
Abstract
Background:
Although inguinal hernia occurs frequently after radical prostatectomy, transabdominal preperitoneal (TAPP) inguinal hernia repair occasionally poses challenges due to fibrosis of the preperitoneal cavity. In patients with severe intrapelvic fibrosis, we have adopted a modified intraperitoneal onlay mesh (IPOM) technique. The surgical factors were compared between patients who underwent modified IPOM and those who underwent TAPP for inguinal hernia repair.
Materials and Methods:
In total, 57 patients underwent laparoscopic surgery for inguinal hernias after radical prostatectomy between February 2013 and January 2020. TAPP was successfully completed in 44 patients, whereas 13 patients underwent modified IPOM converted from TAPP. The surgical results were retrospectively compared.
Results:
The median follow-up duration was 36.0 months (range, 1–84 months). Intraoperative complications, recurrence of hernia, and chronic pain were not observed in both groups. The average duration of surgery in the modified IPOM group was longer than that in the TAPP group (137 versus 107 minutes, P < .05). There was no significant difference in the incidence of the inguinal-related complications such as inguinal pain or inguinal swelling.
Conclusions:
Postoperative complications including recurrence of hernia after modified IPOM are comparable to those after TAPP hernia repair. Modified IPOM repair is a surgical option for repairing inguinal hernias following radical prostatectomy.
Introduction
Inguinal hernia is a common complication after radical prostatectomy. 1 The strong adhesion of the Retzius' space makes conventional laparoscopic procedures, that is, transabdominal preperitoneal (TAPP) inguinal hernia repair after radical prostatectomy, difficult. Hernia Surgery and European Hernia Society guidelines recommend the open anterior repair approach in such cases.2,3 The International Endohernia Society and the European Association for Endoscopic Surgery guidelines recommend that laparoscopic surgery should be performed by skilled surgeons.4–6 At our institution, the TAPP procedure has been applied for inguinal hernia repair subsequent to radical prostatectomy. 6 However, TAPP repair was not feasible in patients with strong adhesions. Although modified intraperitoneal onlay mesh repair (IPOM) could be indicated in such difficult cases, IPOM was deemed inferior to TAPP mainly because of a higher recurrence rate.7–9 A modified IPOM could be considered as an alternative technique to reduce the recurrence rate. There have been no reports of modified IPOM in patients in whom laparoscopic surgery was difficult to complete due to severe adhesion after radical prostatectomy. We herein report the surgical procedures and the results of 13 patients who underwent modified IPOM due to difficulty in performing TAPP successfully. We also compared patients who underwent modified IPOM with those who underwent TAPP.
Materials and Methods
Fifty-seven patients underwent inguinal hernia repair after radical prostatectomy between February 2013 and January 2020. Although TAPP was applied for hernia repair in all patients, TAPP was converted to the modified IPOM procedure if it became difficult to continue due to difficulties in dissection secondary to fibrosis of the Retzius space or peritoneal closure. Finally, 44 patients underwent TAPP repair and the remaining 13 underwent modified IPOM repair. The surgical outcomes and incidence of complications were compared between the two groups. Surgical endpoints included the assessment of the duration of surgery, volume of blood loss, and intraoperative complications. Early postoperative complications were assessed by pain, discomfort, and swelling in the surgical site at the first visit after discharge (2–3 weeks postsurgery). Late postoperative complications were evaluated by recurrence, chronic pain, discomfort, and the presence or absence of inguinal swelling at 6 months or later postsurgery. Three surgeons with technological certifications from the Japan Society for Endoscopic Surgery performed the surgeries in both groups. StatMate Version 4.01 was used for statistical analyses. The Welch test and the t-test were used to compare average values, whereas the chi-square test was used to compare complication rates.
Surgical procedures of modified IPOM
When performing modified IPOM, the following two points are important. First, the abdominal wall is exposed and the mesh is fixed directly to the exposed abdominal wall, with the exception of areas where peritoneal dissection is difficult. Cooper's ligaments should always be exposed to allow the mesh to be fixed to the ligament with tackers (Fig. 1). In areas where peritoneal dissection is difficult, tacker fixation is performed over the peritoneum (Fig. 2). If mesh migration is a concern, full-layer fixation can be added using nonabsorbable thread.

