8.5 years with a male gender prevalence (53.9%). The most frequent primary cause leading to surgery was not oncologic and a dirty‐contaminated wound was found in 49.35%. 38.9% of our patients were ASA 3 followed by ASA 2 (36.36%). About the preoperative laboratory tests, we found an elevated INR (mean 2,04), hypoalbuminemia (mean 2,8) and high inflammatory response markers (leukocytosis, neutrophilia and high CRP).
The principal cause of conversion was failure in the progression of surgery (53.25%) followed by loss of anatomic reference (24.5%). Not controlled incidental lesion and not controlled bleeding was reported as the cause of conversion in 11% of patients each.
With regard of the outcomes, 44.16% of the patients required intensive care unit (ICU) postoperatively, most patients didn't required reintervention (70%) and the mortality rate was 0.65%. Through the years the number of minimally invasive procedures increased, and the percentage of minimally invasive procedures converted decreased (1,7% in 2017) which can be attributed to our surgeons gaining experience with minimally invasive techniques.
Conclusion: Conversion of minimally invasive surgery is a decision the surgeon must make in different scenarios. In our study the main causes of conversion to open surgery was failure in the progression of the procedure, in concordance with other reports in the literature. Other frequent variables were altered preoperative laboratory tests such as INR, albuminemia and inflammatory response markers. In our population most patients were classified as ASA 3, consistent with the fact that our institution is a reference center for complex diseases, had preoperative higher risk and therefore relate with the percentage of postoperative requirement of ICU. Our reintervention and mortality rate were acceptable. In this study it is not possible to determine risk variables associated to conversion, but we were able to describe related factors. We intend to promote a prospective study with a control group.
QS097 LAPAROSCOPIC MANAGEMENT OF FRANTZ‐GRUBER (PANCREATIC) TUMORS IN CHILDREN
Hospital Araujo Jorge
Introduction: The solid pseudopapillary tumor (SPT) of the pancreas (Frantz‐Gruber tumor) is an uncommon tumor in the pediatric population, but one of the most common solid tumors in children, usually after the age of 10 years. It is most frequently diagnosed in the third decade of life and the most frequent symptom of these tumors is upper abdominal pain. An increasing important presentation has been the incidental finding on ultrasound or tomographic scans performed for other reasons. Since the first laparoscopic pancreatic operations 20 years ago, conventional open laparotomies are still the gold standard approach, and there are only 5 reports of more than one laparoscopic resection of SPT in children and adolescents. Our aim is to shown our experience in a series of 6 pediatric patients with different presentations of SPT, treated laparoscopically.
Patients and methods: From Jan/2005 to March/2017, 7 patients aging 9‐15 years old (median 12.6), 5 girls and 2 boys with pancreatic solid tumors, underwent laparoscopic procedures and were found to have SPT. Abdominal pain was the main symptom (n = 5, vomiting in 1), and in 2 girls the mass was incidentally found on computed tomography for spine trauma and complicated pneumonia. One came with recurrence after a laparotomy elsewhere. Two had a previous diagnosis after percutaneous biopsy. All operations were performed using 3 ports (10‐mm, 2x 5‐mm), a umbilical scope, and the procedures included distal pancreatomy preserving the spleen (n = 2), corpus‐caudal preserving the spleen (n = 1), corpus‐caudal with splenectomy (n = 1), enucleation with margin at the head of the pancreas (n = 1), multifocal metastatic resection (n = 1). The specimens were withdrawn through the umbilical port (n = 3) or through a limited Pfannenstiel incision (n = 3). Vascular management used ultrasonic shears or bipolar cautery, or propylene ligations, and green 60‐mm staplers for distal pancreatectomy. No clips were used.
Results: All the procedures could be performed without conversions, transfusions, and there was no complication due to the laparoscopic approach. After a follow‐up period of 1.5‐13 years (mean 8.5 years), there was no recurrence, even the case that already had it. The mean hospital stay was 2.5 days (2‐4), the patients had few pain and were satisfied with the tiny cosmetic scars.
Conclusions: The laparoscopic resections and enucleations of SPT of the pancreas in children are feasible, safe and can be oncologically satisfactory, whatever the location of the tumor, with or without splenectomy, and for the resection of metastatic lesions, with the advantages of minimally invasive surgery.
QS098 LAPAROSCOPIC/ROBOTIC MANAGEMENT OF ACHALASIA CARDIA: EXPERIENCE WITH 5 CASES
PGIMER Chandigarh
Achalasia cardia (AC) is a relatively uncommon condition in pediatric age group. The predominant clinical presentation is dysphagia. The location of gastro‐esophageal junction is easily approachable by minimal access approach. We present our experience with 5 cases of AC treated by MAS including robotics. The technique and outcome is discussed.
Patients & Methods: Their predominant clinical presentation was dysphagia to solids with off and on vomiting. 3 patients had severe weight loss. All patients had contrast esophagogram. Esophageal manometery was done in 2 patients. All patients were under long term treatment with pediatric gastroenterologist and underwent multiple esophageal dilatations. Patients underwent laparoscopic Heller's esophagomyotomy (LHE) with Do'r fundoplication. In the later part of study with the availability of Da Vinci surgical system remaining patients underwent the same procedure robotically. The patients were followed clinically in post‐operative period. A radio nucliede GER scan was done only if the patient was symptomatic for reflux.
Results: 5 patients (3 females) were studied. Mean age 5.5 years. Esophagogram showed bird's beak appearance in all patients. Esophageal manometery was done in 2 patients by treating physician which showed high pressure LES zone and failure of relaxation. First 2 patients underwent LHE and Do'r fundoplication with 5 ports. Later 3 patients underwent the same procedure robotically by Da Vinci Surgical system with 4th arm deployment for liver retraction. A long myotomy was done after esophageal mobilization. Post operatively patients tolerated oral feeds from day 2 onwards. Mean follow up duration is 2 years and none of the patients needed any endoscopic intervention. No follow up GER nuclear scan was done as the patients were not clinically symptomatic for reflux.
Conclusion: Laparoscopic Heller's myotomy is ideal for Achalasia cardia. Use of robot further simplifies the procedure. Once effective myotomy is done these patients do well in long term with no requirement for dilatation.
QS099 3D PRINTED MULTIPLE SKILLS TRAINING SIMULATOR: DEVELOPMENT AND PRELIMINARY VALIDATION
Fundación Hospitalaria
Background: Simulators are emerging with the development of medical engineering technology. Using the MTBOX1, already presented, we extended our resources with a 3D Printed Simulation Tray that can be loaded with exchangeable models, used for essential laparoscopic skills training.

Objective: The aim is to describe the baseline experience and self‐reported evaluation of the usefulness of this single simulator with exchangeable models as a resource for multiple skills training amongst surgeons with different expertise levels.
Methods: The study enrolled 33 surgeons who were stratified in three groups according to their levels of experience and number of cases performed laparoscopically. G1: novice (<10), G2: intermediate (10‐60), G3: expert (<60).
The MTBOX1 universal simulator box with a multifunctional tray to support the models, is manufactured with polypropylene and 3D printed parts, covered in thermoformed EVA foam simulating the abdominal wall of a small infant. (Fig.1) Five models were used to perform different exercises with measurable objectives to accomplish within a limited time frame. (Fig. 2)
E1: transference (acrylic Mandala model)
E2: dissection (self‐supporting gel and silicone vessels model)
E3: extracorporeal nots (acrylic bars model)
E4: suture and intracorporeal nots (silicone pad model)
E5: resection and tubular suture (silicone bowel model)
2/0 Prolene, 5/0 PSD, 5/0 vicryl sutures and 5mm laparoscopic surgical instruments were provided.
The validity of the model was assessed by a 17 item questionnaire. Q1‐9 evaluated its capacity of testing and training and Q9‐17 its relevance of actual laparoscopic surgery. The score of each exercise was obtained by dividing the time to finish the exercise by the number of objectives effectively accomplished.
The correlation between surgical experience and the level of exposure to laparoscopy was evaluated, and the scores of the different groups were compared.
Results: Participants gave a favorable opinion about the MTBOX1 and multifunction tray without inter‐group differences. In G1–G3, the scores correlated with the level of previous exposure to laparoscopic procedures, more‐experienced participants achieved better results than less‐experienced participants.
Conclusion: The data demonstrate the validity of the MTBOX1 and multifunction tray model, suggesting that it can be a useful tool for training and evaluation of laparoscopic procedures.
QS100 DYNAMIC COMPRESSION BRACING FOR TREATMENT OF PECTUS CARINATUM SIGNIFICANTLY INCREASES PATIENT CLINIC ENCOUNTERS
Texas Children's Hospital
[Figure 1. Trend of monthly patient encounters for pectus carinatum before and after introduction of dynamic compression bracing.]

Background: Dynamic compression braces are adjustable braces used for the treatment of pectus carinatum that allow providers to set the pressure of correction applied during treatment. This necessitates a change in the treatment protocol used compared to standard orthotic bracing. The objective of this study was to review the effect of dynamic compression bracing on patient clinic volumes at a single institution.
