
Abstract
Background:
Congenital megaprepuce (CMP) is a malformation consisting of redundant inner foreskin, normal penile shaft, and severe phimosis. The excess inner prepuce pushes the penile shaft deeper causing the appearance of a buried penis. We describe a novel surgical technique using dartos fascial flaps to reconstruct the prepuce giving excellent cosmetic and functional results.
Patients and Methods:
Penile reconstruction was performed by a single surgeon in 07 cases of CMP between January 2018 and December 2019. In all cases, the described surgical technique was used. Following surgery, cosmetic and functional outcomes were reviewed as well as the incidence of complications. The patients' ages ranged from 15 to 27 months (mean = 19). Mean hospital stay was 9 hours (range = 7–12). Operating time was between 50 and 85 minutes.
Results:
Postoperative appearance of the penis was satisfactory for all the parents in our group. Swelling of the penile shaft was seen in all of our patients but settled within one week of surgery. Scrotal hematoma was seen in only one of our patients, but that also did not need any intervention and settled spontaneously. During the follow-up period (mean = 14.5 months, range 6–24) no patient underwent revision surgery. In all our patients, the final appearance was of a circumcised penis. The final similarity to a normal circumcised penis was excellent in all of our patients. Correction of penoscrotal transposition was done in all patients achieving an elongated penile shaft and almost invisible postoperative scarring.
Conclusion:
Our modified surgical procedure to correct CMP is a safe and simple technique, providing good cosmetic results with the appearance of a standard circumcised penis. This also provides a good functional outcome with complication rate quite low. This technique is also easy to reproduce and teach compared with other complex procedures.
Introduction
Congenital megaprepuce (CMP) is a condition that consists of an excess of redundant inner foreskin with an associated severe phimosis but a normal penile shaft. This severe phimosis leads to a nonretractile prepuce. During micturition, the tight ring of the prepuce and excess inner foreskin leads to pooling of urine and results in often large volumes of basal urine remaining inside. This leads to the anatomical aspect of penoscrotal transposition and a classic dome-shaped base to the penis caused by the trapped urine (Fig. 1).

Classic “dome-shaped” base of the penis with “trapped” urine. Stenotic preputial ring with inner preputial ballooning due to urine pooling inside. Color images are available online.
It is due to this phenomenon of urine trapping that children with CMP often present with voiding difficulty and poor urinary stream. Urine dribbling invariably occurs as does dysuria, recurrent urine, and foreskin infections.1,2 Parents often describe having to compress the penis to evacuate the pooled urine from inside the excessive foreskin (Fig. 2). 2 O'Brien et al. 3 presented the first description of congenital phimosis in 1994. They showed and explained the mechanism of gross preputial ballooning and gave it an interesting name, “The Preputial Bladder,” which could only be emptied by manual compression. If the condition progresses to teenage and adult years, then painful erections can also be a symptom. 4 There is no evidence of spontaneous resolution of CMP so these children eventually all require surgical correction. 2

Parents often need to express trapped urine. Color images are available online.
The precise etiology of CMP is not known, however there are multiple theories in the literature. One of the common suggested cause of CMP is the presence of a congenital phimosis along with an associated defective attachment of the inner foreskin, a phenomenon also seen in children with a buried penis.2,5,6 Another theory was put forward by Devine et al., who suggested that there is an abnormal tissue link with the dartos fascial layer; whereas Donahue and Keating hypothesized that the outer foreskin layer is defective and it is due to paucity of outer preputial skin that there is a compensatory increase in the amount of inner preputial skin to cover the penile shaft.7,8
There are two challenges in the surgical management of CMP, first is to be able to achieve an optimum penile length and the second being to provide satisfactory skin cover to the penile shaft. 9 There is an evident shortage of penile shaft skin predominantly on the ventral side of the shaft, and to manage this, some surgeons advocate using the excess inner foreskin skin to provide cover for penile shaft.10–12 Other surgeons recommend using a combination of both outer penile shaft skin with inner foreskin to provide an adequate cover to the penile shaft.1,2,10,13
There are several accepted surgical techniques for the management of CMP. Donahoe and Keating 8 in 1986 presented a technique of preputial unfurling consisting of a Z-plasty procedure to surgically correct congenital phimosis, but there are numerous others such as the ventral V-plasty, Cuckow's technique, and the list goes on. However, there is as yet no consensus in the literature as to a gold standard surgical technique.10,11,14–16
Our article introduces a novel surgical technique for the correction of CMP which we believe gives superior cosmetic and functional outcomes with low rates of postoperative complications.
Patients and Methods
Penile reconstruction using the novel surgical technique (described below) was performed on seven cases of CMP between January 2018 and December 2019 at our hospital. The hospital ethics committee approved the study. Informed consent was taken from the parents of all the children involved in our study. The patients' ages ranged between 15 and 27 months (mean = 19 months). All patients presented with difficulty in voiding; with the main symptoms being ballooning (68%) and dribbling (25%). All patients were otherwise healthy aside from CMP, with no associated hypospadias or chordee. One case had a unilateral undescended testis and underwent inguinal orchidopexy at the same time as CMP correction.
All patients received intravenous gentamicin as prophylaxis at induction of anesthesia and treatment dose trimethoprim after surgery. This was continued until the urethral catheter was removed.
We included data of only those patients who had a minimum of 6 months follow-up after undergoing surgery. During the outpatient follow-up (mean length = 14.5 months), the following were evaluated: hospital stay, postoperative complications (e.g., secondary buried penis, voiding difficulties, retention of urine or urinary tract infections), redo surgery, voiding, and cosmesis. Cosmesis was assessed both by the surgeon, who classified the cosmetic outcome as either “poor,” “satisfactory,” or “excellent,” and the parents, who were asked of their own perception of the cosmetic appearance.
