
Abstract
Background:
The Chinese minimally invasive surgical robot system “Micro Hand S” was developed in 2013. However, there was no bariatric surgery performed with the “Micro Hand S” surgical robot. We first aim to report our experience with the “Micro Hand S” robotic-assisted sleeve gastrectomy and evaluate the safety and feasibility of the “Micro Hand S” surgical robot.
Methods:
Between March 2018 and November 2019, sleeve gastrectomies were performed with the “Micro Hand S” robotic system on 7 consecutive patients by a trained surgeon–assistant team. Preoperative, intraoperative, and postoperative clinical data were collected. A questionnaire was used to investigate surgeons' satisfaction with the “Micro Hand S” robot platform.
Results:
All the patients underwent successful operations. There were no cases of perioperative mortality and complications. The intraoperative blood loss was 20.8 ± 3.6 mL. The average overall operating time was 166.4 ± 16.1 minutes. The weight, body mass index, waist circumference, and hip circumference decreased significantly at 3 months (all P < .01) and 6 months (all P < .01) postoperatively. The percentage excess weight loss was 62.6% ± 10.3% and 85.9% ± 13.3% at 3 and 6 months postoperatively. Surgeons were satisfied with the “Micro Hand S” surgical robot performance in sleeve gastrectomy. Eighty percent of surgeons would incline to use it again.
Conclusions:
The first use of the “Micro Hand S” robotic surgical platform in sleeve gastrectomy was carried out successfully. The perioperative outcomes are satisfying. Further comparative and large-sample studies are warranted to verify our preliminary outcomes.
Introduction
Minimally invasive surgery techniques, initially laparoscopic and then robotic approaches, have increased significantly in certain areas, such as general, cardiothoracic, gynecologic, and urological surgery at present. 1 The data showed that in the past few years, the da Vinci robotic platform has emerged as an attractive technology in bariatric surgery. 2 Currently, only the da Vinci surgical robot is authorized for clinical surgery by the Food and Drug Administration (FDA). 3 There is a huge absence of competition in the robotic surgery market. 4 The Chinese minimally invasive surgical robot system “Micro Hand S” was developed by Central South University and Tianjin University in 2013. 5 It has been applied in cholecystectomy, appendectomy, and colorectal surgery successfully 6 ; however, no bariatric surgery was performed with the “Micro Hand S” surgical system. Sleeve gastrectomy is a relatively simple procedure compared with Roux-en-Y gastric bypass; taking it into account as an appropriate resident training case for robotic surgery,7,8 we performed the first series of the “Micro Hand S” robotic-assisted sleeve gastrectomies (RASGs). The objective of this study is to report our robotic sleeve gastrectomy experiences and evaluate the safety and feasibility of the “Micro Hand S” robotic approach.
Materials and Methods
Participants
We performed RASG on 7 consecutive patients between March 2018 and November 2019. All the patients were evaluated preoperatively by the multidisciplinary team. The inclusion criteria for surgery were as follows: (1) obese patients with a body mass index (BMI) ≥32.5; (2) patients with a BMI between 27.5 and 32.5 who obtained unsatisfactory results after receiving lifestyle and medical therapies and concurrently had obesity comorbidities or at least two additional components of metabolic syndrome; and (3) patients between 16 and 65 years. The exclusion criteria included the following: (1) T1DM, gestational diabetes, and other non-T2DM; (2) drug or alcohol abuse, or severe mental illness; (3) dysgnosia or intellectual immaturity; and (4) general conditions that caused intolerance of anesthesia or surgery. All patients were followed at 3 and 6 months postoperatively. The overall operative time, intraoperative blood loss, pre- and postoperative anthropometry indices, including body weight, BMI, waist circumference (WC), and hip circumference (HC) were collected. Besides percentage excess weight loss (% EWL), perioperative and postoperative morbidity were recorded. % EWL = (weight loss/baseline excess weight) × 100%, where baseline excess weight = baseline weight − ideal weight. The ideal weight was based on a person's weight at a BMI of 25 kg/m2. Questionnaires were administered to survey 5 surgeons' satisfaction with robotic surgery. The questionnaire used a five-point Likert scale, where 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, and 5 = strongly agree. Its items included the convenience of docking, inserting, and removing robotic instruments, the quality of the video system, the less surgeon fatigue from the operation, and the appropriateness of operation time. The questionnaire also investigated whether surgeons would incline to use the “Micro Hand S” surgical robot again.
