
Abstract
Background:
Bariatric surgery is the only treatment for severe obesity recognized as truly effective, and Roux-en-Y gastric bypass is one of the most frequent procedures. The aim of this study is to present a 3D laparoscopic bypass technique with intracorporal anastomosis, performed completely by hand.
Methods:
After positioning the patient and creating the 20 mL gastric pouch, the gastrojejunal anastomosis is performed with two continuous sutures of resorbable V-Lock 3.0. The same technique is used to do the laterolateral jejunojejunal anastomosis. All patients who have undergone the previously described procedure are included in our bariatric enhanced recovery after surgery (ERAS) protocol.
Results:
The combination between the by-pass ERAS protocol and the described technique reduces postoperative pain, and usually allows discharge of patients within 48 hours.
Conclusions:
In our experience, the technique using totally handsewn anastomosis is safe as those previously described in the literature and is cost-effective due to the use of continuous suture for the gastrojejunal and the jejunojejunal anastomoses instead of staplers.
Background
Bariatric surgery is the only treatment for severe obesity recognized as truly effective.
Gastric bypass is one of the most frequent procedures, normally performed using the Roux-en-Y technique, where the restrictive mechanism is combined with the intestinal malabsorption. 1
Since 1994, the most common technique used in bariatric surgery is gastric bypass by laparoscopy, which creates a small gastric pouch of ∼20 mL with restoration of intestinal continuity according to the Roux-en-Y technique. 2 Several techniques have been proposed for performing anastomoses.
In our department, proximal anastomosis is performed by circular staplers and the distal anastomosis by linear staplers. Although for gastrojejunal anastomosis different manual variants have been proposed and accepted, for jejunojejunal anastomosis, there still has not been any consensus.1,3
The manual technique for anastomosis is considered difficult, requiring advanced surgical skills. Nevertheless the complication rate is comparable with the mechanical anastomosis. High success rate of the manual technique is recognized in the literature. 4 For this reason, the teams that have access to robot will use it to perform manual intracorporal anastomosis, reducing the surgical skills required.
