
Abstract
Introduction:
A leak at the esophageal anastomosis can occur in 10%–20% of cases of esophageal atresia (EA). Thoracoscopic repair is trans-pleural, with the potential development of an empyema. Standard treatment of an anastomotic leak in a stable patient is often nonoperative, which can lead to prolonged parenteral nutrition and hospitalization. Our objective is to show that early thoracoscopic redo anastomosis management is safe and feasible.
Materials and Methods:
Retrospective study of a case series of four infants, diagnosed with EA and treated with early thoracoscopic esophageal leak repair between 2013 and 2018. Variables analyzed included age, weight, type of EA, day of leak, surgical approach, time to start feeding, surgical complications, and follow-up.
Results:
Three patients were type III, and one was type I originally repaired with a thoracoscopic approach. Leaking of the anastomosis was found the second postoperative day in one patient, third day in two patients, and the fifth day in the last one. All were confirmed with an esophagogram. All patients were operated in the first 24 hours after diagnosis by the thoracoscopic approach. The site of leak was found and re-sutured. Patients started feeding between the third and fourth day through a transanastomotic tube, starting oral feeding at the seventh day after an esophagogram did not show a leak. No complications were found. Mean time to complete oral feeding was 10 days. Two patients needed esophageal dilations. Mean time of follow-up has been 33 months.
Conclusion:
Early thoracoscopic repair of an anastomotic leak can be considered an alternative to the standard nonsurgical management. The early re-suture of the area of leak is a change in paradigm, but it offers the benefits of preservation of the native esophagus, early resumption of enteral feedings, and a shorter length of parental nutrition and hospitalization.
Level of Evidence:
IV
Introduction
Esophageal atresia (EA) is one of the most challenging surgical conditions in neonates. Even though mortality has decreased over the past 30 years, complications from the operation are still significant. In a 1985 report, Bishop et al. demonstrated that 271 patients with EA who were treated in three different time periods had similar complication rates. 1
An anastomotic leak is one of the most significant complications. Over the past 30 years, these patients have generally been managed by observation, drainage if indicated, and antibiotic administration. In 1990, MacKinnon described his experience with management of babies with EA and found a 21% rate of anastomotic leak. 2 All “minor” leaks were treated conservatively, and two patients with a “major” leak underwent reoperation after failure of conservative management. It was felt that an anastomotic leak was directly related to tension on the anastomosis.
In addition, an anastomotic leak can result in anastomotic stenosis. In a 2003 report, Van der Zee and Bax described his results in patients undergoing EA and distal fistula. 3 Two of 13 infants (13%) had an anastomotic leak, although one of them had a long-gap type III EA. Both were treated conservatively and developed an anastomotic stenosis, which required esophageal dilation.
In 2005, Holcomb et al. 4 described a 7.6% incidence of an anastomotic leak in a multi-institutional study of 104 infants undergoing thoracoscopic repair of EA/tracheoesophageal fistula (TEF). None of these patients underwent early reoperation.
The objective of this report is to describe an early reoperation approach for infants who develop an anastomotic leak and to show that this approach is feasible and safe.
Materials and Methods
This is a retrospective case series of four EA patients, who underwent a thoracoscopic repair from 2013 to 2018, at two different centers. These infants developed a leak as an early complication from their thoracoscopic repairs. The anastomotic leak was identified by saliva in the chest drain or the development of a pneumothorax and was confirmed by an esophagogram. Patients who were treated with an initial open operation or who were managed conservatively were not included in this case series.
Data that were assessed included the patient's age at diagnosis, gender, diagnostic methods, type of EA, operative procedure, day of identification of anastomotic leak, and time to initiation of feeding. Intraoperative and postoperative complications are described as well.
Surgical technique
All patients underwent a thoracoscopic procedure using the same operative approach. The babies were placed in a lateral-prone position, and the reoperation occurred using ports which were placed through the previous sites from their initial operation. First, a 5 mm cannula was introduced at the tip of the scapula, and insufflation was set at a 5 mm Hg. Following initial diagnostic thoracoscopy, two additional 3 mm cannulas were inserted in the axillary region and the seventh intercostal space under visualization. The esophagus was identified and dissected, beginning distal to the anastomosis and proceeding toward the anastomosis. Dissection was carefully and gently performed using a blunt technique until the complete anastomosis could be seen and the area of leak was isolated (Fig. 1). The site of the anastomotic leak was then resutured with 5-0 and/or 6-0 polypropylene or polyglactin interrupted sutures (Fig. 2). A nasogastric transanastomotic tube was introduced in each patient, and a chest drain was situated near the anastomosis.