The “Micro Hand S” system and surgical procedure
The “Micro Hand S” robot is a master–slave system consisting of a surgeon console and a slave cart, as shown in Figures 1 and 2. Other accessories include a three-dimensional (3D) endoscopic and camera system (Fig. 3), surgical instruments, and trocars. After four trocars were inserted as four ports (camera port R0 is for placing the robotic 3D endoscope, robotic instrument ports R1 and R2 are for placing the robotic instrument, and accessory port A0 is for assisting surgery, as shown in Fig. 4), the “Micro Hand S” robot was docked and set up. The surgeon performed an operation via two master manipulators of the surgeon console, and the two assistants assisted the operation beside the slave cart. The first step was to release the gastrocolic ligament in contact with the gastric wall and conduct devascularization from the greater curve of the stomach in the prepyloric region through the short gastric vessels to the angle of His by using the “Micro Hand S” harmonic scalpels. Hiatal laxity was sutured if present. Instead of a bougie, a gastroscope was passed to the pylorus by the assistant as a guide to allow the realization of a narrow gastric sleeve. Continuous stapling started 5 cm from the pylorus toward the angle of His by using a linear stapler via the help of the robotic assistant port to resect the stomach. After gastric resection, staple-line reinforcement was performed with a running absorbable braided 3-0 suture to prevent leakage and hemorrhaging. All preparations of the stomach were made by the console surgeon, and stapling was performed by the assistant. Finally, the resected stomach specimen was removed through the accessory port (A0).

Surgeon console of the robot: ① master manipulators, ② image display system, and ③ control panel.

Slave cart of the robot: ① slave manipulators, ② suspension arm, and ③ column.
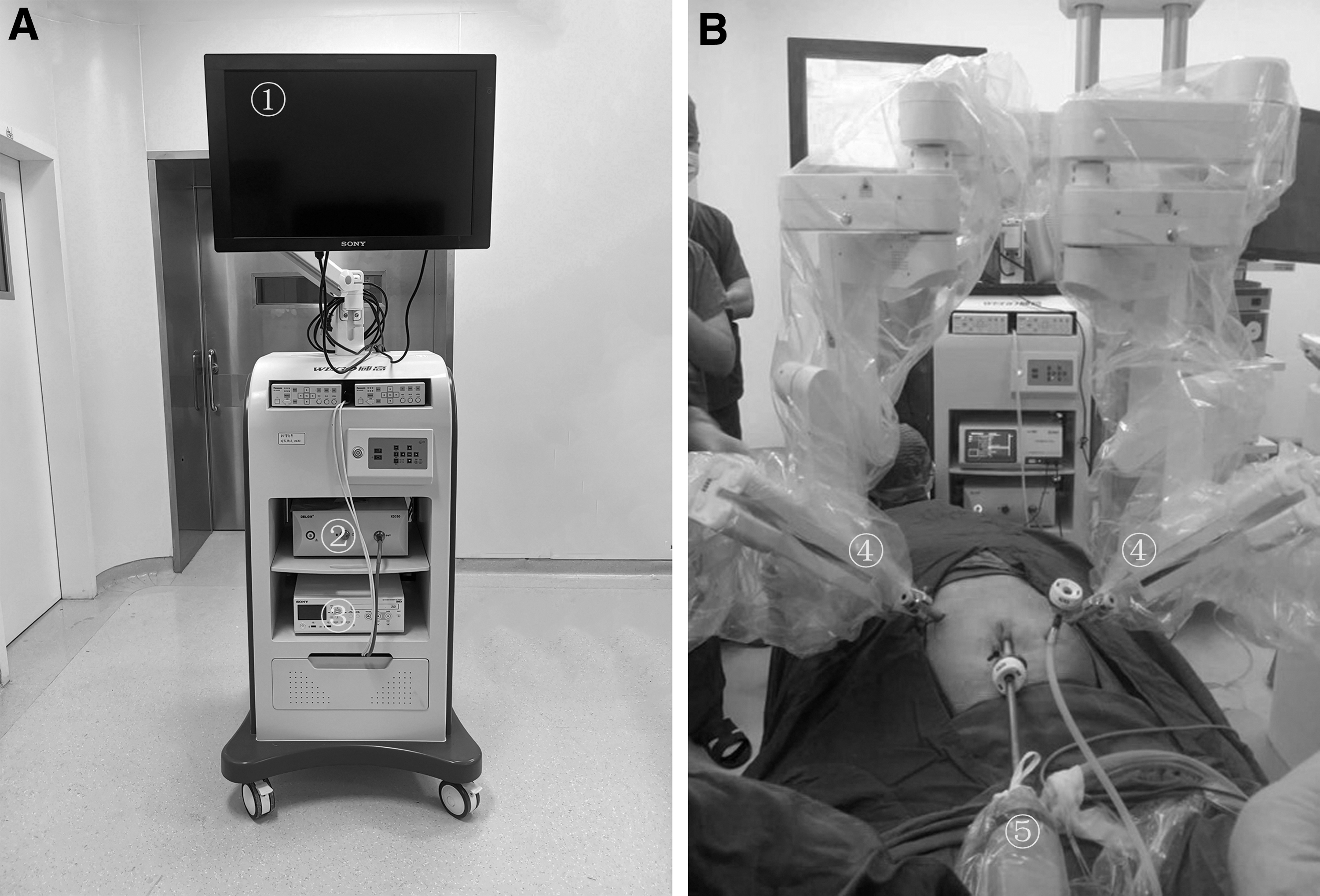
3D endoscopic and camera system:

Locations of the 3D endoscopic and camera port (R0), robotic instruments (R1 and R2), and the accessory port (A0).
