
Abstract
Objective:
To evaluate the clinical efficacy and safety of transanal minimally invasive surgery (TAMIS) for the treatment of benign rectal lesions so that patients can be provided with better surgical alternatives.
Materials and Methods:
A retrospective analysis was conducted on patients with rectal benign lesions who underwent TAMIS in the Department of Gastrointestinal Surgery, the First Affiliated Hospital of Chongqing Medical University from January 2018 to June 2019. The patients' clinical data were thoroughly recorded, such as surgical-related information, postoperative pathology, and so on. At the same time, the patients were followed up regularly and carefully after the surgery.
Results:
A total of 16 eligible patients were enrolled in the study. All patients underwent colonoscopy before surgery and the biopsy results showed that all the removed specimens were rectal benign tumors. All the lesions were resected with TAMIS. The average operation time was 111.94 ± 46.13 minutes. Among the 16 cases, 1 of the patients was found to have undergone peritoneal entry during operation 1 and this showed that the peritoneal cavity was penetrated during the operation. The average postoperative hospital stay was 4.56 ± 1.79 days. The final pathology of the TAMIS specimens revealed a malignant neoplasm in 10 patients, including 9 cases of rectal adenocarcinoma, 1 case of nerve endocrine tumor, and 6 cases of rectal adenoma. No long-term complications were observed during the mean follow-up time of 10.19 ± 5.14 months.
Conclusions:
TAMIS is a safe and effective minimally invasive surgical procedure for the treatment of rectal adenomas, which can minimize the adverse effect on anal function.
Introduction
Due to the special anatomical location of the rectum, surgeons have encountered challenges in choosing the best surgical procedure for resection of rectal tumors.
For rectal benign tumors and early malignant tumors, the lesions are preferentially removed by local excision (LE) to achieve the goal of minimizing surgical trauma. Transanal excision (TE) is the mostly used LE procedure. However, it cannot guarantee high-quality excision of the lesion for the middle and distal rectal lesions due to poor exposure and inferior visibility.1,2 Another surgical procedure is transanal endoscopic microsurgery (TEM). Compared with TE, TEM can achieve full-thickness resection with less trauma. What is more, it can ensure accurate resection of the lesions and enough remaining edge around the lesions via applying precision instruments in a sufficient field of view. 3 However, as a result of the high cost of special equipment and long learning curve, as well as the risk of anal sphincter injury, TEM has not been fully promoted and applied at home and abroad. 4
At the same time, laparoscopic techniques are developing rapidly, and single-hole devices are becoming more widely used. The technical cross between single-port laparoscopy and TEM prompts single-hole devices to be tried for transanal surgery. In 2010, transanal minimally invasive surgery (TAMIS) was used as an emerging minimally invasive technique for LE of rectal lesions. It was first reported and named by Atallah et al., 5 a surgeon at the Florida Hospital in the United States. The technique is to place a single incision laparoscopic surgery port (SILS™ Port, Covidien, Dublin, Ireland) in the anal canal and perform a rectal tumor resection via the anus by using conventional laparoscopic instruments. The application of TAMIS is similar to TEM, mainly for the local resection of the rectal benign or early malignant tumors. 6 However, due to the small amount of data published, it is still necessary to validate TAMIS in a well-defined patient cohort. Therefore, we introduced our initial experience in TAMIS. The purpose of this study was to explore the feasibility, postoperative complication rate, and histological outcome of TAMIS in patients with rectal tumors.
Materials and Methods
The study population included consecutive patients retrospectively identified from a single institution from January 2018 to June 2019. Individual patient data were reviewed and analyzed. Patients receiving treatment with TAMIS were selected according to the following criteria: (1) patients with large or recurrent lesions in the middle and distal rectum, with the colonoscopy biopsy for rectal adenomas; (2) patients who can endure general anesthesia. All TAMIS procedures were performed by a surgeon with sufficient experience in laparoscopic colorectal surgery. The study was conducted in accordance with the ethical standards of the Helsinki Declaration of 1975 and was approved by our hospital's ethics committee.
