
Abstract
Aim:
This study was performed to investigate the feasibility of surgical treatment of port-site metastasis after laparoscopic radical resection of gastrointestinal tumors.
Patients and Methods:
We retrospectively analyzed the clinical data and follow-up data of 8 patients with port-site metastases after gastrointestinal cancer resection in our hospital from January 2014 to January 2018.
Results:
Six of port-site metastases occurred within 6 months after gastrointestinal tumor resection, one of port-site metastases occurred in 10 months after the operation, and one of port-site metastases occurred in 30 months after the operation. Any metastasis to the abdominal cavity or distant metastasis was ruled out before the surgical treatment of the port-site metastases, and all patients recovered well after the extended operation. No incisional infection or incisional hernia occurred. By December 2019, 4 patients had died (they had survived for 12, 13, 18, and 24 months, respectively) and 5 patients had survived. The follow-up duration ranged from 19 to 28 months.
Conclusions:
Surgical resection of port-site metastases is not difficult because of their superficial location. Surgical treatment can improve the prognosis of patients without abdominal metastasis or distant metastasis/recurrence.
Since Stockdale and Pocock 1 first described port-site metastases after laparoscopic surgery in 1985, an increasing number of authors have reported this condition following laparoscopic surgery. However, the incidence of port-site metastases after laparoscopic surgery is very low, and there is a lack of relevant treatment experience. In this study, we retrospectively analyzed the data of 8 patients with port-site metastases after gastrointestinal cancer resection in our hospital from January 2014 to January 2018 and summarized the relevant experience and skills required for treatment of such patients.
Patients and Methods
General data
Eight patients with port-site metastases after gastrointestinal cancer resection in our hospital from January 2014 to January 2018 were enrolled in this study. The inclusion criteria were as follows: (1) the ability to surgically resect the local lesion with no distant metastasis before surgery, (2) pathologically confirmed metastatic or invasive adenocarcinoma after surgery, (3) no coexisting severe cardiopulmonary disease, and (4) no perioperative death. The patients comprised 4 men and 4 women ranging in age from 51 to 73 years (average age, 61.6 years). The gastrointestinal tumors were gastric cancer in 5 patients (in 3 of these patients, the primary tumor was resected at other hospitals), liver cancer in 1 patient, pancreatic cancer in 1 patient, and colonic cancer in 1 patient (Table 1). The study was approved by the Zhejiang Provincial People's Hospital Institutional Review Board.
Clinical Data of Patients with Port-Site Metastases After Laparoscopic Radical Resection of Gastrointestinal Tumors
TNM, tumor-node-metastasis.
Surgical procedure
Patients with tumors that were located in the subcutaneous tissue and did not invade the muscular or aponeurotic system were treated as follows. The skin and its subcutaneous tissue were resected or part of the musculoaponeurosis was excised with a 2 to 3 cm margin from the tumor edge. The abdominal wall defect that formed after tumor resection was type I and was repaired by direct suturing of the skin and subcutaneous tissue.
Patients with tumors that were located inside the abdominal wall or invaded the abdominal wall muscles, skin, subcutaneous tissue, musculoaponeurosis, or peritoneum were treated as follows. The tumor was resected with a 2 to 3 cm margin from the tumor edge. The abdominal wall defect that formed after tumor resection was type III and was repaired by the tissue separation technique and use of implantation materials. 2
Main measures
The main measures in this study were incisional healing, surgical site infection, incisional pain, incisional hernia formation, and tumor recurrence.
Follow-up methods
After discharge, the patients were followed up by telephone or outpatient visits to assess their general condition, tumor recurrence/metastasis, and survival. Follow-up began on the date of surgery for port-site metastasis, and the survival time was calculated from the date of surgery to the date of death or last follow-up (December 2019). The follow-up period lasted 12–36 months (mean, 20.9 months).
Results
Sites of port-site metastasis after resection of gastrointestinal tumors
In most cases, a five-port method was applied during treatment of the primary cancer. 3 Implanted metastasis can occur at any port site (Fig. 1). Port-site metastasis occurred in the umbilical port in 3 patients, right main operating port in 3 patients, right auxiliary port in 1 patient, and left port in 1 patient. According to tumor-node-metastasis (TNM) stage, the primary tumors in 8 patients were T3-4 in invasion depth, 4 patients were T3, and 4 patients were T4.
