
Abstract
Background:
A recent meta-analysis showed that the primary closure (PC) of the biliary duct in the absence of T-tube (TT) drainage is a safe alternative for cholelithiasis after laparoscopic biliary exploration. However, its feasibility, benefits, and indications in hepatolithiasis remain undefined.
Patients and Methods:
From October 2008 to October 2012, we enrolled 84 patients with intrahepatic bile duct stones who underwent laparoscopic bile duct exploration (LBDE) and/or hepatectomy with TT-drainage or PC. The operative outcomes, intraoperative performance, and feasibility of the procedures were compared.
Results:
Forty-one patients who underwent TT insertion were compared with 43 patients who underwent PC. No mortalities were observed following either procedure. The median postoperative hospital stay was shorter in PC (5.4 ± 3.5 days) versus TT (8.9 ± 3.2 days; P = .006). The median recovery time (full activity and return to work) was similarly shorter in the PC group (11.6 ± 5.1 days) compared with the TT group (22.4 ± 13.2 days; P = .005). The incidence of postoperative and biliary complications was lower in the PC versus the TT group.
Conclusions:
PC is beneficial in patients requiring LBDE and/or hepatectomy, and shows a similar safety profile to TT.
Introduction
Traditionally, the biliary duct is closed through the insertion of a T-tube (TT) after choledochotomy,1–3 but this leads to complications and discomfort. To circumvent this, primary closure (PC) of the bile duct has emerged as a safe alternative after laparoscopic biliary exploration.4,5 Theoretically, PC should improve the laparoscopic treatment of hepatolithiasis in the absence of TT drainage, but this to date, remains unexplored.6,7 In this study, we retrospectively analyzed the outcomes and efficacy of patients undergoing laparoscopic hepatectomy and biliary exploration for hepatolithiasis with PC of the biliary duct compared with TT drainage, and investigated its optimal indications.
Patients and Methods
Patients
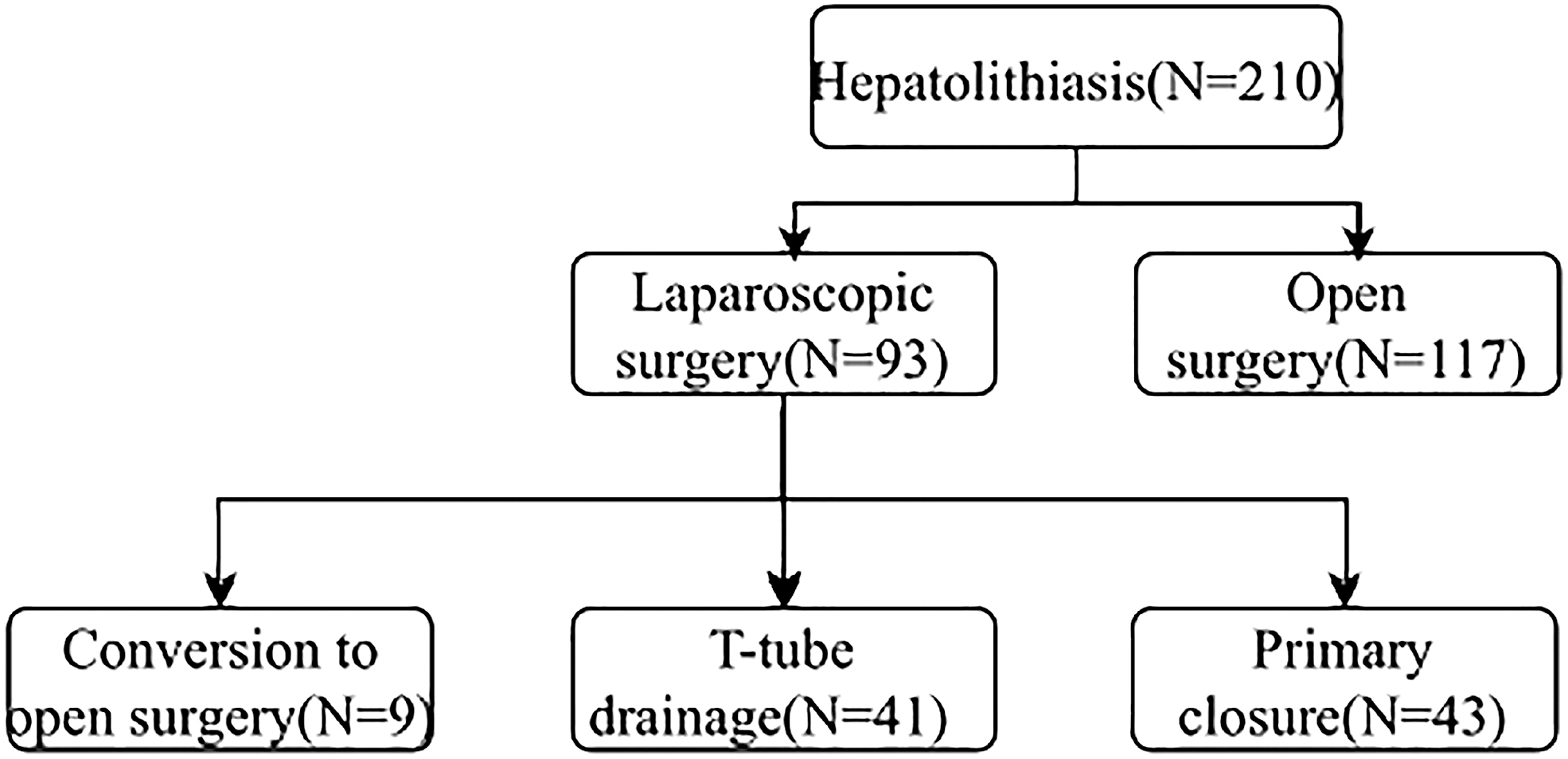