Surgery procedure
(1) Preoperative routine bowel preparation: including oral polyethylene glycol laxative and mechanical enema, prophylactic antibiotics (streptomycin 1 g, po, bid and metronidazole 200 mg, po, tid) 1 day before surgery.
(2) Anesthesia and position: TAMIS was performed on patients under general endotracheal anesthesia and on lithotomy position.
(3) Surgical operation: Routine disinfection was made and draped the area before surgery. The anus retractor was used to enlarge the anus and fix it; then, anal area disinfection was done again. Later, a multi-instrument access port designed for TAMIS (GelPOINT Path Transanal Access Platform; Applied Medical, Rancho Santa Margarita, CA) was inserted through the anus and the rectum was rinsed with iodophor water again. If necessary, the GelPOINT Path was sutured with the perianal skin and a laparoscope was placed. After the TAMIS operating platform device was completed, CO2 was injected into the rectal cavity with the pressure maintained at 10–12 mmHg. The proximal intestinal tube was filled with gauze with a traction line to prevent excessive colon expansion. A concentration of 1:200,000 adrenaline solution was injected to the tumor to reduce bleeding and expose the mucosa clearly. The electric knife was utilized to mark the circumferential edge at 5–10 mm distance from the edge of the tumor. Electroexcision and electrocoagulation were combined to cut the mucosa, submucosa, and muscularis root layer to achieve full-thickness resection. The final purpose was to ensure the integrity of the tumor level and vertical edge, and to maintain a 5–10 mm cutting edge. At the same time, we need to pay attention to protect the surrounding normal tissue. The wound was carefully checked for active bleeding and was sutured with a 3–0 barbed wire after the specimen was taken out.
