
Abstract
Background:
A double-pigtail ureteral stent (DPUS) can cause untoward symptoms, such as urgency, frequency, urinary incontinence, hematuria, and body pain that are bothersome to patient's quality of life (QoL). By reducing the quantity of material in the bladder, it could be reasonable to decrease stent-related symptoms (SRSs). We aimed to evaluate the tolerability of single pigtail suture stent (SPSS) with a validated questionnaire after uncomplicated retrograde semirigid ureteroscopic lithotripsy (URSL).
Materials and Methods
: A total of 130 patients who underwent ureteral stent placement after URSL for unilateral symptomatic ureteral stones with <15 mm diameter were randomized prospectively into two groups. Polyurethane ureteral stent (6 Fr, 24 or 26 cm) was placed in all patients, which was removed postoperatively with a mean of 14 days. There were 65 patients in both groups. All subjects completed the ureteral stent symptoms questionnaire (USSQ), which explores the SRSs. The questionnaires were conducted on the day of stent removal (at week 2) with the stent in situ and 4 weeks after removal (at week 6, poststent). The severity of SRSs and QoL were compared between the two groups.
Results:
SPSS was associated with perfect effect on all domains of USSQ, except from sexual and general health index scores. Pain index scores, visual analog scores (VAS), and analgesic requirements in SPSS group were found significantly low compared with those in the DPUS group. The QoL scores were significantly better in patients indwelling SPSS.
Conclusion:
SPSS is a potentially beneficial option to minimize ureteral SRSs after uncomplicated URSL.
Introduction
Double-pigtail ureteral stents (DPUSs) are commonly used as a basic part of many urological surgeries to alleviate or prevent ureteral obstruction. Despite their many advantages, they are often related with irritating lower urinary tract symptoms (LUTS), hematuria, bladder, and flank or abdominal pain, which might have a negative effect on patients' quality of life (QoL) and sexual health.1,2 The most common complaints after ureteroscopic lithotripsy (URSL) are associated with stents left in place postoperatively. These symptoms caused by placement of ureteral stent have been associated with the local irritation of the distal end of the stent and subsequent bladder and lower ureteral spasms. 3 However, the perfect ureteral stent has not been designed yet. 4
Joshi et al. reported that 78% of patients with DPUSs had disturbing urinary symptoms. More than 80% had pain that affected their daily lives, 58% reported reduced work performance, and 32% reported sexual dysfunction. 1 So far, many medical agents have been tested, such as selective alpha-1 blockers, anticholinergics, analgesics, and botulinum toxin type A to relieve these discomforts, and the results were encouraging.5,6 All these treatments to reduce morbidity should be considered as a palliative approach, and besides that they might cause some other serious side effects.
The main stent-related symptoms (SRSs) are caused by the presence of the pigtail in the bladder and vesicoureteral reflux (VUR). 7 Changes in the form, size, and composition of stents are thought to be reducing stent discomfort. 6 So, we sought safe and suitable solutions to improve SRSs. By reducing the quantity of material within the bladder, it could be reasonable to decrease SRSs. 3 Therefore, we manually developed a single pigtail suture stent (SPSS) from a polyurethane DPUS as a means of decreasing SRSs and improving QoL in patients with indwelling ureteral stents.
In this prospective randomized double-blind study, the effectiveness of the SPSS on SRSs was studied by using a specific questionnaire. To the best of our knowledge, this study is the first to evaluate the tolerance of SPSS with a validated ureteral stent symptoms questionnaire (USSQ) after uncomplicated URSL.
Materials and Methods
This study has been approved by the Ondokuz Mayis University Medical Research Ethics Committee (OMU KAEK 2016/363). Between June 2017 and September 2019, we prospectively included 130 consecutive patients (88 men and 42 women) with unilateral ureteral stone after acquiring informed consent form. All patients with symptomatic unilateral ureteral stones with <15 mm diameter who underwent uncomplicated retrograde semirigid URSL were randomly divided into two groups. There were 65 patients in the standard DPUS group (46 males and 19 females) (mean age 37 years), who were indwelled at the end of the URSL. The SPSS group also included 65 patients (42 males and 23 females) (mean age 38 years) in whom these stents were placed in a similar manner. A sample size of 65 patients in each group was calculated based on the results of previous studies on stents at a significance level of 0.05 and a power of 80%.
