
Abstract
Background:
The endoscopic resection of suspected gastric high-grade intraepithelial neoplasia (HGIN) may incidentally cause the patient to suffer from early gastric cancer (EGC), complicating the subsequent clinical management. Identifying the risk factors for such misstaging may help guide the clinical management.
Methods:
The information obtained from 123,460 patients, who underwent conventional upper gastrointestinal endoscopy at the First Affiliated Hospital of Nanjing Medical University from January 2010 to December 2015, were retrospectively reviewed. Patients with an initial diagnosis of HGIN underwent endoscopic submucosal dissection (ESD), and received a final diagnosis of EGC. The risk factors for the upgraded pathology and noncurative resection were analyzed.
Results:
Among the 134 patients initially diagnosed with HGIN, 35 (26.12%) patients were finally diagnosed with EGC after ESD. A lesion size of ≥2 cm (odds ratio [OR] = 5.16, 95% confidence interval [CI] = 2.04–13.05; P < .01), ≤4 biopsies taken (OR = 2.73, 95% CI = 1.15–6.48; P < .05), and the presence of upper gastrointestinal bleeding (UGIB; OR = 15.64, 95% CI = 1.29–189.75; P < .05) were the independent risk factors for upgraded pathology. In addition, patients >65 years old (OR = 0.022, 95% CI = 0.901–6.549; P < .05) or with a lesion size of ≥2 cm (OR = 4.237, 95% CI = 1.650–10.878; P < .01) were more likely to endure the noncurative resection.
Conclusion:
For suspected gastric HGIN patients, age, lesion size, the number of biopsies, and UGIB should be taken into account before deciding on the ESD.
Introduction
Gastric cancer is the second leading cause of cancer death, which thereby constitutes a major health problem.1–3 Advanced gastric carcinoma (AGC) has an even higher mortality rate. 4 Fortunately, the early detection of precancerous lesions and its subsequent removal can play an important role in the prevention and management of gastric carcinoma. 5 If left untreated, gastric carcinoma generally progresses through a defined inflammation–metaplasia–dysplasia–carcinoma sequence. 6 High-grade intraepithelial neoplasia (HGIN) exhibits a high risk of progression to carcinoma, and thereby requires timely resection.7,8 For such resection, both surgical and endoscopic modalities have been accepted as appropriate treatments for gastric HGIN.9,10 Endoscopic submucosal dissection (ESD) has perceptions of being safe, efficient, and not prone to complications, and this approach has presently become the mainstay of HGIN treatment.11,12 However, following an initial diagnosis that uses endoscopic forceps biopsy (EFB) upon subsequent mucosectomy, it appears that for patients who underwent early gastric cancer (EGC), especially when the margin of the resected tumor specimen is positive, the consequences for subsequent clinical management are substantial.13–15 Therefore, it is important to identify patients with an initial diagnosis of HGIN, who are most at risk of receiving a final diagnosis of EGC.
Unfortunately, these risk factors remain largely obscure at best, despite the efforts of various groups in identifying possible risk factors for the under-diagnosis of EGC in EFB material.16–18 This consideration has prompted the investigators to initiate a comprehensive study on factors that may be useful for predicting the risk for under-diagnosis in patients with apparent HGIN.
Materials and Methods
Patients
A total of 123,460 patients, who underwent conventional upper gastrointestinal endoscopy at the First Affiliated Hospital of Nanjing Medical University from January 2010 to December 2015, were included in this study. Among these patients, 1212 patients were initially diagnosed with HGIN. In the further analysis, patients who had any of the following characteristics were excluded: (1) history of cancer or stomach surgery; (2) prior surgical treatment; (3) signs of deep infiltration or AGC emerging from the endoscopic ultrasonography (EUS), computed tomography (CT), or magnetic resonance imaging (MRI) investigations; (4) the absence of adequate clinicopathological data (Fig. 1). Among these patients, 1212 patients were initially diagnosed with HGIN. Furthermore, 995 patients underwent EUS, 1124 patients underwent CT, and 19 patients underwent MRI. A total of 526 patients with deep infiltration or AGC emerging from the EUS, CT, or MRI were excluded. Subsequently, patients who were successively subjected to ESD were selected, resulting in the identification of 134 patients suitable for analysis.
