
Abstract
Achalasia is a primary esophageal motility disorder characterized by lack of esophageal peristalsis and partial or absent relaxation of the lower esophageal sphincter in response to swallowing. Available treatment modalities are not curative but rather intend to relieve patient' symptoms. A laparoscopic Heller myotomy with Dor fundoplication is associated with high clinical success rates and low incidence of postoperative reflux. A properly executed operation following critical surgical steps is key for the success of the operation.
Introduction
Achalasia is a primary esophageal motility disorder characterized by lack of esophageal peristalsis and partial or absent relaxation of the lower esophageal sphincter (LES) in response to swallowing. 1 The disease is characterized by a functional loss of inhibitory neurons of the esophageal myenteric plexus, which are needed for peristalsis of the esophageal body and relaxation of the tonic LES. 2 Patients often complain of dysphagia, regurgitation of undigested food, respiratory symptoms, chest pain, and/or weight loss. High-resolution manometry is currently the gold standard for diagnosing and classifying the disease. 3
Available treatment modalities are not curative but rather intend to relieve patient' symptoms by decreasing the LES pressure and improving the emptying of the esophagus into the stomach. Nonsurgical modalities include pharmacological therapy, endoscopic botulinum toxin injection, pneumatic dilatation, and peroral endoscopic myotomy. Surgical treatments include laparoscopic Heller myotomy (LHM) and esophagectomy. 4
Several studies have shown that LHM with a partial fundoplication is associated with high clinical success rates and low incidence of postoperative reflux.5–8 A properly executed operation following critical surgical steps is key for the success of the operation.
Preoperative Phase
A liquid diet is recommended at least 24 hours before the operation because achalasia patients are at risk of aspiration during the anesthetic induction. Anesthesiologists should be aware of this risk and take precautions when appropriate. The head of the bed must be elevated 30° until the airway is secured and a rapid sequence induction is recommended.
