
Abstract
Epiphrenic diverticulum is a rare esophageal disorder occurring as an outpouching of mucosa and submucosa through the muscular layers, within 10 cm above the cardia. As the majority of epiphrenic diverticula are asymptomatic, the real incidence varies because of a considerable number of cases detected incidentally during radiographic or endoscopic evaluation. Traditionally, the operation was performed through a left thoracotomy approach and the diverticulectomy was completed with esophago-cardial myotomy and a Belsey Mark IV fundoplication. Laparoscopy offers many advantages in the treatment such as the possibility of extension of the myotomy from the lower esophagus through the stomach and the concomitant antireflux procedure to avoid postoperative reflux. The abdominal approach is also more comfortable for the patients and, as there is no need for transthoracic drains, is more tolerated in terms of postoperative pain. In this article, we do review our technique with all the steps of the operation illustrated by intraoperative pictures.
Introduction
Epiphrenic diverticulum is a rare esophageal disorder occurring as an outpouching of mucosa and submucosa through the muscular layers, within 10 cm above the cardia. As the majority of epiphrenic diverticula are asymptomatic, the real incidence varies because of a considerable number of cases detected incidentally during radiographic or endoscopic evaluation.
A primary esophageal motility disorder is considered the underlying cause of the progressive herniation of the layers and eventually of the diverticulum development. 1 The most frequent motility disorders associated are achalasia and diffuse esophageal spasm. Often, patients with normal ambulatory motility test, when studied with prolonged manometry recording show an intermittent spastic activity, validating the hypothesis of the esophageal motility disorder as primary cause; however, these testing facilities have mainly investigational application. 2
Most commonly reported symptoms are dysphagia and regurgitation of undigested food with respiratory complaints and frequent airways infections due to aspiration, which is more common in larger diverticula. Chest pain and weight loss are also frequent and can be caused by the underlying motility disorder.
To date, the standard available treatment to solve specific symptoms is surgery. The disease is so rare that only small series had been published and different approaches proposed, depending on the surgeon's preference and expertise. Traditionally, the operation was performed through a left thoracotomy approach and the diverticulectomy was completed with esophago-cardial myotomy and a Belsey Mark IV fundoplication. After the increasing success of minimally invasive surgery for benign foregut surgery, a laparoscopic approach was proposed3,4 and rapidly diffused, but transthoracic access is still performed. 5
In our opinion when a treatment is indicated, the surgical efforts should include the resection of the diverticular pouch as well as the treatment of underlying motor disorder, and the prevention of postoperative reflux. In cases of small symptomatic diverticula, an esophageal myotomy without diverticulum resection can be enough as afterward the diverticulum tends to shrink.
The advantages offered by laparoscopy are the possibility of extension of the myotomy from the lower esophagus through the stomach and the concomitant antireflux procedure to avoid postoperative reflux. The abdominal approach is also more comfortable for the patients and, as there is no need for transthoracic drains, is more tolerated in terms of postoperative pain.
Innovative approaches, including peroral endoscopic myotomy (POEM), with or without dissection of the muscular fibers of the septum, have been reported with good results, but experience and follow-up is limited.6,7
Patient Evaluation and Selection
Since only a small number of patients are symptomatic a careful interview of the patient is mandatory to achieve a good result after surgery. Particular attention must be paid to assess the history of gastroesophageal symptoms and distinguish them from food or salivary regurgitation.
Preoperative workup includes barium swallow, endoscopy, and esophageal manometry. Barium swallow defines the maximal diameter of the pouch and of the septum, the location and the distance of the diverticular neck from the gastroesophageal junction as well as a concomitant hiatal hernia. It also shows the esophageal diameter and presence of tertiary contractions or features of achalasia. Endoscopy is mandatory to rule out malignancy and to detect esophagitis due to stasis. It is also useful to place the manometry catheter in case of difficult insertion (Fig. 1).
