
Abstract
Background:
The injection of tissue adhesives has been proposed as an alternative to standard laparoscopic inguinal hernia repair but no evidence is available in the pediatric population. This study aimed to evaluate safety, efficacy, and feasibility of injection of tissue adhesives for inguinal hernia repair in a rabbit model.
Materials and Methods:
Thirty-six New Zealand White male rabbits underwent laparoscopic inguinal hernia repair. In each animal, the hernia defect was repaired using glue on the right side and purse-string suture on the left side. The animals were divided in 3 groups, each 1 of 12 animals, according to the glue used: Glubran 2® (cyanoacrylate), Histoacryl® (cyanoacrylate), and BioGlue® (bovine serum albumin-based). For each group, 6 animals were sacrificed at 7 days postoperatively, and 6 animals at 90 days postoperatively. Histopathological exam of testis and spermatic bundle was performed.
Results:
The hernia defect was successfully closed on both sides in all cases. The injection of glue was faster than suture repair (P = .001). Postoperative complications (epiploon-parietal adhesions, spermatic vessel ectasia, and hydrocele) rate was significantly higher on the right side compared to the left side at both short- and long-term follow-up (P = .001). Furthermore, a lower maturity of testicles treated by adhesive compared with suture was histologically demonstrated at both short- and long-term follow-up (P = .001).
Conclusions:
The present experimental study confirmed the feasibility and efficacy of inguinal hernia repair by injection of tissue adhesive. However, several critical issues emerged about the safety of this technique. The use of glue was associated with higher incidence of postoperative complications and significant decrease of testicular maturity compared with standard suture repair. Based upon these preliminary results, repair using suture remains the standard of care for inguinal hernia in children. Further experimental studies are needed to assess the safety of injection of tissue adhesives for pediatric inguinal hernia repair.
Introduction
The incidence of inguinal hernia in children ranges from 0.8% to 4.4%. 1 There is still an ongoing debate about the best approach between open surgery and laparoscopy for inguinal hernia repair in children.2,3 In the recent years, the laparoscopic approach has gained a widespread diffusion for this indication. 1 However, the laparoscopic procedure requires advanced laparoscopic skills, related to intracorporeal suturing and a long learning curve, especially in premature babies with low weight at birth, because of the very limited working space.
More recently, the injection of tissue adhesives has been reported in experimental studies on rat models as a feasible alternative to the traditional technique for inguinal hernia repair.4–6 The results of these studies were conflicting and contradictory: some authors showed effective repair of inguinal hernia at the time of surgery, no recurrence at long-term follow-up, no damage to spermatic cord structures, and no clear impact on fertility4,5 whereas other authors reported concerns about an increased risk of intestinal obstruction by adhesive syndrome, hernia recurrence, postoperative hydrocele, and long-term carcinogenesis. 6 In adults, the technique of inguinal hernia repair involves the use of a mesh to cover the defect. Fixing the mesh with surgical adhesives was introduced as a method to reduce tissue damage and improve long-term results.7–9 Little evidence is currently available about safety and efficacy of tissue adhesives for inguinal hernia repair in children. 10
A pilot clinical study was started in 2015 at Great Ormond Street Hospital (London, United Kingdom), to assess feasibility and outcome of inguinal hernia repair using tissue adhesive in children. The procedures were effectively performed using the FDA-approved and CE-marked BioGlue® (purified bovine serum albumin [BSA] added with glutaraldehyde), reporting no immediate adverse effects in all patients. However, during the long-term follow-up, development of ipsilateral hydrocele was observed in some children. The morphology and the vascular supply of testes were normal at Doppler ultrasound. However, the surgeons decided to discontinue the study since they hypothesized that the postoperative hydrocele, which was considered an unexpected adverse event, was due to a local tissue reaction to the glutaraldehyde present in the adhesive. Based upon these preliminary results, a novel experimental study was planned to further assess feasibility and safety of inguinal hernia repair with injection of tissue adhesive.
This multi-institutional experimental study aimed to evaluate safety, efficacy, and feasibility of injection of tissue adhesives for inguinal hernia repair in a rabbit model.