After safe endotracheal intubation, the patient is positioned supine in low lithotomy position over an inflated beanbag with the lower extremities extended on stirrups, with knees flexed 20°–30°. We strongly recommend usage of pneumatic compression stockings to reduce the risk of deep vein thrombosis. The surgeon stands between the patient's legs, and the first and second assistants on the left and right side of the operating table, respectively.
Ports Placement
Five 10 mm ports are used for the operation. Port 1 is placed in the midline or slightly to the left about 14 cm below the xiphoid process. This port is used for insertion of the 30° scope. Ports 2 and 3 are placed about 2 cm below the right and left costal margins (forming an angle of about 120°). Port 4 is placed at the level of port 1 in the right mid-clavicular line (this is used for the liver retractor) and port 5 is placed at the level of port 1 in the left mid-clavicular line (Fig. 1).
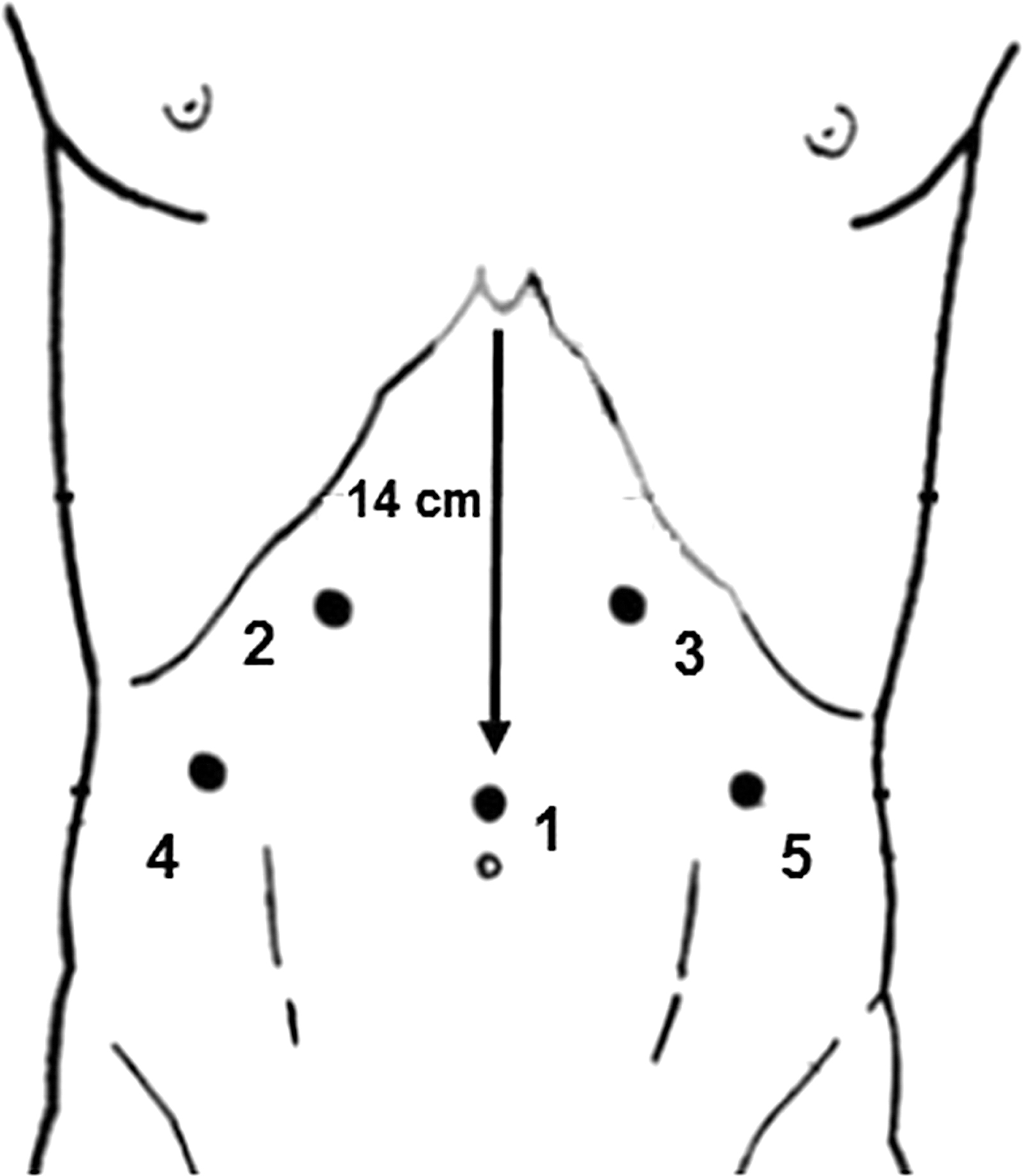
Placement of abdominal ports.
Division of Gastrohepatic Ligament
Once the left segment of the liver is retracted and the gastroesophageal junction (GEJ) is adequately exposed, the gastrohepatic ligament is divided starting above the caudate lobe of the liver toward the right crus. The esophagus is then separated from the right crus with gentle maneuvers and blunt dissection. At this point, the posterior vagus nerve should be identified and preserved.
Division of Phrenoesophageal Membrane
The phrenoesophageal membrane is lifted, incised, and divided clockwise above the esophagus. The anterior vagus is identified and left attached to the esophageal wall. The esophagus is then gently separated from the left pillar or the crus. If a Dor fundoplication is planned, there is no need to perform a posterior dissection. Therefore, the dissection is usually limited to the anterior and lateral aspects of the esophagus.
