
Abstract
The hybrid esophagectomy is a procedure that combines an initial laparoscopic approach in which the gastric conduit is prepared preserving the right gastroepiploic artery, followed by a right thoracotomy for resection of the esophagus, gastric pull-up into the chest, and esophagogastric anastomosis. Critical surgical steps should be carefully respected to perform a safe operation.
Introduction
The esophagectomy is a technically challenging procedure, which requires advanced skills in abdominal and thoracic surgery. Better patient selection, enhanced perioperative care, and embracement of minimally invasive techniques have certainly contributed to reduce mortality rates of esophageal resection for cancer.1,2
The hybrid esophagectomy is a procedure that combines an initial laparoscopic approach in which the gastric conduit is prepared preserving the right gastroepiploic artery, followed by a right thoracotomy for resection of the esophagus, gastric pull-up into the chest, and esophagogastric anastomosis. 3 Previous studies have shown that both totally minimally invasive esophagectomy and hybrid esophagectomy were associated with decreased blood loss, decreased time in the ICU, less complications (including pulmonary complications), and shorter hospital stay, as compared with open esophagectomy.4,5 Moreover, the laparoscopic gastric mobilization has proven to reduce in-hospital, 30- and 90-day postoperative mortality after surgery for esophageal cancer. 6
A recent multicenter open-label controlled trial randomized 103 patients to a hybrid esophagectomy (laparoscopic gastric mobilization and open right thoracotomy) and 104 to an open esophagectomy; hybrid minimally invasive esophagectomy resulted in less intraoperative and postoperative major complications, specifically pulmonary complications, without compromising overall and disease-free survival. 7
Overall, current data suggest that hybrid esophagectomy is an excellent option for patients with esophageal cancer undergoing surgical treatment.
Preoperative Phase
Before starting the operation, the patient is intubated with a double lumen endotracheal tube and two large bore intravenous, arterial line, and urinary catheter are inserted. The anesthesiologist also places an epidural catheter for postoperative pain management. An upper endoscopy is often performed to determine the location and extent of the tumor and any associated Barrett's esophagus. Air insufflation should be minimal and adequately suctioned out with the scope, and an orogastric tube should be placed to completely decompress the stomach.
The patient is positioned supine in low lithotomy position over an inflated beanbag with the lower extremities extended on stirrups, with knees flexed 20°–30°. Pneumatic compression stockings are always used as prophylaxis against deep vein thrombosis. The surgeon stands between the patient's legs, and the first and second assistants on the left and right side of the operating table, respectively.
Laparoscopic Phase
Five 10 mm ports are used for the operation. Port 1 is placed about 18 cm below the xiphoid process in the midline. This port is used for insertion of the 30° scope. Ports 2 and 3 are placed about 2 cm below the right and left costal margins (forming an angle of about 120°). Port 4 is placed at the level of port 1 in the right mid-clavicular line (this port will be used for the liver retractor). Port 5 is placed at the level of port 1 in the left mid-clavicular line (Fig. 1). In case a pyloroplasty is performed, an additional port is placed in between ports 1 and 4, usually about 5 cm below them.

Placement of abdominal ports.
The dissection begins by identifying the right gastroepiploic artery and opening the gastrocolic omentum (Fig. 2). Staying away from this artery, the dissection is then continued along the greater curvature toward the fundus taking down all the short gastric vessels all the way to the left pillar of the crus, which is gently separated from the esophagus.
Dissection along the greater curvature of the stomach.
The gastrohepatic ligament is divided respecting the right gastric artery, proceeding superiorly until reaching the right crus. The esophagus is then separated from the right pillar of the crus. If an accessory left hepatic artery is encountered, it can usually be safely divided in between clips. The phrenoesophageal membrane is then divided, and the esophagus is dissected in the posterior mediastinum for about 5 cm. The esophagus is then completely encircled with a Penrose drain, which is pushed as high as possible into the mediastinum. The Penrose drain will be retrieved from the chest during the thoracic phase and will help with the thoracic dissection.