Patients aged between 18–60 years were included to this study. The exclusion criteria included (1) patients with bilateral ureteral stent insertion, bilateral ureteral or kidney stones; (2) concomitant renal or residual calculi on the postoperative kidney–ureter–bladder (KUB) film and urinary ultrasonography; (3) history of ureteral stent placement in the past 6 months; (4) patients with bleeding diathesis, congenital urinary abnormality; (5) patients with other diseases that causes LUTS, including prostate disease (benign prostatic hyperplasia, chronic prostatitis), urogenital system tumor, neurogenic bladder, ureteral obstruction, overactive bladder, interstitial cystitis, chronic pelvic pain syndrome, pregnancy, pelvic irradiation, diabetes, and recurrent urinary tract infection; (6) concomitant medication with alpha-blockers, 5-alfa reductase inhibitors, PDE5 inhibitors, anticholinergics or analgesics drugs; and (7) patients not available for follow-up.
The lower ureteral part of the conventional DPUS was sectioned perpendicularly to the main axis that includes 2 cm straight part and modified by two threads of synthetic nonabsorbable silicone coated surgical sutures made of polyester (PTFE), (Politer®, Dogsan, Turkey) to reduce irritation of the bladder and distal ureter. The tail of the SPSS was formed of two sutures and knots were tied at the sectioned edge. Only the renal pigtail and ureteral parts of the stent were preserved and elongated with a thin tail-shaped thread ending in knitted two sutures that prevents proximal migration and aids stent removal (Fig. 1). The replacement of distal loop with extraction thread at the vesical end resulted in the presence of only small amounts of suture in the bladder. Our suggested method is a possible way to minimize the irritation and VUR, and potentially to reduce SRSs.