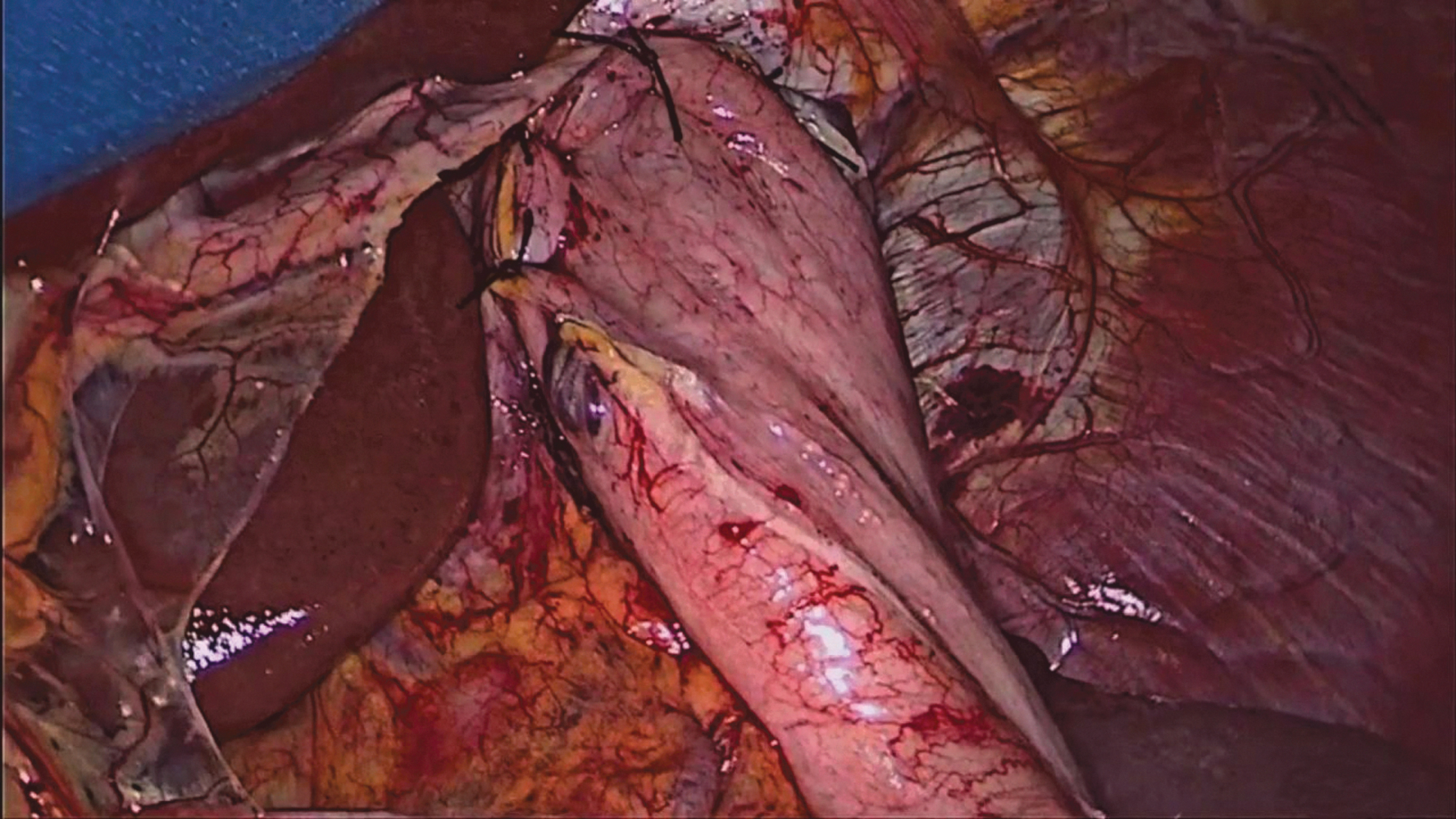
Division of Short Gastric Vessels
Starting from a point midway along the greater curvature of the stomach, the short gastric vessels are taken down with a vessel sealing system toward the fundus and all the way to the left pillar of the crus. This will allow for sufficient mobilization of the upper fundus needed for the fundoplication. Excessive traction of the short gastric branches should be avoided to prevent bleeding from the spleen (Fig. 2).