We enrolled 210 patients from October 2008 to October 2012, with 117 receiving hepatolithiasis with open surgery and 93 receiving laparoscopic surgery. Surgery was performed by 3 doctors across two institutes (Fig. 1). Of those receiving laparoscopic surgery, 9/93 required open surgery due to laparoscopic bile duct exploration (LBDE) failure. Of the 84 successfully treated patients, 43/93 underwent PC and 41/93 received TT drainage. Both groups were retrospectively reviewed according to demographic data, operation time, the duration of hospital stay, and occurrence of complications. Patients were followed up for ≥1.5 years.
Patients were randomized to either T-tube or primary closure by the intended method.
Surgical procedures
Laparoscopic hepatectomy (LH) and LBDE were performed as previously described.6,8,9 Liver transection was performed with ultrasonic shears (Qingsheng) or electric scalpels (Tianjin). After general anesthesia, patients were placed in the supine position and CO2 mediated pneumoperitoneum pressure was applied (13–15 mmHg). The porta hepatis was dissected to expose the hepatic artery, and portal vein branches were prepared for clipping or occlusion. An excised line was marked on the liver surface and the liver parenchyma was transected with the selective occlusion of the liver lobe inflow and small vascular and biliary structure. The main hepatic vein branches were divided with clips. 7 After dissection of the liver parenchyma, the hepatic bile ducts were left open for exploration through the remnant orifice. Postexploration, the ducts were closed through the insertion of a TT for decompression. The resected specimen was then divided and extracted through a small incision created through the extension of the wound at the epigastric port.7,8
Laparoscopic bile duct exploration
We used a dual camera to visualize the intra-abdominal and intraductal regions. Calot's triangles were dissected and cystic ducts and arteries were isolated. Longitudinal choledochotomy was performed at the anterior wall of the common bile duct (CBD). A 5 mm flexible choledochoscopy (external diameter 4.9 mm; OLYMPUS CHF P20, Japan) was inserted into the duct and advanced proximally and distally to identify stones and ductal structures.6–8 Stone identified in CBD and intrahepatic bile duct stones (IHD) were removed through irrigation, a stone basket, and a balloon-tipped catheter.