Surgical procedure
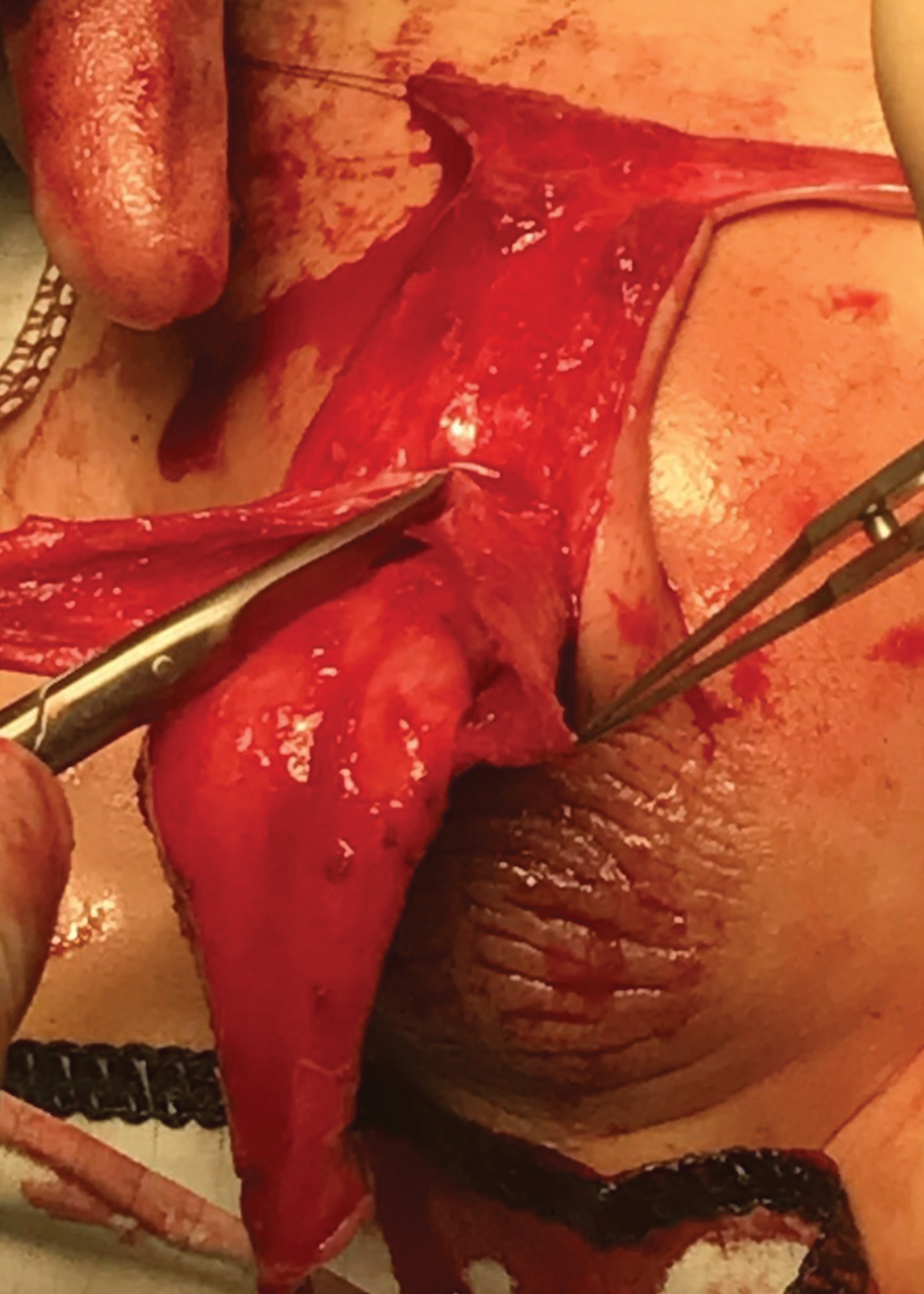
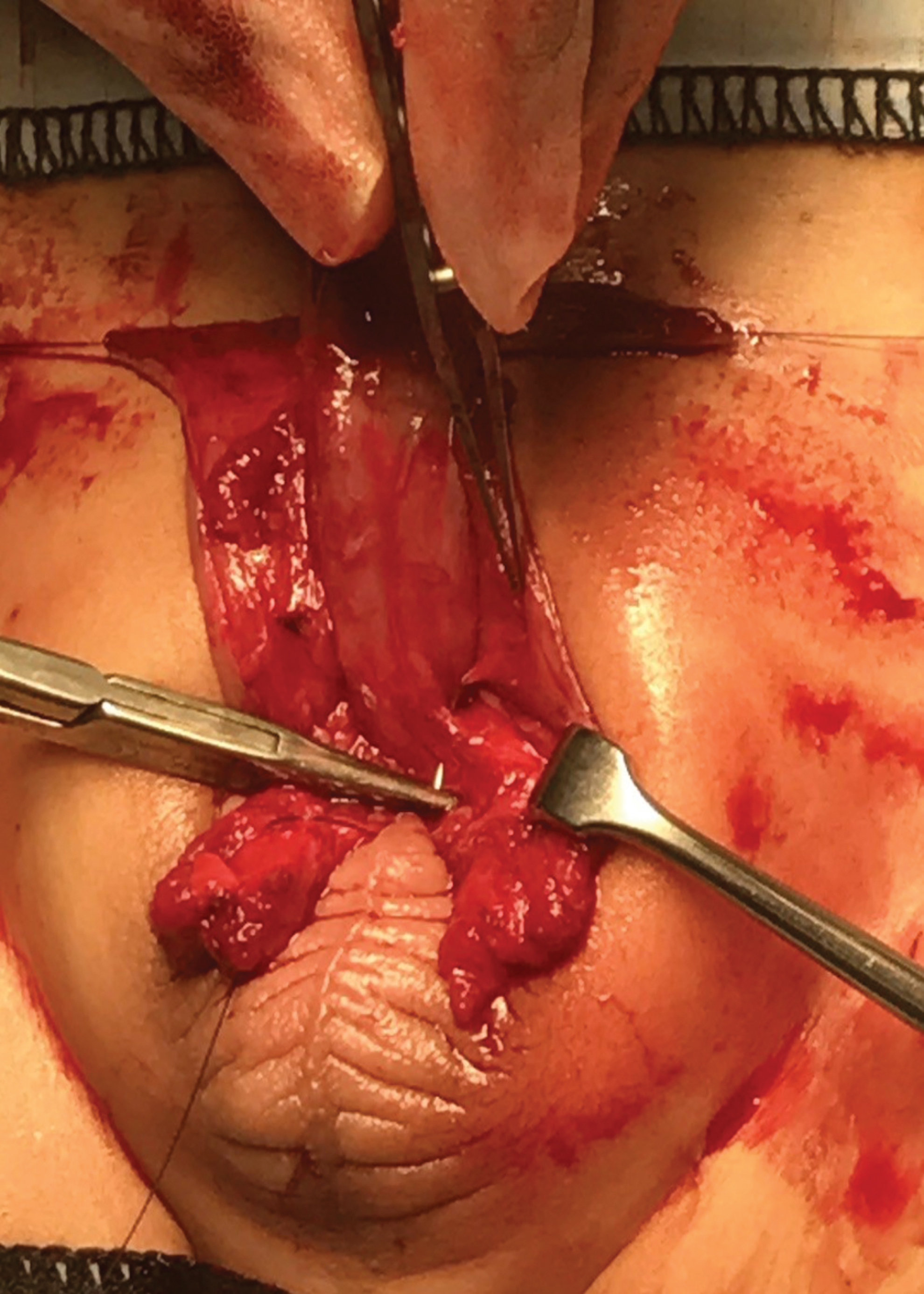
The initial surgical step is to apply traction stitches at the distal phimotic ring at 6 and 12 O’ clock positions (Fig. 3). This is followed by making the circumferential skin incision line at the border of outer and inner foreskin layers (Fig. 4). The incision is then deepened to reveal the plane between the outer and inner preputial skin (Fig. 5). An inverted Y-shaped incision is made on the ventral aspect of the penile base and scrotum to begin correction of the penoscrotal transposition (Figs. 6 and 7). This incision is crucial as it aids in providing much needed skin cover ventrally and helps mobilize the scrotum caudally. After this incision is made, careful degloving of