Methods: In October 2016 we initiated the use of dynamic compression bracing for the treatment of pectus carinatum at a tertiary‐care children's hospital. As part of this new treatment we established a protocol where patients underwent an initial consultation during which the patient was measured for the brace if dynamic compression bracing was recommended. Patients then underwent a subsequent visit for initial brace fitting followed by monthly visits for brace adjustment until complete correction of the pectus carinatum. After complete correction of the pectus carinatum patients were weaned off the brace over the next three months. In this study we performed a retrospective review of all patients seen for pectus carinatum from December 2014 – July 2018. In the first 22 months of the study period patients were treated with standard orthotic bracing by an outside vendor. In the latter 22 months of the study period patients were treated with dynamic compression bracing under our new treatment protocol. Patient volumes were compared between the two cohorts.
Results: There were 1134 total patient encounters and 482 unique patients with a diagnosis of pectus carinatum from December 2014 – July 2018. In the 22 months prior to introduction of the dynamic compression brace there were 334 encounters for 224 unique patients referred for standard orthotic bracing by an outside vendor. During the 22 months after introduction of the dynamic compression brace there were 800 encounters for 258 unique patients. This represents a 140% increase in total encounters and a 15% increase in unique patients in less than 2 years. In addition, the median number of encounters seen per month increased from 15 (IQR, 13‐17) to 32 (IQR, 25‐43) [p < 0.01]. The trend of increasing patient encounters is shown in Figure 1.
Conclusion: Dynamic compression bracing requires routine follow‐up for ongoing brace adjustments throughout treatment. This type of treatment protocol results in a rapid significant increase in patient encounters and necessitates institutional planning for allocation of resources to meet the demand.
QS101 BIOLOGIC MESH UNDERLAY IN THORACOSCOPIC PRIMARY REPAIR OF CONGENITAL DIAPHRAGMATIC HERNIA CONFERS REDUCED HERNIA RECURRENCE IN NEONATES
Emory University
Biologic Mesh Underlay in Thoracoscopic Primary Repair of Neonatal Congenital Diaphragmatic Hernia Confers Reduced Hernia Recurrence.
Purpose: The purpose of this study was to determine if addition of biologic mesh underlay during thoracoscopic congenital diaphragmatic hernia (CDH) repair would decrease hernia recurrence rates.
Methods: We performed a retrospective review for all primary CDH repairs utilizing a thoracoscopic approach between 1/1/2003‐6/31/2013. Inclusion criteria were all CDH patients repaired primarily with or without a biological mesh underlay. A minimum 5 year follow up was deemed necessary to exclude recurrence. The cumulative annual hernia recurrence as well as other demographic factors was analyzed.
Results: Within the study period, forty‐six patients were identified that met study criteria. Three patients were lost to follow up. Fifteen of the remaining patients (15/43: 34.9%) had a biologic underlay. Within the cohort, seven recurrences were noted (7/43; 16.7%). One out of 15 mesh underlay patients experienced a recurrence (6.6%). This was clinically silent and was discovered incidentally during another laparoscopic procedure. Six of 28 primary repairs without mesh recurred (21.4%). Four recurrences occurred within the first post‐operative year, and all occurred by the third post‐operative year.
Conclusions: Thoracoscopic primary repair of CDH can be successfully performed in select patients. The use of a biologic underlay in this subset of patients may protect against recurrence; however, our sample size was too small to show this. We recommend a multi‐institutional study of recurrence rates with biologic mesh underlay.
QS102 WHEN ARE THE TRAINEES READY TO TRANSFER SKILLS FROM LAB TO THE OR?
1Life and Health Sciences Research Institute (ICVS), School of Medicine, University of Minho, 4710‐057 Braga, Portugal. ICVS/3B's‐PT Government Associate Laboratory, 4710‐057 Braga/Guimarães, Portugal. Pediatric Surgery, University of Szeged, Szeged, Hungary. Institute of Surgical Research, University of Szeged, 6725 Szeged, Hungary, 2Life and Health Sciences Research Institute (ICVS), School of Medicine, University of Minho, 4710‐057 Braga, Portugal. ICVS/3B's‐PT Government Associate Laboratory, 4710‐057 Braga/Guimarães, Portugal. Department of Pediatric Surgery, Hospital de Braga, 4710?243 Braga, Portugal., 3Life and Health Sciences Research Institute (ICVS), School of Medicine, University of Minho, 4710‐057 Braga, Portugal. ICVS/3B's‐PT Government Associate Laboratory, 4710‐057 Braga/Guimarães, Portugal., 4Institute of Surgical Research, University of Szeged, 6725 Szeged, Hungary
Introduction: Proper laboratory skill training is highly recommended before conducting human minimally invasive surgery. Among the forms of training, laparoscopic surgery on live animal is likely the most appropriate method to simulate real surgical scenarios.
Aim: The goal was to create a completely standardized duodenum atresia repair model in rabbits by which learning curves can be compared, and the number of interventions necessary for a successful human application can be defined.
Materials and Methods: Two groups of surgeons were involved with advanced and beginner laparoscopic surgeons with 7 and 8 participants, respectively. In the advanced group, pediatric surgery fellows with previous experience of laparoscopic procedures in humans were recruited. The beginners did not have any previous experience with minimally invasive surgery, but underwent a basic systematic box‐trainer training for at least 12 hrs with the same supervisor in a preparatory period. To compare the groups, the participants were invited to perform laparoscopic diamond‐shape duodeno‐duodenostomy on anesthetized New Zealand rabbits (2500‐3000 g bw) by 8 times. Surgery time and anastomosis quality (leakage) were statistically compared using two‐way RM ANOVA analysis followed by the Holm‐Sidak test.
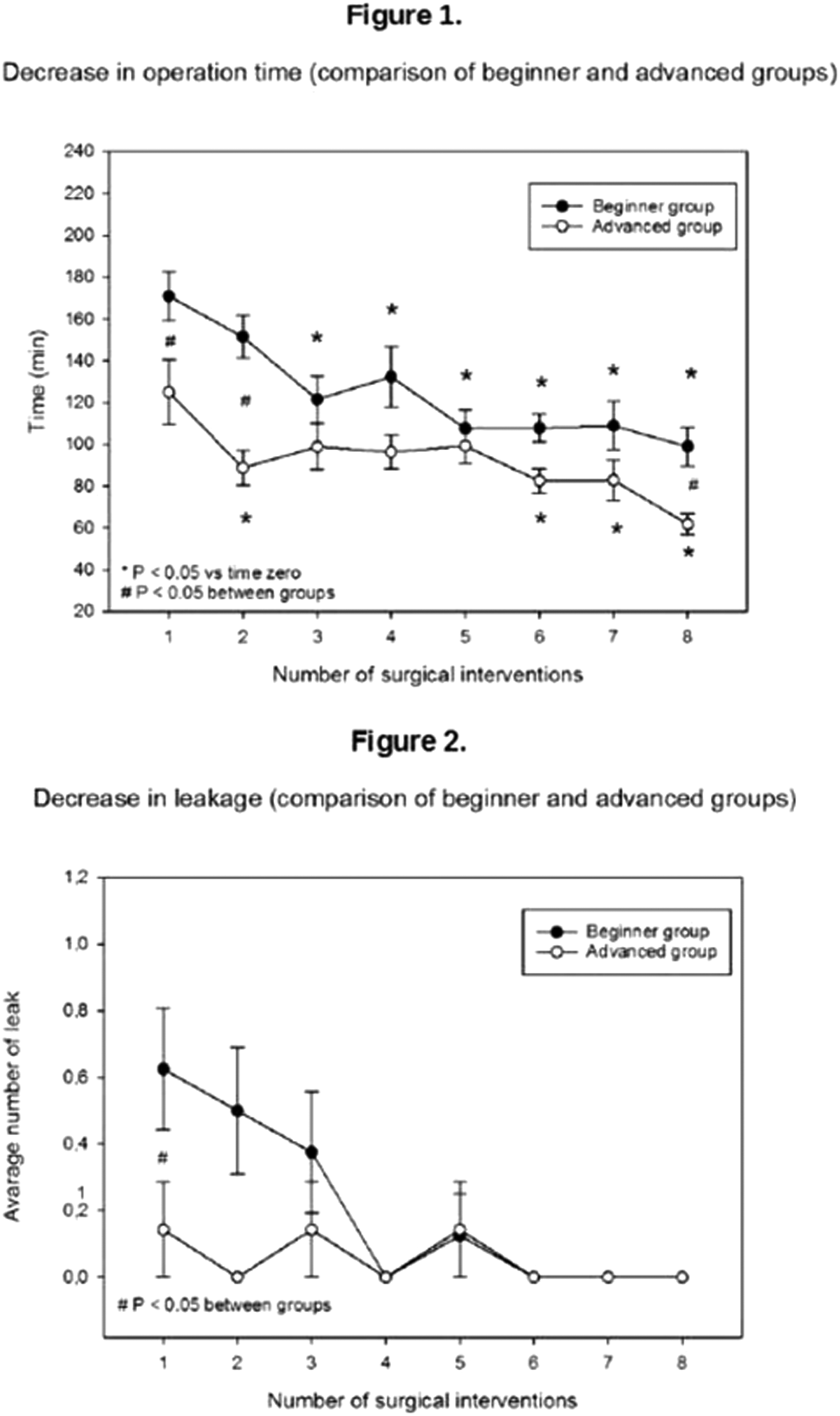
Results: The duration of the first operation was significantly lower in advanced group (125 ± 41 min, and 170 ± 33 min, respectively, P < 0.05). The surgical time significantly improved from the third operation onwards, and reached similar values in both groups later on (see figure 1). This parameter reached a plateau by the fifth surgery in beginner group, but the improvement continued in the advanced group until the last surgery. Leakage rate was also significantly lower in advanced group (1/8 and 5/7, respectively, P < 0.05) after the first operation which was followed by a dramatic improvement in the beginner group also. Starting from the sixth session, no leakage was detected in any of the groups (see figure 2).