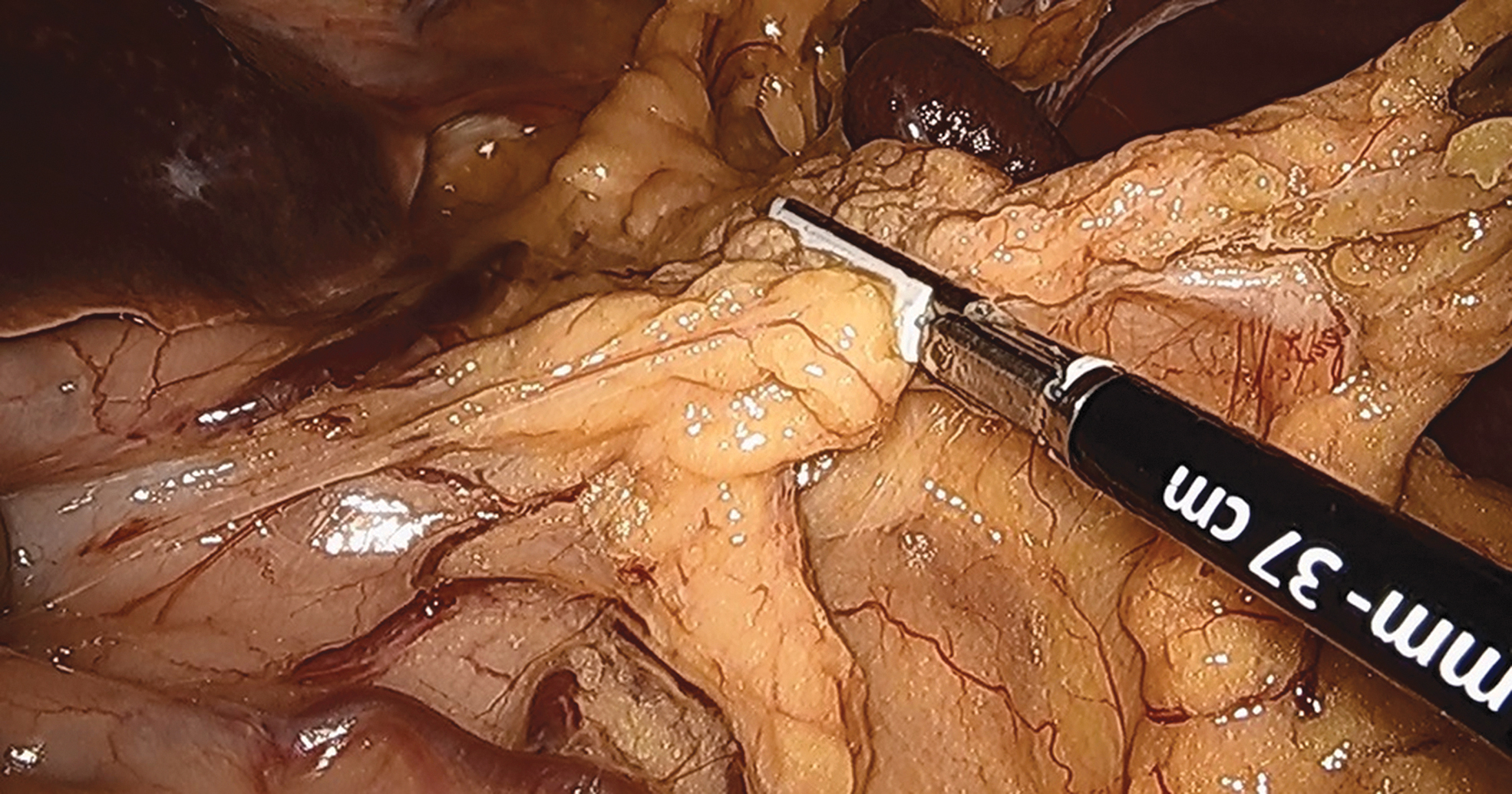
The left gastric, splenic, and common hepatic arteries are identified, and a complete dissection of their associated nodes is performed. Peritumoral injection of indocyanine green (ICG) during the preoperative endoscopy can help visualizing these nodes. 8 The coronary vein and the left gastric artery are skeletonized and carefully dissected all the way to their base to retrieve as many lymph nodes as possible, and then are transected using vascular stapler (Fig. 3).

The left gastric artery and coronary vein are transected at their base with a vascular stapler.
The blood supply of the stomach is now based only on the right gastric and right gastroepiploic arteries. Careful handling of the stomach is important to help preserving the submucosal collateral vessels. Attachments between the posterior wall of the stomach and the pancreas are taken down using the cautery. Division of the gastrocolic ligament is continued caudally toward the pylorus, which should be freely mobile and nearly reach the hiatus. A Kocher maneuver is exceptionally needed.