the penis is done followed by release of all tethering fibrotic dartos tissue bands until the penis is freed to its base (Fig. 8).

Stay sutures at 6 and 12 O’ clock position. Color images are available online.

Incision at the junction of outer and inner foreskin all around. Color images are available online.
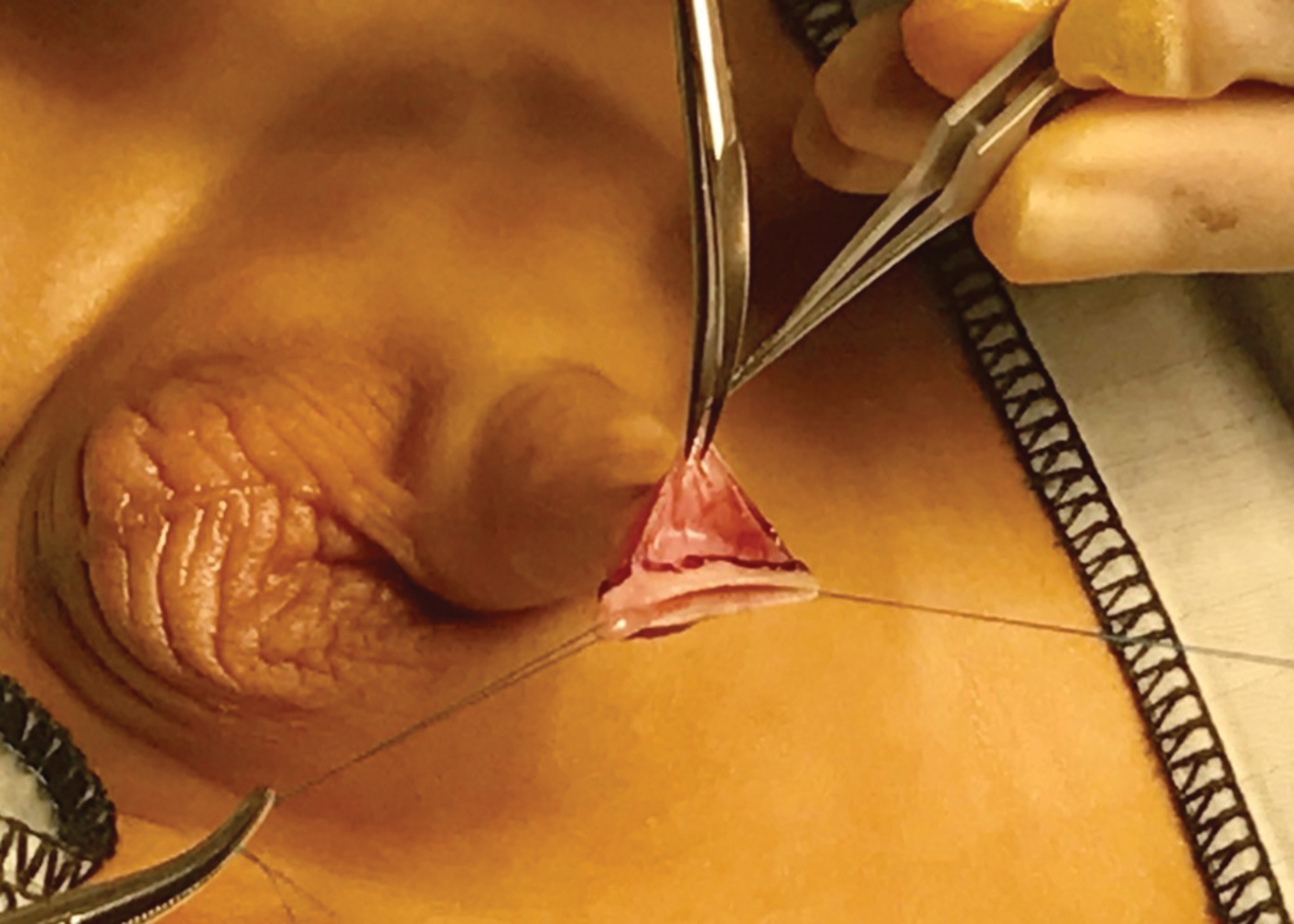
Plane between outer and inner foreskin is developed. Color images are available online.

Inverted Y incision for penoscrotal web on ventral penile shaft. Color images are available online.

Y incision helps provide penile shaft skin cover on much-needed ventral shaft side. Excision of excessive fibrotic Dartos tissue on the ventral side. Color images are available online.
Note the excess inner preputial skin. Color images are available online.