Evaluation of stone clearance and follow-up
Cholangiography was performed with ultrasonography (US) and/or computed tomography (CT) to confirm the clearance of the stones. Liver function tests and US were performed every 3–6 months or upon the reporting of symptoms to rule out stone recurrence. CT and/or cholangiography were further performed. We defined stone recurrence as cholangitis or the actual visualization of the recurrent stones.
Statistics
Categorical data are shown as counts and percentages. Chi-square tests were used to compare TT and PC groups. Continuous variables are shown as the mean ± SD, median, and interquartile range. A Student's t-test or Mann–Whitney test was used for data comparisons. P ≤ .05 were deemed significant differences.
Results
The baseline characteristics of the patients were similar in TT and PC groups (Table 1). We identified extrahepatic stones in 52 patients (61.9%). In terms of treatment procedures, 51 patients (60.7%) underwent LBDE and hepatectomy, and 33 patients (39.3%) underwent LBDE alone. A single PC patient and 2 TT patients retained stones after LBDE. A single PC patient underwent endoscopic sphincterotomy (EST) to remove their retained stone. Two TT patients received postoperative cholangiography with the retained stones removed through the sinus tract of the TT through the application of a choledochoscope.
Patient Characteristics
ASA, American Society of Anaesthesiologists; COPD, chronic obstructive pulmonary disease.
The median duration of postoperative hospital stays was lower in the PC (5.4 ± 3.5 days) versus TT group (8.9 ± 3.2 days; P = .006, Table 2). The median recovery time (deemed as full physical activity and return to work) was shorter in the PC (11.6 ± 5.1 days) versus the TT group (22.4 ± 13.2 days; P = .005). The median operative time was lower in the PC versus TT group, but the differences were not significant. No differences in loss of bleeding or median time to remove the peritoneal drain were observed between the groups.
Comparison of Clinical Outcomes Between the Two Groups
IQR, inpatient quality reporting; LBDE, laparoscopic bile duct exploration; LH, laparoscopic hepatectomy.
No postoperative deaths were reported. In the PC group, 5 patients reported complications postsurgery (11.6%), with 4 (9.3%) showing biliary complications (Table 3). In the PC group, 2 of the patients reported low-level bile leakage, which spontaneously ceased upon prolonged peritoneal drainage. A single patient reported subhepatic bile accumulation on day 3 postoperation, which showed a favorable outcome after endoscopic retrograde cholangiopancreatography and stent insertion. Other complications included acute pancreatitis (1 patient) and deep venous thrombosis.
Biliary Complications in the Two Groups
In the TT group, complications were reported in 11 patients (26.8%), 9 of which (21.9%) were biliary associated (Table 3). Leakage occurred in 4 patients around the TT drainage site, which ceased spontaneously with extended peritoneal and TT drainage. A single patient received percutaneous drain insertion treatment due to subhepatic bile accumulation, and was responsive to conservative therapy. In 2 patients, jaundice due to a twisted TT and bile duct obstruction occurred. This patient was treated with a replacement TT through repeated laparotomy. A total of 2 patients displayed acute pancreatitis but responded to medical intervention. A single patient reported acute pneumonia and deep vein thrombosis.
The number of postoperative and biliary complications was higher in the TT group (Table 3), but the differences were not significant. No patients were missed during follow-up. Median follow-ups were 18 months with no reports of bile duct stones or strictures recorded.
Discussion
Hepatolithiasis is deemed a refractory disease, typically treated with liver resection and operative IHD to remove stones through choledochotomy. Hepatectomy shows efficacy for hepatolithiasis therapy; however, some hepatic stones persist, resulting in bile duct strictures, fibrosis, abscesses, and carcinomatous bile ducts.10,11 In recent years, laparoscopic surgery has improved liver resection and is increasingly documented as an effective procedure.12–14 A single lobe or hemi-liver infection showing intrahepatic strictures, with stones absent in the other liver lobe are the optimal indications of laparoscopic liver resection and intrahepatic bile duct stones exploration. However, upon the occurrence of hepatolithiasis in the liver lobes, or in situations of severe intrahepatic duct strictures bilaterally with stones filling the peripheral bile duct branches making them inaccessible for exploration, LR is challenging and open surgery is preferred. Laparoscopic exploration of the intrahepatic bile duct stones can be performed to remove duct remnant oracles. CBD excision can also achieve LH. Intraoperative choledochoscopy for intrahepatic stones improves the visualization of the biliary tree.10,11 Intrahepatic bile duct exploration can completely remove the stones, but intrahepatic stones remain small in the absence of bile duct stenosis. In this study, we demonstrated that laparoscopic intrahepatic bile duct exploration produces favorable therapeutic outcomes for the treatment of intrahepatic stones, if no association with the severe ductal strictures and impacted stones are observed.