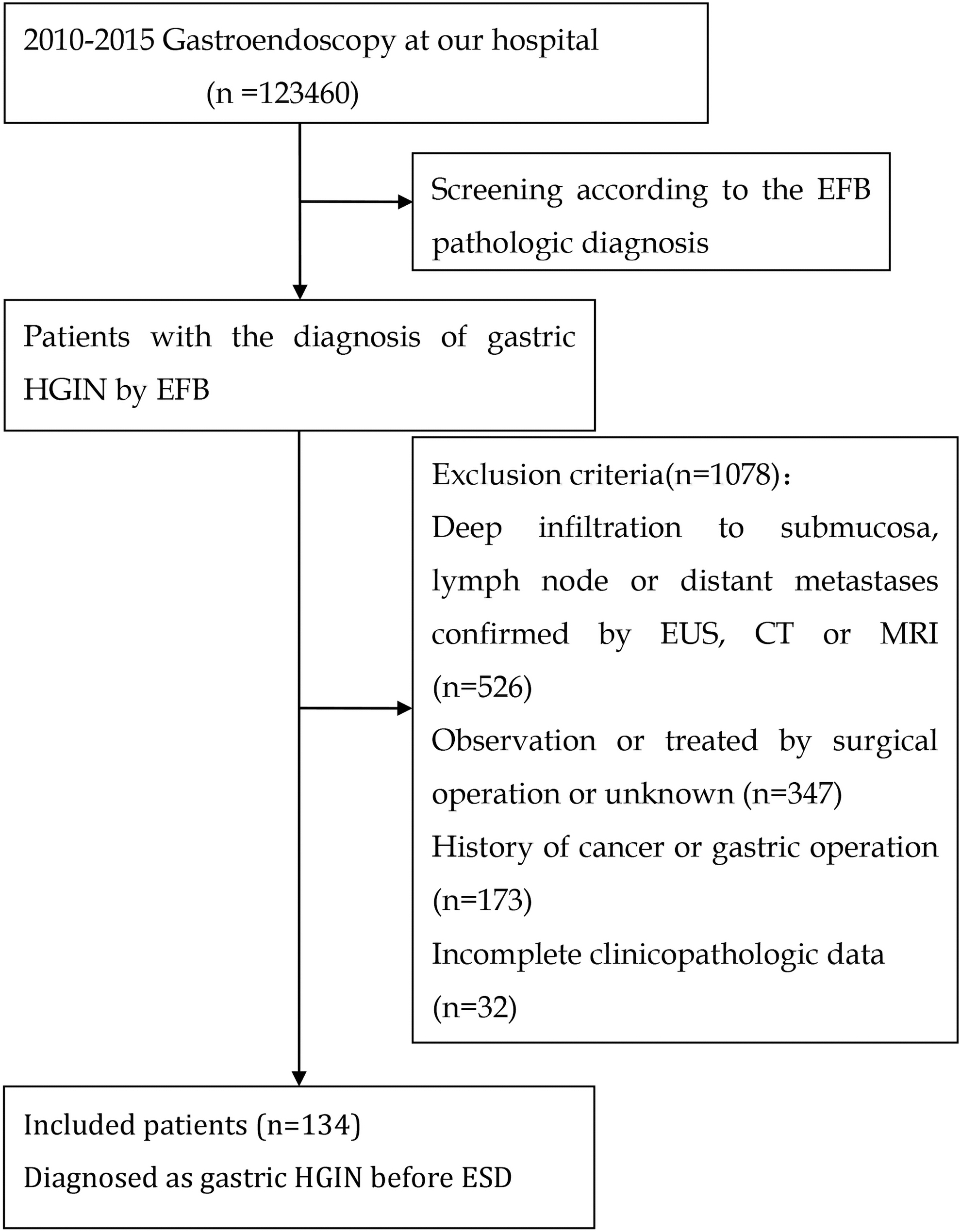
Schematic description of the screening methodology. CT, computed tomography; EFB, endoscopic forceps biopsy; ESD, endoscopic submucosal dissection; EUS, endoscopic ultrasonography; HGIN, high-grade intraepithelial neoplasia; MRI, magnetic resonance imaging.
The data on clinical manifestation, the endoscopic appearance of the lesion (e.g., lesion location, size, erythema, or the presence of apparent erosion), and the procedural characteristics (e.g., the number of biopsies), as well as the histopathological information that emerged from the pathological analysis following ESD, were analyzed (e.g., depth of infiltration, macroscopic pattern, and surgical margin) and collected. Then, the pathological diagnosis before and after ESD were compared, and the risk factors for discrepancies were analyzed. In addition, factors that predispose to noncurative resection (i.e., margin positivity) were analyzed. An informed consent was routinely obtained from patients before the endoscopic procedure. Due to the retrospective nature of the study, informed consent was waived. The privacy of all the participants was maintained with confidentiality. The study was approved by the Medical Ethics Committee of the First Affiliated Hospital of Nanjing Medical University (approval no. 2018-SR-234).