Conclusion: All of the trainees showed improved laparoscopic skills during the repetitive exercise involving a highly advanced neonatal laparoscopic approach. Our results suggest that after a basic skill training, at least 5 laboratory training sessions are needed on live animals (for this type of surgery). This should be performed to attain the skills that likely enable the participants to carry out the procedure in humans.
QS103 DEVELOPMENT OF HIGH FIDELITY TRAINING SIMULATOR OF LAPAROSCOPIC SURGERY FOR CHOLEDOCAL CYST AND BILIARY ATRESIA
Department of Pediatric Surgery, Research Field in Medicine and Health Sciences, Medical and Dental Sciences Area, Research and Education Assembly, Kagoshima University, Kagoshima, JAPAN
Background and Aim: Recently, laparoscopic surgery for choledocal cystandbiliary atresia has become popular in the pediatric field in light of these procedures' approval for coverage under the national health insurance system by the government in Japan. However, the number of cases performed per institution is limited, so standardizing and improving these techniques with the accumulation of cases is difficult. Therefore, the development of a high‐fidelity simulator reproducing a disease‐specific surgical procedure and facilitating training using simulators is important for young pediatric surgeons. We developed a simulator of laparoscopic hepatico‐jejunostomy for congenital biliary dilatation and laparoscopic portoenterostomy (Kasai's procedure) for biliary atresia.
Materials and Methods: We developed these model through industry‐university cooperation with Kyoto Kagaku Co., Ltd. A pneumoperitoneum body model of a one‐year‐old infant was reproduced using computed tomography (CT) data and the body surface data measured with a three‐dimensional scanner (Figure 1a). The organ models inside the simulator were produced using urethane and styrene materials. Surgeons in training can change the port layout according to their preference (Figure 1b).
Results: Choledocal cyst model: This model was mainly made for laparoscopic hepatico‐jejunostomy. The intestines and bile duct are organs that are grasped directly with forceps. The texture of these organs is therefore important for performing suturing operations, so the size, softness, stretch, and color were thoroughly considered. Figure 2ashows our clinical case of hepatico‐jejunostomy in a one‐year‐old girl. We sometime use the technique of suspending the anterior wall of the hepatic duct to visualize the anastomotic site clearly and facilitate needle driving, as shown in Figure 2b. Our simulator of choledocal cyst can represent the same situation as in clinical cases. The standard diameter of the hepatic duct is 10 mm, but the diameter can be resized from a tiny 3 mm to a relatively large size. The operator can also perform duct plasty. The performance of hepatico‐jejunostomy was evaluated by a leak test using liquid. Biliary atresia model: In Kasai's operation, the most important procedure is careful dissection of the remnant tissue at the hepatic portal region. In our surgical model of biliary atresia, resectable remnant tissue of the hepatic portal region was successfully reproduced, as shown in Figure 3. Detachable remnant tissue was placed on the bifurcation of the portal vein. After dissecting the remnant tissue, the operator can perform portoenterostomy. The evaluation point is homogeneous peeling in points of depth and area of remnant tissue. These parameters were evaluated using an image recognition software program. The performance of portoenterostomy was evaluated by a leak test using liquid.
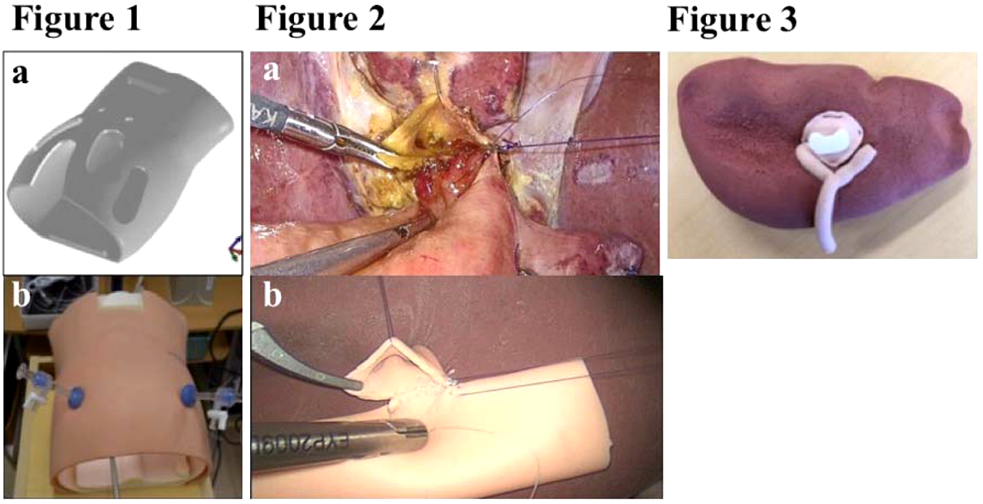
Conclusion: We developed high‐fidelity models simulating choledocal cyst and biliary atresia. A validation study using experts and trainees should be conducted in order to assess the usefulness of our models.
QS104 MINIMALLY INVASIVE EXPOSURE OF THE THORACIC AND LUMBAR SPINE IN CHILDREN WITH IDIOPATHIC SCOLIOSIS UTILIZING A THORACOSCOPIC TRANSDIAPHRAGMATIC APPROACH
St. Christopher's Hospital for Children
Introduction: Traditional treatment of scoliosis requires an invasive operation with placement of hardware to mechanically straighten the spine until it fuses. Exposure of the lower thoracic and lumbar spine has traditionally required either thoracoscopic or thoracotomy combined with an open lumbar incision. We have developed a novel minimally invasive approach for exposure and instrumentation of the lower thoracic and lumbar spine. Exposure is obtained with a thoracoscopic transdiaphragmatic retroperitoneoscopic approach that eliminates the incision that was previously necessary for treatment. Utilizing three 5mm and two to three 15mm ports, a diaphragmatic incision is made to create a retroperitoneal working space contiguous to the hemi‐thorax thus avoiding an additional lumbar incision. In addition, instead of the bulky hardware required for traditional scoliosis treatment, this system utilizes fusionless anterior vertebral body tethering. This tethering system is a new growth‐ and motion‐sparing technique for the treatment of skeletally immature growing children with progressive idiopathic scoliosis. We report our experience using this method in a series of patients with idiopathic scoliosis.
Methods: Retrospective analysis of children with idiopathic scoliosis undergoing anterior vertebral tethering of the thoracolumbar spine (T5 to L3) at a single institution utilizing a minimally invasive thoracoscopic transdiaphragmatic approach after obtaining IRB approval. The records of all children were reviewed. No patients were excluded. Pre‐operative, operative and post‐operative records of the children were abstracted for analysis.
Results: There were 12 patients identified with a mean age of 12.7 years. Ten patients were female. The mean skeletal immaturity scores were Risser 0.4 and Sanders 2.9. Operation included a mean of 8.3 vertebral levels tethered with a mean operative time of 157 minutes. Median estimated blood loss 242ml. The length of stay included PICU mean of 2 days and hospital mean stay 5.4 days. The operative result achieved thoracic curve correction of 77% and lumbar curve correction of 96% at mean of 19.5 month follow‐up assessment. There were no mortalities. There were three complications (respiratory insufficiency secondary to fentanyl, hypertrophic scar, and transient thigh numbness due to lumbosacral plexus stretch). No patients were converted to traditional open surgery or required blood transfusion.
Conclusion: Anterior exposure of the thoracic and lumbar spine including the thoracolumbar junction (up to L3) can be safely performed using a novel thoracoscopic transdiaphragmatic approach with minimal morbidity and excellent results.
QS105 OUTCOMES OF LAPAROSCOPIC ANDERSON‐HYNES PYELOPLASTY: ONE INSTITUTION EXPERIENCE
Hospital Dr. Luis Calvo Mackenna
Objective: We evaluated the characteristics of the patients and outcomes of our laparoscopic pyeloplasty procedures.