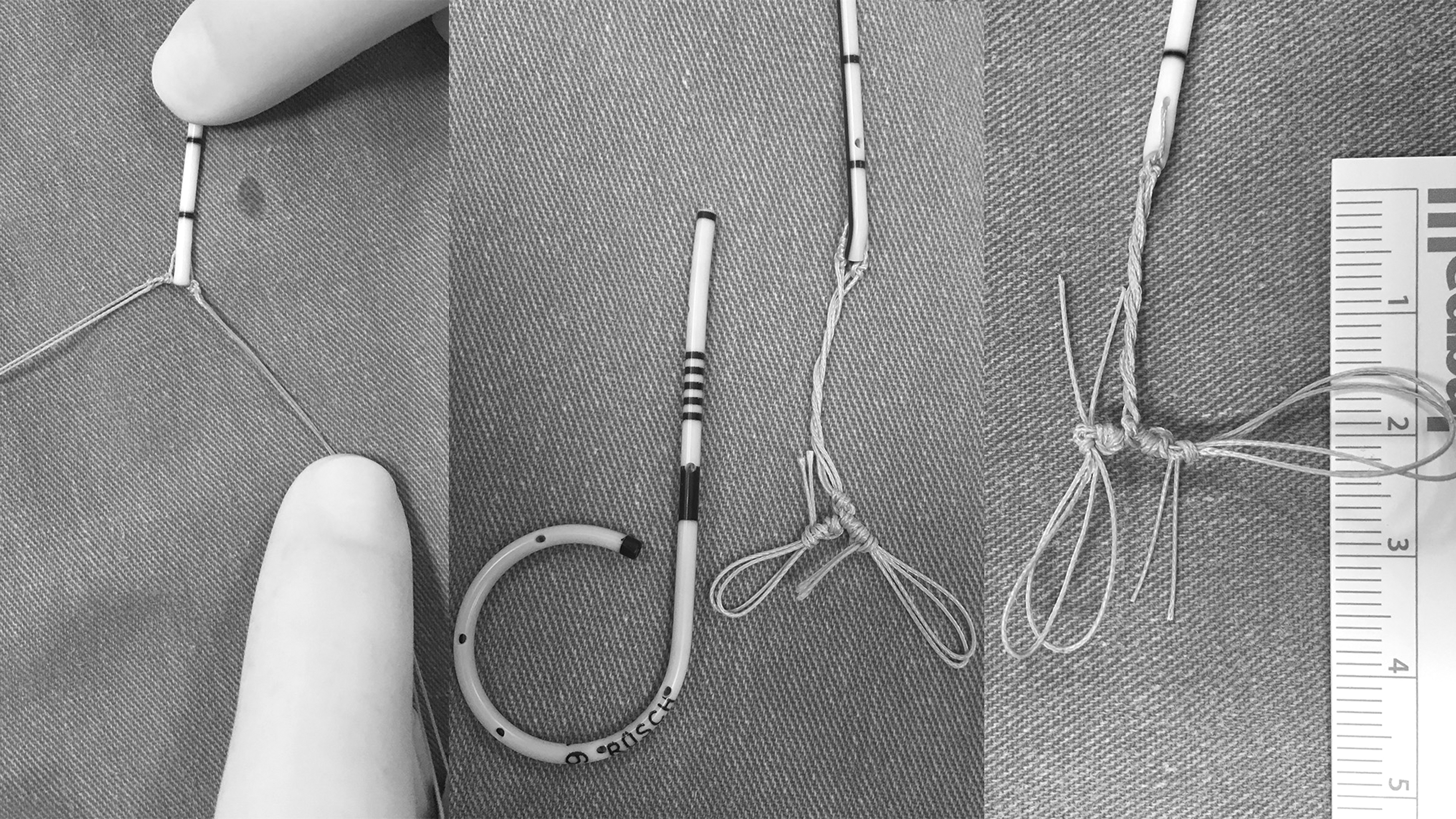
Preparation of the SPSS. SPSS, single pigtail suture stent.
All patients with a negative preoperative urine culture received a single dose antibiotic prophylaxis (Cefazolin 1 g, iv) during the induction of anesthesia. Surgery was performed under general anesthesia. The stones were disintegrated by a 4.5 Fr semirigid ureteroscope (Richard Wolf, Knittlingen, Germany) with a 30 W (5–10 Hz and 0.5–1.0 J) Holmium–YAG laser.
All stents were inserted retrogradely through a guidewire under fluoroscopic control at the end of the URSL. The ureteral stent was composed of polyurethane material (Integral Rusch, Teleflex Medical), and its diameter was 6 Fr; the lengths were 24 cm or 26 cm. Ureteral stent length was selected according to the body height of the patients. No patient had any complications from the procedure.
Urethral catheters were removed from all patients on the day after URSL and then the patients were discharged. During the ureteral stent indwelling time, analgesic intake was standardized with diclofenac potassium 50 mg when required, up to three times per day.
A plain X-ray of KUB (Fig. 2) and urinary ultrasonography were performed in all patients on the day of stent removal to confirm the position of stent and the stone-free status. The stents were removed under local anesthesia, 2 weeks after the surgery, by a flexible cystoscopy with the aid of forceps. The extraction thread at the vesical end could facilitate stent removal in the SPSS group (Fig. 3).

KUB film shows SPSS. KUB, kidney, ureter, and bladder; SPSS, single pigtail suture stent.