Histopathological evaluation
According to Japanese guidelines, ESD is appropriate for gastric HGIN. 19 The pathologists routinely assessed the lateral and/or vertical margins, depth of invasion, and presence of lymphovascular invasion in the lesion. The diagnosis was made based on the Vienna classification system for gastric intraepithelial neoplasia (GIN) and carcinoma. 9 All patients successfully received endoscopic en bloc resection, which resulted in the removal of the intact lesion. A classification of complete resection (R0 resection) was made for en bloc resection specimens that were negative for apparent cancer cells in both the horizontal and vertical margins. Upon detection of carcinoma cells and/or atypical hyperplastic cells at the lateral margins, a positive resection margin was called. 19 For this analysis, a resection was deemed curative when all the following conditions were met: an en bloc resection was performed, the tumor size was ≤2 cm, the tumor had a differentiated histology, the classification was pT1a, the horizontal margin was negative, the vertical margin was negative, and no signs of lymphovascular infiltration.20,21
Postoperative treatment and subsequent follow-ups
The postoperative clinical management for all patients included adequate continuous proton-pump inhibitor therapy for ∼4 to 8 weeks, together with the prescription of a gastric mucosal protectant. 22 Prophylactic antibiotics were administered to patients who had large surgical wounds, underwent an unduly long operation time, or were otherwise deemed to be at risk for infection. The follow-up for this study was maintained up to November 2016. Further assessments were performed on the obtained curative effect, the presence of potential complications, the nature of further management, and other data, such as recurrence and survival. The median follow-up period was 35.5 months, and the mean was 35.2 months.
Statistical analysis
All continuous variables were presented as mean ± standard deviation. The baseline characteristics were compared using χ 2 -test. The risk factors that correlated with the upgraded pathology and noncurative resections after the ESD were analyzed using logistic regression analysis. P < .05 was considered statistically significant. The statistical analysis was carried out using SPSS version 20.0.
Results
Clinical and endoscopic characteristics of patients before ESD
A total of 134 patients with an initial pathological diagnosis of HGIN and subsequent treatment of ESD were included for analysis in this study. As given in Table 1, the M/F ratio of the cohort was 3.62 (105:29), and the mean age of the cohort was 62.60 ± 9.59 years old (range: 34–82 years old). With respect to the macroscopic aspect of the lesions, 48.50% were classified as elevated type lesions, 26.86% were classified as depressed type lesions, and the remaining 24.63% were classified as flat type lesions. The mean diameter of these lesions was 2.16 ± 1.38 cm, and the mean number of biopsies obtained from these lesions was 4 (3, 6). Within the total group of apparent HGIN lesions, 55.98% of cases had erosions and 50.75% of cases had erythema. Within the entire group, 4.478% of patients presented with a family history of gastric cancer and 88.81% of patients presented with clinical symptoms, such as abdominal distension (47.01%), dull pain (43.28%), upper gastrointestinal bleeding (UGIB, 2.99%), or weight loss (11.19%). It was concluded that the present cohort was representative, which would allow for the analysis of risk factors for potential EGC.
Clinical and Endoscopic Characteristics of Patients Before Endoscopic Submucosal Dissection (n, %)
Upper portion of the stomach: Cardia and fundus of the stomach; Middle portion of the stomach: Gastric body; Lower portion of the stomach: Gastric antrum.
IQR, interquartile range; SD, standard deviation; UGIB, upper gastrointestinal bleeding.