Materials and Methods
Thirty-six male rabbits New Zealand White strain with an average weight of 4.2 kgs (range 2–6) underwent laparoscopic inguinal hernia repair. In each animal, the hernia defect was repaired using tissue adhesive on the right side and purse-string nonabsorbable suture on the left side, according to the case cross-over model. The animals were divided in 3 groups, each 1 of 12 animals, according to the glue used for the closure of the hernia defect: Glubran 2® (cyanoacrylate basis glue, modified by the addition of a monomer synthesized by the manufacturer) (GEM Italy) [G1], Histoacryl® (N-butyl-2-cyanoacrylate [b-CNA]; B. Braun Milan SpA) [G2], and BioGlue (purified BSA added with glutaraldehyde; CryoLife, Inc.) [G3]. For each group, 6 animals were sacrificed at 7 days postoperatively (Line 1) and other 6 animals, if survived, were sacrificed at 90 days postoperatively (Line 2). After each sacrifice, gross examination and histopathological exam of the removed testes with the related spermatic bundle were performed.
The use of adhesives was compared to standard suture regarding the following items: efficacy, postoperative complications (hydrocele, epiploon-parietal adhesions, and spermatic vessel ectasia), and histopathological modifications (maturation, fibrosis, and distortion of seminiferous tubules). Furthermore, the different adhesives were compared among them, to establish the glue with the better outcome.
The statistical analysis was performed using χ 2 test with Yates' correction. A P-value <.05 was considered statistically significant.
The study received ethical approval from the National Health Institute. It also received appropriate Institute Review Board (IRB) approval at Federico II University of Naples, in Naples, Italy.
Surgical technique
After induction of general anesthesia with endotracheal intubation, a 5-mm trocar was inserted in the umbilicus via open approach for the 0° 5-mm optic. After induction of the pneumoperitoneum, two 3-mm working trocars were placed under vision in the right and left iliac fossa and in triangulation with the optic port. On the left side, the peri-orificial peritoneum was divided with the monopolar hook and a purse-string suture was performed with nonabsorbable suture, that was introduced trans-abdominally (Fig. 1). Thereafter, the tissue adhesive applicator was inserted through the right 3-mm trocar and brought to the level of the right inguinal orifice. The instillation of the tissue adhesive (max 2 mL) was followed by external compression on the inguinal region for about 2 minutes. The effective closure of the hernia defect was visually confirmed before removal of laparoscopic instruments (Fig. 2). The trocars' orifices were closed with absorbable sutures. All the surgical interventions were recorded.

The left inguinal orifice was closed with nonabsorbable suture.
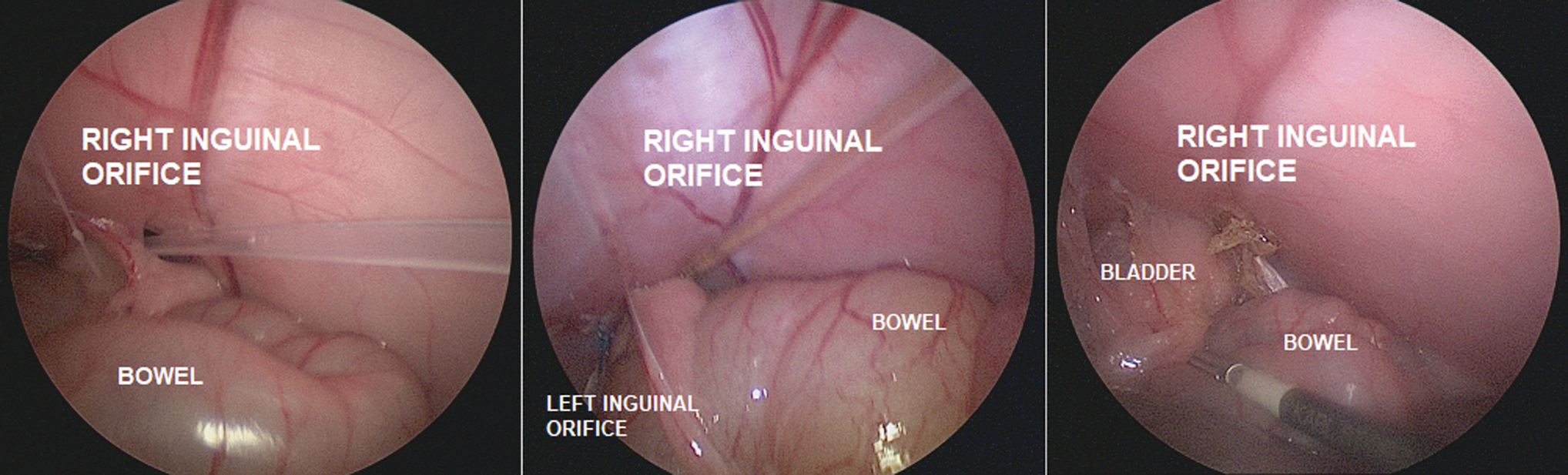
The right inguinal orifice was closed by injection of tissue adhesive.