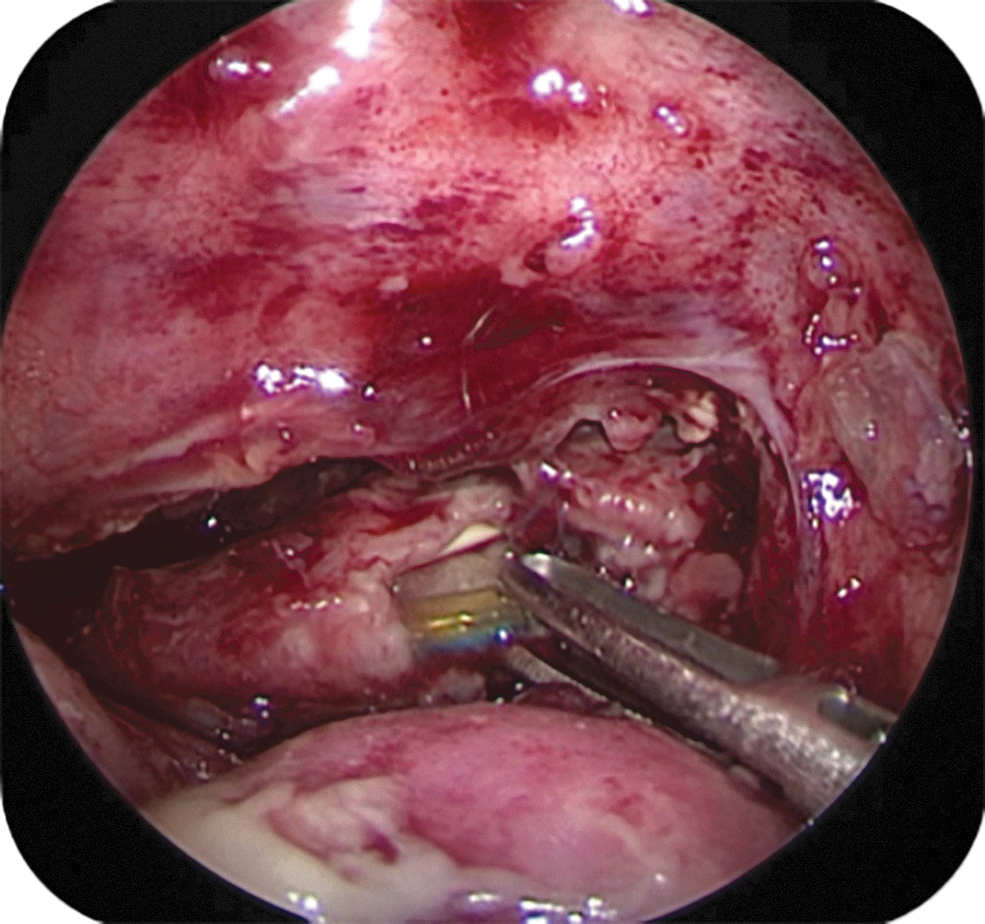
Visualization of the disrupted anastomosis previous repair.