Methods: Retrospective revision of patient's characteristics, surgery details and outcomes of ureteropelvic junction obstruction cases resolved by laparoscopic Anderson‐Hynes pyeloplasty between the years 2011 and 2018 at our institution.
Results: 20 procedures were performed in the described period. 9 (45%) had prenatal diagnosis. 19 (95%) had a preoperative MAG3. 4/19 (21%) had a kidney function less than 40%. Mean patient age was 54.2 (3‐182) months. Mean patient weight was 29.2 (7.4‐48) kilograms. 8 (40%) were girls. All procedures were primary surgeries. 10 (50%) had a crossing vessel, 7/10 (70%) of them obstructive. 3 (15%) procedures were converted. Continued suture was used in all laparoscopic cases (17/20). 4 (20%) were left without a JJ stent. 11 (55%) were left with a Foley catheter. Mean operative time was 227.25 (120‐310) minutes. Mean hospital stay was 2.9 (1‐6) days. There were no infections. One patient had a filtration that resolved with a Foley catheter. 2 patients (10%) recurred and required redo surgery. Both were left a JJ stent in the first surgery. One was explored by laparoscopy and was found an ureteropelvic junction obstruction. An open pyeloplasty was done. The second one was explored by an open approach. There was not found an ureteropelvic junction obstruction, so there was not made a redo pyeloplasty.
Conclusion: Our outcomes are similar to those mentioned in literature. Considering that our casuistry is still initial, laparoscopic pyeloplasty is a safe and effective procedure in children with ureteropelvic junction obstruction in our hands.
Podium Video Abstracts
V001 VIDEO‐ASSISTED THORACOSCOPIC SURGERY FOR EXPOSURE OF VERTEBRAL BODIES FOR SCOLIOSIS CORRECTION
1University of Missouri Columbia School of Medicine, 2Department of Surgery, Brooke Army Medical Center, 3Division of Pediatric Surgery, Department of Surgery, Children's Hospital, University of Missouri
Adolescent idiopathic scoliosis (AIS) is a lateral, rotated curvature of the spine greater than 10 degrees occurring in patients aged 10‐16 years. Vertebral body tethering is an innovative and minimally invasive option for surgical management of AIS that has been shown to have advantages over the more traditional open techniques. This video demonstrates the technique for thoracoscopic exposure of thoracic vertebral bodies by pediatric general surgery in order to facilitate vertebral body tethering by the orthopedic surgery team for correction of AIS. The patient in this case was an otherwise healthy 16‐year‐old female with a pre‐operative thoracolumbar curve of 55 degrees. There were no immediate post‐operative complications. At her 8‐week post‐operative appointment, her only complaint was mild incisional pain and her curve had decreased to 18 degrees. We have performed this procedure or a variation of it on a total of 46 patients with average follow‐up of 1.26 years.
V003 DEVELOPING A “GRUYERE” LIKE TRAINER TO USE IN THE TRANSITION BETWEEN BASIC AND NEONATAL SIMULATION BASED MIS SURGICAL EDUCATION (VIDEO)
Garrahan Children's Hospital
We developed a low cost endotrainer for advanced training in pediatric MIS before using the specific neonatal trainers.
It consists in a manequin opened in half. We call it “Gruyere” because of the multiple orificies placed to perform abdominal, pelvic, mediastinal and pulmonary procedures in different positions. Synthetic components and ex vivo porcine tissue may be placed in the model. An abdominal wall was created with synthetic matherials.
Pelvic procedures like ovarian cystectomty and linfadenectomy can be achieved. Refine suturing practise can be done resembling an hepaticoyeyunostomy using porcine live tissue. We can see the practise of the shoeshine maneuver and suturing in a simulated Nissen. The prone position is meant to access the esophagus and mediastinum.
A detailed tutorial of matherial, steps of each procedure, and evaluation sheet has been designed to facilitate its use. We plan to use it in remote places with telementoring concepts.
V004 ROBOTIC‐ASSISTED RELEASE OF THE MEDIAN ARCUATE LIGAMENT FOR PEDIATRIC MALS
Cincinnati Children's Hospital
Median Arcuate Ligament Syndrome is a chronic abdominal pain syndrome characterized by epigastric pain, nausea, and vomiting that leads to anorexia and weight loss. It is a diagnosis of exclusion, hypothesized to be caused by compression of the celiac artery and celiac plexus by the median arcuate ligament at the junction of the right and left diaphragmatic crura. Due to the presence of an identifiable mechanical constriction, the management of MALS is surgical. In this video, we present the key features of the robotic approach for its release in the pediatric population.
V005 SMALL SURGERIES, BIG SMILES: REDUCING SEDATION THROUGH VIRTUAL REALITY
Stanford University
Introduction: This video presents the novel use of virtual reality (VR) to reduce the need for procedural sedation in children undergoing minor surgical procedures.
Methods: Patients were offered the opportunity to use VR instead of procedural sedation or general anesthesia. Outcome measures included the Pain Catastrophizing Scale for Parents, the Child Fear Scale, the Childhood Anxiety Meter, and child, caregiver, and clinician satisfaction surveys.
Results: The study enrolled 7 patients with a median age of 9.6 years. Procedures included hormone implant placement/removal and cecostomy tube replacement, with a mean duration of 17 minutes. No sedating medications were needed. Post‐procedure, parents' concerns about their child's pain decreased, as did children's self‐reported anxiety, pain, and fear. Overall satisfaction was very high. All patients would want VR again for a similar procedure.
Conclusion: It is feasible to use VR to reduce the need for procedural sedation during minor surgical procedures in children.
V006 USE OF ICG AND NEAR INFRARED FLUORESCENCE LAPAROSCOPY TO IDENTIFY AND RESECT RECURRENT HEPATOBLASTOMA IN A FOUR YEAR OLD CHILD
Rocky Mountain Hospital for Children
Near infrared fluorescence has bee used in laparoscopy to help identify biliary structures. Recent data suggests it may be useful in identification of hepatic tumors. This video represents a unique case where indocyanine green (ICG) was given to a 4 yo boy with evidence of recurrent hepatoblastoma to help identify the tumor at laproscopy. 48 hours prior to surgery the child was injected with 0.5mg/kg of ICG. He then underwent standard laparoscopy using the PINPOINT endoscopic imaging system (Stryker Endoscopy, USA). The procedure was performed switching between the white light ilumination and near infrared fluorescence (NIF) mode to allow for identification and complete gross resection of the tumor. The tumor was easily identified and resected with the NIF mode. The child was discharged on POD1 and started chemotherapy two days later. The use of NIF and ICG may play a unique role in the management of childhood biliary tumors.
V007 PULMONARY VEIN HEMORRHAGE DURING THORACOSCOPIC LEFT UPPER LOBECTOMY
Children's Mercy Hospital
Purpose: We present a thoracoscopic left upper lobectomy where potentially disastrous bleeding was encountered after using a stapler for vascular control of the pulmonary vein, which was controlled thoracoscopically.
Methods: A 9‐month‐old underwent thoracoscopic resection of a congenital cystic lung lesion. The procedure commenced as normal. A 5mm stapler was used to secure the pulmonary vein. After firing the stapler, there was oozing from the staple line that quickly turned into high pressure bleeding. This was grasped and another 5mm port was placed. A clip applier then secured the staple line before more significant hemorrhage or air embolism developed. The patient remained asymptomatic. The remainder of the operation proceeded uneventfully.
Results: The patient recovered well and was discharged home the next day and continues to do well in follow‐up.
Conclusions: Bleeding from the pulmonary hilum during thoracoscopic lobectomy can be controlled thoracoscopically with adequate experience and readily available equipment.
V008 NOVEL COMBINED APPROACH OF A PRENATALLY DIAGNOSED OROPHARINGEAL TERATOMA. VIDEO
1Fundación Hospitalaria, 2CEMIC
Prenatal: An oropharingeal mixed tumor was diagnosed during prenatal scan. The mass grew steadily and invaded the nasal fosase.
Birth: An EXIT procedure was done at 35 weeks of gestation. During direct laringoscopy a mixed mass was identified at the oropharinx invading the fossa nassae. Orotracheal intubation was succesfully accomplished.
Postnatal: On the fourth day of life, a multidisciplinary approach of the patient began with a resection of the extracavitary components of the tumor, both nasal and oral. And endoscopic exploration of tha oral cavity revealed a soft palate fissure from which the tumor emerged. A nasal endoscopic exploration allowed identification of the nasal root of the tumor in a posterior location. Dislodgement of the nasal component towards the pahrinx was done so that and oral endoscopical complete resection was achieved. Follow up was uneventful.
V009 DEVELOPING SIMULATION MODELS FOR FETAL THERAPY
Garrahan Children's Hospital
In 2018 we start developing simulation‐based models as educational strategy for intrauterine invasive techniques. The approach to fetal surgery includes ultrasound guided procedures, fetoscopy and endoscopic suturing.