Incidence of EGC following an initial diagnosis of HGIN and resection performance following ESD
In the present patient group, the mean interval time between the initial diagnosis and endoscopic treatment was 1.34 ± 2.49 months. As given in Table 2, although most of these cases were proven to be pathologically identical between the EFB-based diagnosis and subsequent ESD, there were still 35 cases (26.12%) with submucosal infiltration, and this was consistent with EGC. Among the 35 patients who received an upgraded diagnosis of EGC, a total of 15 patients finally underwent noncurative resection after ESD. All 134 patients underwent en bloc resection, and the resulting mean maximum specimen diameter was 3.53 ± 1.38 cm. Among these ESD procedures, 106 patients (79.10%) achieved a successful resection, that is, the lateral margin was judged as tumor or dysplasia free. However, a total of 28 patients apparently had noncurative resections (20 patients had positive lateral resection margin residues, 5 patients had positive vertical resection margin residues, and the remaining 3 patients had both positive lateral and vertical resection margin residues). Furthermore, none of the cases had undifferentiated adenocarcinoma, lymphatic invasion, or vessel invasion. Hence, it could be concluded that EGC following an initial diagnosis of HGIN is relatively common, and that it is thereby important to identify the risk factors for this condition, especially in view of the non-negligible rates of noncurative resections.
Margins and Pathological Diagnoses of the Final Resection Specimens
EGC, early gastric cancer; HCIN, high-grade intraepithelial neoplasia.
Risk factors for EGC after ESD for HGIN
There were no statistically significant differences in terms of lesion characteristics, such as erosion, ulceration, erythema, lesion location, and macroscopic pattern, between the concordant and EGC groups (Table 3). However, compared with the concordant group, a lesion size of ≥2 cm (odds ratio [OR] = 5.162, 95% confidence interval [CI] = 2.042–13.048, P < .01), a number of biopsies of ≤4 (OR = 2.731, 95% CI = 1.150–6.484, P < .05), and signs of UGIB (OR = 15.636, 95% CI = 1.289–189.749, P < .05) were all independent risk factors for the subsequent upgraded pathology staging (Table 4). Thus, these factors should be taken into account when deciding on the use of ESD for suspected HGIN.
Risk Factors for Upgraded Pathological Diagnosis After Endoscopic Submucosal Dissection
Upper: Cardia and fundus of the stomach; Middle: Gastric body; Lower: Gastric antrum.
P < .05; **P < .01.
GC, gastric cancer; UGIB, upper gastrointestinal bleeding.
Multivariate Analysis of Risk Factors Associated with the Upgraded Pathology
P < .05; **P < .01.
CI, confidence interval; OR, odds ratio; UGIB, upper gastrointestinal bleeding.
Risk factors for noncurative ESD
The present data allow for the identification of factors associated with noncomplete ESD-mediated lesion removal. There were no statistically significant differences in lesion characteristics, such as erosion, ulceration, erythema, lesion location, and macroscopic pattern, between the noncurative and curative groups. Furthermore, it was observed that age, lesion size, the depth of invasion, and pathological diagnosis after ESD were significantly different between patients who underwent curative or noncurative resection (P < .05; Table 5). The further multivariate regression analysis confirmed that age >65 years old (OR = 0.022, 95% CI = 0.901–6.549; P < .05) and a lesion size of ≥2 cm (OR = 4.237, 95% CI = 1.650–10.878; P < .01) were indeed independent risk factors for noncurative resection (Table 6). However, the present analysis did not allow this assessment to have a predictive effect for gender, because the M/F ratio of the enrolled cases was too large (3.62).
Risk Factors for Noncurative Resection
Upper: Cardia and fundus of the stomach; Middle: Gastric body; Lower: Gastric antrum; *P < .05; **P < .01.
GC, gastric cancer; UGIB, upper gastrointestinal bleeding.
Multivariate Analysis of Risk Factors Associated with Noncurative Resection
P < .05, **P < .01.
CI, confidence interval; OR, odds ratio.
Analysis of complications and long-term follow-ups following ESD with the intent of treating HGIN
A total of 6 patients were lost to follow-up with respect to the final outcome, although their 6-month postprocedural medical information was retrieved. Delayed bleeding occurred in 2 patients at days 3 and 8, respectively, following the ESD procedure. Both patients were successfully managed by conservative treatment and endoscopic hemostasis. One patient (0.75%) had postoperative respiratory failure, and recovered following ventilator support in the intensive care unit. There were no cases of perforation or serious infection following ESD. For the 28 patients who underwent apparently noncurative ESD, 18 patients underwent additional surgery within 3 months without further need of radiotherapy or chemotherapy, and all these patients did not suffer from recurrence during the follow-ups. The remaining 10 patients who rejected further surgery were treated using adjuvant therapy, and were subjected to intense clinical monitoring. A total of 4 patients developed EGC at 10, 18, 19, and 32 months, respectively, following apparently noncurative ESD. In the curative group, there was no recurrence during the follow-ups. However, 1 patient died of noncancerous disease within 10 months post-ESD.