Supplementary Video S1 shows all steps of the surgical technique.
Postoperative evaluation
During the first 24 hours postoperatively, the rabbits were strictly monitored to evaluate weight loss, food recovery time, and early postoperative complications including hydrocele, hernia recurrence, bowel obstruction, and systemic reactions to tissue adhesive.
Necropsy and histopathological exam
The histopathological exam was performed by a pathologist, who was blinded to the group identity of the specimens. The following postmortem evaluations were performed in all survived animals of each group at 7 and 90 days postoperatively.
Evaluation of repair and epiploon-parietal adhesions
On gross examination, the integrity of the hernia defect closure, the presence of peritonitis and epiploon-parietal adhesions, defined as visceral adhesions to abdominal wall at the operative site, were documented.
Assessment of local tissue reaction
The spermatic cord and the testis were removed bilaterally and fixed in 5% paraformaldehyde. The spermatic cord and the testis were cross-sectioned (4 μm sections) and treated with hematoxylin–eosin and red picrosirius staining. The tissues were evaluated for patency of the vas deferens/testicular vessel, architecture of testicular tissue, infiltration of inflammatory cells, fibroblasts, elastic fibers, neovascularization, and collagen content. The severity of fibrosis and tubular distortion, defined as swelling, sloughing, and disorganization of the seminiferous tubules, were both scored on a 4-point scale, based on the grading system proposed by Dixon et al.,11,12 with 0 = no abnormality; 1 = mild distortion affecting <25% of the tubules; 2 = moderate distortion affecting 25%–75% of the tubules; and 3 = severe distortion affecting >75% of the tubules.
Assessment of testicular maturity
The testes were scored on a scale of increasing maturation from 1 to 5: (1) the leading wave of germinal cells in most tubules is spermatogonia and a few tubules contain spermatocytes; (2) the leading wave of germinal cells in most tubules is spermatocytes; (3) the leading wave of germinal cells is round spermatids; (4) similar to grade 3 except that a few tubules contain elongating spermatids; (5) the leading wave of germinal cells is elongating spermatids.13,14 To assess spermatogenic activity in the seminiferous tubules, the rate of tubules that showed normal spermatogenesis (score 5), hypospermatogenesis (score 3–4), and maturation arrest (score 1–2) were recorded.
Results
Line 1
The average duration of surgery using tissue adhesive (8 minutes) was significantly shorter compared to standard suture repair (16 minutes) (P = .001). The survival rate of Line 1 animals was 100%. All the animals restarted oral feeding on the first postoperative day and no postoperative weight loss was recorded. In the first 24 hours postoperatively, a right-sided hydrocele was recorded in 50% of G2 rabbits and in 33% of G3 rabbits. Neither bowel obstructions nor systemic reactions to the adhesive occurred in all animals. On gross examination, the defect appeared correctly closed on both sides in all animals. The incidence of right-sided epiploon-parietal adhesions was significantly higher in G1 (67%) and G2 (100%) compared with G3 (16%) (P = .001) (Fig. 3). No epiploon-parietal adhesions were found on the left side in all animals.

Epiploon-parietal adhesions on the right side at 7 days postoperatively.
At histopathological exam, spermatic vessel ectasia, mostly represented by spermatic vein dilation, was observed in 5 G2 rabbits (83%). Mild fibrosis and distortion (score 1) of seminiferous tubules were observed in 1 G3 rabbit (16%). The rate of seminiferous tubules that showed normal spermatogenesis (score 5) was significantly lower in the right testicle compared with the left testicle in each group (G1: 56% versus 90%; G2: 65% versus 90%; G3: 42% versus 83%) (P = .001). Conversely, the rate of tubules that showed hypospermatogenesis (score 3–4) was significantly higher in the right testicle compared with the left testicle in each group (G1: 20% versus 10%; G2: 18% versus 10%; G3: 27% versus 15%) (P = .001). Finally, the rate of tubules with maturation arrest (score 1–2) was significantly higher in the right testicle compared with the left testicle in each group (G1: 24% versus 0%; G2: 17% versus 0%; G3: 31% versus 2%) (P = .001). No difference regarding the impact on the maturity of seminiferous tubules was found among each surgical adhesive (P = .22).
Outcomes of G1, G2, and G3 groups in Line 1 are reported in Table 1.