We propose a Maternal‐fetal model: a 1.5 cm height gel plate simulates skin and anterior uterine wall. It is placed over a jumbo‐size balloon containing water to simulate the amniotic sac and cavity. Insidem there is a gel fetus with a cyst, a umbilical cord with red‐coloured content, and a gel‐placenta that can be placed anterior, posterior or laterally by rotation of the model. Through this, cordocentesis, fetal anaesthesia injection, stent placing, fetoscopic procedures, are all allowed.
Another model modified from Dr. Gine's model is developed for intrauterine fetoscopic suturing in a bosu ball sealed by a gel‐port.
We look foward these models can contribute to the fetal therapy procedural skill learning curve and patient outcomes.
V010 LAPAROSCOPIC ANTERIOR “PARS FLACCIDA” APPROACH MEDIAN ARCUATE LIGAMENT RELEASE
Women's and Children's Hospital, South Australia
Median arcuate ligament syndrome is a rare pathology in both children and adults. It results in symptomatic compression of the coeliac axis. Definitive treatment involves division of the constricting median arcuate ligament to release impingement of the coeliac trunk at its take‐off from the aorta. The traditional open approach necessitates a high morbidity laparotomy. Numerous laparoscopic approaches have been described, including trans‐gastrocolic ligament “lesser sac” and trans‐hepatogastric ligament (pars flaccida) “anterior” techniques. This video illustrates our recommended anterior “pars flaccida” approach to this pathology and discusses respective merits. Pediatric surgeons benefit from familiarity with this approach due to shared surgical exposure and dissection steps that occur with operations such as laparoscopic fundoplication.
V011 THORACOSCOPIC REPAIR OF A TYPE 3 TEF IN A 1KG NEONATE. TECHNIQUE, CHALLENGES, AND LUCK!
Rocky Mountain Hospital for Children
A 29 week gestation premature female was born with a previously undiagnosed Type 3 tracheo‐esophageal fistula and esophageal atresia. The patient weighed 1.05 kg and was hemodynamically and respiratorially stable. An ECHO showed a normal right arch and there were no other anomalies. She underwent thoracoscopic division of her TEF with primary anastomosis at 8 hours of life. The patient was monitored with NIRS as well as endtidal CO2 and pulse oxymertry. The procedure was performed using 3 ports, 1‐4mm and 2‐3mm. The procedure took 110 minutes. A transanastomitic tube was left in place. A contrast study on Day 7 showed no contrast flowing past the NG tube. On day 10 a G tube was placed. At 14 days a contrast study should a small caliber anastomosis. This was later dilated without difficulty. This video demonstartes the unique challanges of performing a thoracoscopic TEF in a 1 KG neonate.
V012 INNOVATIVE USE OF MINILAP INSTRUMENT TO PLACE A NEPHROURETERAL STENT
1Hospital Interzonal Dr. Jose Penna, Bahía Blanca, Argentina. Universidad Nacional del Sur, 2Hospital Municipal Leonidas Lucero, Bahía Blanca, Argentina
Our approach for ureteropelvic junction obstruction is laparoscopic pyeloplasty at all age groups. Different alternatives are use for postoperative urinary drainage like double J stent (DJ), pyelostomy tube, nephrostomy, nephroureteral stent (NS). For older patients we usually use a DJ. For patients using diapers our preferred method of urinary drainage is a home‐made silicone NS, placed in a retrograde fashion from inside the kidney towards the skin level. The holes fashioned in the stent are fit in the pelvis and ureter providing an excellent external drainage to a double diaper. Foley catheter is not used and patients are discharge home on the first postoperative day. In this video we demonstrate an innovative use of minilap instrument for a precise placement of a NS in the preferred calyx. This technique has provided a simple, bloodless placement of the stent with a sharp and neat exteriorization at the skin.
V013 LAPAROSCOPIC MORGAGNI HERNIA REPAIRS WITH AN INTUITIVELY‐CONTROLLED ARTICULATING INSTRUMENT
1University of Michigan, Pediatric Surgery Section, 2Penn State Hershey Children's Hospital
This video demonstrates two pediatric Morgagni hernias repaired with a novel intuitively‐controlled articulating laparoscopic instrument. A 6‐month old presented with an incidental Morgagni on the first day of life. Delayed elective surgery was planned and a primary repair utilizing this novel tool is demonstrated. The second patient was status post‐omphalocele repair when she was noted to have a Morgagni hernia during a URTI at 12‐months of age. While awaiting elective repair she presented with a bowel obstruction and underwent diagnostic laparoscopy. Adhesive bands in the chest were lysed including direct adhesions to the right atrial appendage. After reduction, her hernia was repaired laparoscopically with a Gortex mesh secured using the articulating laparoscopic instrument. Both cases were facilitated by the robotic‐like articulation and intuitive twirl to complete these repairs.
V014 GASTRIC PERORAL ENDOSCOPIC MYOTOMY (G‐POEM) FOR TREATMENT OF CONGENITAL PYLORIC STENOSIS – FIRST INITIAL EXPERIENCE
1Irkutsk State Medical University, 2St. Petersburg Medical University, 3Children's Hospital Kemerovo, 4Children's Hospital Irkutsk
A new technique, gastric peroral endoscopic myotomy (G‐POEM), has been proposed as an alternative to surgical pyloromyotomy for the management of congenital pyloric stenosis. For myotomy was used gastroscope with diameter 5.4 mm and instrumental channel 2 mm. After proper preparation, a submucosal injection oof saline mixed with methylene blue was made at the greater curvature about 4 cm from the pyloric ring. The creation of mucosal entry was performed at the site of the initial submucosal bleb. After them, submucosal tunneling was made towards the pylorus using the soft or spray coagulation. The sphincter was identified as a round muscular bundle when the scope reaches the pylorus. For G‐POEM a cutting only the inner circular muscle of the pylorus is recommended, but it is not possible at infants with pyloric stenosis and we performed full‐thickness myotomy. The entry site and mucosal incision was closed with special clips.
V015 RECURRENT PULMONARY CYSTS AFTER PLEURO‐PULMONARY BLASTOMA: A CHALLENGING PATHWAY
1Buzzi Children's Hospital, Milan, Italy, 2Rocky Mountain Hospital for Children, Denver, Colorado, USA and Columbia University College of Physicians and Surgeons, New York, NY, USA
Our 7‐year‐old patient had been previously operated at the age of one month, after a severe respiratory distress due to massive macrocystic lesions affecting all the lobes of the right lung. After thoracotomy resection, the histology had shown a type 1 pleuropulmonary blastoma and a chemotherapy had been needed. At follow‐up, CT and MRI showed two large cystic formations of the right upper lobe and 6 additional cysts of the middle and lower lobes. After 3D reconstruction from CT images and a multidisciplinary discussion with international experts, we decided to perform a 3‐trocar thoracoscopic resection of the upper lobe and the residual cysts, using 3 mm and 5 mm instruments. The procedure was carried out without complications and the postoperative period was uneventful. Luckily, the histological examination allowed to demonstrate a cystic dilation of the alveolar spaces associated with chronic inflammation, without blastoma recurrence.
V016 AORTIC LEVITATION FOR THE MANAGEMENT OF NON‐DETECTED RIGHT AORTIC ARCH IN EA
Clínica Las Condes
Right‐sided Aortic Arch (RAA) is a cardiac anomaly that can be found in 0,1% of adult population. It has a higher incidence in Esophageal Atresia. Echocardiography does not detect 100% of RAA. Usual recommendation of experts is changing to the left when a RAA is detected during a Right thoracoscopic approach. We present a Traditional Left thoracoscopic approach in RAA, and a patient with non‐detected RAA with a right thoracoscopic approach. We manage to place a percutaneous vasoloop surrounding the aorta. By lifting it, we made place to work with the esophagus without harming the aorta. Continuously hemodynamic monitoring showed no alteration. We find left thoracoscopic approach is a good alternative for patients with RAA. But RAA does not contraindicate a Right approach. “Aortic levitation” was useful to let the surgeon do a thoracoscopic anastomosis without compromising the patient. This trick can be useful to avoid changing sides in selected patients.
V017 THORACOSCOPIC REPAIR OF PROXIMAL H‐TYPE TRACHEOESOPHAGEAL FISTULA
Children's Hospital of Wisconsin
Thoracoscopic repair of esophageal atresia and associated tracheoesophageal fistula (TEF) is a procedure that has become popular, however current literature still advocates for a transcervical approach to repair of isolated H‐type TEF located above the T2 vertebral level. Transcervical tracheoesophageal fistula repair has been associated with as high as a 50% rate of recurrent laryngeal nerve injury in one series. We present the case of a 16 month old otherwise healthy baby girl with an H‐type TEF identified at the C5‐C6 vertebral level that was successfully repaired via a thoracoscopic approach. Normally functioning vocal cords were seen on postoperative laryngoscopy. This case demonstrates that thoracoscopic repair is both feasible and effective in repairing H‐type TEF above the T2 level. This not only allows for a less invasive approach but may also confer a lower risk of injury to the recurrent laryngeal nerve.