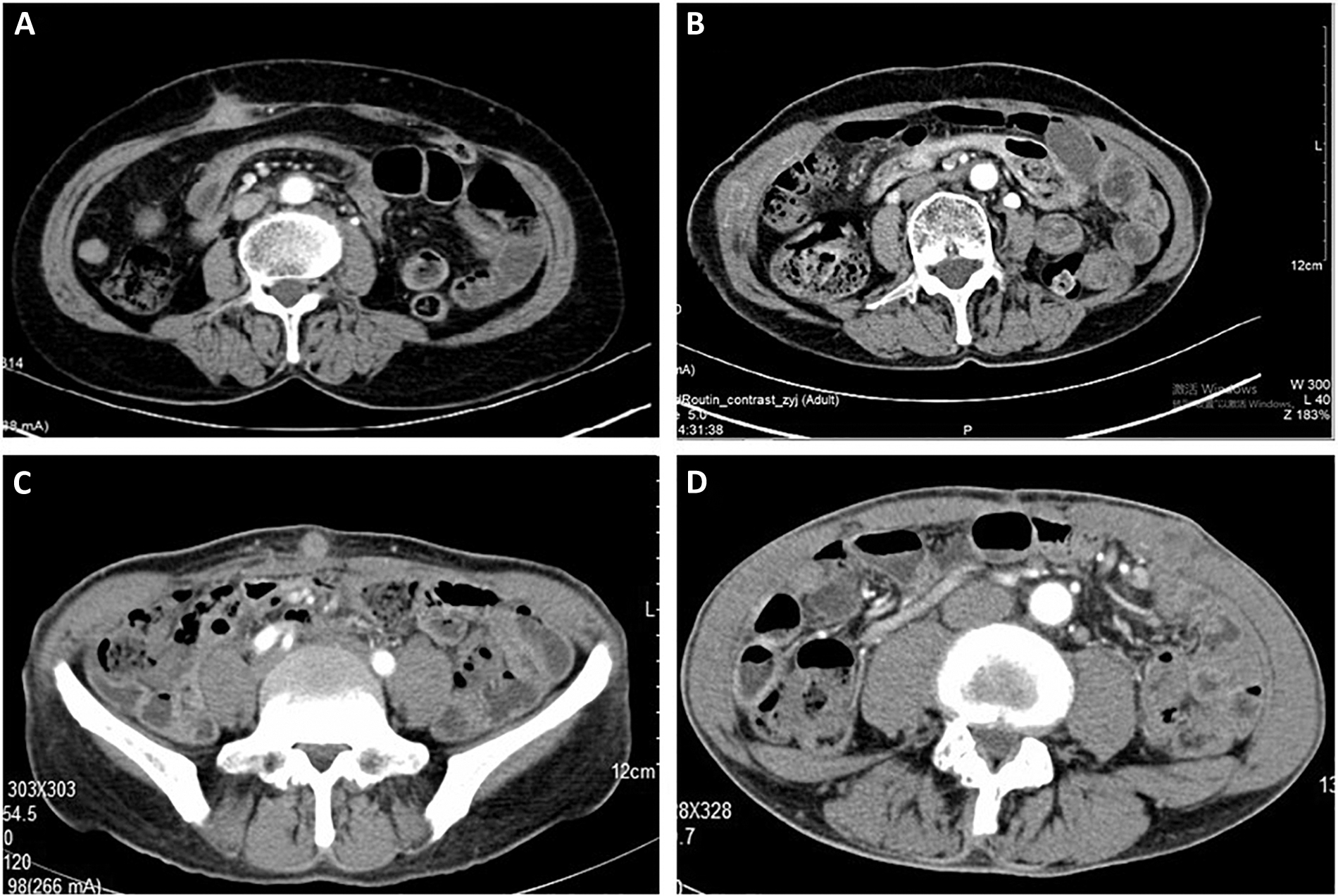
Sites of port-site metastasis.
Time to occurrence of port-site metastasis after resection of gastrointestinal tumors
Port-site metastases occurred 2–30 months after resection of the gastrointestinal tumors. More specifically, they occurred within 6 months after gastrointestinal tumor resection in 6 patients, 6–12 months after the operation in 1 patient, and 30 months after the operation in 1 patient.
Treatment of port-site metastases
Any metastasis to the abdominal cavity or distant metastasis was ruled out before surgical treatment of the implantation metastases, and all patients recovered well after the operation. No incisional infection or incisional hernia occurred. The tumors were located in the subcutaneous tissue (n = 3), muscular layer (n = 3), and umbilical port (n = 2). The abdominal wall defect that formed after tumor resection was type I (n = 3) and was repaired by direct suturing of the skin and subcutaneous tissue. Five patients developed a type III abdominal wall defect after tumor resection. Two patients underwent abdominal wall tumor resection plus abdominal wall defect repair (sublay or intraperitoneal onlay mesh/underlay), 2 patients underwent reconstruction of the abdominal wall defect by the tissue separation technique following abdominal wall tumor resection, and 1 patient underwent reconstruction of the abdominal wall defect by the tissue separation technique following abdominal wall tumor resection plus partial resection of the transverse colon because of invasion of the transverse colon and metastasis in the abdominal wall.
Prognosis of patients with port-site metastasis
All patients were followed up via telephone and/or outpatient visits after resection of the port-site metastasis. By December 2019, 4 patients had died (they had survived for 12, 13, 18, and 24 months, respectively) and 5 patients had survived. The follow-up duration ranged from 19 to 28 months.