(4) Specimen processing: No frozen section was taken during the operation. The removed tumor specimens were flattened after surgery, and they were fixed with multiple pins. The tumors were sent for pathological staging after treatment with formalin solution (Fig. 1).
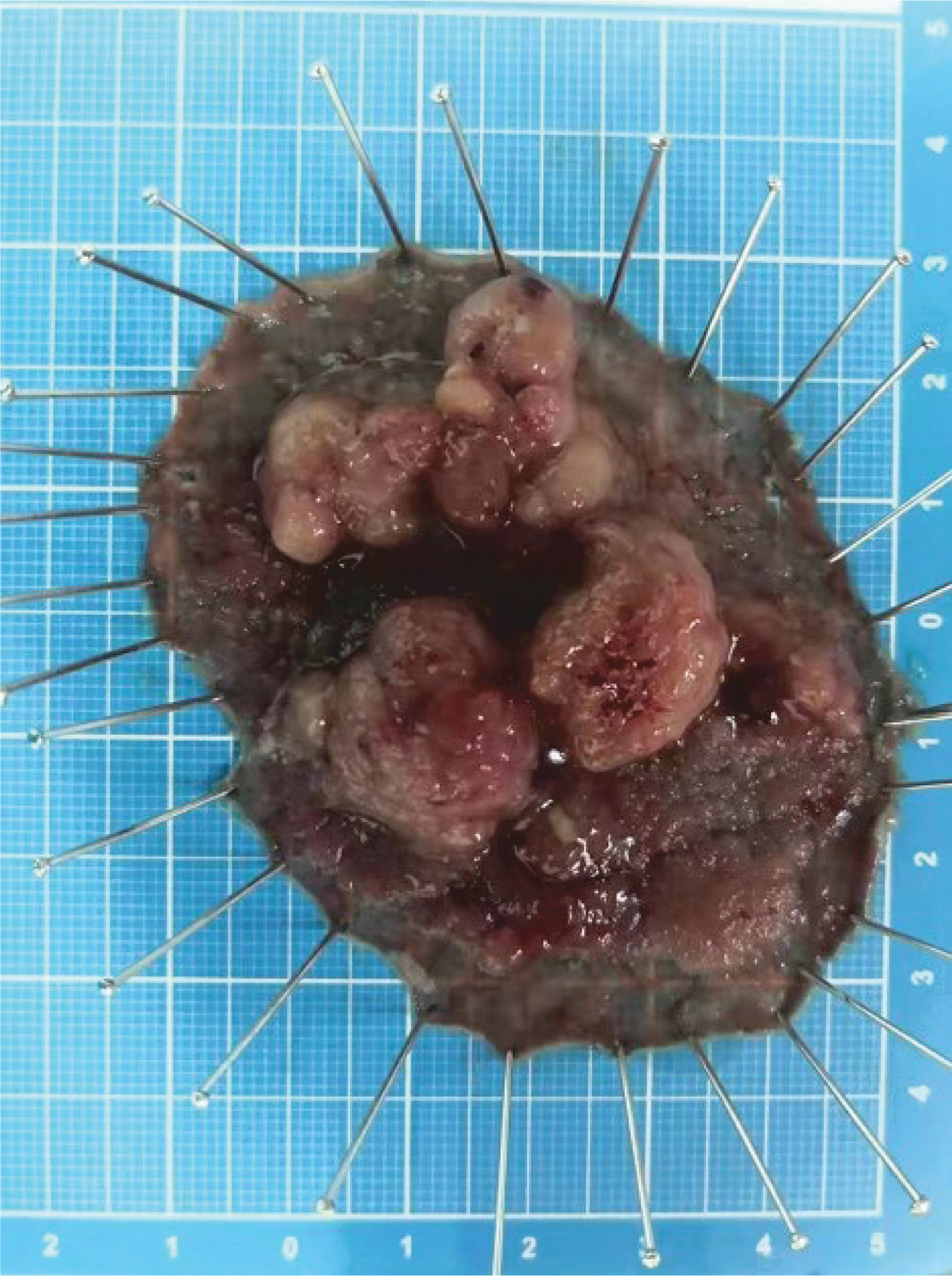
Fixation of a rectal adenoma specimen on a plate after TAMIS. TAMIS, transanal minimally invasive surgery.
Statistical analysis
Statistical analysis was performed with the SPSS statistical package SPSS v.24.0 (SPSS Inc, Chicago, IL). Continuous variables were expressed as the means ± standard deviation. Statistical comparison was conducted by using the Student's t-test for parametric data and the χ2 test for nonparametric data, respectively, with significance assumed at P < .05.
Results
All the 16 cases of surgery were successfully completed. The operation field was clear and stable. No air leaked and no accidents occurred during the surgery. According to the postoperative pathological results of the patients, they are divided into benign and malignant groups. Patients' demographics, clinical characteristics, operative characteristics, and pathologies are shown in Tables 1 and 2.Ten of the 16 patients were men.
Patients' Clinical Characteristics
SD, standard deviation; TAMIS, transanal minimally invasive surgery.
Patients' Operative Characteristics and Pathologies
NET, nerve endocrine tumor; SD, standard deviation.
The mean age of the patients was 64.63 ± 12.31 years old, and the average body mass index was 22.79 ± 4.36 kg/m2. Among the 16 patients, 3 of them underwent local resection of the endoscopic lesion before TAMIS surgery, with the exception that the lesion in 1 out of the 3 cases was too large (80 mm × 60 mm) to be completely removed by colonoscopy, so the lesion of (40 mm × 40 mm) size was retained. The average diameter of the lesion was 3.16 ± 2.28 cm, and the average distance to the anal margin was 6.94 ± 3.87 cm. Postoperative pathological results showed that all the rectal tumors of 16 cases were completely resected, with all the margins being negative.