Bile duct exploration (BDE) during open surgery and laparoscopically is typically accompanied by TT drain placement. TT permits BDE exploration and allows stones to be extracted with the steerable catheter. TT also controls the biliary fistula; and provides ease of access for holedochogrophy or direct visualization of the bile duct to ensure complete clearance, in addition to the exploration of the distal BDE for other possible causes of obstruction. However, complications occur when using TT for biliary drainage, including fluid and electrolyte imbalances, infection, dislodgement, bile leakage, pain, peritonitis, biliary fistulae, and late biliary strictures. The TT tube also fails to prevent bile leaks in situ.1,2,15 Magnetic resonance cholangiography (MRC) is the most accurate noninvasive (nonendoscopic) procedure to detect common bile duct stones, with a sensitivity of 85%–92% and a specificity of 93%–97% reported in large study cohorts.16–18 Choledochogrophy through TT can substitute for MRC, but the sensitivity of detection does not improve. Controversy regarding PC exists due to the ease of access of choledochogrophy for direct visualization and extraction of the retained stones postoperatively. Retained stones are challenging during hepatolithiasis therapy1,10,11,13,19,20 as they fill peripheral bile duct branches that are inaccessible to exploration in residual liver lobes. Typically, HL is indicated for laparoscopic assessments if a single lobe is impacted. The stone must be cleared and if retained and biliary stenosis occurs during endoscopic ultrasonography or intraoperative colangiogram, the placement of TT is mandatory. In our series, a single PC patient retained a stone, compared with 2 TT patients. It is, therefore, important to define the indication using these surgical procedures.
Laparoscopic exploration of the CBD is performed during LH for the management of hepatolithiasis. The rationale was the same as the open technique for the one-stage approach for common bile duct stones to avoid endoscopic stone extraction and its associated costs and complications. Previous studies21,22 revealed the procedure to be both safe and feasible and could significantly reduce operative times, morbidity, and hospital stays in the common bile duct exploration compared with TT drainage during open and laparoscopic procedures, with no increase in stenosis. With increasing acceptance of the technique and improved surgeon experience, laparoscopic cholecystectomy bile duct exploration in the absence of biliary drainage is more widely practiced. In this series, we observed significantly shortened hospital stays and complications during PC compared with TT. These factors could have been influenced by other factors that are independent of postoperative recovery. Over time, we used TT drains with decreasing frequency as selective as opposed to routine use was employed. With our increasing experience, TT drains were employed in cases of retained impacted stones and biliary stenosis that required endoscopic extraction, or demonstrated severe cholangitis in the CBD. Similarly, Krauss and Kern 23 in studies of 867 open choledochotomy patients with PC, received TT drainage for cholangitis, gross inflammation, or a thin CBD. While we observed minimal bile leakage in PC, 3 cases were observed, 2 of which originated from choledochotomy excision after TT drainage, with the other case originating from the liver transection area. All patients were conservatively treated with a suction drain and made a rapid recovery.
In summary, this series showed that LH and/or LBDE is effective for type A and B hepatolithiasis. PC was feasible, beneficial, and as safe as TT drainage in patients with hepatolithiasis in which at least one lateral lobe was not impacted, and peripheral stones lacking bile duct or sphincter of Oddi strictures were observed. This prospective study now requires confirmation in a larger cohort to confirm the indications for PC.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.