The introduction of 3D laparoscopy can achieve the same result as robotic surgery, with fewer complications and a shorter operating time than conventional laparoscopy. 5
A study from 20146 demonstrates how manual and mechanical techniques have a similar anastomosis leak rate, and have a similar outcome and improvement of comorbidities. In addition, the choice to perform anastomoses manually significantly reduces the cost of gastric bypass.
The aim of this study is to present a 3D laparoscopic bypass technique with intracorporal anastomosis, performed completely by hand.
Methods and Techinque Description
Patient installation and trocar positioning
The patient is positioned supine, with the legs apart, the right arm alongside the body, and the left arm apart. A gastric tube with uninflated 38F balloon is placed by the anesthetist. Installation is completed by positioning the arm of the hepatic retractor.
The pneumoperitoneum is performed using a Veress needle positioned in the left hypochondrium. Once a pressure of 15 mmHg is reached, we proceeded with the introduction of an optical trocar on the median line, between the umbilicus and the xiphoid processes, by using the Optiview technique with a 3D, 30° optics. Next, we proceeded to the introduction of two 5 mm trocars on the left flank and a third on the right flank under visual control. The trocar positioning is completed with the introduction of a hepatic retractor to allow retraction of the left lobe of the liver and allow full exposure of the area.
Gastric pouch
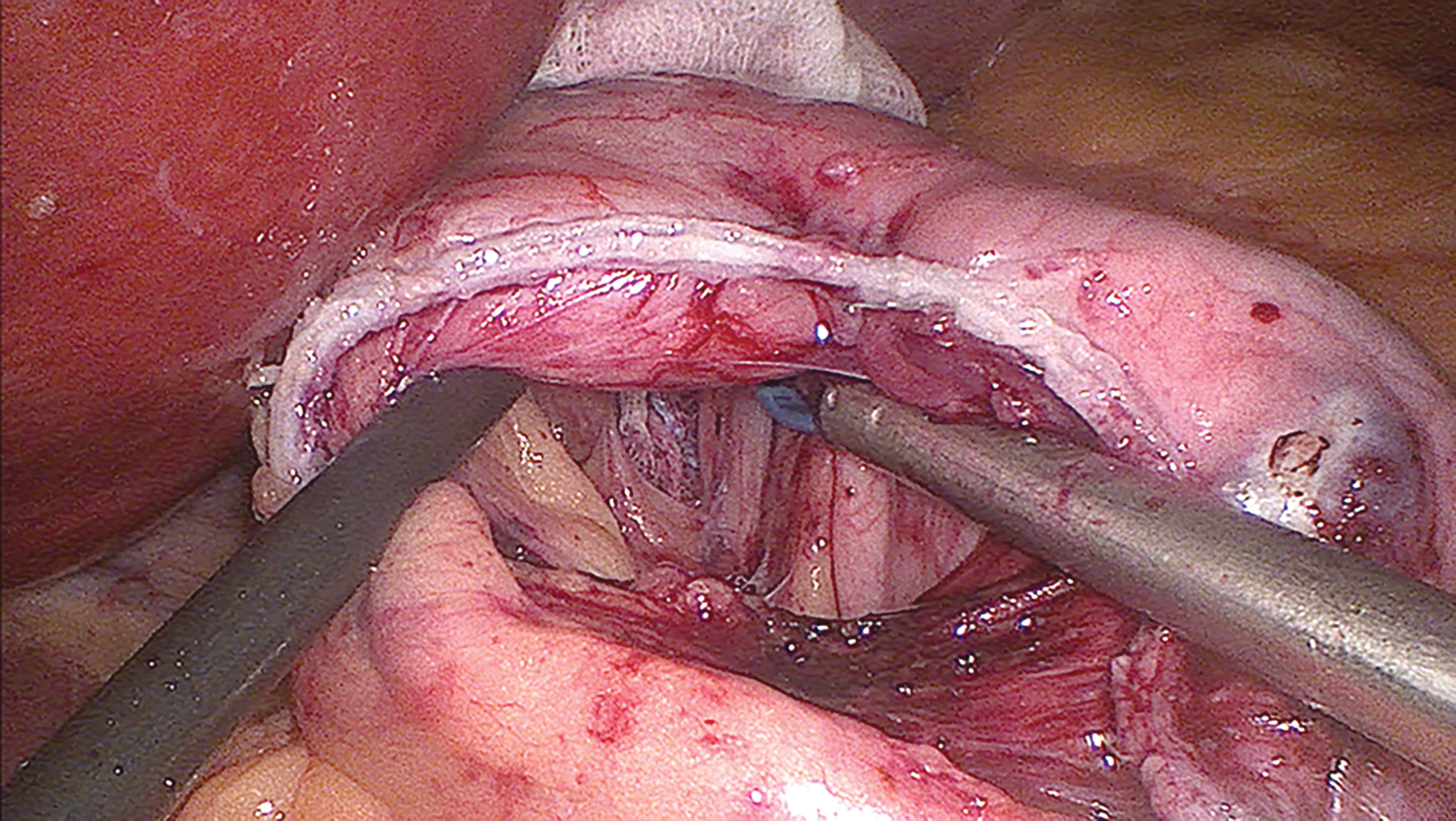
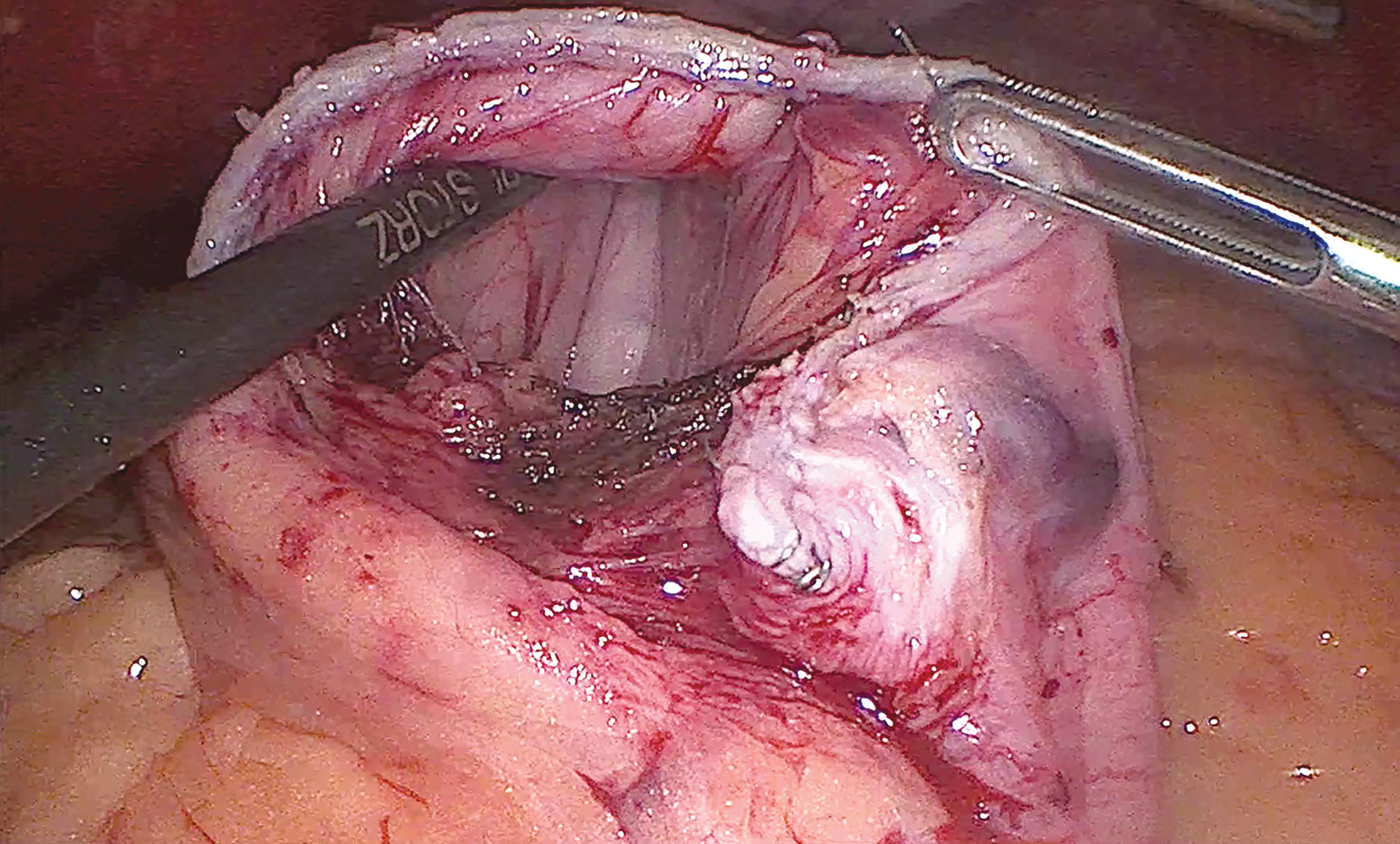
Dissection begins at the left diaphragmatic pillar, using an ultrasonic dissector device (Ultracision®), to penetrate the lesser sac. A surgical pad is placed in the retrogastric space (Fig. 1), and dissection of the omentum on the right side of the stomach allows the operator to enter the retrogastric cavity. Visual acquisition of this space is facilitated by the surgical pad previously positioned on the left side (Fig. 2), which joins with the angle of His. The gold finger is passed from the right side to the left to spread the stomach and allow the linear stapler to be inserted. Given the presence of a single 10 mm trocar, the stapling is performed by means of a 5 mm 2D camera introduced through the left trocar. This step avoids the insertion of a second 10 mm trocar, therefore, reducing postoperative pain.