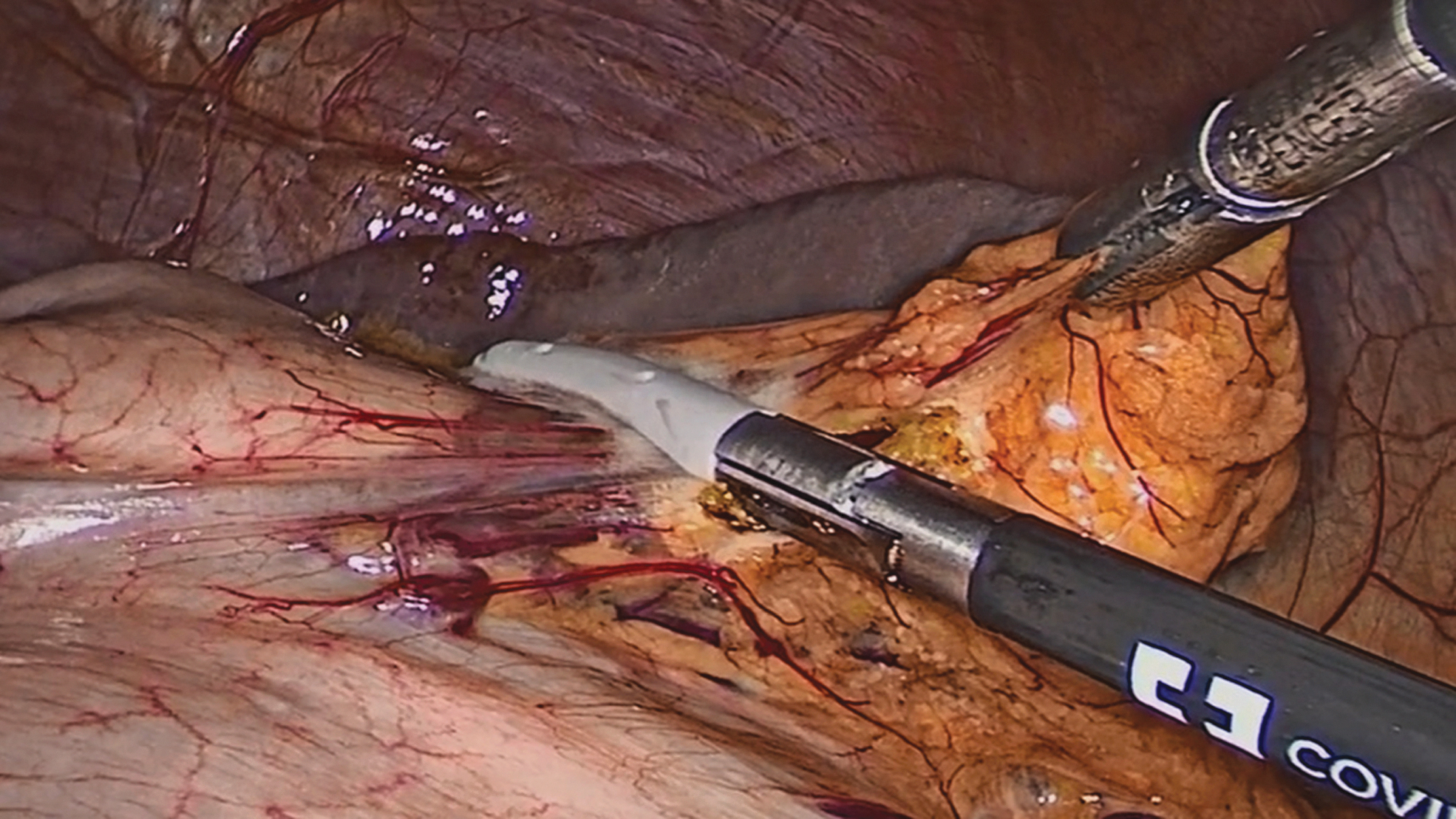
Division of short gastric vessels.
Esophageal Myotomy
The gastroesophageal fat pad should be dissected off the anterior surface of the stomach to expose the GEJ. Once the surface of the myotomy is visualized, the esophagus is pulled downward and to the left using a Babcock clamp applied over the junction. This maneuver will expose the right side of the esophagus. The myotomy should not be started at GEJ (at this level the layers are poorly defined and is hard to reach the appropriate submucosal plane) but rather about 3 cm above the GEJ at the 11 O' clock position (Fig. 3). Once the submucosal plane is identified, the myotomy is extended proximally for about 6 cm above the GEJ, and distally for about 2.5 cm onto the gastric wall. Therefore, the total length of the myotomy is about 8–9 cm (Fig. 4).
