
Abstract

Dear Editor:
D
Ischemia–reperfusion injury (IRI) is a damage caused by two different but inseparable successive events (ischemia and reperfusion).1–3 It subsequently causes cellular dysfunction death. 4 Ischemic changes are time dependent. IRI contributes to pathology not only by the presence of embolism or trombosis but also by wide range of conditions. 5 Laparoscopic surgeries cause IRI after insufflation and deflation phases acting as ischemia and reperfusion, respectively.2,3,6 Laparoscopic surgery can be regarded as an ischemia/reperfusion (I/R) model.2,7 So it is important to prevent and/or modulate the damage during each of these two phases.1,5 Although the purpose of ischemia is to prevent energy breakdown due to oxygen deprivation, the purpose of reperfusion is to prevent the oxidation process.1,4
The terminologies that cause confusion in the literature and the studies using these terminologies are tried to be summarized in the following figures.
“Precondition” is a phenomenon that has been first described by Murry et al. and shown in a dog heart. 8 By precondition (early classical preconditioning), blood flow to an organ or tissue is cessated for a short time (usually <5 minutes) and then restorated. By application of this method before I/R, tissue damage can be reduced.4,9–12
“Preconditioning” in laparoscopy (human or rat model) (Fig. 1).
“Preconditioning” in laparoscopy (human or rat model).
“Ischemic precondition(ing)” consists of brief and repetitive episodes of I/R, to increase tissue resistance against I/R damage. Its beneficial effects have been shown in experimental and clinical studies but clinical studies are very limited.3,4,9–11,14
“Ischemic preconditioning” in laparoscopy (human or rat model) (Fig. 2).
“Ischemic preconditioning” in laparoscopy (human or rat model).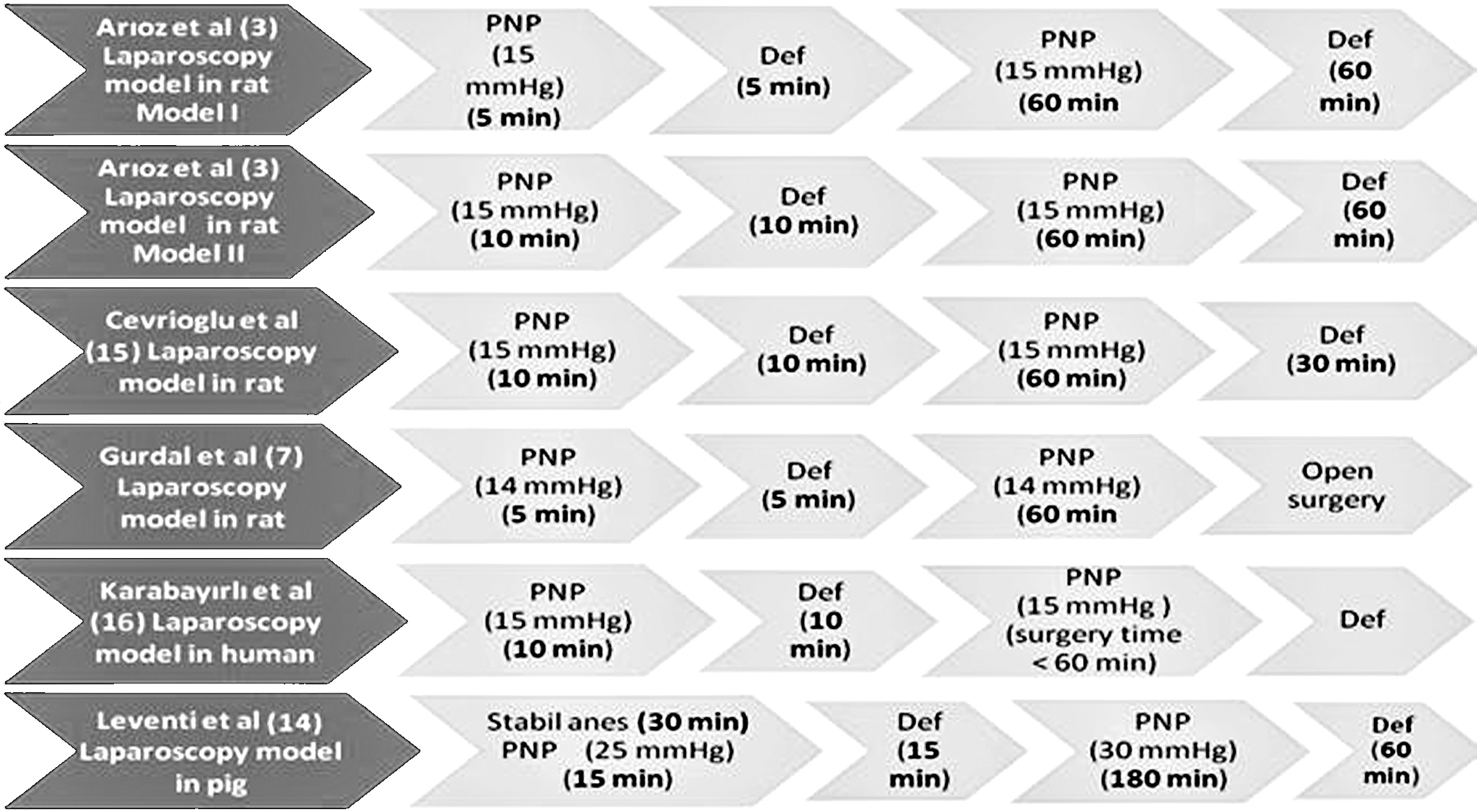
“Ischemic preconditioning” in superior mesenteric artery (Fig. 3).