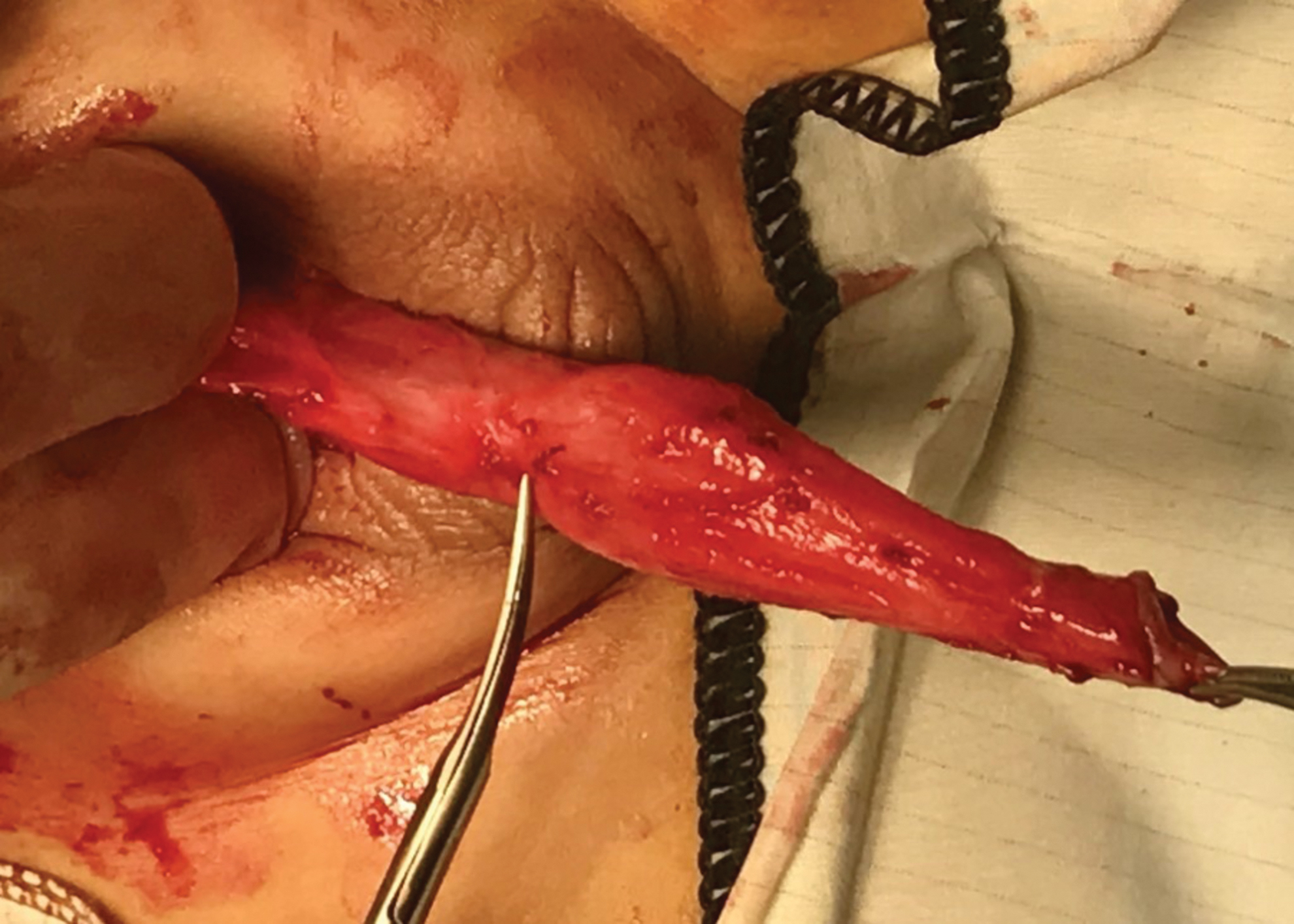
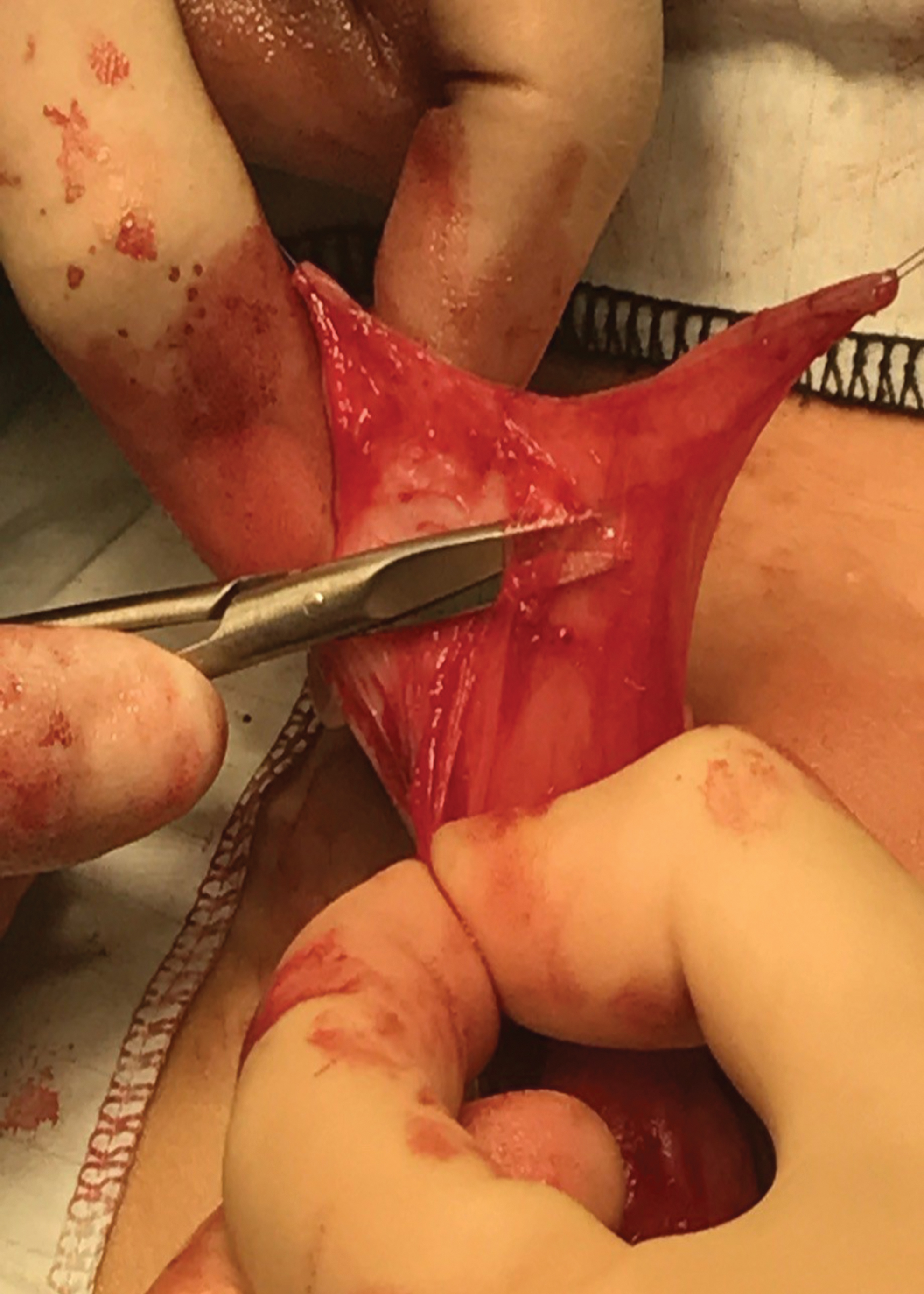
Dartos fascial flaps are then raised from the outer prepuce as classically described in hypospadias surgery (Fig. 9). This dartos flap is raised by starting from the distal edge of the outer foreskin and following the plane between the dermis and dartos down to the shaft base. This dorsal dartos flap is then split in the midline in two equal halves (Fig. 10) before being wrapped around the penile shaft to meet at the ventral aspect. At the base of the stretched penis, the ventrally brought dartos flaps are stitched together with Buck's fascia near the base of the corpora cavernosa on either side. The sutures are positioned between 2 and 5 O'clock on one side and between the 10 and 7 O'clock position on the other (Fig. 11). We used absorbable monofilament sutures. Once these sutures are in place, the excess distal dartos tissue is removed.
Dartos fascial flaps raised from outer foreskin. Color images are available online.
Dartos fascial flaps split in the midline in two equal halves. Color images are available online.
At the base of the stretched penis, the ventrally brought Dartos flaps are stitched with Buck's fascia near the base of the corpora cavernosa to reconstruct the penoscrotal angle. Color images are available online.
This anchoring of dartos fascial flaps to the base of stretched penis on either side not only corrects the penoscrotal web, but also helps reconstruct the penoscrotal angle. This step also improves the buried appearance of the penile shaft.