Statistical analysis
SPSS version 21.0 (IBM; SPSS Statistics) was used to analyze the data. The results were expressed as the means ± standard deviations. Paired-samples t-tests were performed to analyze the changes of data between the baseline and 3 or 6 months postoperatively. All tests were considered statistically significant for P values < .05.
Results
Perioperative outcomes
Seven patients received the “Micro Hand S” RASG successfully. Baseline characteristics of patients in terms of age, sex, weight, BMI, WC, and HC are described in Table 1. No patients experienced perioperative mortality. In terms of perioperative complications, all the patients had a smooth perioperative period and recovered well. There were no cases of surgical site infection, gastrointestinal/abdominal bleeding, or conversion to an open operation. The amount of intraoperative blood loss was 20.8 ± 3.6 mL. The overall operating time was 166.4 ± 16.1 minutes (Table 2).
Baseline Characteristics
BMI, body mass index; HC, hip circumference; WC, waist circumference.
Perioperative Clinical Variables of Patients in Robotic-Assisted Sleeve Gastrectomy
Postoperative outcomes
All anthropometric data showed evident changes compared with baseline at 3 and 6 months postoperatively (all P < .01), as shown in Table 3.
Changes of Anthropometric Indices Between Baseline and 3 or 6 Months Postoperatively
P < .01 compared with baseline.
EWL, excess weight loss.
Surgeons' satisfaction survey
According to the surveys (Table 4), surgeons were satisfied with the convenience of docking, inserting, and removing robotic instruments, the quality of the video system, and the less fatigue from the operation. Though they considered that it was out of the appropriateness in total operation time (scores), 80% of surgeons would incline to use it again.
Survey of Surgeons' Satisfaction with the “Micro Hand S” Surgical Robot Platform
Likert scoring degree: 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree.