“Ischemic preconditioning” in superior mesenteric artery.
Gurdal et al. 7 applied pneumoperitoneum in rat model before applying open surgery and named this method as “nonischemic preconditioning.”
“Nonischemic preconditioning” (Fig. 4).
“Nonischemic preconditioning.”
“Laparoscopic preconditioning” (LPre) is a technique that is performed at the beginning of laparoscopy by administrating short periods of insufflation and deflation sequence(s). 6
“Laparoscopic preconditioning” (Fig. 5).
“Laparoscopic preconditioning.”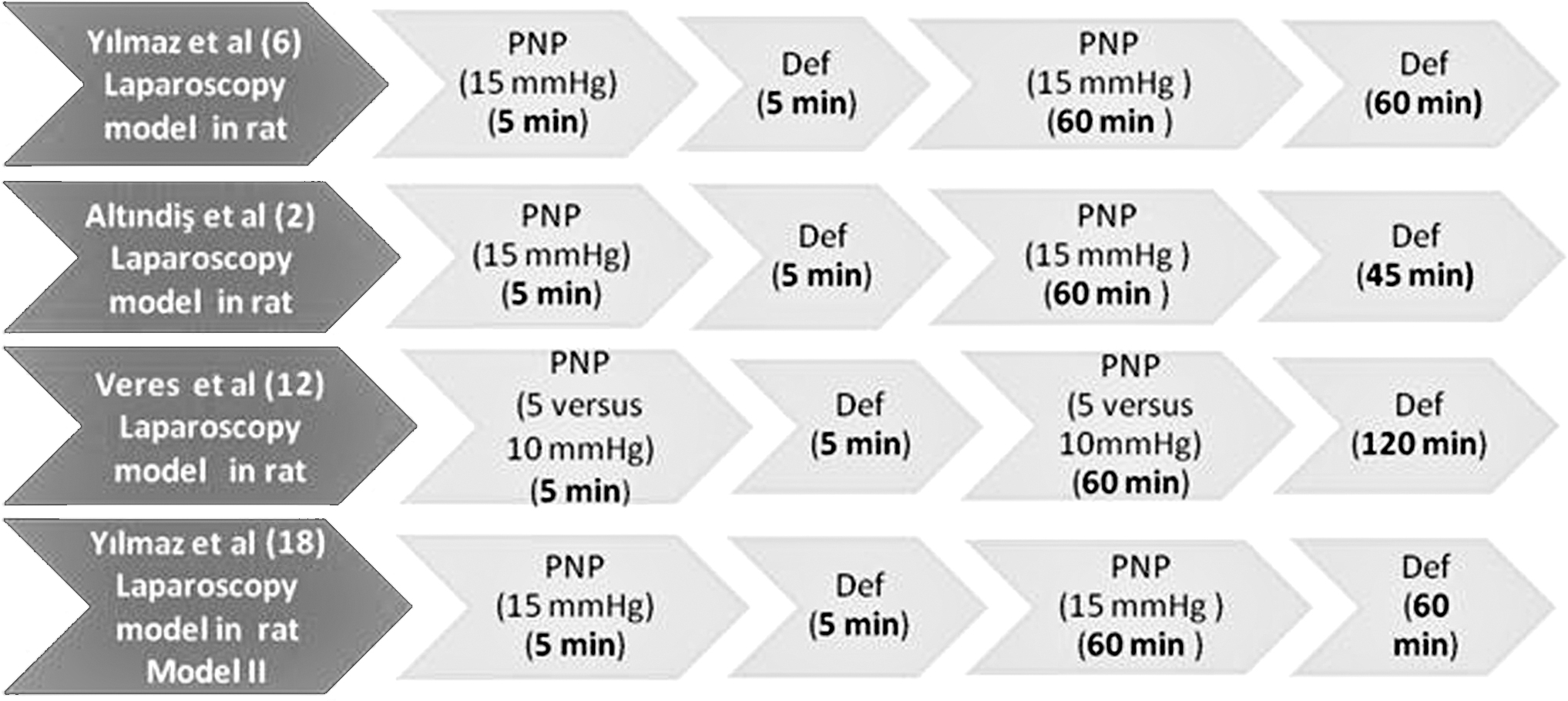
“Prelaparoscopy conditioning” (Fig. 6).