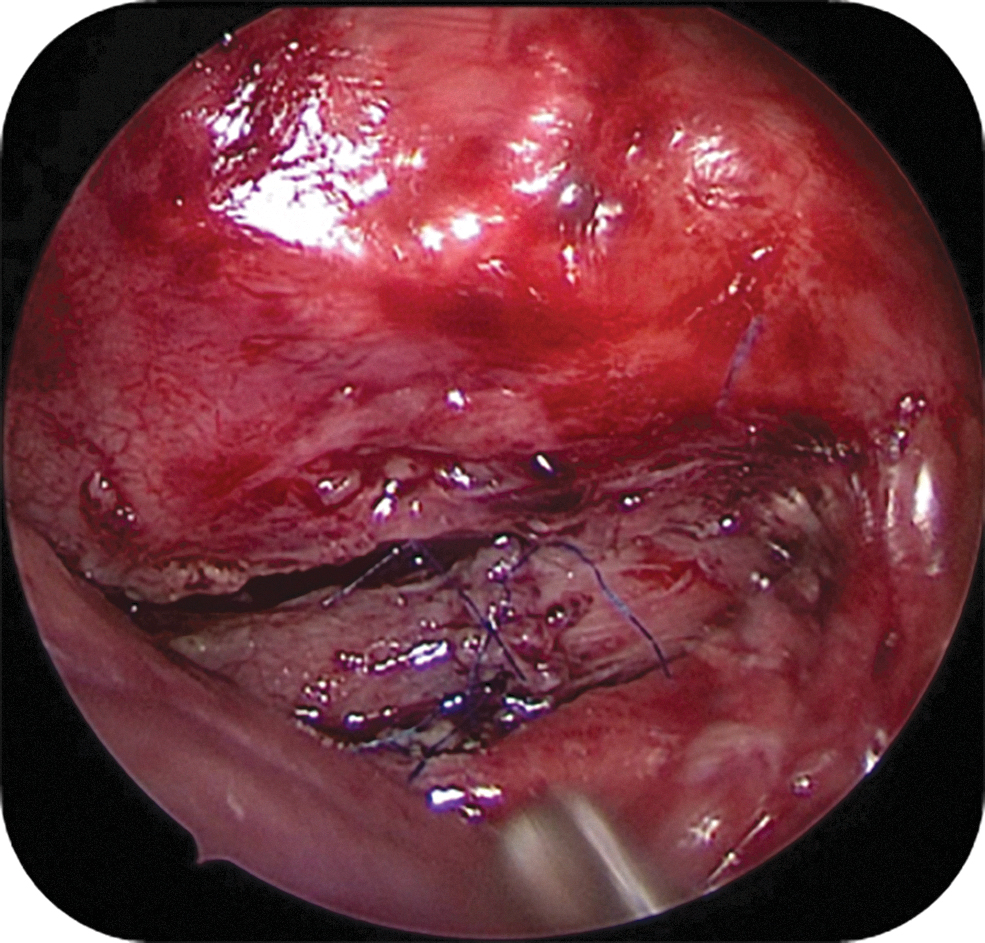
Final visualization of repaired anastomosis.
Results
Four patients underwent early operation for their anastomotic leak. All patients were born at term with the mean birth weight of 2.7 kg. Three patients had a type III EA, and 1 had a type I EA. The three type III patients underwent their initial operation within the first 2 days of life, and the patient with type I EA underwent initial gastrostomy and 6 weeks later underwent the thoracoscopic EA repair. In all four patients, the anastomotic leak was identified between the second and the fifth day after the operation: the second day in one patient (Fig. 3), the third day in two patients (Fig. 4), and the fifth day in the final patient (Fig. 5). Diagnosis was made by observing saliva in the chest drain or pneumothorax in a chest X-ray. Our standard consists on confirming the leakage with an esophagogram in every patient. They only presented mild ventilatory requirement and were hemodynamically stable, without signs of sepsis. All four patients underwent operation within 24 hours after diagnosis of the anastomotic leak. The site of leaking was identified and repair performed as described. These babies started feeding either on the third or fourth postoperative day through the transanastomotic tube. Oral feeding started on the seventh postoperative day after an esophagogram was performed and no leak was identified. No immediate complications were found during and after the second operation. Long-term follow-up found that one patient needed two esophageal dilations and another one needed four dilations in addition to a Nissen fundoplication. The other two patients did not require any other further operative procedures or dilations. The mean time of follow-up has been 33 months.

Esophagogram with a leak on day 3 after primary repair on patient 1.
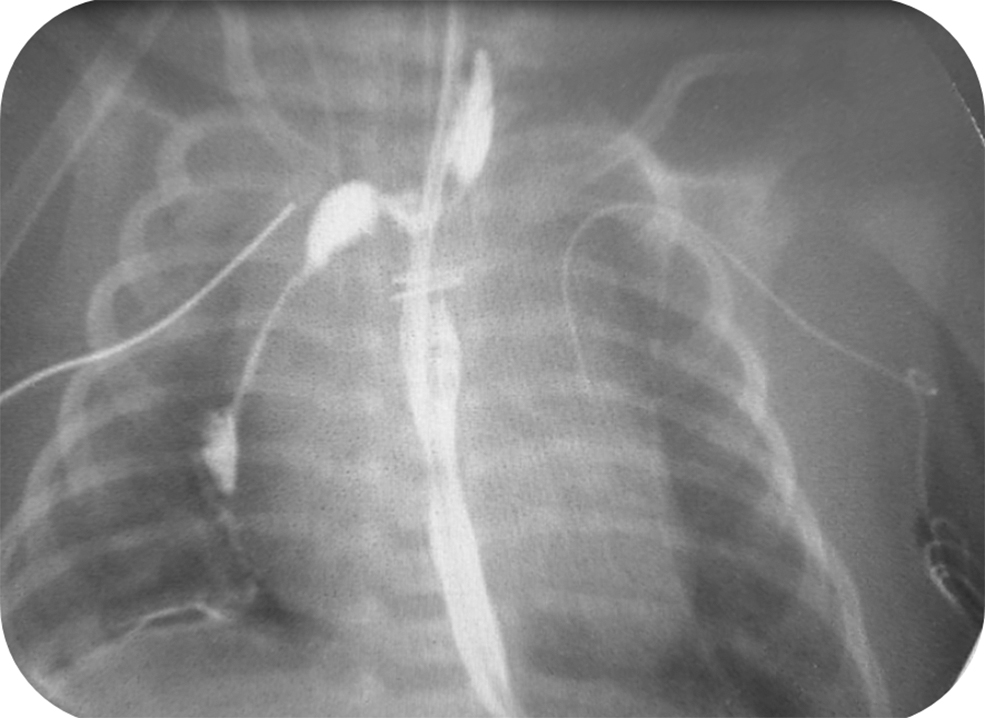
Esophagogram with a leak on day 2 after primary repair on patient 2.