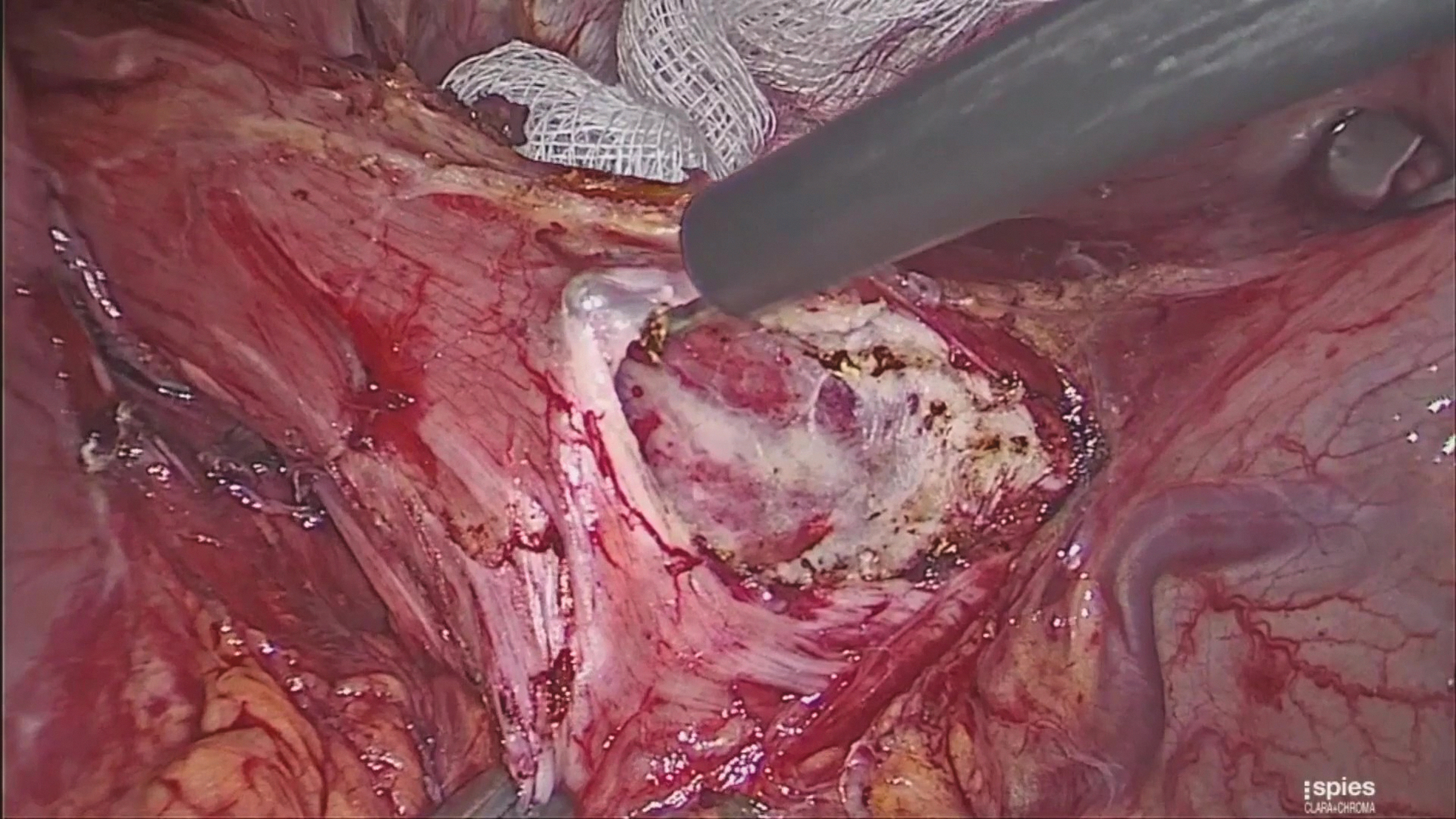
Beginning of esophageal myotomy.