Cooper's ligaments should be always exposed to allow the mesh to be fixed to the ligament with tackers.
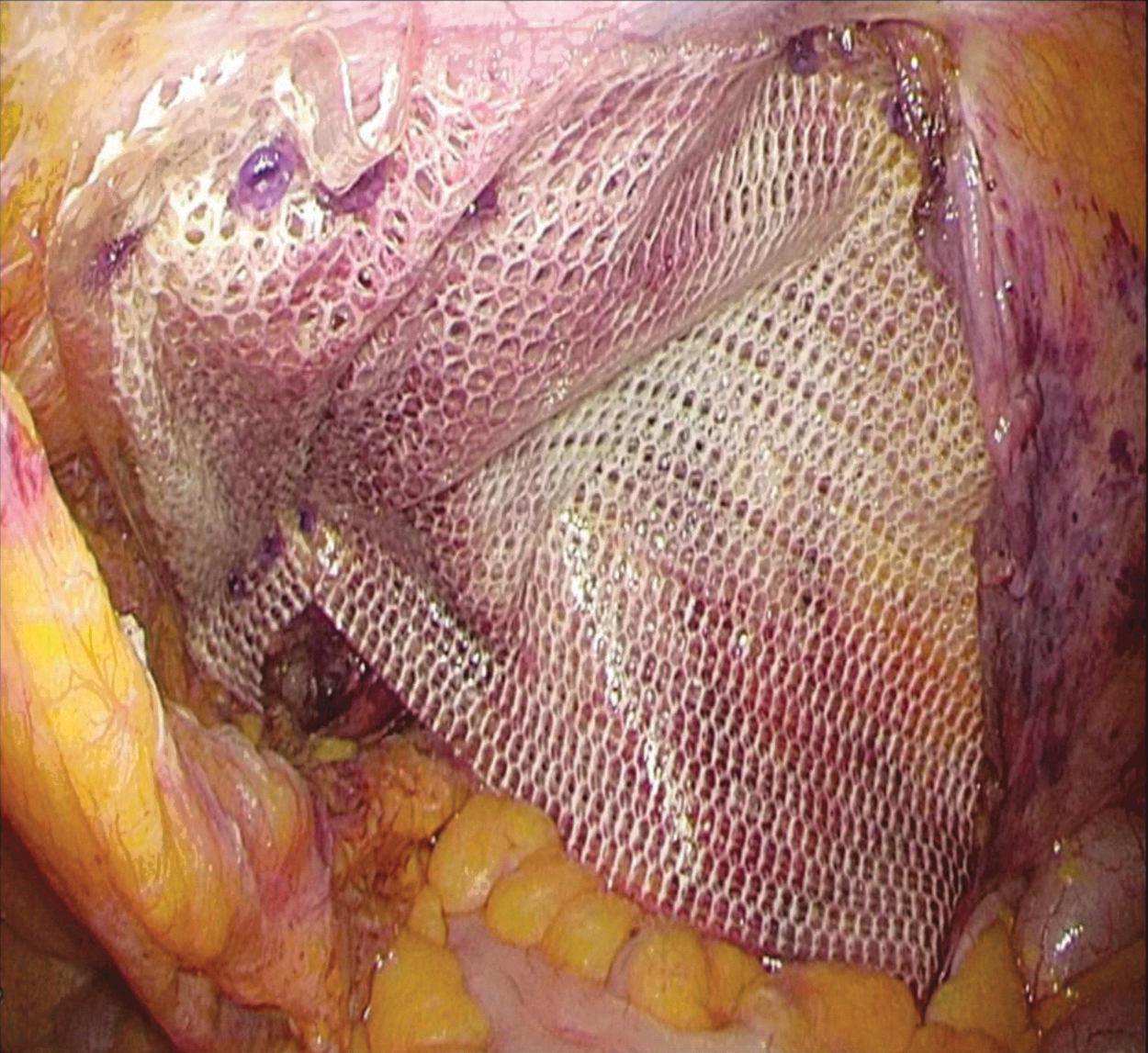
In areas where peritoneal dissection is difficult, tacker fixation is performed over the peritoneum.