V018 THORACOSCOPIC RESECTION OF A ESOPHAGEAL LOBE IN A NEONATE
UT Southwestern Medical Center
Background: Thoracoscopy has been well established for resections of lung lesions, foregut duplication cysts, tumors as well as repair of esophageal atresia anomalies. This approach however, has not been frequently reported in a newborn infants with unusual anatomic variants of these anomalies.
Methods and Materials: We present a case of a 3250g infant born with fevers and tachypnea found to be secondary to refractory right upper lobe collapse. A contrast enhanced CT scan demonstrated direct communication between the right upper lobe and the esophagus. An esophogram confirmed communication between the esophagus and the right upper lobe.
Thoracoscopic right upper lobectomy was performed. Division of the fistulous connection was performed using a 5 mm linear cutting stapler.
Results: A postoperative esophogram demonstrated no contrast extravasation and a rapid emptying esophagus. The patient was discharged the next day on full feeds. Pathology was consistent with an esophageal lobe.
Conclusions: Thoracoscopic management of rare congenital variants is feasible.
V019 INDOCYANINE GREEN USE DURING PEDIATRIC LAPAROSCOPIC CHOLECYSTECTOMY
John R. Oishei Children's Hospital
Purpose: To demonstrate that the use of indocyanine green (ICG‐FC) in the pediatric patient population during laparoscopic cholecystectomy (LC) allows identification of the biliary tree and is safe and reproducible.
Method: After reconstitution 2.5 mg ICG injected intravenously in the operating room prior to incision. A fluorescent laparoscopic imaging system was used. Intra‐operatively switching the camera view from normal to ICG wavelength allows visualization of the biliary tree.
Results: ICG‐FC was used in 29 pediatric LC. Ages ranged from 6‐18 years. In all patients the dye delineated the extra‐hepatic biliary anatomy, illuminating the common hepatic and common bile duct. There were no complications noted.
Conclusions: ICG‐FC provides a noninvasive real‐time visualization of the extrahepatic biliary tree. We demonstrate that ICG‐FC can successfully be used as an adjunct in pediatric patients and has the potential to facilitate with the dissection and minimize risk of bile duct injuries during laparoscopic cholecystectomies.
V020 LAPAROSCOPIC TYPE I CHOLEDOCHAL CYST EXCISION WITH INTUITIVELY‐CONTROLLED ARTICULATING INSTRUMENT
1University of Michigan, Pediatric Surgery Section, 2Penn State Hershey Children's Hospital
This video demonstrates the laparoscopic excision of a type I choledochal cyst using a novel intuitively‐controlled articulating instrument. A 19‐month old girl presented with obstructive jaundice and mild pancreatitis. MRCP demonstrated a 2.9 cm type I choledochal cyst. After clinical resolution of her pancreatitis, she underwent a laparoscopic choledochal cyst excision with a hepaticoduodenostomy reconstruction. This video demonstrates the application of the articulating instrument to facilitate the anastomosis within the confines of limited abdominal domain in this 14kg child. The hand‐held instrument permits completion of this case by providing robotic‐like articulation and control without requiring robotic infrastructure. The patient recovered well and is symptom‐free after three months of follow‐up. This video demonstrates the tool's potential versatile applications to pediatric surgical procedures.
V021 THORACOSCOPIC RESECTION OF INTRADIAPHRAGMATIC BRONCHOPULMONARY SEQUESTRATION
Akron Children's Hospital
Background: Extralobar bronchopulmonary sequestration is a rare variant of an uncommon congenital malformation, occurring in 25% of patients with sequestration, which itself has an incidence of 0.15‐1.7%. Even rarer is the subtype of extralobar sequestration that occurs within the diaphragm. Only 17 instances of this subtype exist in the literature, seven of which were repaired thoracoscopically.
Methods: The patient is a four‐month‐old female who presented after a congenital pulmonary airway malformation was detected on prenatal ultrasound and confirmed on both prenatal MRI and postnatal CTA. Intraoperatively, no lesion was found on the lung; instead, it was discovered within the diaphragm. In this video, the thoracoscopic treatment of an intra‐diaphragmatic sequestration is detailed.
Results: The patient recovered uneventfully and was able to be discharged home on post‐operative day 2.
Conclusion: To our knowledge, ours is the first video of a thoracoscopic repair of an intra‐diaphragmatic bronchopulmonary sequestration.
V022 ROBOTIC ASSISTED BILATERAL LAPAROSCOPIC ADRENALECTOMY: SETTING UP FOR SUCCESS
Nationwide Children's Hospital
Bilateral robotic‐assisted laparoscopic adrenalectomy: setting up for success.
This video demonstrates a bilateral robotic adrenalectomy for functional neuroblastic tumors in a pediatric patient. The video focuses on the pre‐operative planning including room‐set up, patient positioning, robot docking, and port placement to facilitate safe and efficient case completion. The intraoperative video highlights the tremendous visualization of the robotic platform along with the utility of the robotic instruments to facilitate in dissection and successful completion of the operation.
Preoperative planning allowed this approach to avoid a cumbersome transition between laterality, and required minimal repositioning of the robot, elimination of the need to re‐drape, and reduction of number of ports.
V023 LAPAROSCOPIC CHOLEDOCHAL CYST EXCISION WITH TOTALLY‐INTRACORPOREAL CREATION OF JEJUNOJEJUNOSTOMY & ROUX LIMB USING 5MM LAPAROSCOPIC STAPLER
Children's Hospital Los Angeles
We are presenting a laparoscopic choledochal cyst excision using a 5 mm stapling device for totally‐intracorporeal creation of the jejunojejunostomy and roux‐en‐Y limb for hepaticojejunostomy. A 2 year old girl with type IV choledochal cyst presented with cholangitis and after imaging evaluation and delivery of IV antibiotics, she was taken for laparoscopic surgery. We avoid the need to exteriorize the small bowel for creation of the JJ by using a 5mm laparoscopic stapler.
V024 LAPAROSCOPIC GASTROSTOMY TUBE PLACEMENT WITH TRANSABDOMINAL SUTURE
Stanford University
Introduction: We present a novel transabdominal suture technique for laparoscopic G‐tube placement.
Methods: Two ports are utilized; one umbilical/camera port and one working port that becomes the site for the G‐tube. Transabdominal Georgeson sutures are placed through the stomach wall. The stomach entered using a transabdominal needle under direct vision. After serially dilating the tract over a wire, two additional Stamm sutures are placed using our novel transabdominal technique. The needle passes through the incision and stomach opening, through the stomach and abdominal walls; however, before the swage edge of the needle exits the skin, the needle is backed through the LUQ incision subcutaneously.
Results/Conclusions: These transabdominal Stamm sutures secure the stomach to the abdominal wall even after the Georgeson sutures are released. The added fixation ensures that the stomach will not fall way from the abdominal wall, even if the gastrostomy tube is dislodged in the early postoperative period.
V025 FRANCOAMERICAN HYBRID TECHNIQUE (FAHT) OF PULMONARY LOBECTOMY IN INFANTS
Northwest Permanente Physicians and Surgeons
This hybrid technique utilizes a sealing device to control the vessels, and a stapler for the bronchus. Notably, with an alternate port position, the telescope looks directly up the fissure, allowing for a more intuitive orientation to the pulmonary hilar structures.
V026 THORACOSCOPIC FENESTRATION FOR HEMORRHAGIC CARDIAC TAMPONADE INDUCED BY CARDIOTOXICITY OF CYCLOPHOSPHAMIDE
1Department of Pediatric Surgery, Research Field in Medicine and Health Sciences, Medical and Dental Sciences Area, Research and Education Assembly, Kagoshima University, Kagoshima, JAPAN, 2Department of Pediatrics, Research Field in Medicine and Health Sciences, Medical and Dental Sciences Area, Research and Education Assembly, Kagoshima University, Kagoshima, JAPAN
Background: Various approaches have been described for cardiac tamponade. We herein report a case of surgical management of recurrent pericardial effusion using a video‐assisted thoracoscopic pericardial window.
Case: A 4‐year‐old boy had a history ofcardiac tamponade. The patient was treated by subxiphoid pericardiocentesis. However, his cardiac tamponade relapsed, so thoracoscopic fenestration was planned.
Operative findings and Procedure: Under general anesthesia, the patient was placed in the right three‐quarter position. Three 5‐mm camera ports were inserted at the 4th,5th, 6th intercostal space of the anterior and middle axillary line. A pericardial window was created using an ultrasonically activated device. The size of the created window was 4.5 × 2.5 cm.
Results: The cardiac function was normalized immediately and showed no recurrence.
Conclusion: Thoracoscopic fenestration for cardiac tamponadewas found to be an effective procedure for the treatment of pericardial effusions in this case.
