
Abstract
Background:
This study evaluates the feasibility, safety, and clinical results of the self-pulling and latter transected delta-shaped anastomosis (Delta SPLT) in totally laparoscopic distal gastrectomy (TLDG) for gastric cancer.
Methods:
We performed a retrospective study of 66 patients with gastric cancer undergoing laparoscopic distal gastrectomy with Billroth-I anastomosis from May 2017 to December 2018 in Zhoushan Hospital. TLDG with Delta SPLT was carried out in 26 patients (Group 1), and TLDG with conventional delta-shaped anastomosis (DA) was performed in 40 patients (Group 2). Statistical analysis was conducted to compare clinical data between the two groups.
Results:
All patients successfully underwent TLDG. There were no significant differences between the two groups in terms of demographic indicators, operation time, anastomosis time, intraoperative blood loss, number of lymph nodes harvested, and resection margin (all P > .05). The gastrointestinal functional evaluation index (first flatus, first liquid/semigeneral diet foods, and out-of-bed mobilization) and hospital stay did not differ between the two groups, but the mean hospital charges were significantly lower in Group 1 than in Group 2 (P < .05). No difference was observed in the overall postoperative complication rate (P > .05). However, Group 1 had a lower incidence of complications associated with anastomosis (3.8%, versus 7.5% in Group 2; P = .016).
Conclusions:
Delta SPLT is potentially a safe, feasible, and reproducible reconstruction option for TLDG, and was superior to conventional DA in terms of hospital charges and complications related to anastomosis.
Introduction
With the rapid development of laparoscopic technology and devices, laparoscopic radical gastrectomy is being performed worldwide. Although the standard procedure of laparoscopic gastrectomy with D2 lymph node dissection has been established, laparoscopic intracorporeal anastomosis after gastrectomy remains a significant challenge for many surgeons.
Owing to the upsurge in production of advanced stapling devices, the number of totally intracorporeal anastomosis procedures has risen, making it possible to perform totally laparoscopic gastrectomy (TLG). In 2002, Kanaya and colleagues first reported a Billroth-I delta-shaped anastomosis (DA) in totally laparoscopic distal gastrectomy (TLDG). 1 Randomized controlled trials indicated that DA was a safe and efficient method during the learning curve, and was easily adoptable by surgeons after radical gastrectomy. 2
Although conventional DA became an established procedure for intracorporeal Billroth-I anastomosis, it continued to face several technical and economic problems, 3 which Hong J et al. attempted to solve by developing the self-pulling and latter transected delta-shaped anastomosis (Delta SPLT) in TLG. The Delta SPLT method effectively simplified the anastomosis procedure and reduced the required quantity of linear staplers.4,5 Generally, only two linear stapler cartidges are required to complete the gastric-duodenum (GD) anastomosis in Delta SPLT, and three staplers are applied to perform conventional DA because an extra linear stapler cartidge is used to cut completely the duodenum after D2 lymph node dissection.
However, to date there have been few reports on the effect of the Delta SPLT procedure in TLDG, which our institution has adopted in recent years. The aim of this study was to evaluate the safety, feasibility, and clinical results in patients undergoing Delta SPLT for gastric cancer.
Materials and Methods
Patient population
DA was performed for 40 patients with gastric cancer who underwent TLDG (Group 2) at our institution between May 2017 and May 2018. After the Delta SPLT procedure was introduced in May 2018, it replaced conventional DA, and 26 patients underwent the Delta SPLT procedure (Group 1). Among these 66 gastric cancer patients, a retrospective trial was carried out from May 2017 to December 2018. There were no statistically significant differences in demographic indicators between the two groups (Table 1).
Comparison of Patient Characteristics of the Two Groups (x ± s)
TNM, primary tumor (T), regional nodes (N), and metastasis (M).