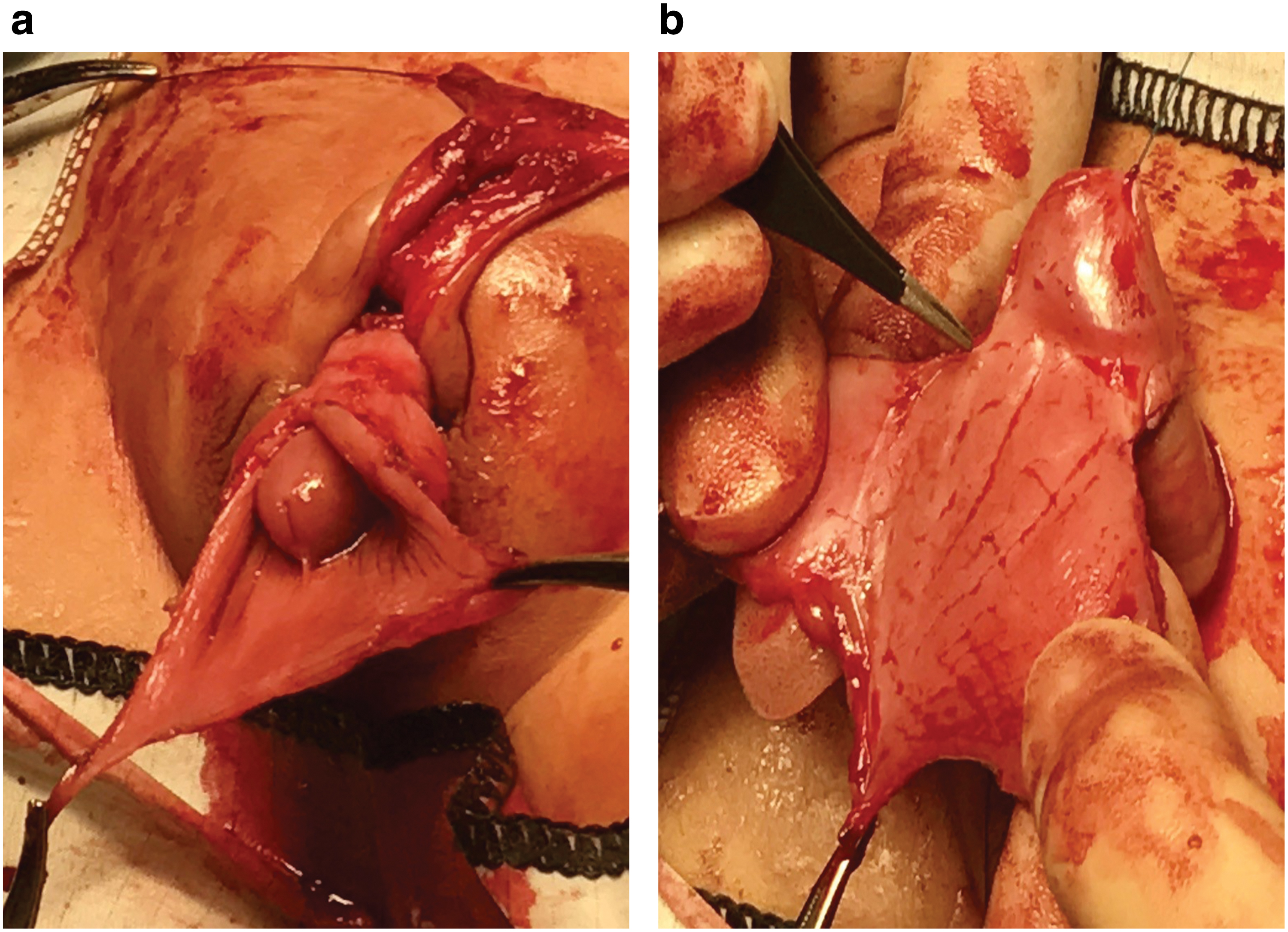
An incision is then made on the inner prepuce around 5 mm from the corona circumferentially. Dissection is deepened superficial to and along the Buck's fascia, it is important while performing this step to divide any aberrant attachment of the skin and dartos fascia to the deeper tissue layers. This dissection frees the penile shaft from abnormal tethering and further allows the scrotum to assume a more caudal position creating a more defined penoscrotal angle thus improving the penoscrotal transposition and elongating the appearance of the penile shaft. The redundant and excess inner prepuce is excised leaving a small mucosal cuff proximal to the glans of around 5–8 mm (Fig. 12a, b).
It is important at this stage to ensure that skin cover of the penile shaft is accomplished only by the use of outer penile shaft skin and effort is made to limit the use of inner preputial skin as it does not provide a cosmetically good appearance. We use interrupted, absorbable 6x0 monofilament sutures on the skin. The aim is to achieve a final appearance of a circumcised penis (Fig. 13).

Excellent creation of the penoscrotal and penopubic angle. Color images are available online.
Hemostasis is achieved by judicious use of bipolar diathermy throughout and use of a foam dressing (Allevyn Gentle ®dressings). A urethral catheter is inserted and left for 5–7 days. The catheter helps prevent possible urine retention after penile surgery, a common port-operative issue due to pain as well as edema after the extensive penile dissection (Fig. 14). The patients are sent home on oral antibiotics for as long as the catheter remains in, along with analgesia and anticholinergic medication to prevent bladder spasms.