V027 A MULTIDISCIPLINARY APPROACH TO A COMPLEX ANORECTAL MALFORMATION AND UROLOGIC ANOMALY
Loma Linda University Children's Hosptial
The purpose was to describe a multidisciplinary approach to a complex anorectal and urologic malformation.
A 38‐week‐gestation male underwent a divided colostomy on day of life 2 for a high anorectal malformation. At 1 month, he developed a scrotal abscess. At drainage, a foley catheter was placed and pus was aspirated. Ultrasound revealed a cystic mass in the pelvis. He was discharged with plans for further imaging, but returned 2 weeks later with a recurrent abscess. Collaboration between pediatric urology, surgery and radiology provided a thorough understanding of the anomaly. Combined imaging and endoscopic techniques demonstrated a utricle cyst connected to the rectum, urethra and vas. A wire‐guided drain was placed and secured. With daily flushes, the infections resolved. The infant underwent a successful pull‐through. The cyst obliterated.
Conclusion: A multidisciplinary approach for complex anorectal malformations provides a thorough understanding of the etiology and aids in complex reconstructive procedures.
V028 THORACOSCOPY MEDIASTINAL MASS EXCISION WITH IATROGENIC BRONCHIAL INJURY REPAIR
Saint Louis University
We present the case of a 13 y/o boy who presented to our institution with history of dysphagia for over a month. He reports recent tick bit, for which he received prophylactic antibiotics (Lyme's). At our institution, his initial work up included Esophagram which showed external compression of mid esophagus. EGD showed external compression and Chest MRI showed a 5 × 4 cm mass in posterior mediastinum with diferential diagnosis of histoplasmoma vs infected esophageal duplication cyst. Although his histoplasma titers were normal. Given this presentation he was taken to the operating room for right thoracoscopic excision of posterior mediastinal mass. Intraoperative frozen biopsy showed evidence of esopgeal muscularis in the wall of the cyst and decision was made to proceed with compelte excision. The procedure was complicated by intraoperative iatrogenic bronchial injury which was recognized and repaired thoracoscopically. Patient did well and wa dischage after POD 7
Late Breaking Podium Abstracts
S022 THORACOSCOPIC CLOCK‐WISE LOWER LOBE RESECTION IN CHILDREN
West China Hospital, Sichuan University
Objective: Stylized surgical procedures are an inevitable trend in the development of thoracoscopic lobectomy in children. Thoracoscopic surgery in children has small chest space and is characterized by benign diseases. It is significantly different from thoracoscopic surgery in adult. Therefore, it is necessary to have a stylized lobectomy method that is suitable for children, especially infants. This study reviewed the clinical data of children undergoing thoracoscopic clock‐wise lower lobe resection in our hospital, analyzed the surgical points, and summarized the surgical procedures.
Methods: The cases that accepted thoracoscopic clock‐wise lower lobe resection in our hospital from June 2015 to June 2018 were reviewed retrospectively. During the procedure, three valved endoscopic ports were used. The trocars were positioned in the anterior, middle and posterior axillary lines in the 5th, 8th and 9th interspace respectively. The lens was inserted through the middle trocar. The procedure started from the ligament and released it until the inferior pulmonary vein. Then the dissection began to turn around the hilum, the left procedure followed clockwise and the right one followed counterclockwise to dissect around the bronchus. After the fissure tissues and pulmonary artery was dissected and sealed along the direction, it rotated back to the inferior pulmonary veins. After the veins were sealed, then the bronchus was dissected completely, sealed it and completed the procedure.
Results: Total 143 cases were included in this study, 78 were boys and 65 were girls. The ages ranged from 4 months to 13 years (mean,10 months). 107 cases were diagnosed prenatally. There were 66 left lower lobes and 77 right lower lobes. The operative times ranged from 30 minutes to 70 minutes (average, 42 minutes). The chest tubes were not placed in 78 patients. As to the others, the chest tubes were removed within 24 hours post‐operatively. The patients recovered to normal diet and activities in 6 hours after operation. There were 2 patients that developed a delayed pneumothorax which was found after operation and resolved spontaneously in 2‐week control. No air leak, bleeding, bronchopleural fistula and other complications occurred. All patients discharged on the 3th day post‐operatively. During the following, all patients recovered well, and no recurrence or other complications occurred.
Conclusions: Thoracoscopic clockwise lower lobe resection facilitates the operation. This procedure can reduce the intraoperative meaningless flipping of the lung, the operative trauma, the postoperative complications, and accelerate postoperative recovery.
S058 PEDIATRIC ENDOSCOPIC PILONIDAL SINUS TREATMENT (PEPSIT): AN EFFECTIVE PROCEDURE FOR CHILDREN WITH RECURRENT PILONIDAL SINUS DISEASE AFTER FAILED OPEN SURGERY
Pediatric Surgery Unit, Department of Traslational Medical Sciences, Federico II University of Naples, Naples, Italy
Background: The traditional open excision of pilonidal sinus disease (PSD) is extremely invasive, with a high postoperative morbidity and high recurrence rates. We recently published our preliminary experience with pediatric endoscopic pilonidal sinus treatment (PEPSiT). We aimed to report outcome of PEPSiT also for treatment of recurrent PSD after failed open repair.
Methods: All patients with recurrent PSD after open excision who underwent PEPSiT over the last 2 years were included in the study. During surgery, a fistuloscope was introduced through a fistula's orifice. All identifiable hairs were removed using endoscopic forceps. Thereafter, the cavity was debrided with endoscopic brush and ablated with monopolar electrode. External openings were not closed.
Results: In the last 2 years, 40 patients with PSD were operated using PEPSiT in our Unit. Ten/40 patients (6 boys and 4 girls with an average age 16.8 years [range 14–18]) had a recurrent PSD after open surgery and were included in the study. The average operative time was 27.7 minutes (range 24–43). No peri‐operative complications occurred. The average analgesic requirement was 20 hours (range 16–26) and the average hospitalization was 22.4 hours (range 18–36). The average time to return to full daily activities was 2.3 days (range 1–5) and all patients were highly satisfied of postoperative course. At 1 month postoperatively, the external openings were completely healed. No recurrence was recorded at a mean follow‐up of 18 months (range 1–24).
Conclusions: Our results demonstrated that PEPSiT is an excellent technique for surgical treatment of PSD in children and teenagers. In fact, it is technically easy and fast to perform, with a short and painless hospital stay and it allows to the operated patients an early return to full daily activities without any physical limitations. Furthermore, our results confirmed that it is highly effective also for treatment of recurrent PSD after failed open repair.
Late Breaking Quickshot Abstracts
QS011 A CHEST TUBE MAY NOT NECESSARY IN CHILDREN WITH THORACOSCOPIC LOBECTOMY
West China Hospital, Sichuan University
Objectives: Drainage of the thorax after thoracic surgery by chest tubes is a standard procedure in thoracic surgery. However, chest tubes can induce morbidities such as pain, immobilization and increase risk of infection, deteriorates the ventilation capacity and increase difficulty of postoperative management, especially for children. This study aims to investigate the safety and effectiveness without chest tubes after thoracoscopic lobectomy in selected patients.
Methods: A retrospective review of medical records was performed in West China Hospital of Sichuan University from January 2014 to June 2018. Patients underwent thoracoscopic lobectomy without chest tubes were recorded. The other patients who with severe pulmonary infection, extensive thoracic adhesions or undeveloped interlobar fissure were excluded.
Result: Totally, 246 patients were performed a thoracoscopic lobectomy without chest tubes after operation and none needed a chest drain insertion or reintervention during the hospitalization and 90‐day following up. Among them, two (0.81%) patients had developed a delayed pneumothorax which was found after operation and resolved spontaneously in 2‐week control. No hemothorax, atelectasis and bronchial fistula was found. One hundred ninety nine (80.8%) patients developed subcutaneous emphysema which was asymptomatic and spontaneously absorbed in 3–7days. The mean length of postoperative hospital stay was 2 days. Patients could recover to free mobilization in 6h. Post‐operative 6h, they could resume regular diet. All patients accepted at least 3 months following up, and no complication was found in other patients and all patients recovered well.
Conclusions: This study shows that chest tube placement in selected patients may not necessary in children thoracoscopic lobectomy in selected patients. the minimally invasive procedure and meticulous resection have been the precondition of this procedure, and which may contribute to rapid recovery and can avoid the chest tube‐related complications effectively.
QS017 LAPAROSCOPIC MANAGEMENT OF MÜLLERIAN DUCT REMNANTS ‐ PRESENTATIONS, SURGICAL INDICATIONS AND TECHNICAL EXPERIENCE WITH LAPAROSCOPIC APPROACH
Cairo University Specialized Pediatric hospital
Introduction: Müllerian ducts regress in males under the effect of anti‐ Müllerian hormone (AMH), produced by pre‐ sertoli cells. Müllerian duct remnants (MDRs) persist due to (a) AMH deficiency (b) receptor insensitivity (C) mixed gonadal dysgenesis (45, XO/ 46, XY) or (d) 46 XY gonadal dysgenesis.