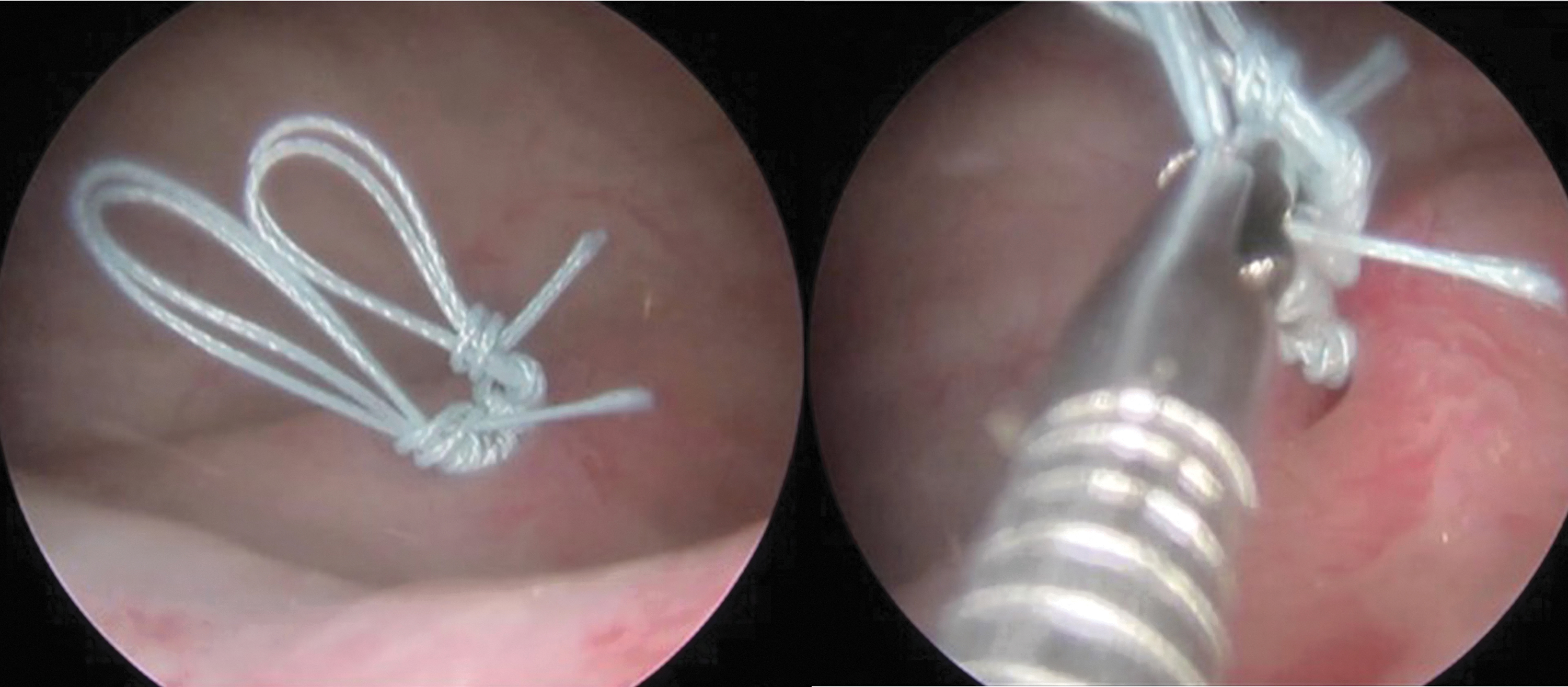
Cystoscopic removal of the SPSS. SPSS, single pigtail suture stent.
Joshi et al. presented USSQ, which consists of six different sections to explore urinary symptoms, body pain, general health, work performance, sexual dysfunction, additional problems, and general satisfaction. Each domain has several questions. The scores of answers per domain are picked up to determine an index score, and high score means more bothersome. 8 Turkish translation of the validated USSQ was used for the assessment of SRSs and their impact on patients' QoL. 9 All patients were requested to complete the USSQ in outpatient clinics to evaluate their symptoms on the day of stent removal (week 2) with the stent in situ. Four weeks after stent removal (week 6, poststent), we utilized a brief form of USSQ, which included only urinary section (U1–U11). We hoped that symptoms would have been fully resolved in 4 weeks after stent removal. Thus, answers to poststent questionnaire about the urinary symptoms that patients have experienced were proposed to be the baseline data.
All questionnaires were conducted and assessed by a single physician, who did not participate in any of these surgeries. Both physician and patients were unaware of distribution of patients. Consumption of any other drugs, overall analgesic intake, significant complications, and readmissions due to stent-related complications were recorded in each group and each group's W2 and W6 scores were compared.
Statistical analysis
The data were analyzed using IBM SPSS Statistics for Windows, Version 21.0 (IBM Corp., Armonk, NY). Data are expressed as n (%) or mean ± standard deviation. Continuous data were compared with independent sample t test when normally distributed or Mann–Whitney U test when not normally distributed. Categorical data were compared with chi-square test. Significance of the statistical tests was set at P value <.05.
Results
Totally 130 patients were included in the study (88 men and 42 women, 65 in each group). The mean age was 37.8 years. The baseline patient characteristics are listed in Table 1. Regarding age, gender, anthropometric measurements, stone sizes, stone location, and operative times, statistically significant differences did not exist between the groups (P > .05).