“Prelaparoscopy conditioning.”
Although “preconditioning,” “ischemic preconditioning,” “laparoscopic preconditioning,” and “prelaparoscopy conditioning” mean the same mechanism, the authors named them differently in clinical and experimental studies.
Recently “postcondition” has been reported as protective against I/R damage like precondition. 9 Then in 2003, Zhao et al. 19 introduced “Ischemic postcondition,” which was defined as short periods of ischemia and reperfusion in the early period of reperfusion after prolonged ischemia.4,9,10,12,19,20
“Postlaparoscopy conditioning” (Fig. 7).
“Postlaparoscopy conditioning.”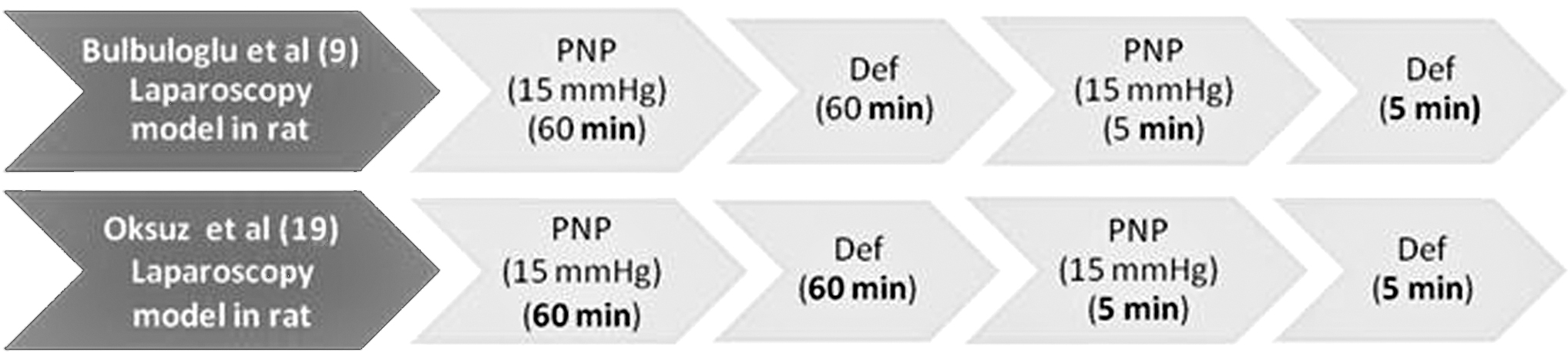
“Laparoscopic postconditioning” (Fig. 8).
“Laparoscopic postconditioning.”
The difference between researchers using “postlaparoscopy conditioning” and “laparoscopic postconditioning” terminologies is that the time permitted for reperfusion is different (60 minutes versus 5 minutes). The time that was permitted for reperfusion (deflation time) after pneumoperitoneum should be standardized to comment corretly between studies.
Recently in some studies, “ischemic postconditioning” was applied immediately after an ischemic phase subsequently before the permanent reperfusion occurs. The application was as one or more short cycles of reperfusion followed by one or more short cycles of ischemia. 17
“Ischemic postconditioning” in superior mesenteric artery (Fig. 9).
“Ischemic postconditioning” in superior mesenteric artery.
In previous studies, “ischemic postconditioning” was in the form of I/R model after reperfusion (5 minutes versus 60 minutes); in the studies of Chu et al. 10 and Liu et al. 17 (“immediately ischemic postconditioning” study), “ischemic postconditioning” was applied in the form of R/I model (reperfusion [30 seconds]/ischemia [30 seconds]) after long-term ischemia.
The model that Liu et al. 17 named as “delayed ischemic postconditioning” coincides with the terminologies of “postlaparoscopy conditioning” and “laparoscopic postconditioning.” The only difference between these studies is the time permitted for reperfusion after ischemia.
The confusion in terminology has been increased with the introduction of “postconditioning” terminology to the literature and the acceptance of laparoscopic surgery itself as an I/R model.
Although so many pre- and/or postconditioning procedures have been applied, there is still no ideal and standard model available to reduce laparoscopy-related IRI. 18 The experimental animals used in animal experiments are small and their anatomy is quite different from human anatomy. Therefore, it is difficult to accept their results in clinic applications. In contrast, clinical studies in the literature is very limited. We thought that further studies using common terminology and standards are needed to better discuss and interpret the results of the studies.
Footnotes
Disclosure Statement
No competing financial interests exist.