Surgical procedures
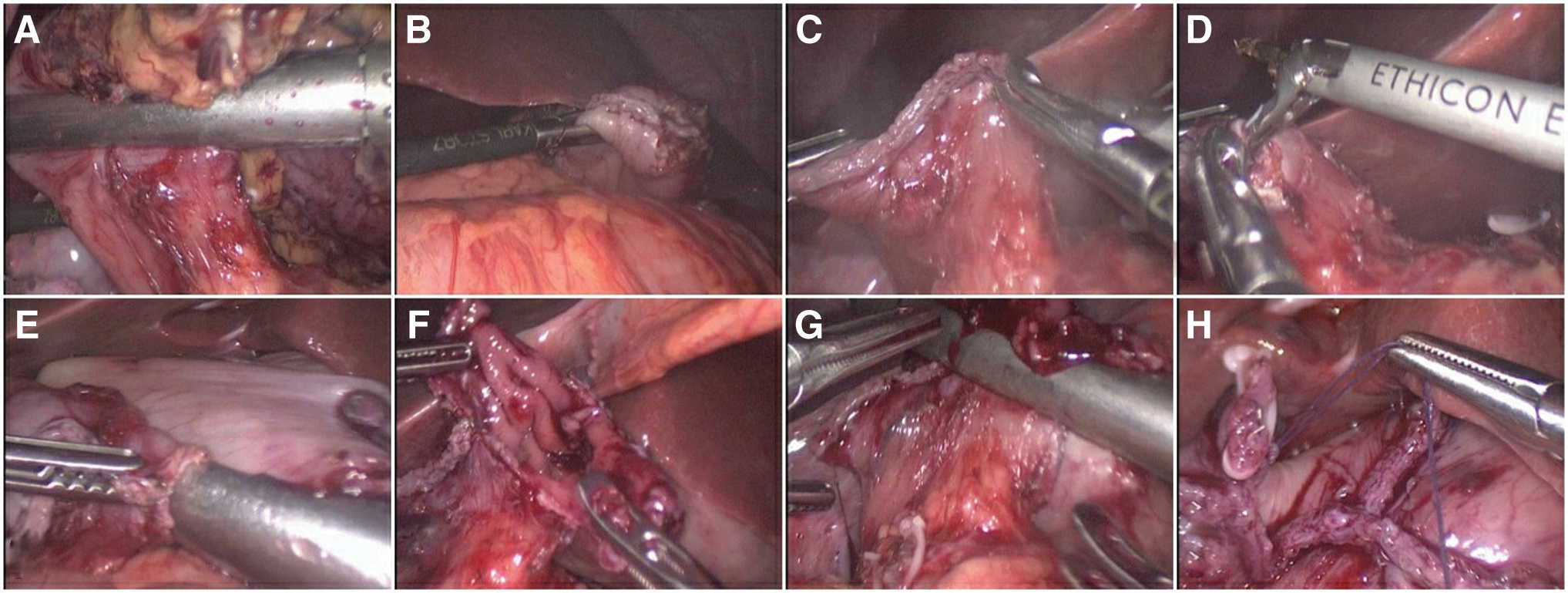
All operations were performed by the same surgical team that was proficient in laparoscopy and gastrectomy. The Delta SPLT procedure was performed according to the original procedure developed and reported by Hong J et al. (Fig. 1). 4 After general anesthesia, the patient was placed in supine position with the legs apart and head elevated ∼10° to 20°. The operation was conducted with carbon dioxide insufflation through subumbilical incision pressure of 12 mmHg. During the operation, five trocars were inserted (one 10 mm, one 12 mm, and three 5 mm). The surgeon divided the stomach and duodenum, D2 lymph node dissection was carried out using standard fashion, and the stomach and duodenum were routinely mobilized.

Delta SPLT anastomosis procedure. The pylorus was then ligated using a hemp rope
After evaluating the tension between the stomach pouch and the duodenal stump, linear staplers were inserted to perform stomach pouch transection until the stomach was completely cut off; the pylorus was then ligated using a hemp rope 12–15 cm in length (Fig. 1A). During the course of reconstruction, the ligature rope was held to drag the proximal duodenum to rotate 90° in the counterclockwise direction (Fig. 1B), allowing easier attachment of it to the stomach segment. Next, small holes 1.0 cm in diameter were created on the posterior wall of the proximal duodenum (Fig. 1C) and on the greater curvature of the remnant stomach (Fig. 1D). The upper and lower anvils of a 60-mm linear stapler were inserted into each hole, to attach the posterior walls of the duodenum to the stomach pouch (Fig. 1D, E).
Thereafter, the duodenum was pulled up toward the proximal stomach to create a V-shaped connection of the anastomotic line (Fig. 1F). A functional lateral/lateral anastomosis of the stomach pouch and the duodenal stump was carried out, and the common gastrojejunal incision was closed by a 60-mm linear stapler clamping transversely to the long axis of the duodenum, and the proximal duodenum above the level of the entry hole was simultaneously transected by the same stapler (Fig. 1G), and the Delta SPLT procedure was finished (Fig. 1H).
If necessary, laparoscopic reinforcement suture was carried out using barbed suture. After removal of the specimen, a closed drain was placed on the dorsal side of the stomach pouch. No bleeding was found through visual inspection, and the pneumoperitoneum was closed.
The conventional delta-shaped gastroduodenostomy has been described in detail previously (Fig. 2). 1 After full mobilization around the stomach and duodenum with D2 lymph node dissection, the stomach and duodenum were transected completely in the respective predetermined position using endoscopic linear staplers instead of using a ligature rope to pull the pylorus (Fig. 2A, B).