Pyloric drainage procedures are controversial. Although in the past we used to perform a laparoscopic pyloroplasty in every patient, we now prefer endoscopic injection of botulinum toxin into the pylorus in case of delayed gastric emptying.
Placing a feeding jejunostomy in the left mid-abdomen is strongly recommended.
After a final inspection, the ports are removed under visualization, the trocars sites are closed, local anesthesia is injected, and sterile dressings are applied.
Thoracic Phase
The patient is now repositioned in a left lateral decubitus, with the right side up in preparation for a right thoracotomy. Single-lung ventilation will help exposing the posterior mediastinum. The chest is entered through a muscle sparing posterolateral thoracotomy in the fifth intercostal space. We recommend resecting a 1.5-cm long segment of the posterior portion of the sixth rib to achieve optimal exposure of the surgical field.
The lung is retracted and the inferior pulmonary ligament is divided. The pleura is then opened above and below the azygous vein, which is circumferentially dissected and divided with a vascular stapler. The esophagus is then dissected beginning about 3 cm above the azygous vein all the way down to the hiatus, thus joining the mediastinal dissection previously performed during the laparoscopic phase (the Penrose drain is retrieved). All the periesophageal fatty and lymph nodes should be swept toward the specimen side.
The stomach is pulled up into the chest, and a window is opened along the lesser curvature about 8 cm below the gastroesophageal junction (at least a 5 cm margin from the tumor is needed). The stomach is tubularized along the greater curvature using a Endo-GIA stapler maintaining a width of 4–5 cm. After the gastric conduit is created, ICG is injected intravenously as a bolus to assess the adequate perfusion of the conduit with fluorescence imaging (assessing perfusion of the tip of the gastric conduit where the anastomosis will be performed is particularly important) (Figs. 4 and 5). 9
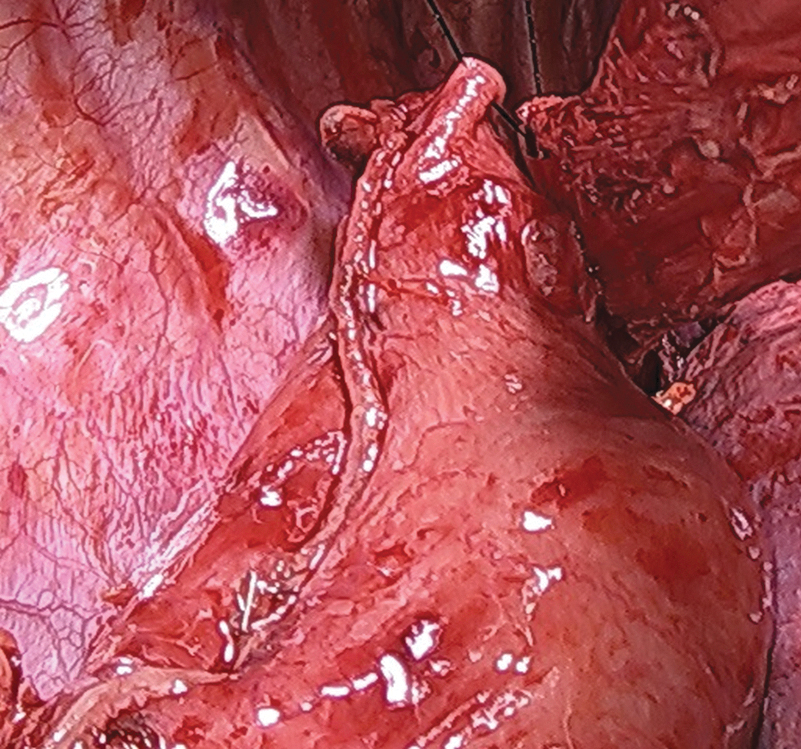
Gastric conduit.