Outcomes in G1–G2–G3 at 7 Days Postoperatively (Line 1)
Line 2
The average duration of surgery using tissue adhesive (7 minutes) was significantly shorter compared with standard suture repair (18 minutes) (P = .001). The survival rate of Line 2 animals was respectively 83% in G1, 67% in G2, and 33% in G3. Regarding the causes of death, 1 rabbit developed a severe respiratory distress causing the death 28 days postoperatively; no other evident causes of death, even at autoptic exam, were found in the other 6 rabbits that died. It was unclear if these deaths were strictly related to the surgery or the tissue adhesive that was used. All the animals restarted oral feeding on the first postoperative day and no postoperative weight loss was recorded. In the first 24 hours postoperatively, an episode of dyspnea occurred in 1 G3 rabbit (16%) whereas a right-sided hydrocele was recorded in 1 G2 rabbit (16%). No bowel obstructions occurred in all animals. On gross examination, the hernia defect appeared correctly closed on both sides in all animals. Right-sided epiploon-parietal adhesions were found in 4 G1 rabbits (67%) (P = .001). No epiploon-parietal adhesions were found on the left side in all animals.
At histopathological exam, spermatic vessel ectasia, mostly represented by spermatic vein dilation, was found in 1 G3 rabbit (16%). Severe fibrosis and distortion (score 3) of seminiferous tubules were observed in 4 G2 rabbits (75%) and in 2 G3 rabbits (33%) (Fig. 4). The rate of seminiferous tubules that showed normal spermatogenesis (score 5) was significantly lower in the right testicle compared with the left testicle in each group (G1: 62% versus 86%; G2: 71% versus 90%; G3: 50% versus 85%) (P = .001). Conversely, the rate of tubules that showed hypospermatogenesis (score 3–4) was significantly higher in the right testicle compared to the left testicle in each group (G1: 25% versus 11%; G2: 19% versus 8%; G3: 28% versus 14%) (P = .001). Finally, the rate of tubules with maturation arrest (score 1–2) was significantly higher in the right testicle compared with the left testicle in each group (G1: 13% versus 3%; G2: 12% versus 2%; G3: 22% versus 1%) (P = .001).

A marked enlargement of right spermatic cord and testicle compared with left side was observed at 90 days postoperatively.
No difference regarding the impact on the maturity of seminiferous tubules was found among each surgical adhesive (P = .51).
Outcomes of G1, G2, and G3 groups in Line 2 are reported in Table 2.
Outcomes in G1–G2–G3 at 90 Days Postoperatively (Line 2)
Discussion
With advancements in pediatric laparoscopic surgery, laparoscopic repair of inguinal hernia has become widely adopted.1–3 However, laparoscopic hernia repair requires advanced technical skills related to intracorporeal suturing and knotting, and this issue has limited its widespread use in pediatric surgical practice. The use of tissue adhesives for correction of inguinal hernia has been proposed as an attractive, easy, and reproducible therapeutic alternative, to overcome the challenges of standard suture repair. 10 Tissue adhesives have been previously employed in pediatric surgery with the aim to reduce the risk of postoperative complications, especially in cases of parenchymal resection or vascular anastomoses.15,16 They have also been applied in pediatric laparoscopic surgery as good means of controlling bleeding in the case of intervention on the spleen or liver and a valid method to complete and secure the sutures in case of organ perforation. 17
More recently, the injection of tissue adhesives has been reported in experimental studies on rat models as a feasible alternative to the traditional technique for inguinal hernia repair.4–6 The results of these studies were conflicting and contradictory: some authors showed effective repair of inguinal hernia at the time of surgery, no recurrence at long-term follow-up, no damage to spermatic cord structures, and no clear impact on fertility4,5 whereas other authors reported concerns about an increased risk of intestinal obstruction by adhesive syndrome, hernia recurrence, postoperative hydrocele, and long-term carcinogenesis. 6 Despite these concerns, Park et al. reported very promising results with laparoscopic surgical glue injection hernioplasty in children.18,19 Their method required only one working port and one camera port and b-CNA glue was adopted to close the defect after the mesothelial layer surrounding the internal inguinal ring was electrically cauterized. The main limitation of this study was that it did not include male patients to avoid potential damage to the vas deferens. Moreover, a direct comparison with conventional laparoscopic hernia repair was not performed and the follow-up was not enough long to check for recurrence.
A pilot clinical study, that was started in 2015 at Great Ormond Street Hospital (London, United Kingdom), confirmed the feasibility of pediatric inguinal hernia repair using the FDA-approved and CE-marked BioGlue surgical adhesive but concerns emerged about the clinical safety of the technique since at long-term follow-up hydrocele appeared on the side of hernia repair in some patients. The surgeons decided to discontinue the study since they hypothesized that the postoperative hydrocele, which was considered an unexpected adverse event, was due to a local tissue reaction to the glutaraldehyde present in the adhesive. Based upon these preliminary results, a novel experimental study in an animal model was planned to further assess feasibility and safety of inguinal hernia repair with injection of tissue adhesive.