DA anastomosis procedure. After full mobilization around the stomach and duodenum with D2 lymph node dissection, the stomach and duodenum were transected completely in the respective predetermined position using endoscopic linear staplers instead of using a ligature rope to pull the pylorus
Under the guidance of surgical instruments, the duodenal stump was pulled up close to the proximal stomach to complete the gastrointestinal reconstruction (Fig. 2C). The small holes were made on the stomach pouch and duodenum. A 60-mm endoscopic linear stapler was inserted into each incision (Fig. 2D, E), and the forks of the stapler were closed to create a V-shaped anastomosis on the posterior wall (Fig. 2E), then the common stab incision was pulled and closed with the stapler (Fig. 2F, G). The DA anastomosis was finished (Fig. 2H). The subsequent surgical procedure was similar to that of the aforementioned Delta SPLT.
Data collection
For each group, the patients' clinicopathological characteristics associated with the surgical techniques were collected, including operative time, anastomotic time, intraoperative blood loss, extent of lymph node dissection, histological measurement of the specimen margin, time to the first flatus passage, diet initiation, length of stay in hospital, hospitalization expenses, and complications.
The hospital charges were the sum of all medical expenses during hospital stay. In our study, the same type of staplers (ECR60-staplers, Blue staple cartridge, 3.5 mm, 6 rows; Price: ¥2208, Brand: ECHELON FLEX Johnson & Johnson) were used in both groups.
Postdischarge follow-up
Postdischarge follow-up was generally conducted through outpatient clinics. A gastroscopy was advised for all patients at 1 month postoperatively. Follow-up visits were scheduled every 3 months in the first 2 years after surgery and every 6 months thereafter, and hospital readmission rates within 3 months after surgery were recorded. The termination date of follow-up was June 2019.
Statistical analyses
Statistical analyses were performed using the SPSS version 18.0 statistical software package (SPSS, Chicago, IL). Data are presented as the mean ± standard deviation. Comparisons of quantitative data in both groups were analyzed using t-tests, and comparison of postoperative complications was analyzed using the Chi-squared test. P values of <.05 were considered significant.
Results
Intraoperative outcomes
The demographics of the two groups are outlined in Table 1and there was no statistical difference in any of the variables assessed. Table 2 shows that the median operative and anastomotic time for the Delta SPLT procedure was shorter than that for the conventional DA procedure, although the difference was not statistically significant. In addition, Group 1 had a significantly lower median blood loss than Group 2 (140 ± 45.5 mL versus 160 ± 30.5 mL), but this difference was not statistically significant. The two groups did not differ in terms of number of lymph nodes harvested, tumor size, and surgical margins (Table 2).
Comparison of Intraoperative Outcomes of the Two Groups
Postoperative outcomes
The gastrointestinal functional evaluation index (with parameters such as first passage of flatus, first consumption of liquid/semigeneral diet foods, and out-of-bed mobilization) was measured.
In both groups, oral feeding was started after first flatus passage, beginning with clear fluids and gradually progressing to a normal diet over a period of 2–6 days. There was consensus regarding postoperative advancement of diet for these patients, and appropriate dietary advice was based on gastrointestinal recovery. As shown in Table 3, there was no significant difference between Groups 1 and 2, which indicated that Delta SPLT did not influence the patients' gastrointestinal functional recovery after abdominal surgery in comparison with the conventional DA procedure.
Comparison of Postoperative Outcomes of the Two Groups
RMB, renminbi.
However, the mean hospital charges were significantly lower for Group 1 than Group 2 (P < .05). The patients should be considered ready for hospital discharge when there was tolerance of oral intake, recovery of gastrointestinal function, no severe abdominal pain, ability to mobilize and self-care, no evidence of complications or untreated medical problems, and the mean hospital stay was similar for both groups.
Postoperative complications
Postoperative complications are listed in Table 4. The overall postoperative complication rate did not differ significantly between the two groups (23.1% for Group 1 versus 22.5% for Group 2), but Group 1 had a lower incidence of complications associated with anastomosis than Group 2 (3.8% versus 7.5%, P = .016). Anastomotic hemorrhage occurred in only 1 patient of Group 1 during the operation, while in Group 2 one patient developed anastomotic stricture and one experienced anastomotic stricture and bleeding after surgery, both of whom were managed successfully by reoperation. Some adverse events other than anastomosis-related complications (delayed gastric emptying, lymphatic fistula, lung infection, and incision infection) developed in both groups.
Comparison of Postoperative Complications of the Two Groups
Data are shown as number of patients (percentage).