Patients' Demographic and Operative Details
BMI, body mass index; SPSS, single pigtail suture stent.
Poststent period urinary index scores (at W6), which were considered as the baseline characteristics for urinary symptoms, were not statistically significant among the two groups. Comparison of mean urinary symptom scores before and after stent removal showed significant decrease in all domains for both groups (P < .05).
The overall ureteral stent symptom score results are listed in Table 2 for both groups. SPSS has greatly reduced SRSs. Almost all of ureteral stent symptom scores other than sexual and general health index scores showed significantly lower scores in SPSS than in DPUS. The analysis of the questionnaire at W2 revealed a significant difference in urinary index score (24.2 versus 19.3, P < .01), pain index score (19.6 versus 14.8, P = .02), work performance score (8.4 versus 6.3, P = .01), and QoL scores (4.0 versus 3.2, P < .01) between the two groups. We found that visual analog scores (VAS) scores were favoring the SPSS group (3.7 versus 1.7, P < .01). Also mean analgesic consumption was significantly less in SPSS group as compared with standard DPUS group (15.7 versus 8.9, P < .01). SPSS group showed a numerical decrease in sexual and general health scores and there was a trend favoring SPSS use, but they were not statistically significant (6.4 versus 5.9, P = .07 and 14.5 versus 12.7, P = .09, respectively).
Ureteral Stent Symptom Scores
Bold indicates values that are statistically significant, p < 0.05.
QoL, quality of life; VAS, visual analog scores.
During stent removal, one of the SPSSs had to be withdrawn under ureteroscopy, because the thread had migrated into the ureter. In this case, it was easy to remove the stent through the ureter without the need for further enlargement of ureteral orifice. We observed a clear dilation of the distal ureteral orifice without inflammation around the sutures. In all patients, the SPSS provided effective renal drainage. In 1 case, lower ureteral part of the SPPS migrated into the bladder. None of the ureteral stents migrated into the urethra in any of the patients.
Five patients (2 SPSS, 3 DPUS group) developed single attack of febrile urinary tract infection requiring antibiotic therapy, 3 patients were admitted to hospital due to flank pain (all were patients with DPUS) and 1 patient (with DPUS) came to the emergency room for gross hematuria during the study period.
The reported additional problems, such as urinary system infection, need to take antibiotic, or seek medical assistance, were similar between the two groups. Stent extraction threads did not result in increased number of infections (P > .05).
Discussion
Ureteral stent placement is an essential part of many urologic surgeries particularly in endourology practice. Although it has been stated in some studies that ureteral stent use is redundant after uncomplicated URSL, 10 in this study, we routinely placed ureteral stent as a kind of insurance toward possible complications such as development of hydronephrosis and renal colic. Ureteral stents assist the urine flow continuation by keeping the passage open in the ureter in which it is placed. Together with multiple benefits, stents may cause severe morbidities even though they are properly placed in the right size. SRSs and complications may develop in many patients. Severity of ureteral SRSs may change specific to patient; however, it is believed that it affects 80% of patients in different severity levels. 11 These undesired side effects and complications could cause negative impacts on patients' QoL, work performance, and sexual life, 1 and even sometimes, these symptoms could require early removal of stent. 12 Side effects related to DPUS and patient morbidity are assumed as potential health problems.1,13
The relationship between stent characteristics such as size, material, softness, position, and loop completeness and the SRSs has been investigated with the aim of reducing SRSs, but to date evidence remains conflicting.4,14,15 If it is possible to use suitable sized stents in patients, distal migration of stent and consequently SRSs could be decreased. 16 It seems that short bladder loops are more favorable than long loops that extend throughout the bladder.3,7 So, we thought that it is necessary to minimize the amount of material in the bladder to decrease SRSs. More material in the bladder that would lead to more symptoms was supported by previous studies. A different design was introduced in the tail stent model with a 7Fr proximal pigtail and 7Fr shaft that tapers to a lumenless straight 3Fr tail that lies in the bladder. Dunn et al. showed that the 7Fr tail stent produced significantly less overall irritative voiding symptoms than standard 7Fr DPUS. 17 Lingeman et al. described SRSs for various types of ureteral stents. The short loop type ureteral stents showed lower SRS scores than long loop type ureteral stents and standard DPUSs. 3 Vogt et al. replaced the lower part of a DPUS with a 0.3-Fr suture. They reported significant decreases in urinary symptoms. 18
Multiple theories have been suggested but the exact etiology of these SRSs is still not clear. One possible theory is lower ureteral smooth muscle spasms and local irritation to neuronal-rich trigonal mucosa by the intravesical portion of the stent and body pain, related with urine reflux from the bladder to the kidney that leads to an excessive rise in intrapelvic pressure, especially triggered during voiding. 19 Chew et al. reported that changes in body position cause mobility of distal edge of DPUS in bladder and this could result in local tissue irritation and load on SRSs. 20 It has been thought that gross hematuria could be closely related to stent friction in the collecting system because of physical activity. However, low urine volume and retrograde pressure caused by stent-related excessive and steady spasm in ureter have also been associated with hematuria development. 21 Although there has been no macroscopic hematuria development observed in the SPSS group of the study, in the DPUS group, macroscopic hematuria was reported in 4 patients and 1 patient was admitted to the emergency room with macroscopic hematuria. We believe that nonexistence of local irritation, persistence ureteral spasm, and reflux, which exist in the DPUS group, in the SPSS group is effective on those results.