Among them, 6 cases were rectal adenoma and 10 ones were malignant tumors, including 1 case of nerve endocrine tumor and 9 cases of adenocarcinoma. Patients were placed in the lithotomy position during the surgery. The average operation time was 111.94 ± 46.13 minutes, and the average volume of blood loss during operation was 19.19 ± 22.64 mL. Inadvertent peritoneal entry occurred in 1 patient with an anterior quadrant rectal lesion. The suture repair was successfully conducted with no obvious signs of peritonitis after surgery. The average postoperative hospital stay was 4.56 ± 1.79 days with no surgical death or serious complications. One of the patients had a final pathological diagnosis of T2 with a negative margin, and the preoperative examination showed no peripheral lymphatic and vascular invasion. But he refused further surgery of rectal low anterior resection because of his old age (81 years old) and poor health.
Two of the 16 patients developed postoperative complications. One patient complained of obvious abdominal pain and self-limited fever, with surged postoperative blood cell count, such as the white blood cell count being 12.48 × 109/L and 11.49 × 109/L, the percentage of neutrophils being 91.3% and 88.8%, respectively on the first and third day after surgery. Thus, the diagnosis of peritonitis was considered and the symptoms were relieved after anti-infection management with cephalosporin. Another patient manifested mild abdominal pain and the symptom was relieved with no special treatment. The average follow-up time was 10.19 ± 5.14 months and none of the following situations occurred during this period, such as local recurrence, difficulty in defecation, and rectal stenosis.
Discussion
The TEM has been widely recognized and considered safe and effective since its first launch. 7 It utilizes a specific equipment and endoscopic instrument to enlarge the three-dimensional view of the 220° rectum, and it can reach to the position of 24 cm distance from the anal verge so that the selected low, middle, and high positions of rectal tumors can be accurately removed. 8 However, TEM has not been widely used for a variety of reasons, including the requirement for expensive and professional equipment as well as steep learning curves. What is more, TEM technology has a risk of postoperative anal dysfunction and its indications are very limited. 4
Therefore, TAMIS has been introduced as a hybrid technique for TEM and single-port laparoscopic resection of rectal lesions. The indications for TAMIS are similar to those of TEM and TE 9 ; TAMIS gains an upper hand over TEM on the short installation time, greater rectal lumen visibility (360° versus 220°), greater adaption to the existing laparoscopic instruments, and being significantly less costly.5,10–14
Traditional TE can be used to remove lesions within 6 cm from the anal verge. 15 But due to the tightness of the anal canal and limited surgical area, the operation can be difficult for the lesions on the position beyond the lower rectum, namely 4–5 cm from the anal margin. Therefore, for middle rectal lesions, TE does not guarantee adequate marginal or full-thickness resection. TAMIS can solve this problem perfectly. The average distance from rectal lesions treated with TAMIS to the anal margin in our study was 6.94 ± 3.87 cm. Other reports have indicated that the median distance from the anal margin to the lesion treated with TAMIS is 10 cm (range from 6–16 cm), 16 which is much longer than the average distance of our study. So TAMIS can be utilized to solve the problem of upper rectal lesions under the safety insurance.
Our average operation time is 111.94 ± 46.13 minutes, longer than that of 55–86 minutes shown in other reports.5,10,17–19 The varied timing method may result in this difference. First, we generally started the time when the TAMIS operation platform was installed, which may take longer lengths of time because of the relatively unskilled installation method. Second, the operation on those patients with larger lesions and wider basement is relatively more difficult, resulting in a longer average operation time.
In our study, lithotomy position was chosen for the operation no matter whether the lesion was located in the anterior or posterior wall of the rectum; for this reason, this is the first choice for most anesthesiologists and it is much easier for the installation of the TAMIS platform. Of course, other positions can be selected, such as jackknife position or lateral position. Jackknife position can be used for anterior quadrant rectal lesions, but what has to be considered is that the peritoneal cavity can be mistakenly broken for those lesions on the anterior and upper rectal wall.