Post-discharge follow-up
All patients were followed up for 6–24 months. Although all patients had the same postoperative follow-up schedule, a difference arose in follow-up duration as a result of the different initial operation time and compliance. Patients underwent endoscopic examination 1 month after surgery, and gastroscopic examination revealed anastomotic patency for all patients except the aforementioned 2 patients with anastomotic stricture. Anastomotic complications occurred in 15 patients in Group 1 and in 21 patients in Group 2. All patients were followed-up within the 6 months after surgery, and afterward our cohort of patients had a lower mean followed-up rate (<29% and 27% in Groups 1 and 2, respectively) because of the patients' poor compliance, therefore, some valuable indicators such as survival time, quality of life, and disease-free survival were missing.
Discussion
Since the introduction of the delta-shaped anastomotic technique for gastric cancer in 2002 (Ref. 1 ), this approach has been accepted worldwide as a standard reconstruction method in TLDG with Billroth-I reconstruction.6,7 Although conventional DA was effective for intracorporeal gastroduodenostomy, one of its disadvantages was that it was more expensive in terms of equipment because it required multiple linear stapler cartridges,8–10 and several anastomosis-related surgical complications were reported. 11 In response to these drawbacks of conventional Delta-SA, modified intracorporeal gastrointestinal anastomosis techniques have been developed in recent years.12–14
Hong J et al. invented the novel reconstruction method of Delta SPLT in TLDG to improve conventional Delta-SA. The Delta SPLT method optimized the conventional Delta-SA approach in terms of delta-shaped anastomosis. Although Delta SPLT is also more expensive compared with open traditional radical gastrectomy, it has a greater cost-benefit advantage than conventional DA because Delta SPLT minimizes the number of stapler cartridges used. Compared with conventional Delta-SA, the Delta SPLT procedure reduced the incidence of complications related to anastomosis. Our hospital commenced performing Delta SPLT in May 2018, since then we have completed 26 cases.
One of the noticeable features of the Delta SPLT method is the “self-pulling” maneuver. In Delta SPLT, after full mobilization around the stomach and duodenum, the pylorus is fastened by a rope to perform the self-pulling process. In our experience, self-pulling can adequately mobilize the duodenum to adjust the anastomosis angle, which dramatically reduces operational difficulties. In our clinical study, both the operative and anastomotic times were shorter in Group 1 (245.3 and 30.8 minutes, respectively) than in Group 2 (262.9 and 32.5 minutes, respectively), although the difference was not statistically significant. Possible reasons for a statistically insignificant result may be related to smaller sample size and the learning curve for new surgical methods.
Another important feature of the Delta SPLT method is the “latter transection.” In conventional Delta-SA, the stomach and duodenum are transected completely before gastrointestinal reconstruction, after which the duodenal stump is clamped and pulled toward the proximal stomach by surgical instruments to complete the gastrointestinal anastomosis. Because of local point-like pulling, the partial duodenal serosal layer may be torn inadvertently during this process.
By contrast, during the “latter transection” of the Delta SPLT procedure, this duodenal transection is not performed until delta anastomosis is completed. Avoiding local point-like pulling, pulling the rope on the pylorus drags the whole duodenum to the proximal stomach and reduces the risk of duodenal injury. Moreover, by eliminating an extra step in the conventional Delta-SA method, transection of the duodenum and closure of the entry hole can be finished at the same time by using a single stapler. Therefore, the “latter transection” not only simplifies the anastomosis procedure but also decreases the number of linear staplers used. The same types of staplers were used in both groups in our study, but the reduction in linear staplers in Group 1 led to less operating room expense and significantly lower mean hospital charges.
Regarding the complications related to anastomosis, the morbidity rate of Group 1 (3.84%) was lower compared with Group 2 (7.5%), owing to the optimization of surgical procedures. Of all the patients in Group 1, only 1 experienced a minor anastomotic hemorrhage during the operation, the bleeding being controlled by a barbed suture. Among the 40 patients in Group 2, one developed anastomotic stricture and another experienced anastomotic stricture and bleeding after surgery, both of whom were treated successfully by reoperation. Anastomotic leakage, a serious complication of anastomosis, did not occur in either group.
Some complications unrelated to anastomosis did occur in both groups, including delayed gastric emptying, lymphatic fistula, incision infection, and pulmonary infection, but the overall postoperative complication rate did not differ significantly between the two groups. The clinicopathological characteristics of the patients in both groups were comparable, with no significant differences in the number of lymph nodes harvested, proximal resection margin, or postoperative outcomes (e.g., first liquid diet, first flatus, out-of-bed mobilization, and hospital stay). These results indicated that the surgical safety of Delta SPLT was similar to that of conventional DA, and the chosen anastomotic technique was not a risk factor for surgical complications.
Conclusions
Delta SPLT promises to become a safe, feasible, and reproducible reconstruction option for TLDG, and was superior to conventional DA in terms of hospital charges and complications related to anastomosis. Our clinical practice supports a more widespread implementation of this strategy, and we expect that more desirable surgical outcomes can be achieved as more surgeons gain further experience of this procedure.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.