In this study, it was hypothesized that reduced LUTS should occur with less material in the bladder. Indeed, all of ureteral stent symptom scores other than sexual and general health index scores were significantly lower in the SPSS group than the standard DPUS group. It is reasonable that SPSS improves the SRSs by alleviating bladder and ureteral spasm and VUR. 21
General and sexual health may be affected by the URSL. Morbidity, hospitalization, and lost work hours associated with these procedures can negatively affect the health-related QoL of the patients.22,23 Joshi et al. have identified sexual dysfunction in stented patients as a result of decreased level of self-confidence and libido and this has been associated with urinary system symptoms and pains occurring because of DPUS existence. 24 The SPSS group showed a numerical decrease in sexual and general health scores and there was a trend favoring SPSS use, but they were not statistically significant (6.4 versus 5.9, P = .07 and 14.5 versus 12.7, P = .09 respectively). Standard DPUS group patients were less able to carry out physical exercises and had discomfort during sex, which reduced their overall satisfaction. The decrease in urinary symptoms and associated pain in patients with SPSS might explain for better sexual and general health scores.
In normal healthy ureters, urine generally passes in between the ureter wall and the stent and rarely through the holes of the stent. It seems that bladder loop does not have a role in urine drainage. 25 DPUSs bypass intravesical sphincter resulting in renal reflux and flank pain during micturition. The replacement of bottom of the stent with a tail-shaped thread, resulting in the absence of an internal channel, potentially reduces the incidence of renal reflux and subsequent flank pain. Thus, stent tolerance might be improved. In addition to flank pain, abdominal pain and urethral pain could negatively affect the QoL. 21 In our study, pain index scores, VAS, and analgesic requirements in the SPSS group were found significantly low compared with the DPUS group. The QoL scores were significantly better in patients with indwelling SPSS.
Despite the significant symptom improvement with SPSS, statistically significant decrease in urinary symptom scores was observed in both groups after removing the stent. So, to decrease the morbidity, stenting period should be kept as short as possible,18,26 even the stent is SPSS. Thanks to the ongoing studies in this field, new developments in ureteral stent design are promising for patients with stent.4,14,19
The limitations of our study are as follows. First, the present series included a well-selected cohort of patients undergoing uncomplicated URSL. However, ureteroscopic surgery has its own inevitable traumatic effects on urinary system and primarily on ureter. Complicated URSLs will also be responsible for the LUTS. 21 As this situation might alter the efficacy of SPSS in complicated cases, we have only included uncomplicated URSL cases into our study. Second, this study includes relatively smaller sample size.
Conclusion
Currently, there is no ideal stent that does not cause complications. SPSS is a cheap easy solution that can be prepared in operating rooms in minutes for relieving SRSs with improved QoL and less requirement of analgesic. We may speculate that design of SPSS prevents trigonal and lower ureteral irritation and decreases VUR. There is need for further studies and developments on new stent designs, materials, and treatment strategies to decrease SRSs, and our findings should be confirmed in larger populations.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.