Second, the peritoneum is closed for preventing internal hernias. If the peritoneum cannot be completely closed, care should be taken to avoid causing internal hernias. If the upper and lower peritoneal borders cannot be bound together, the upper and lower peritoneum can be fixed to the indwelt mesh to break the continuity between the peritoneal cavity and the preperitoneal space and to prevent the intestine in the peritoneal cavity from entering the preperitoneal space. Because the peritoneum will be sutured to the coated surface of the mesh, nonabsorbable suture is used (Fig. 3).
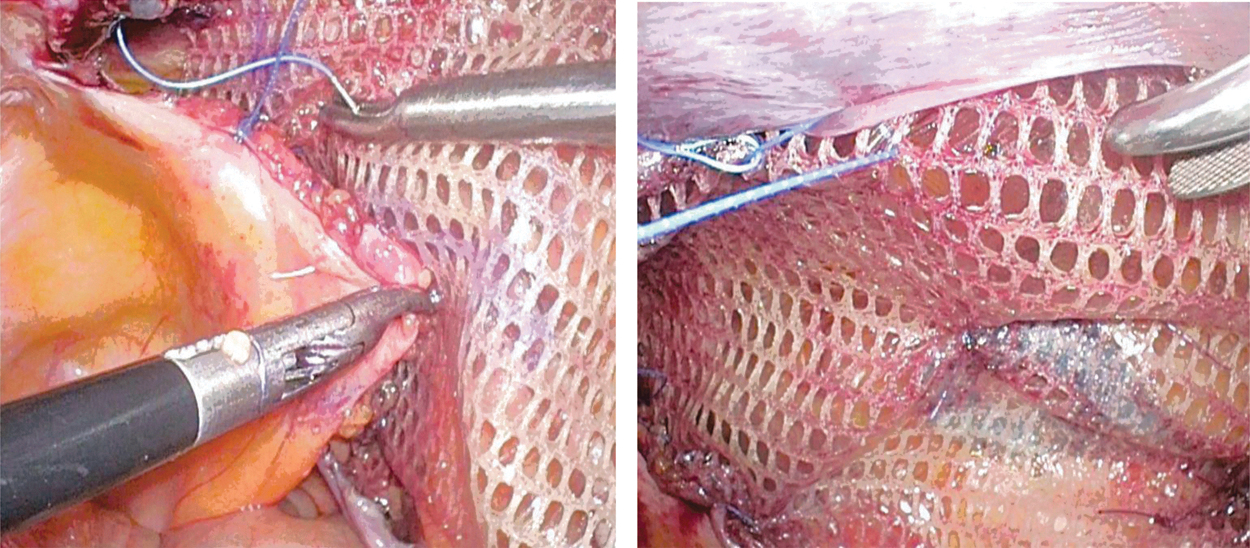
If the upper and lower peritoneal borders cannot be bound together, the upper and lower peritoneum can be fixed to the indwelt mesh to prevent the intestine from entering the preperitoneal space.
The mesh used is a mesh with collagen film (Symbotex mesh or Optimized PCO mesh; MEDTRONIC Japan Co., Ltd., Tokyo, Japan).
Results
The characteristics of the 13 patients who underwent modified IPOM are summarized in Table 1. Twelve patients had unilateral disease, whereas 1 patient had bilateral disease. Regarding the types of hernias, 11 had indirect hernias, 1 had a direct hernia, and 1 had a combination of both types. Five patients underwent retropubic radical prostatectomy, whereas 8 patients underwent robot-assisted laparoscopic radical prostatectomy. Table 2 shows preoperative demographic characteristics of the two groups. There were no differences in patient background factors, such as age, body mass index, laterality, hernia type, and the type of prostate cancer surgery between the modified IPOM and TAPP groups. Table 3 shows the surgical results of the two groups. A larger (15 × 10 cm) collagen mesh was used in the modified IPOM group. The average duration of surgery in the modified IPOM group was 138 minutes (only unilateral patients), which was significantly longer than that in the TAPP group (107 minutes; P < .05). Intraoperative complications such as organ and vascular injuries were not observed in both groups. Table 4 revealed early and late complications in the two groups. There was no significant difference in the incidence of early postoperative pain and inguinal swelling between the two groups. Only 1 patient in the TAPP group complained of inguinal region discomfort at 6 months or later after the surgery. However, there were no other late postoperative complications such as inguinal pain or swelling in both groups (Table 4).