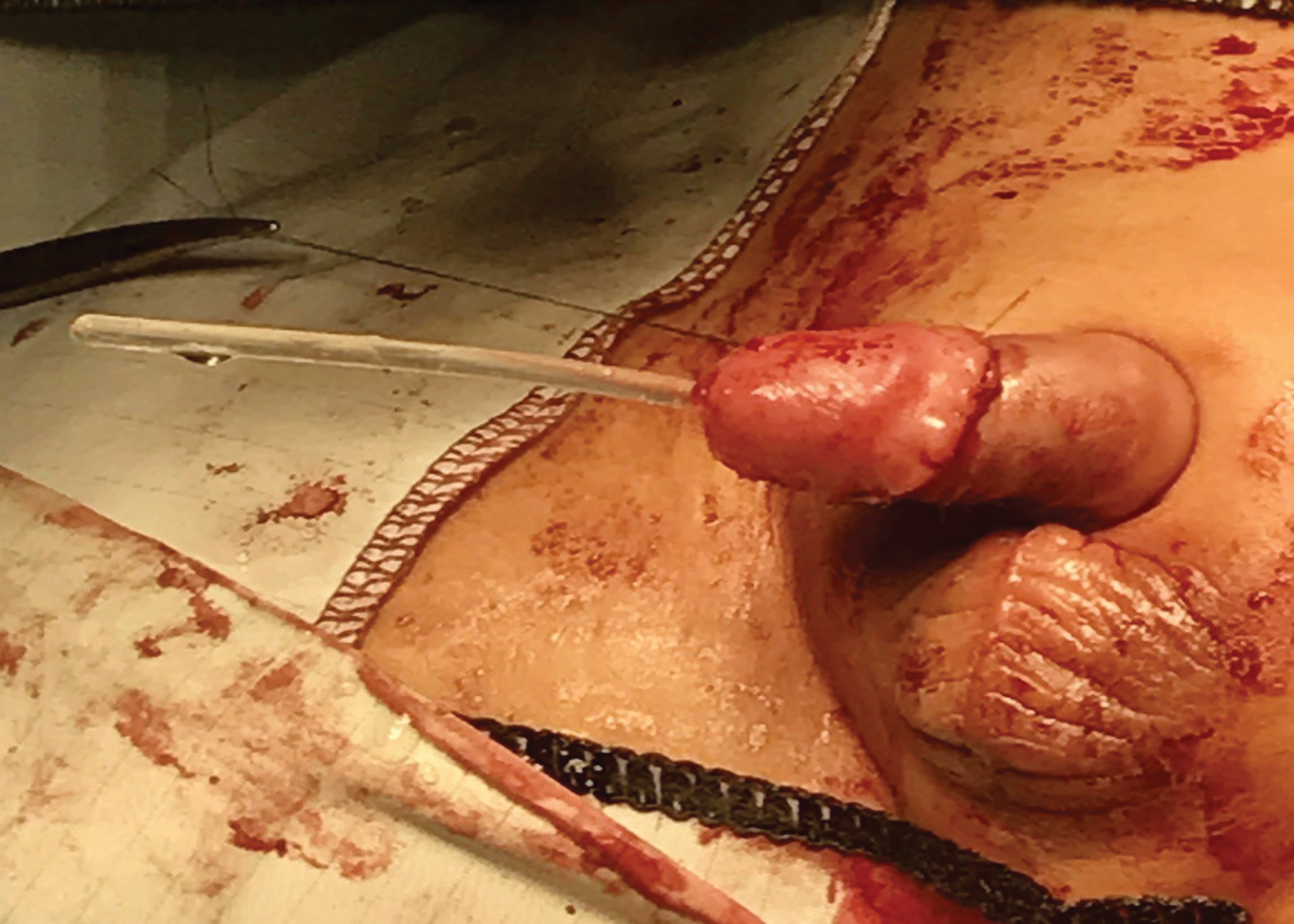
Urethral stent for few days. Color images are available online.
Results
The average operative time across our series was 65 minutes with a range of 50–85 minutes.
Mean length of inpatient hospital stay was 9 hours (7–12 hours).
With regard to cosmetic outcomes, correction of the penoscrotal transposition was achieved in all our patients. There was minimal scarring and we found that the avoidance of using inner prepuce skin for final skin cover, and preferential use of the comparatively normal-appearing outer preputial skin, gave a good-to-excellent final cosmetic appearance. After surgery, the parents of all patients were satisfied with the postoperative penile appearance. An appearance akin to a normal circumcised penis was satisfactorily achieved in all cases.
In terms of functional outcomes, all patients demonstrated a good urinary stream after the procedure without urinary retention or urinary infections.
Lastly, our technique was found to have a favorable postoperative complication rate. As to be expected, immediately after surgery, all patients developed slight edema of the penile shaft skin. In all cases, this disappeared spontaneously within one week of surgery. One patient suffered from a scrotal hematoma, which again, subsided without need for treatment or intervention. There were no significant postoperative complications, such as skin necrosis, wound infection, or wound dehiscence. There was no constriction band formation at the anastomosis site of outer and inner foreskin in any of the patient series. During a mean follow-up time of 14.5 months (range 6–24 months), no patient had to undergo revision surgery.
Discussion
The current literature contains numerous descriptions of differing surgical techniques to treat megaprepuce. However, in the authors' opinion most, if not all, of these techniques are quite technically complex, can be quite perplexing to learn, and are challenging to reproduce. Furthermore, of the various described surgical techniques for the correction of CMP, many achieve good functional outcomes but fail to achieve consistently optimal cosmetic results. A persistent buried appearance of the penile shaft postsurgery, due to a failure to adequately reconstruct the penoscrotal angle, is a commonly reported problem in the literature. At present, and as previously mentioned, there remains no single surgical technique offering a reliably acceptable cosmetic result.3,4,17
The most vital part of our modified surgical technique is the anchoring of dartos fascial flaps to the penile base at the level of Buck's fascia (Fig. 11). This step of the technique significantly helps in generating the cosmetically crucial penoscrotal junction and attaining a prominent and elongated penile shaft appearance (Figs. 13 and 14).