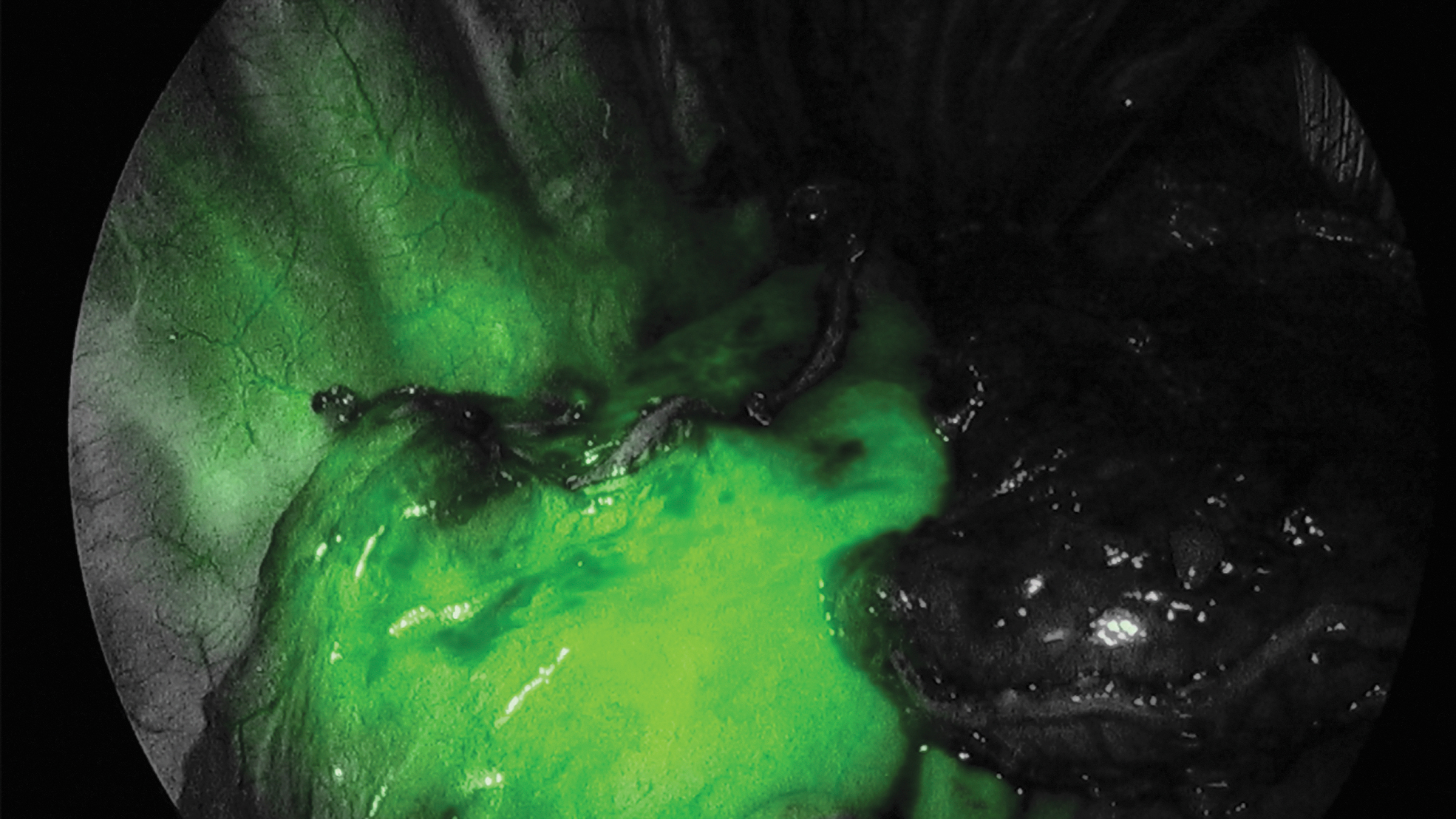
Perfusion assessment of the gastric conduit with ICG fluorescence imaging. ICG, indocyanine green.
Several anastomotic techniques are described. We believe surgeon's preference and experience are critical for determining the type of esophagogastric anastomosis used. We prefer a side-to-side linear stapled anastomosis. We start by placing the esophagus over the anterior wall of the gastric conduit, clamped with a Satinsky clamp (this avoids separation of the mucosa from the muscular layers) and transected ∼3 cm above the azygous vein. Full-thickness 3-0 silk stay sutures are placed to keep the posterior wall of the esophagus aligned with the anterior wall of the gastric fundus. In addition, 3-0 silk stay sutures are also placed at the four edges of the esophageal opening (keeping together the mucosa with the muscular layers of the esophagus) to avoid sliding of the esophageal mucosa when the stapler is inserted. A gastrotomy is then performed just distal to the esophageal transection line and interrupted 3-0 silk stitches are placed to fix the gastrotomy to the posterior wall of the esophagus. The thinner branch of 45 mm Endo-GIA stapler is inserted into the stomach and the thicker branch into the esophagus (Fig. 6). Once the stapler is fired, a 4 cm long side-to-side anastomosis between the posterior wall of the esophagus and the anterior wall of the stomach is constructed. Under direct visualization, the anesthesiologist passes a nasogastric tube through the anastomosis into the stomach. The anterior aspect of the anastomosis is closed in two hand-sewn layers: an inner layer of running 3-0 absorbable braided suture, followed by an outer layer of interrupted 3-0 silk sutures (Fig. 7).