Patient and Hernia Characteristics (n = 13)
ASA-PS, American Society of Anesthesiologists physical status; BMI, body mass index; RALP, robot-assisted laparoscopic radical prostatectomy (transperitoneal); RRP, retropubic radical prostatectomy (transperitoneal).
Preoperative Demography of the Two Groups
Welch test; bt-test; cchi-squared test.
ASA-PS, American Society of Anesthesiologists physical status; BMI, body mass index; IOPM, intraperitoneal onlay mesh repair; RALP, robot-assisted laparoscopic radical prostatectomy (transperitoneal); RRP, retropubic radical prostatectomy (transperitoneal); TAPP, transabdominal preperitoneal inguinal hernia repair; n.s., not significant.
Comparison of Surgical Results Between the Two Groups
Operation time: patient who underwent bilateral hernia repair was excluded.
t-Test; bWelch test; cchi-squared test.
IOPM, intraperitoneal onlay mesh repair; TAPP, transabdominal preperitoneal inguinal hernia repair; n.s., not significant.
Comparison of Early and Late Complications Between the Two Groups
Chi-squared test.
IOPM, intraperitoneal onlay mesh repair; TAPP, transabdominal preperitoneal inguinal hernia repair; n.s., not significant.
Discussion
The present study clearly showed that modified IPOM was useful when TAPP was difficult to continue due to severe adhesion. The decision to use modified IPOM was made after an exploratory incision into the preperitoneal space revealed substantial fibrosis, making proper dissection of the posterior inguinal wall difficult and thereby reperitonization questionable. Although the open anterior approach is an alternative method, it is not easy to convert to an open anterior approach after peritoneal incision or if peritoneal dissection is performed widely. Moreover, performing the procedure on both the anterior and posterior layers is not a good option as it is very difficult to perform surgery if recurrence occurs. Consequently, we performed laparoscopic surgery via a modified IPOM approach in patients in whom TAPP repair was difficult to perform, thereby avoiding conversion to an open anterior approach.
The difference between the modified IPOM approach and the IPOM approach lies in the fixation of the mesh to the abdominal wall. In the modified IPOM approach, there is as much direct fixation as possible (not via the peritoneum) to the abdominal wall with tackers. Cooper's ligaments are always identified and exposed, and fixation of the mesh to Cooper's ligament is performed using tackers. When tackers are used for fixation through the peritoneum, full-layer abdominal wall fixation is employed using nonabsorbable thread if vulnerability of the fixation is suspected. In other words, modified IPOM adds the direct fixation of the abdominal wall with a tacker and the full-layer fixation of the abdominal wall using nonabsorbable thread to reduce the vulnerability of IPOM abdominal wall fixation.
Another concern regarding the modified IPOM approach is that the boundary between TAPP and IPOM may cause intestinal obstruction. To overcome this drawback, the boundary is closed with continuous sutures using nonabsorbable thread to the mesh surface.
Although no intraoperative complications were recognized in either the modified IPOM or the TAPP group, the duration of surgery was longer in the modified IPOM group than in the TAPP group. This may be because of the two following reasons.
First, the modified IPOM group included patients for whom there was great difficulty in successfully completing TAPP.
Second, it was difficult to standardize the modified IPOM procedure because there was a lot of diversity among the patients.
There were no differences in the incidence of postoperative pain and inguinal swelling between the two groups. Additionally, there were no instances of recurrence or chronic pain in both groups.
Hyllegaard and Friis-Andersen reported the surgical results of 37 patients with complicated inguinal hernias who underwent modified IPOM. In this report, 5% recurrence and 11% chronic pain was noted, which were similar or better than the results of the Liechtenstein method. 10
This study had several limitations. These include facts that the sample size was small, the observation period was short, it was a retrospective study, and the criteria for the use of modified IPOM were left up to the surgeon's discretion.
In conclusion, when TAPP is difficult for patients with inguinal hernias following radical prostatectomy, modified IPOM appears to be an alternative option to an open anterior approach. The postoperative complications following modified IPOM, including hernia recurrence, are comparable to those after TAPP.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.