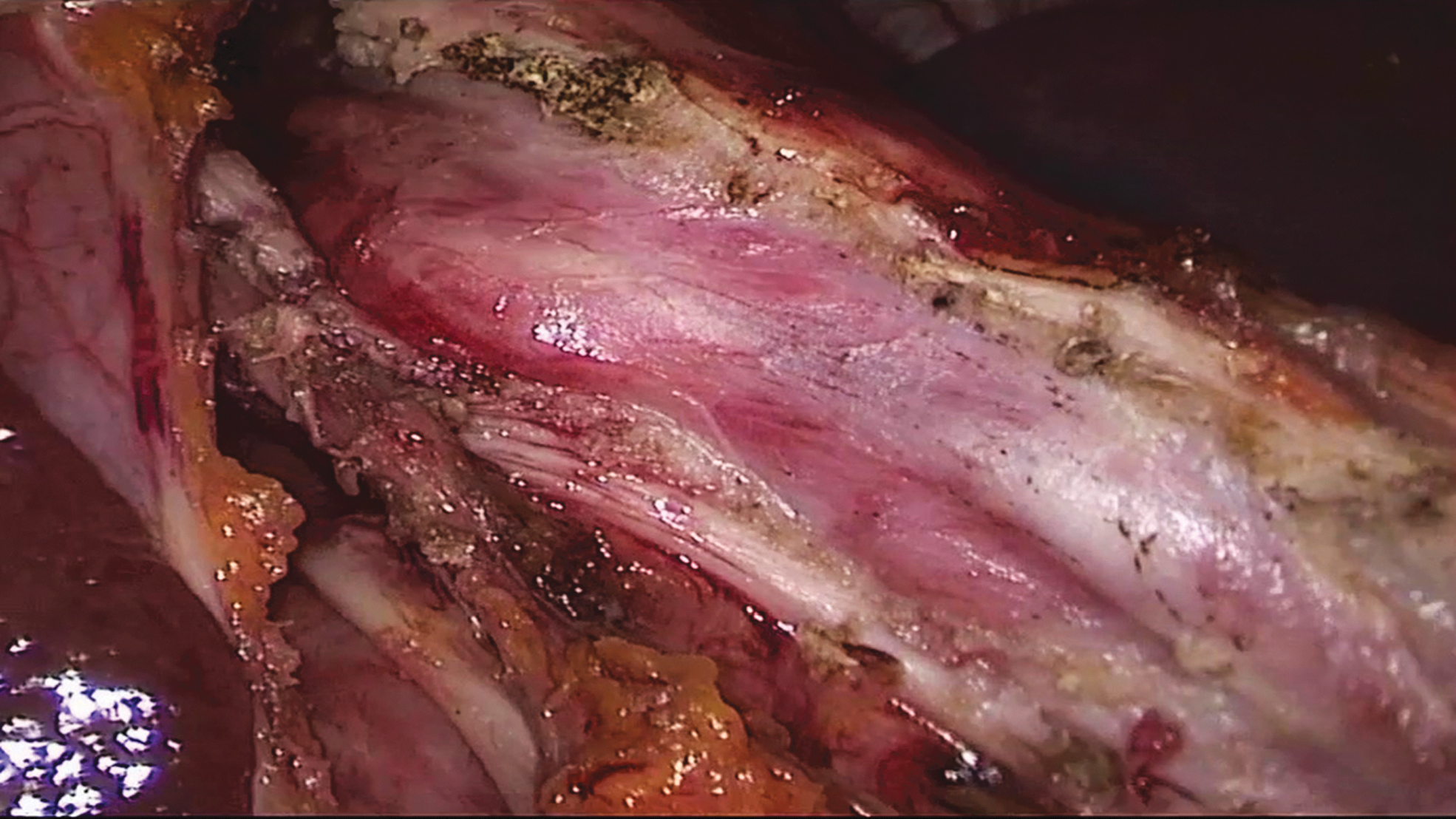
Complete esophageal myotomy.
Although different instruments can be used for the myotomy, we prefer an electrocautery with a 90° hook that allows to carefully lift and divide the circular fibers. Bleeding can occur from the muscle edges or the submucosal plexus. Compression with gauze is preferable to electrocautery to avoid injuring the esophagus. If an esophageal perforation occurs it should be repaired using a fine (4-0 or 5-0) absorbable suture material.