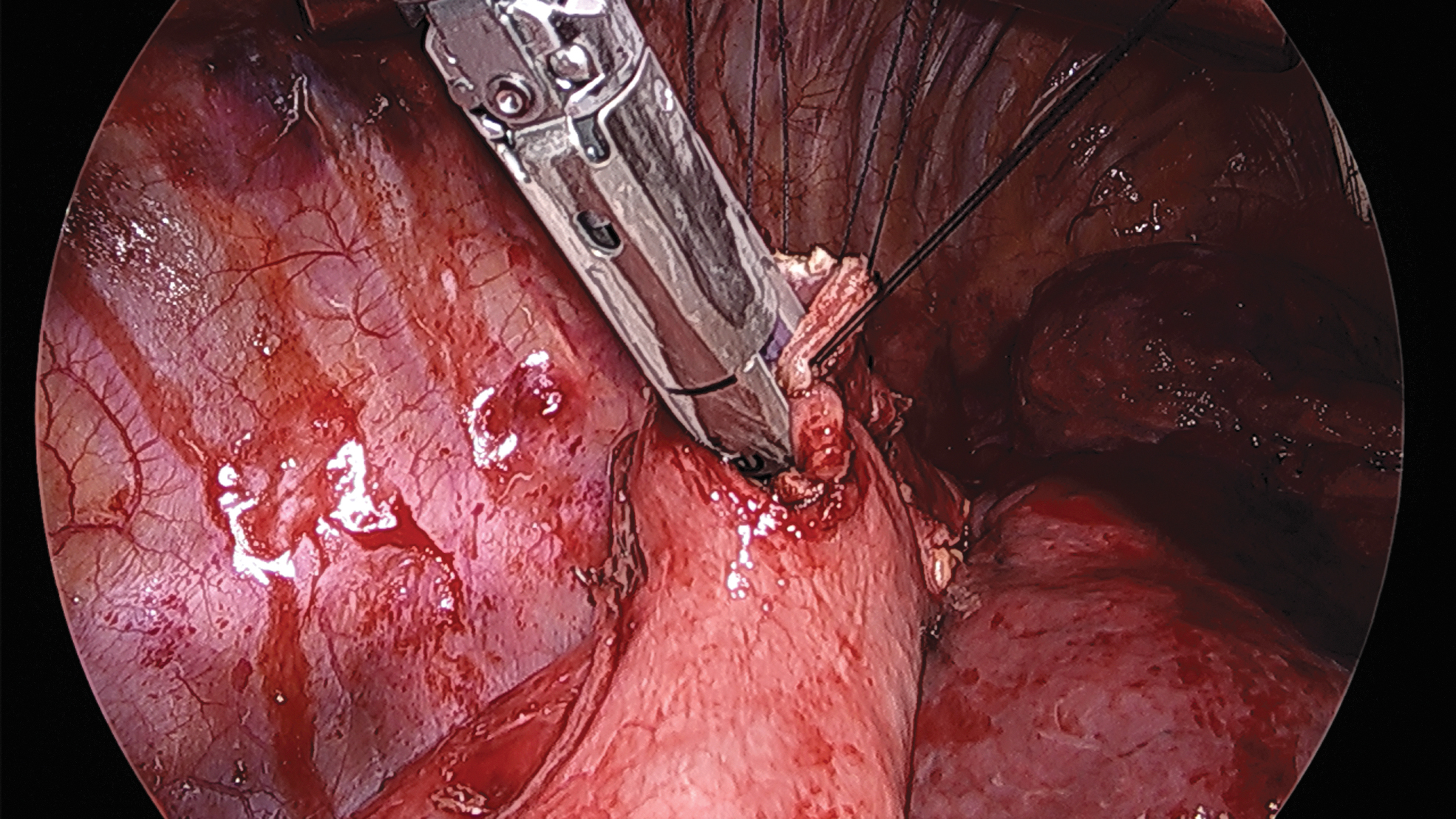
Side-to-side linear stapled anastomosis.