Placing the compress in the retrogastric space.
Identification of the compress that facilitates entry into the retrogastric space.
For linear stapling, we usually use Medtronic®'s Endo-Gia, with a 45 mm purple horizontal charger and one or two 60 mm purple chargers. Before stapling, it is imperative to retract the gastric tube previously installed. Once the gastric section has been completed, the surgical pad is removed (Fig. 3).
Creation of the gastric pouch using a Covidien® Endo-Gia with a 45 mm purple charger. Vision is obtained by a 5 mm camera through the lateral trocar with the stapler passing through the umbilical trocar.
Gastrojejunal anastomosis
After locating the angle of Treitz, the following 50 cm of jejunal loop will become the future biliary loop (for diabetic patients consider 100 cm7). This loop is raised up to the gastric pouch, in ante-colic position, and fixed with a Vicryl stitch.
The cut on both the gastric pouch and the jejunal loop is measured to obtain 2 cm diameter anastomosis. Such cut is performed using the ultrasonic dissector device. Gastrojejunal anastomosis is performed with two continuous sutures (first on the posterior wall, followed by the anterior one) of resorbable V-Lock 3.0. The gastric tube is used to calibrate the anastomosis (Fig. 4a, b).

A stitch between the alimentary loop and the excluded stomach is performed with Ethibond 2.0 to avoid a twist of the anastomosis. Subsequently, the alimentary loop is separated from the biliary loop using a 60 mm beige Endo-Gia. To check the tightness of the anastomosis, an air test is performed at the end of the gastrojejunal anastomosis procedure.
Jejunojejunal anastomosis
An Ethibond 2.0 traction wire is placed on the alimentary loop at 100 cm from the gastric pouch. The wire has the role to unite this loop with the previously sectioned biliary loop, and allow, using traction, a good exposure of both sides of the laterolateral anastomosis. The anastomosis is then started on the posterior wall with a continuous suture (full thickness stitches) of resorbable V-Lock 3.0.
Once the suturing of the posterior wall is completed, both sides of the anastomosis are opened for a length of 2 cm with Ultracision. The anastomosis is completed with a second continuous suture of the anterior wall with resorbable V-lock 3.0 (extramucosal stitches) (Fig. 5).