Among our 16 patients, 1 patient suffered from peritoneal entry (6.25%). The lesion was located in the anterior rectal wall 7 cm away from the anal margin. After the lesion was completely removed, the wound was found to be extremely weak and it seemed that the peritoneal cavity was penetrated. Abdominal laparoscopic examination showed that the anterior wall of the rectum was weak, so the 3–0 barb line was used to strengthen the suture. The patient had no other complications after surgery except for the increased operation time. It was reported that peritoneal entry is unavoidable during the full-thickness resection for the lesions on the upper rectal anterior wall, thus it cannot be considered as a complication in this condition. 20
The TAMIS platform is more flexible than the TEM rigid rectoscope, with a smaller diameter (30 mm versus 40 mm) and a shorter length. Different from the four large-aperture sleeve holes of TEM equipment, the three-channel diameter of the SILS™ Port is 5, 5, 5 mm (which can be replaced by 12 mm). It has been reported that one of the cannulas can be replaced with a special casing pipe with an air valve to improve intraoperative smoke effects. 21 This type of equipment is equipped with a gas injection hole to establish a gas chamber with a standard CO2 pneumoperitoneum device. A 30° laparoscope is inserted into a 5-mm cannula for a 360° two-dimensional field of view, or an electronic colonoscope is used as a lens to obtain a proximal view of the lesion better. 22 Surgery is mainly performed by ordinary laparoscopic equipment (graspers, electric hook, ultrasonic scalpel, etc.). In summary, TAMIS devices are more flexible and easier to acquire than TEMs.
Studies have found23,24 that TEM is associated with short-term anal dysfunction, including a decrease in anal sphincter tension and a significant reduction in maximum resting and systolic blood pressure for up to 6 weeks after surgery. TAMIs' single-port multi-channel device is made of plastic and is flexible for a safe, noninvasive transanal access. Compared with TEM, TAMIS can reduce the effect on anal function.25,26 Our results also initially confirmed this conclusion. According to postoperative follow-up data, all patients had no symptoms of mild fecal incontinence or anal pendant expansion 2–6 weeks after surgery. A study has shown 25 that in most patients with impaired anorectal function before surgery, the anorectal function was significantly improved after TAMIS. Unfortunately, we did not evaluate the anorectal function of the patient before the operation, so we could not verify this conclusion.
In our study, all patients receiving TAMIS were confirmed to be diagnosed as having rectal adenomas before surgery, but the pathological stage of some patients was eventually upgraded from rectal adenoma to adenocarcinoma or focal cancer. It suggests that during the process of TAMIS, the circumferential margin should be marked more carefully and the margin should be far enough away from the tumor, so that a new treatment strategy can be provided for early rectal cancer. The average follow-up time of 16 patients was 10.19 ± 3.87 months, without any of the following situations, such as local recurrence, distant metastasis, anal dysfunction or rectal stenosis. However, it is not enough to explain the recurrence rate, survival rate, and other related issues because of our short follow-up time, so long-term follow-up and monitoring are needed to further verify them.
Of course, TAMIS also has certain technical flaws. For lesions farther from the anal margin, laparoscopic and electrocoagulation hooks, operating clamps, and other instruments are easy to interfere with each other, making the surgical field of the upper rectum narrow and difficult to operate. We only had 1 patient with a 20 cm lesion from the anal verge, the position of which seemed too high for TAMIS. But the TAMIS was still determined after discreet evaluation and finally successfully performed due to the tumor's small size and narrow base. Similarly, lesions at very low rectal locations are difficult to remove, because TAMIS devices may cover the lowest part of the rectum, which is a general limitation of the TAMIS platform.
At present, due to the scarcity of oncology data, only benign lesions and histologically favorable early malignant tumors are considered to be indications for TAMIS surgery because they are treatment-intended surgery. Suffering from IV Stage disease or local advanced stage is not an indication of TAMIS, unless the goal is to relieve the symptoms. 27 Like other local resection technique, TAMIS does not clear the lymph nodes, so it may cause insufficient resection. This limitation places emphasis on the correct selection of eligible patients and enhanced postoperative monitoring.
Conclusions
In a limited number of case reports, TAMIS has been shown to be safe and feasible. It provides a safe and effective method for benign rectal tumor resection and reduces the adverse effects on anal function. However, controlled studies and long-term follow-up are still needed to further verify the safety and effectiveness of this technique.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.