Cases may present with proximal hypospadias and / or testicular maldescent of various combinations. MDRs may be missed on ultrasonography thus escape early detection, present as an intraoperative surprise, or post urethroplasty complications or may change malignant.
Methods: We reviewed a case series consists of 10patients with MDRS. They were collected prospectively as candidates for laparoscopy and were decided to be raised as males by both endocrine and surgery teams at cairo university specialized pediatric hospital (CUSPH) according to karyotyping, hormonal essay and HCG stimulation test.
Results:
·6 cases with +ve consanguinity
·Karyotyping: 3 cases were mosaic turner (45 XO/ 46XY), 5cases (46 XY), 1 case true hermaphrodite (46 XX/ 46XY), 1 Case 46XX testicular disorder (46XX Male)
·8 cases were presented with hypospadius (7 penoscrotal hypospadius and 1 midshaft)
·7 cases were presented with bilateral undescended testis and 3 cases with unilateral undescended testis
·Mullein duct remnants and gonads were visualized by ultrasound and MRI in 4 cases only, 1 case MDRs were visualized radiologically without visualization of the gonads and MDRS couldn't be detected radiologically in the other 5 cases in which MRDS were discovered accidentally during orchidopexy (open or laparoscopic)
In this study we performed 16 laparoscopic maneuver:
·6 Diagnostic Laparoscopy and biopsy
·10 Therapeutic
·6 MDRs excision, 3 of them associated with Gonadectomy for dysgenetic gonads
·3 MDRS division
Conclusion:
·Laparoscopy has an evident diagnostic accuracy for MDRS and gonads that couldnot be detected radiologically
·Excision\Division of MDRS by Laparoscopy Is technically feasible and provides a favourable outcome
·Absolute indications for removal/division of MDRs were to achieve tension‐free orchidopexy as they anchor the testis preventing normal descent and prior to proximal hypospadias repair to avoid felling with urine, hence stasis and infection
·However a larger sample is needed to support this study
QS052 THORACOSCOPIC ANATOMICAL SEGMENTECTOMY IN CHILDREN
West China Hospital, Sichuan University
Objective: Thoracoscopic segmentectomy as a method of sparing‐lung surgery have received increasing attention in recent years. With the development of thoracoscopic techniques and experience of anatomical lobectomy in children, it provided the necessary technical preparation and accumulation for thoracoscopic anatomical segmentectomy in children. This study aimed to evaluate the safety and effect of this procedure.
Methods: The cases that accepted thoracoscopic anatomical segmentectomy in our hospital from June 2014 to June 2018 were reviewed retrospectively. The chest thin‐section CT were performed before surgery to ensure feasible segmental resection. During the procedure, three valved endoscopic ports were used. The vessels, fissures and branchi of the segments that lesions located in were dissected respectively, and then the segmental arteries, veins and bronchi were sealed by hemolock and ligasure in sequence. After closing the segmental bronchus, the lungs were reinflated by the anesthesiologist. The segmental boundary could be judged from the surface of the lung reinflation and lung consolidation. The lung tissues were sealed and separated by Ligasure or ultrasonic scalpel along the boundary to complete the segmental resection. A chest tube drainage was left after the procedure.
Results: Total 92 cases were included in this study, 49 were boys and 43 were girls. The ages ranged from 5 months to 9 years (mean, 14 months). The operative times ranged from 50 minutes to 100 minutes (average, 78 minutes). There were 55 S7‐10, 3 S6, 2 right S5, 11 left S4+S5, 7 left S1+S3, 6 right S1‐3, 5 right S2 and 3 S1. The chest tubes were removed within 24 hours postoperatively. The post‐operative hospital stay were 3 days. 3 patients developed pneumothorax because of small air leak after discharge and required a chest tube replacement. bleeding, bronchopleural fistula or other postoperative complications were not found in all cases. All patients accepted at least 3 months following. During the following up, the remaining lung compensated well, and no recurrence or other complications occurred in all cases.
Conclusion: Thoracoscopic anatomical segmentectomy in children is a safe and effective means of lung parenchymal preservation in selected patients. It seemed that has a lower complication rate comparable with the other sparing‐lung surgery.
QS089 THORACOSCOPIC TREATMENT OF NEUROGENIC TUMORS OF THE POSTERIOR MEDIASTINUM IN CHILDREN
West China Hospital, Sichuan University
Objective: Neurogenic tumors of the posterior mediastinum are common diseases in thoracic surgery. Compared with traditional thoracotomy, thoracoscopic technique has the advantages of less trauma and better vision. In this study, we reviewed the cases of neurogenic tumors that accepted thoracoscopic surgery and tried to summarize the experience in a single center.
Method: The cases that accepted thoracoscopic resection of neurogenic tumor in our hospital from August 2011 to January 2018 were reviewed retrospectively. The clinical data of all cases were analyzed and summarized. During the surgical procedure, three valved endoscopic ports were used. The appropriate position of trocar was to select according to the location of the tumor. After the tumor was removed, it was taken out by the endoscopic pocket. A chest tube drainage was left after the procedure.
Results: Total 83 cases were included in this study, 34 were boys and 49 were girls. The ages ranged from 6 months to 13 years (mean, 7.8 years). Except for one patient who was diagnosed with Horner syndrome, the other children had no specific clinical symptoms, which were found by accidental chest imaging. Preoperative CT in all cases indicated that the tumor had not crossed the midline and the maximum diameter was less than 10 cm. The operations were successfully completed under thoracoscopy. The operation time ranged 30–160 min, and the intraoperative blood loss was 5–50 ml. The pathologic examination revealed 19 cases of neuroblastoma, 11 cases of ganglion neuroblastoma, and 53 cases of ganglionoma. All patients accepted chest CT on the 1–2 days after operation and the chest tubes were removed on the 2–3th day post‐operatively. 12 patients developed Horner syndrome, and no other complications such as atelectasis and pneumonia occurred. N‐myc gene test was routinely performed in malignant patients. Three cases were positive, and 27 cases were negative. The patients whose N‐myc gene tests were positive received routine chemotherapy for 3–6 months. The other patients were only followed up. During the following, the chest CT revealed that no recurrence or other complications occurred.
Conclusion: Thoracoscopic surgery for the treatment of mediastinal neurogenic tumors is safe and feasible in selected patients. Compared with open surgery, it has better vision, less trauma and complications, shorter hospital stay and better cosmetic results. Choosing the right cases and strictly grasping the indications maybe the key to ensure successful operation.
QS106 ROBOT‐ASSISTED LAPAROSCOPIC PYELOPLASTY (RALP) IN CHILDREN WITH HORSESHOE KIDNEYS: RESULTS OF A MULTICENTRIC STUDY.
1Division of Pediatric Urology, Federico II University of Naples, Naples, Italy, 2Division of Pediatric Urology, Meyer Children Hospital, Florence, Italy, 3Division of Pediatric Urology, Hôpital Necker‐Enfants Malades, Paris, France, 4Division of Pediatric Urology, Ospedale Maggiore Policlinico, Milan, Italy, 5Division of Pediatric Urology, Istanbul Medeniyet University, Istanbul, Turkey
Background: A limited evidence is currently available about the role of minimally invasive surgery (MIS) for treatment of symptomatic pelvi‐ureteric junction obstruction (PUJO) in children with horseshoe kidneys (HSK). This multicentric study aimed to report our experience with robot‐assisted laparoscopic pyeloplasty (RALP) in children with HSK.
Methods: The records of 14 patients (11 boys and 3 girls with an average age of 9 years), who underwent RALP for repair of PUJO in HSK in 5 international pediatric urology units over a 5‐year period, were retrospectively reviewed. The transperitoneal robotic ports were placed more caudally than usual for improved access to the PUJ. A dismembered pyeloplasty with no division of the isthmus was performed in all cases.
Results: The average operative time including docking was 143.5 minutes (range 100–205). No conversions to laparoscopy or open surgery neither intra‐operative complications occurred. Patients were discharged on post‐operative day 2 following catheter and drain removal. The JJ stent was removed at mean 33 days postoperatively. Overall success rate was 92.8%. As for postoperative complications, we recorded a urinary tract infection (UTI) and stent‐related irritative symptoms, managed with medical therapy, in 2 patients (II Clavien) and an anastomotic stricture in one patient needing surgical revision with no further recurrence (IIIb Clavien). At follow‐up, all patients (one after redo‐surgery) reported complete resolution of symptoms, improvement of hydronephrosis on ultrasound and no residual obstruction on diuretic renogram.
Conclusions: Our experience suggested that RALP in HSK is safe, feasible and with good medium‐term outcomes in expert hands. An accurate pre‐operative planning associated with a standardized technique are key‐points to achieve good surgical and functional outcomes in these challenging cases. The da Vinci robot technology offers the advantages of MIS procedures and overcomes the technical challenges of laparoscopic approach.