Discussion
GIN is a precursor of gastric carcinoma, which is described as a complex of structural and cytological abnormalities in the gastric mucosal epithelium associated with subsequent transformation. The term GIN was proposed by the World Health Organization (WHO) to resolve the differences between Western and Japanese pathologists with respect to the diagnostic classification of epithelial neoplastic lesions.9,10 Hence, this was further subdivided into two different types, namely, low-grade intraepithelial neoplasia and HGIN. Gastric HGIN, severe dysplasia, intramucosal carcinoma, carcinoma in situ, and the suspicion of invasive carcinoma were all classified in the fourth category (noninvasive high-grade neoplasia), according to the WHO classification. 23 The diagnosis depends on the pathological examination of the biopsy material, and is supported by medical imaging results for further guidance in clinical decision making.
The evidence obtained hitherto strongly suggests that patients with HGIN are at high risk of progression to carcinoma or synchronous carcinoma. 7 Thus, this condition calls for timely treatment. Endoscopic treatment and surgical resection are the preferred treatment modalities for HGIN, 15 in which the former has been perceived as more safe and patient friendly, whereas the latter has been perceived to be obviously superior with respect to the radicality of lesion removal. A number of studies have suggested that there are no significant differences between ESD and surgical resection, in terms of efficiency, safety, 5-year survival rate, and recurrence. However, patients treated by ESD had better outcomes, including shorter operation time, lower incidence of complications, shorter hospital stay, and better quality of life compared with patients treated by radical surgery. 11 However, notably, the discordant diagnosis of EGC following ESD may require a speedy additional surgical resection, which is associated with substantial patient discomfort, additional patient risk, and increased economic burden for the patient. Thus, there is a strong incentive to avoid unnecessary ESD. In this study, the investigators aimed to identify factors that may provide guidance to the practitioner in this aspect.
The present diagnosis of HGIN of the stomach continues to heavily rely on histopathological results, which are usually derived from the examination of biopsy specimens. Although new endoscopic techniques that directly assess the histopathological type of mucosal lesions are emerging, this still remains an experimental and unproven technology.24,25 Hence, EFB analysis remains the gold standard for the diagnosis of GIN. In addition, it was also observed in this study that differences between the initial pathological diagnosis on the EFB material and final postoperative diagnosis on the resection material constitutes an important concern.13,26 Zhu et al. 27 revealed that among the 227 patients with an initial diagnosis of intraepithelial neoplasia, 57 (25.1%) patients had an upgraded pathology at postresection. Furthermore, among the 91 patients initially diagnosed with HGIN, 25.27% (23/91) of these patients were eventually diagnosed with gastric cancer, which is broadly in keeping with the results of this study. Although other studies reported discrepancies in 41.3% of EFB and ER specimens, this study revealed that 26.12% (35/134) of patients had an upgraded pathological diagnosis, postoperatively, and the investigators consider that the results of this study are in keeping with those reported in literature. Hence, the investigators considered that the present data can be used for guidance to the community of practitioners who have patients with apparent gastric HGIN.
In this context, it was particularly relevant in these present findings that a large lesions size, a small number of biopsies, and apparent UGIB all emerged as factors independently associated with the later diagnosis of EGC. Especially when observed in conjunction, this can serve as an indication that potential under-diagnosis may have occurred. Hence, this should be taken into account when deciding on clinical management. This fits well with earlier studies, which revealed that there is greater likelihood for EGC after an initial diagnosis of HGIN in patients with depressed lesions and lesions ≥2 cm. 18 Similarly, Min et al. 17 reported that age (≤60 years old), female gender, gastric body, a flat or depressed lesion type, and tumor size >2 cm were independent predictive factors for the subsequent diagnosis of EGC, which is discordant with the earlier EFB-based diagnosis. In addition, it has been described that diagnostic accuracy decreased in patients with <4 biopsies. 16 Thus, the present findings fit well with the contemporary body of biomedical literature, but argues for the copious EFB sampling in patients with suspected HGIN, especially when the lesion is large and signs of UGIB are present.