We decided to enroll in our study only male New Zealand White rabbits, since the anatomy of their internal inguinal ring, that is always patent, reproduces authentically the inguinal hernia defect in children. 20 The results of the present experimental study confirmed that laparoscopic inguinal hernia repair with injection of tissue adhesive is feasible, technically easy, reproducible, not requiring advanced laparoscopic skills, with a short learning curve and a shorter operating time compared with standard laparoscopic repair using suture. The method was highly effective in our series, since no hernia recurrences were recorded at both short- and long-term assessment.
A point of debate is the influence of the type of tissue adhesive on the procedure outcome. Cyanoacrylate (CNA) polymerizes in contact with moisture, produces heat during polymerization, and releases toxic products. Short-chain CNAs can cause toxicity in human tissue, but long-chain CNAs such as b-CNA or o-can (2-octyl-cyanoacrylate) minimize tissue toxicity. 21 Since we hypothesized that postoperative hydrocele, which occurred in the previous pilot study, was a side effect of the glutaraldehyde present in the adhesive (Bioglue), we decided to adopt three different types of tissue adhesives and to compare their outcome: Histoacryl (b-CNA), Glubran 2 (CNA basis glue, modified by the addition of a monomer synthesized by the manufacturer GEM), and Bioglue (purified BSA associated with glutaraldehyde). The tested tissue adhesives showed to be equivalent in terms of applicability, intraoperative maneuverability, and efficacy. However, the study highlighted several critical issues about the safety of tissue adhesives application in children.
First, use of tissue adhesives showed a higher incidence of epiploon-parietal adhesions compared with suture repair. Histoacryl was associated with adhesions in all animals (100%) sacrificed at 7 days postoperatively, Glubran 2 was associated with a statistically equivalent incidence (67%) of adhesions at 7 and 90 days postoperatively whereas Bioglue was associated with adhesions in only 16% of the animals sacrificed at 7 days postoperatively. Despite the considerable incidence, postoperative adhesions were not clinically associated with bowel obstruction in any animals. Another consideration is that the incidence of postoperative adhesions was significantly higher in the short-term follow-up (7 days) group compared with the long-term assessment (90 days) group. This finding might be assumed to be due to the slow degradation of tissue adhesives, especially b-CNA, which usually occurs between 3 and 9 months following the application.
It should also be noted that use of Histoacryl was associated with a high incidence of spermatic vessel ectasia (83% in Line 1) and severe fibrosis and distortion of seminiferous tubules (75% in Line 2). We observed that the spermatic vein was dilated in most cases, suggesting an obstructed venous outflow due to total or partial venous occlusion. This observation would support the hypothesis that tissue adhesive could determine migration of particles that may predispose to an increased risk of venous thrombosis. However, further evidence is required to confirm this hypothesis.
The incidence of postoperative hydrocele was also not negligible, ranging from 33% in the early BioGlue group (Line 1) to 50% in the early Histoacryl group (Line 1) and 16% in the late Histoacryl group (Line 2). However, although use of Histoacryl reported the worst outcome compared with Glubran 2 and Bioglue, none of the tested adhesives showed to be the ideal product in terms of safety.
Another important finding of this study was the significant negative impact of the tested tissue adhesives on the testicular maturity compared with the standard suture. At histopathological exam, the rate of seminiferous tubules that showed hypospermatogenesis and maturation arrest in the right testicle (tissue adhesive) was significantly higher compared to the left testicle (suture) in each group at both short- (Line 1) and long-term (Line 2) evaluation, with no significant difference between the three surgical adhesives. Additionally, the incidence of severe fibrosis and distortion of seminiferous tubules was significantly higher in the long-term observation groups (Line 2) compared with the short-term follow-up groups (Line 1). These results supported the evidence of a negative long-term effect of tissue adhesives on the spermatogenesis.
In conclusion, the present experimental study confirmed the feasibility and efficacy of inguinal hernia repair by injection of tissue adhesive. However, several critical issues emerged about the safety of this technique. The use of glue was associated with higher incidence of postoperative complications and significant decrease of testicular maturity compared with standard suture repair. Based upon these preliminary results, we believe that repair using suture remains the standard of care for inguinal hernia in children. Further experimental studies are needed to assess the safety of injection of tissue adhesives for pediatric inguinal hernia repair.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.