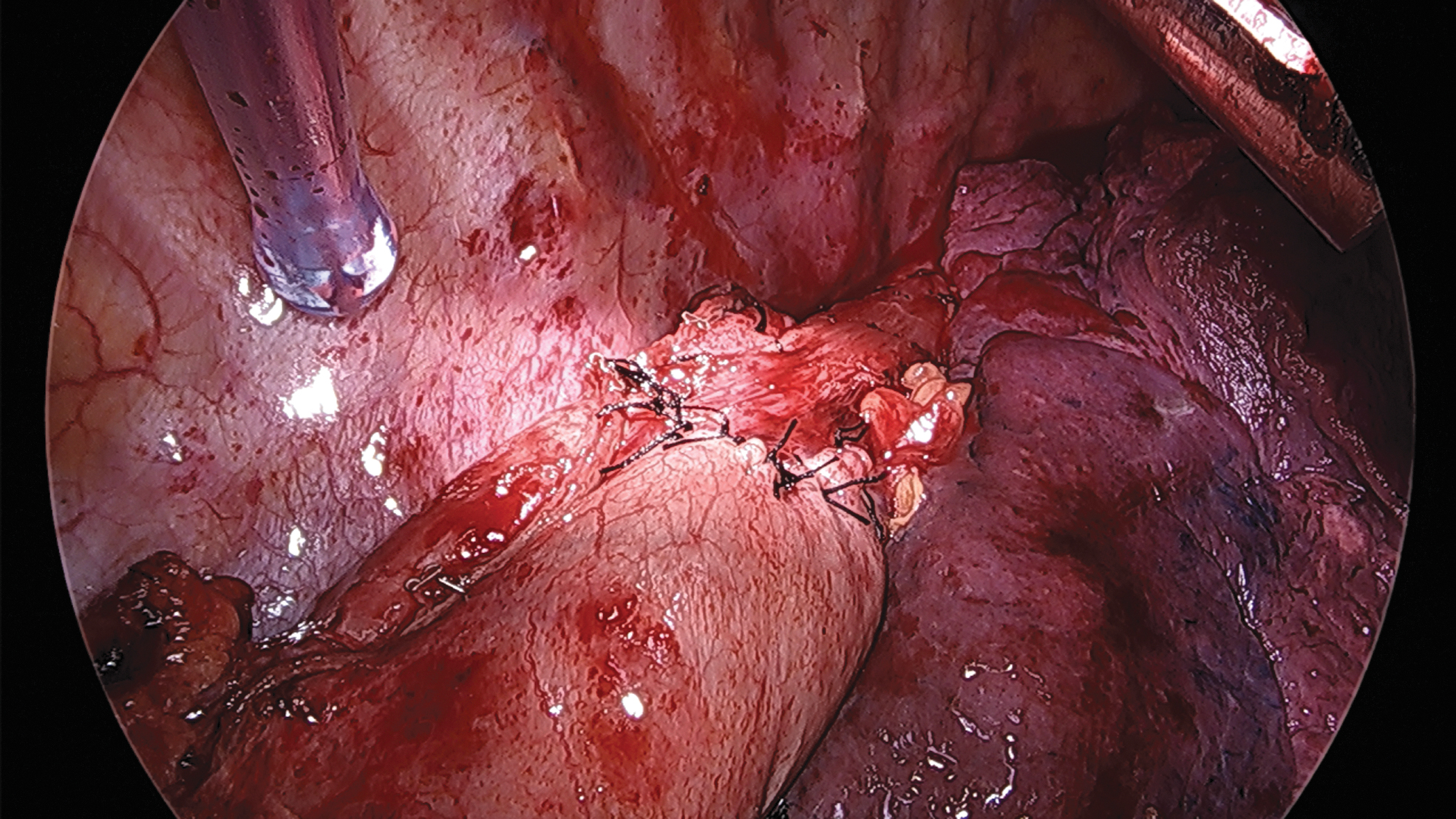
Esophagogastric anastomosis completed.
After the anastomosis is completed, a chest tube is placed and the expansion of the lung should be visualized. The thoracotomy is then closed in the standard manner.
Postoperative Course
The patient is often extubated in the operating room, and monitored in the intensive care unit overnight. The nasogastric tube can be usually removed on POD 3 and clear liquids are often started on POD 4 and 5. The chest tube can be safely removed once a chyle leak has been ruled out after initiating tube feeds or diet and if there are no signs of anastomotic leak. Incentive spirometry and respiratory exercises are strongly encouraged.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.