Dor Fundoplication
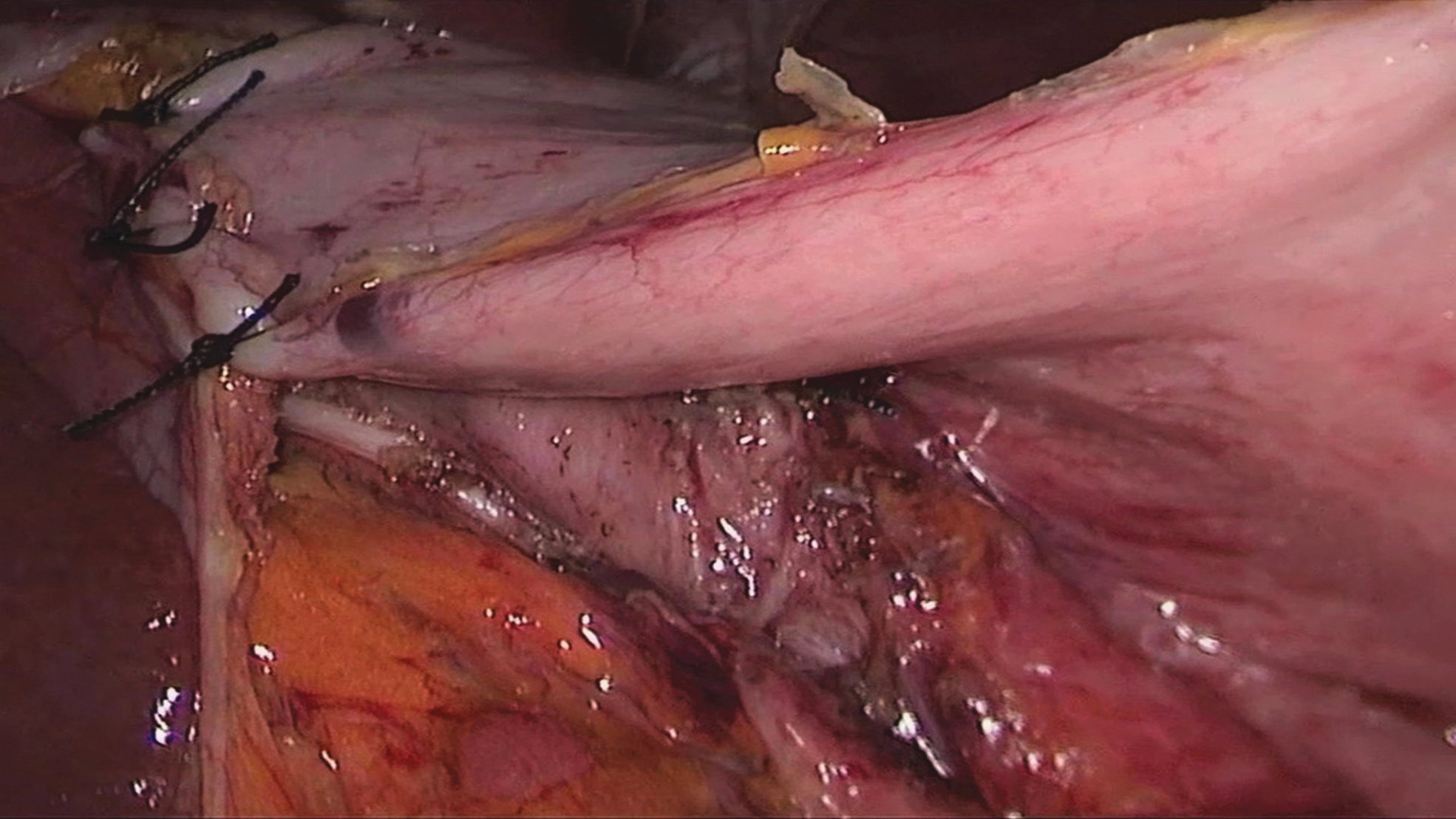
A partial fundoplication is performed to cover the myotomy and create a low-pressure valve, which will significantly decrease the risk of postoperative reflux. The Dor fundoplication is an 180° anterior fundoplication that has two rows of sutures (left and right). The left row is constituted by three stitches: the uppermost stitch incorporates the fundus, the esophageal wall, and the left pillar of the crus; the other two incorporate the stomach and the cut edge of the myotomy (Fig. 5). The gastric fundus is then folded over the exposed mucosa, placing the greater curvature next to the right pillar of the crus. The second row of stitches comprises three stitches between the fundus and the right pillar of the crus. We recommend placing one or two additional stitches between the superior edge of the fundoplication and the rim of the esophageal hiatus to remove tension from the second row of stitches (Figs. 6 and 7).

Dor fundoplication (first row of stitches).
Dor fundoplication (second row of stitches).
Complete Dor fundoplication.
Postoperative Course
Patients are fed the morning of the first postoperative day and are instructed to avoid meat, carbonated drinks, and bread for 2 weeks. Most patients are discharged within 48 hours and resume their regular activity within 2 weeks.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.