Pneumothorax on day 5 on patient 3.
Discussion
Historically, management of an anastomosis leak has been conservative and nonoperative, with the use of a chest tube, parenteral nutrition, and broad-spectrum antibiotics. 5 It is presumed that there is a higher risk of stricture 6 and also a higher risk of a second anastomotic leak or further disruption of the esophageal anastomosis if an early attempt at operative repair of the leak is undertaken. Our goal was to reduce time until full feed and to minimize the percentage of stenosis in patients resolving spontaneously.
In 2015, Askarpour et al. showed that utilizing a double layer anastomotic technique and the use of blood transfusions are risk factors associated with an anastomotic leak. 6 In another report, the type of atresia and the gap length were not significantly associated with a leak. 7 Chittmittrapap and Spitz also demonstrated a higher risk of stricture in patients following an anastomotic leak operated on by an open approach. 7 In this report, 71% of the patients with a leak who were managed conservatively developed some grade of an anastomotic stricture. In another report, Zhao et al. compared two groups with and without an anastomotic leak: 29% of the patients with a leak developed an anastomotic stricture, while 11% of the cases without a leak developed an anastomotic stricture. 5 Nevertheless, in this report, the percentage of patients who underwent esophageal dilation was not significantly different between the two groups.
In the multi-institutional study authored by Holcomb et al., there was a 7.7% incidence of an anastomotic leak and 31.7% incidence of patients who required at least one dilation in this series. However, the report did not mention how many of the patients requiring a dilatation also had an anastomotic leak. 4 In our small series, half of the patients developed an esophageal stricture in the long-term follow-up, and these strictures were managed by esophageal dilation with good results.
Regarding nutrition, in the report by Zhao et al., the authors showed an average of 11.7 ± 4.08 days of intravenous nutritional support in the patients who were treated nonoperatively. This means that the patients did not start oral feeding until almost 12 days after their initial operation with increased hospitalization and total cost. In our study, the mean time to complete oral feeding was 10 days. Even though there is cost associated with a second operation, it allowed our patients to start feeding earlier with less days of parenteral nutrition and chest tube and resulted in a shorter hospital stay.
In a case series of 21 patients, Zhu et al. described patients who were reoperated on with an open approach, somewhere between 3 and 6 months after their first operation. 8 Only one of their patients had an anastomotic leak out of 16 patients who underwent a reoperation (the other patients had anastomotic strictures or recurrent TEF). In this patient, the baby was managed nonoperatively with good success, and the leak resolved without known complications.
In our limited experience with these four patients, we found that the dissection can be difficult because of inflamed tissues and adhesions, but the esophagus itself was not compromised in any infant. None of them developed another anastomotic leak, but two patients required dilations because of stricture. The size of the esophageal disruption was not directly proportional to the state of the patient. Even though large disruptions were found in all of them, the patients were not unstable. They probably benefited from an early reoperation, avoiding a leakage for a long time in the mediastinum and, therefore, mediastinitis, sepsis, or posterior stenosis.
The early re-suture of the leaking zone is a change in paradigm because it offers the benefits of preservation of the native esophagus, early resumption of enteral feedings, and shortening the length of parental nutrition and hospitalization.
Footnotes
Disclaimer
This study was approved by the institution investigation and ethics committee.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.