Discussion
The incidence of port-site metastasis remarkably differs among different surgical treatment techniques for port-site metastases after laparoscopic resection of gastrointestinal tumors. In 1995, Wexner and Cohen 4 found that the incidence of port-site metastasis after early laparoscopic colorectal cancer surgery ranged from 1.5% to 21.0%. In 1996, Reilly et al. 5 studied 1711 patients with colon cancer and found that the incidence of port-site metastasis was 0.64%. According to three large-scale, multicenter, and randomized controlled studies (COST, COLOR, and UK MRC CLASICC) performed in 2007, 2009, and 2010, respectively, the incidence of port-site metastasis was 0.9% (2/435), 1.3% (7/534), and 2.4% (9/526); it was 3%, 6%, and 14% in patients with T4 stage cancer.6–8 In 2007, Lee et al. 9 reported the first case of port-site metastasis following laparoscopic-assisted gastrectomy. In 2012, Emoto et al. 10 reported that the incidence of port-site metastasis in patients with gastric cancer who developed peritoneal metastasis and were undergoing peritoneal chemotherapy was 1.5% (2/131). According to Berger-Richardson et al. 11 the incidence of port-site metastasis after gallbladder cancer surgery from 2000 to 2014 was significantly lower than that from 1991 to 1999 (10.3% versus 18.6%, respectively). No reports have described the incidence of port-site metastasis following laparoscopic hepatectomy. The present study comprised 8 patients with port-site metastases after gastrointestinal cancer resection in our hospital from January 2014 to January 2018. Among them, 3 patients had undergone resection of the primary cancer at other hospitals. Due to the high rate of loss to follow-up after resection of gastrointestinal tumors, it is impossible to accurately calculate the incidence of port-site metastasis after resection of gastrointestinal tumors in our center.
Clinical studies have demonstrated that extended resection of abdominal wall tumors can remarkably improve the prognosis and that this procedure is an important option for the treatment of tumors with abdominal wall invasion and metastasis.12,13 For all patients with abdominal wall invasion and metastasis, the size of the abdominal wall tumor and its relationship with adjacent organs should be identified by radiological examinations before the operation. If necessary, functional imaging by positron emission tomography/computed tomography can also be performed to identify any metastasis at other sites. Among our 8 patients with port-site metastasis, 7 had tumors confined to the abdominal wall and no recurrence in other sites. In the remaining 1 patient, the port-site metastasis also invaded the transverse colon but had no recurrence in other sites; after resection of the metastatic tumor, the patient's survival time exceeded 24 months. Few reports have described the treatment of port-site metastasis after laparoscopic surgery. Kim et al. 14 reported a case of port-site metastasis after laparoscopic gastrectomy for gastric cancer; the patient developed no recurrence after the resection during a 50-month follow-up. Kihara et al. 15 reported a case of port-site metastasis after laparoscopic liver resection for liver cancer; likewise, the patient developed no recurrence after the resection during an 8-month follow-up.
Abdominal wall tumors are superficially located. Surgical removal of these tumors is not difficult. In principle, a 2 to 3 cm rim of normal liver tissue around the tumor is required. After resection, an abdominal wall defect is formed and needs to be repaired and reconstructed. In a type I abdominal wall defect, only skin and parts of the subcutaneous tissue are lost; normally, direct suturing of the skin and subcutaneous tissue can repair such defects. A free skin graft may be considered when direct suturing of a large skin defect is difficult. A type II abdominal wall defect is mainly a defect of the myofascial tissue in the abdominal wall, but the integrity of the skin is preserved. In most cases, autologous tissue (obtained using tissue separation technology) or implanted materials are needed to complete the repair and reconstruction of type II abdominal wall defects. Type III abdominal wall defects are full-thickness defects. In addition to tissue separation technology and repair with implanted materials, flap technology is useful for the repair and reconstruction of type III abdominal wall defects. 16 According to the guidelines regarding the diagnosis and treatment of abdominal incisional hernias (2018 edition), 3 patients in our series had a type I abdominal wall defect after tumor resection, and these defects were repaired using a continuous simple suture. A type III abdominal wall defect formed after tumor resection in 5 patients, 3 of whom underwent abdominal wall tumor resection plus abdominal wall defect repair and 2 of whom underwent reconstruction of the abdominal wall defect by the tissue separation technique following abdominal wall tumor resection.
Direct implantation, contamination of surgical instruments, aerosolization of tumor cells, chimney effect, surgical technique, excessive manipulation of tumor, pneumoperitoneum, hematogenous spread, and local and systemic effects of carbon dioxide with pneumoperitoneum could cause of port-site metastasis.17,18 Tumor invasion into the serous layer can cause tumor cells to fall off into the abdominal cavity. TNM stage, the primary tumors of 8 patients in this study, was T3-4 in invasion depth. During surgery, avoiding to touch the tumor can effectively avoid port-site metastasis.
As noted above, abdominal wall tumors are superficially located and not difficult to remove. Surgical treatment can improve the prognosis in patients without abdominal metastasis or distant metastasis/recurrence. After resection of abdominal wall metastases, the abdominal wall defect should be reconstructed according to the specific type of defect.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by Zhejiang Provincial Medical Science Research Foundation (2020KY038).