Discussion
This is the first application of the “Micro Hand S” robotic surgical system for treatment of obese patients. Surgeons who had previous laparoscopic experience and received robotic training performed these surgeries. In the present series, RASG was performed safely on 7 patients, and no perioperative mortality and complications appeared. Standard laparoscopy has some limitations, including the straight rigid instruments, limited degrees of freedom, two-dimensional image platform, and poor ergonomics of the instruments. However, problems related to thick abdominal walls and visceral fat as well as limited space to maneuver the instruments were always encountered in bariatric surgery. Compared with laparoscopy, the “Micro Hand S” robot platform possesses a 3D image system and has instrument tips that rotate and angulate in multiple directions, which is optimal for the identification of small anatomical structures within the narrow cavity. Hence, robotic surgery could present the advantage of using the robot over standard laparoscopy in bariatric procedures. In the surgical procedure of releasing the fundus of the stomach, we need to conduct devascularization of short gastric vessels. Nevertheless, short gastric vessels are behind the fundus of the stomach, which makes it difficult for laparoscopy to fulfill devascularization. We found that it could be more dexterous for the “Micro Hand S” robot to handle this. With the “Micro Hand S” robot, the surgeon is seated comfortably at a console, the hands are positioned in a natural forward position, and the forearms are given a rest to lean on, which alleviates much stress on the operation for surgeons and filters out hand tremors. Based on the surgeons' satisfaction survey, surgeons who participated in surgical robotic-assisted sleeve gastrectomy also recognized that robots have their unique operational advantages. All these may bring about less tissue damage and alleviate blood loss. Our data indicated that the blood loss was 20.8 ± 3.6 mL. According to our experiences, we consider that surgeons who perform sleeve gastrectomy with the “Micro Hand S” surgical robot should pay attention to the following matters: (1) locations between each port require a longer distance than laparoscopic ports relatively to ensure adequate space between the arms and minimize the appearance of external and internal collisions; and (2) differing from the da Vinci robot system, the “Micro Hand S” surgical robot is designed with master–slave motion mapping strategies. 9 At the current stage, the surgeon's movements could be downscaled by the motion of the instrument tip in portions of 1/10, 1/6, or 1/3. This function facilitates surgeons to carry out a refined operation. In our series of RASG, it needs to be adjusted to 10:1 when the gastric fundus is dissociated, whereas it is 3:1 in the other gastric parts. Our clinical data showed that the mean overall operative time was 166.4 ± 16.1 minutes. In our experience, these data are longer than those of laparoscopy, and our surgeons acknowledge that robotic surgery takes a much longer surgical time. It is known that when a new equipment and technique is to be used in surgery, a learning curve must be taken into account. This study was the preliminary application of the “Micro Hand S” robot platform in sleeve gastrectomy. All of the docking and setup times were relatively longer in the early stage, which is a common problem in robotic surgery. In fact, research has manifested a reduction of the learning curve when bariatric surgery is performed on the robotic platform,10,11 and a trained surgical team could reduce these times. One study has shown that 25 cases are required to achieve familiarity in da Vinci RASG. 12 We did not establish the robotic surgery learning curve, but we found increased experiences coupled with a reduction in the operative time. Overall, it is found that surgeons who participated in the “Micro Hand S” surgical robotic-assisted sleeve gastrectomy felt satisfied with the robotic performance in the survey of the satisfaction of surgeons; though they considered it was out of the appropriateness in total operation time, most of the surgeons would incline to use it again.
According to current research, the surgical robot as a new technique in bariatric surgery seems not to be superior to traditional laparoscopic surgery in terms of efficacy of weight loss. It is reported that after the da Vinci RASG, patients experienced weight loss comparable to that after laparoscopic sleeve gastrectomy. Research 13 assessed postoperative BMIs at 6 and 12 months and found that there were no significant differences in the BMIs between the RASG group and the LSG group. In another nonrandomized and controlled retrospective review, 14 the % EWL and BMI were compared at 3 months, 6 months, 9 months, 1 year, 2 years, and 3 years postoperatively between an RASG group and an LSG group, and no differences between the groups were found. Similarly, the mean BMI decrease was not different in both groups. Our data showed that anthropometric indicators (weight, BMI, WC, and HC) decreased notably at 3 and 6 months after surgery. The % EWL was 62.6% ± 10.3% and 85.9% ± 13.3% at 3 and 6 months postoperatively. Though a comparative analysis was absent in our series of sleeve gastrectomy, the short-term results showed that the “Micro Hand S” surgical robotic-assisted sleeve gastrectomy provided an evident weight loss effect.
Conclusion
In conclusion, the first series of sleeve gastrectomies assisted by the “Micro Hand S” robot system were carried out successfully. The clinical safety and efficacy need to be confirmed further in a large sample along with long-term outcomes.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the New Xiangya Talent Projects of Third Xiangya Hospital of Central South University [Grant No. JY201628].