There is evidence in literature, like the technique advocated by Rod et al., for the fixing of the penile skin to the base in a manner similar to our anchoring of the dartos. 2 Rod et al. used a four-suture technique to restore the penoscrotal and penopubic angles. He suggested stitching the Buck's fascia and the dermis of the shaft skin at the penile base using two ventral sutures on either side of the corpus spongiosum and two sutures on the dorsal side of the corpora. The stitch they used was monofilament nonabsorbable 5/0 suture, However, in our series we only use two 4/0 PDS II (Polydioxanone—Ethicon) at the base of the stretched penis, stitching the ventrally brought dartos flaps with the Buck's fascia near the base of the corpora cavernosa that helps reconstructing the penoscrotal angle (Fig. 11).
There is also an ‘anatomical repair’ described in the literature, which involves stitching the base of the dorsal penile shaft skin to the Buck's fascia. 17 Ruiz et al. advocated fixing the external penile base to the Buck's fascia. 10 We think that this technique helps in mild-to-moderate cases of CMP, but with severe cases, the cosmetic appearance may not be that good and could lead to the persistent buried appearance of the penis especially in younger patients with increased suprapubic fat.
Although there is precedence in the literature advocating the use of dartos flaps for surgical repair in the correction of buried penis and penile torsion, its use has not yet been reported for use in the correction of CMP.18,19 We believe this report to be the first ever to advocate the use of dartos flaps for the correction of CMP. We feel through our study and the results described that we have justified the claim that our modified technique using dartos flaps attains a consistently excellent penile shaft length postoperatively and corrects the persistent buried appearance so often encountered with other techniques. This, along with other aspects of the technique, provided our patients with a superior cosmetic result without any sacrifice in functional outcomes or any increase in the rate of complications.
We would also further emphasize the crucial nature of the inverted Y-shaped incision made early in the technique. Not only is this incision vital as it aids in mobilizing the scrotum caudally and further helps in correcting the penoscrotal transposition, but it also helps in providing much-needed skin cover ventrally. Furthermore, this incision once made, assists the surgeon by revealing the boundary of the glans and the excessive inner prepuce.
We strongly believe that the inner excess foreskin should not be used wherever possible to provide shaft skin cover, particularly on the dorsal penile shaft, as this results in variances in skin color and texture leading to unacceptable cosmetic results. Besides being unsightly, the use of inner preputial skin has been associated with an increased risk of edema and swelling, along with a postoperative redundant skin collar. 20 To overcome these issues, various surgical modifications have been described, including inner prepuce tailoring or excision of the excess mucosal cuff. There is also published reports of excision of the subcutaneous tissue and quilting sutures, thereby thinning the inner prepuce.5,6,10,11
We recommend trying to limit the use of the inner prepuce to provide shaft skin cover by preferential use of the penile outer shaft skin. This can be achieved by division of the penoscrotal web. Our surgical technique includes dissection of the penile shaft skin to penile base, which helps to unfurl the inner prepuce layer, allowing the surgeon to then excise all the excess inner foreskin. This leaves the outer and normal-looking prepuce to provide nearly all the shaft skin cover rather than using the cosmetically unacceptable inner prepuce. By using only outer penile skin to cover the penile shaft, our technique enables the end cosmetic result to resemble closely that of a standard circumcision. This is due to the normal skin appearance in terms of color and texture without the furled appearance seen with the inner prepuce. This end result is, from our experience, highly acceptable to patients' parents.
With our technique, we invariably made an incision on the phimotic ring at the level of our traction stitches. Some surgeons excise this ring, like suggested by Leao et al., for fear of constriction band formation, but we believe that if we preserve the ring that helps provide an often essential little bit of extra skin that can be used for additional penile shaft skin cover particularly on the ventral side of the shaft. 21
All of our cases of megaprepuce had no associated chordee, so we felt there to be no need to routinely perform an erection test. However, there are other reports in Literature like Liu et al. who have performed artificial erection in all of their cases. 16
Postoperatively, there is only one scar visible aside from that of the circumcision scar and this is on the ventral aspect of the penile shaft in the midline. In all our cases we found that this acceptably resembles the penile midline raphe. This scar is as a result of the inverted Y-shaped incision made to correct the penoscrotal transposition. It could be considered, and is by the authors, that this ventral scar is a small price to pay for the cosmetic benefit afforded by the new caudal position of the scrotum made possible by this incision (Figs. 6 and 7). Placement of these incisions in the midline on the ventral penile shaft and skin creases helps form a scar that is almost invisible by the time it is seen postoperatively at a few months thus providing little to no compromise on an excellent cosmetic result.
In our series, seeing as we encountered no major complication and none of the patients needed redo surgery, our procedure of megaprepuce correction can be regarded, in our opinion, as safe. We appreciate that the number of cases presented in this study is relatively small, but given the excellent cosmetic and functional results achieved, we believe this technique to be the sign of a promising future for patients with CMP.
Conclusion
Our modified surgical procedure to correct CMP is a safe and simple technique, providing good cosmetic results with the appearance of a standard circumcised penis. This also provides a good functional outcome with a low complication rate. This technique is easy to reproduce and teach compared with other complex procedures.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no funding for this study.