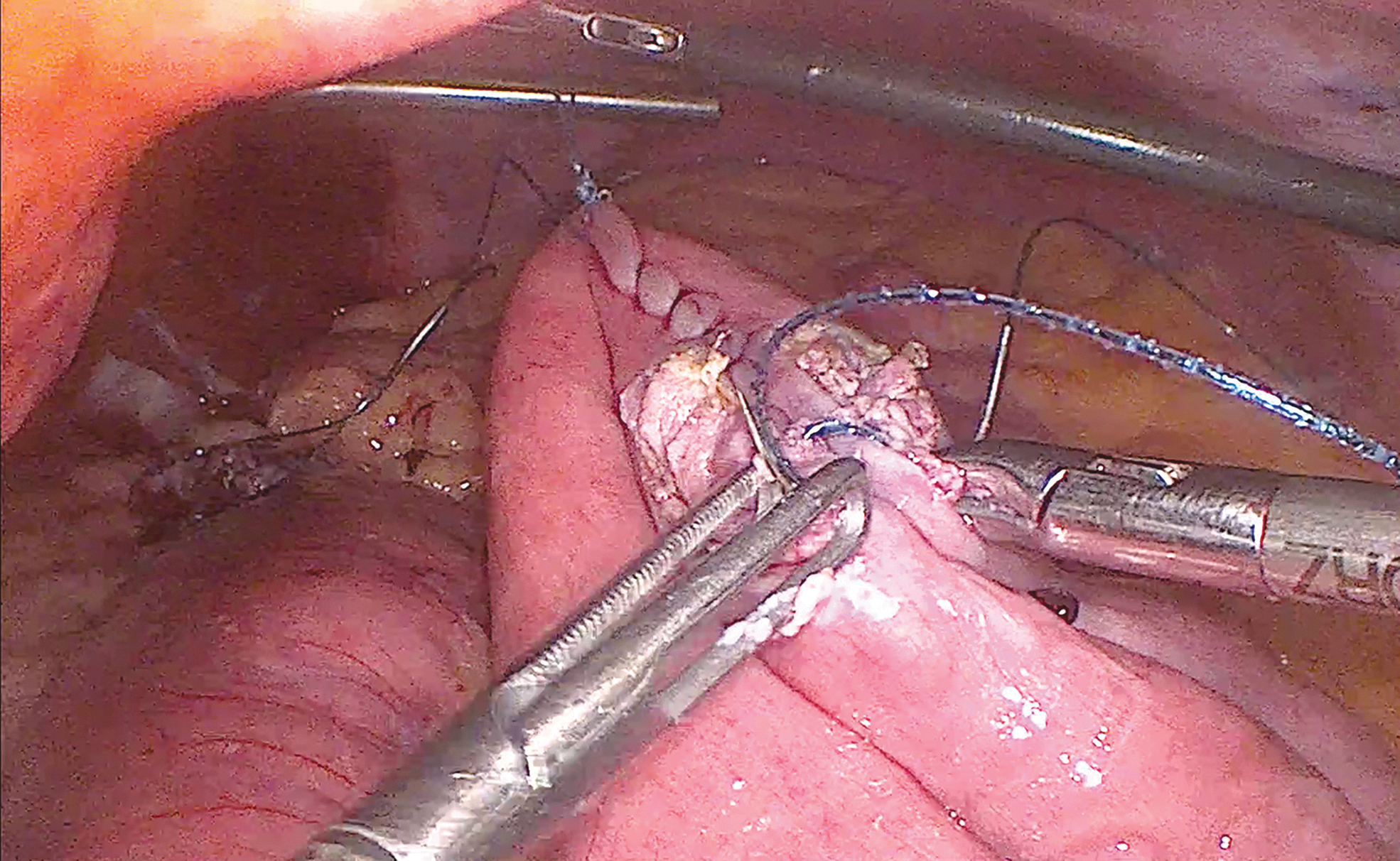
Closure of the anterior wall of the jejunojejunal anastomosis with a second continuous suture using resorbable V-lock 3.0.
Mesenteric windows and abdominal wall closing
The mesenteric window is closed with a nonresorbable V-Lock 3.0 continuous suture. Using the same technique, also the Petterson window is closed. Hemostasis is performed if needed, making sure that the systolic blood pressure is at least 130 mmHg.
Trocars are removed under visual control. The abdominal wall at the umbilical level is not necessarily sutured. The skin is closed with inverted stitches of Monocryl 4.0 and cyanoacrylate glue. The video of the entire procedure is available in Supplementary Video S1.
All patients who have undergone the previously described procedure are included in our bariatric enhanced recovery after surgery (ERAS) protocol.
Results
The combination between the by-pass ERAS protocol and the described technique reduces postoperative pain, and usually allows the discharge of the patients within 48 hours.
Conclusion
In our experience, the technique using totally handsewn anastomosis is safe as those previously described in the literature and is cost-effective due to the use of continuous suture for the gastrojejunal and the jejunojejunal anastomoses instead of staplers.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.