In this study, the overall performance of en bloc resection and achieving a margin-free resection was 100.0% and 79.0% (106/134), respectively. This is in line with other studies that reported parameters of 86.8%–99.0% and 79.9%–97.1%, respectively.28–30 In this sense, these present findings can be extrapolated to clinical practice outside that of our own institution. Nevertheless, a curative resection rate of 79.0% appears to require further improvement. The present analysis demonstrates that there are two independent risk factors with respect to noncurative resection: age (>65 years old) and lesion size (≥2 cm). This is partly consistent with the findings reported by Fu et al., 31 in which potential risk factors associated with a positive lateral margin were assessed, and the identified location (the upper third of the stomach being at risk, which is a factor that did not emerge from this study), size (>3 cm, in broad agreement with this study), and histological tumor classification (which was not assessed) were risk factors in this aspect. For the curative resection rate, there was no significant difference between patients with poor lesion lifting and good lesion lifting. Unfortunately, the highly skewed gender ratio in this study did not allow for the assessment of the effect of gender on resection success, and this thereby awaits further investigation.
The main complications associated with ESD for HGIN are pain, bleeding and perforation. Delayed bleeding is a common complication that occurs in up to 6.9% of patients who underwent standard ESD. 32 In the present study, delayed bleeding was only recorded in 2 (1.49%) patients, and both patients were successfully managed by conservative treatment and endoscopic hemostasis. During the follow-up, 4 patients (2.98%) from the study group progressed to EGC after ESD, which is in general agreement with those observed elsewhere (0.9%–5.1%).33,34 Hence, it is fair to say that the present study supports the broadly accepted idea that ESD is safe and effective for the treatment of gastric HGIN.
Important innovations are ongoing in endoscopy, especially chromoendoscopy, confocal laser endomicroscopy, fluorescence endoscopy, Fuji intelligent chromoendoscopy (FICE), magnifying endoscopy (ME), and narrow band imaging (NBI), which are all promising new avenues. FICE can provide clear images of vessels, which improves the diagnosis of EGC and the accuracy of biopsy sampling. 35 NBI technology allows more targeted biopsies to be obtained, and thereby improves the number of biopsies in which aberrancies are detected, and concomitantly improves the overall sensitivity and specificity for the diagnosis of EGC. As an example, Horiuchi et al. reported that the diagnostic accuracy of the ME-NBI technique is 36.5% higher than that of the white-light imaging technique alone. 36 Kiyotoki et al. compared ME-NBI and indigo carmine chromoendoscopy (ICC) in terms of the success of evaluating tumor margins, and found that the accuracy rate of ME-NBI was significantly higher than that of ICC. 37 However, NBI is still very much in the process of being introduced into clinical practice (e.g., only 16 cases [11.94%] involved NBI due to limited resources), and this technique remains only partly proven in the preoperative setting of HGIN. Hence, it was considered that until the full potential of NBI becomes evident, these present findings will have relevance for guiding the decision-making of physicians in apparent gastric HGIN. A similar situation also holds true for chromoendoscopy and indigo carmine double staining.
Although these present findings are of relevance to this field, the limitations of this study should also be recognized. First, the present study is retrospective in nature, and was heavily reliant on the quality of information obtained from medical records, which may provoke reporting biases. For instance, lesion size was based on the EUS data owing to the absence of information on this aspect of the lesion in several pathological reports. Similarly, some patients without complete information were excluded, which conforms to the inclusion criteria, thereby having an influence on the comparison of results. Finally, as a single institution study, the number of participants was relatively limited. Nevertheless, these results were statistically robust. Hence, it was considered that these limitations do not negate the results obtained.
Conclusion
In conclusion, it was observed that ESD is not always the optimal choice for patients with suspected diagnosis of gastric HGIN. Furthermore, age, lesion size, the number of biopsies, and potential UGIB should be taken into account before performing ESD.
Availability of Data and Materials
All data generated or analyzed during the study were included in the article.
Footnotes
Authors' Contributions
H.-H.Z. and J.-X.J. designed the research; H.-H.Z. performed the research and drafted the article; M.D.S., H.-M.S. and J.-L.C. collected the data; S.-F.X. and H.-H.Z. analyzed the data; J.-X.J. contributed in the analysis and supervised the report. All authors provided intellectual input to the study and approved the final version of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the 12th Six Talents Peak Project of Jiangsu Province (No. 2015-WSN-028), the Research Project of Education Science in the 12th Five Year Plan of Nanjing Medical University (No. NY2222015030), the Research Project of Chinese Medical Association and Chinese High Education Association (No. 2016B-KC019), and the Priority Academic Program Development of Jiangsu Higher Education Institutions (PAPD) (JX10231801). The authors declare that they have no financial relationship with the organization that sponsored the research, and the funding body was not involved in the study design, data collection, analysis, and writing of the study.