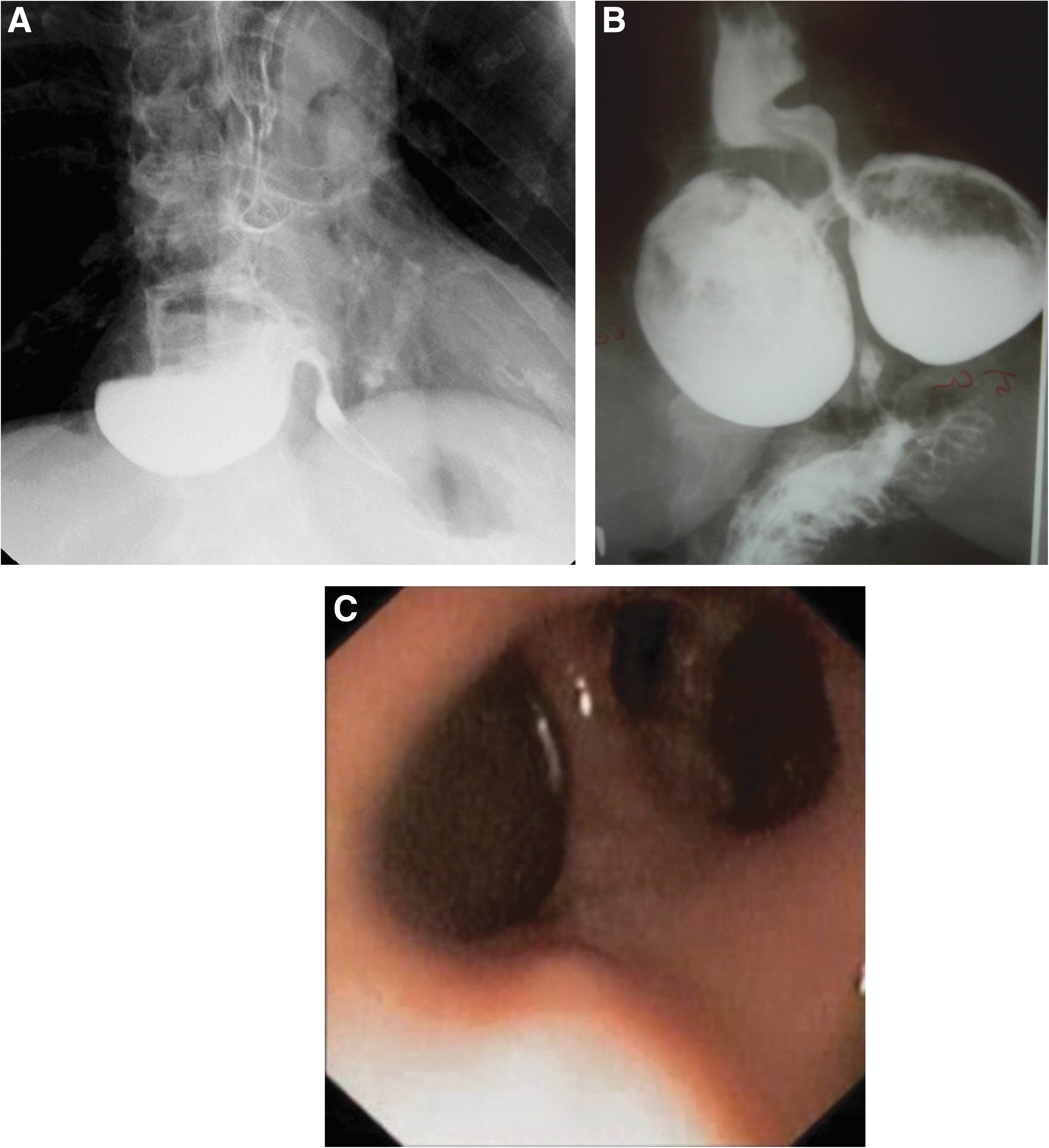
Preoperative workup.
Given the low incidence of the disease, most of the historical cases refer to perfusion manometry and the most common underlying disorder detected and reported in the literature is achalasia. These series also report a high rate of unspecific or even no evidence of motility disorder, but the sensibility of the conventional manometry is low.
High-resolution manometry is now considered the standard test to measure lower esophageal sphincter basal and resting pressure as well as to assess peristalsis, therefore classifying the underlying esophageal motor disorder.
Our database includes 48 patients treated for symptomatic epiphrenic diverticula between January 1994 and January 2019 in two institutions by the same surgical team. Patient's management and technique has been slightly refined since our previous reports.8–11
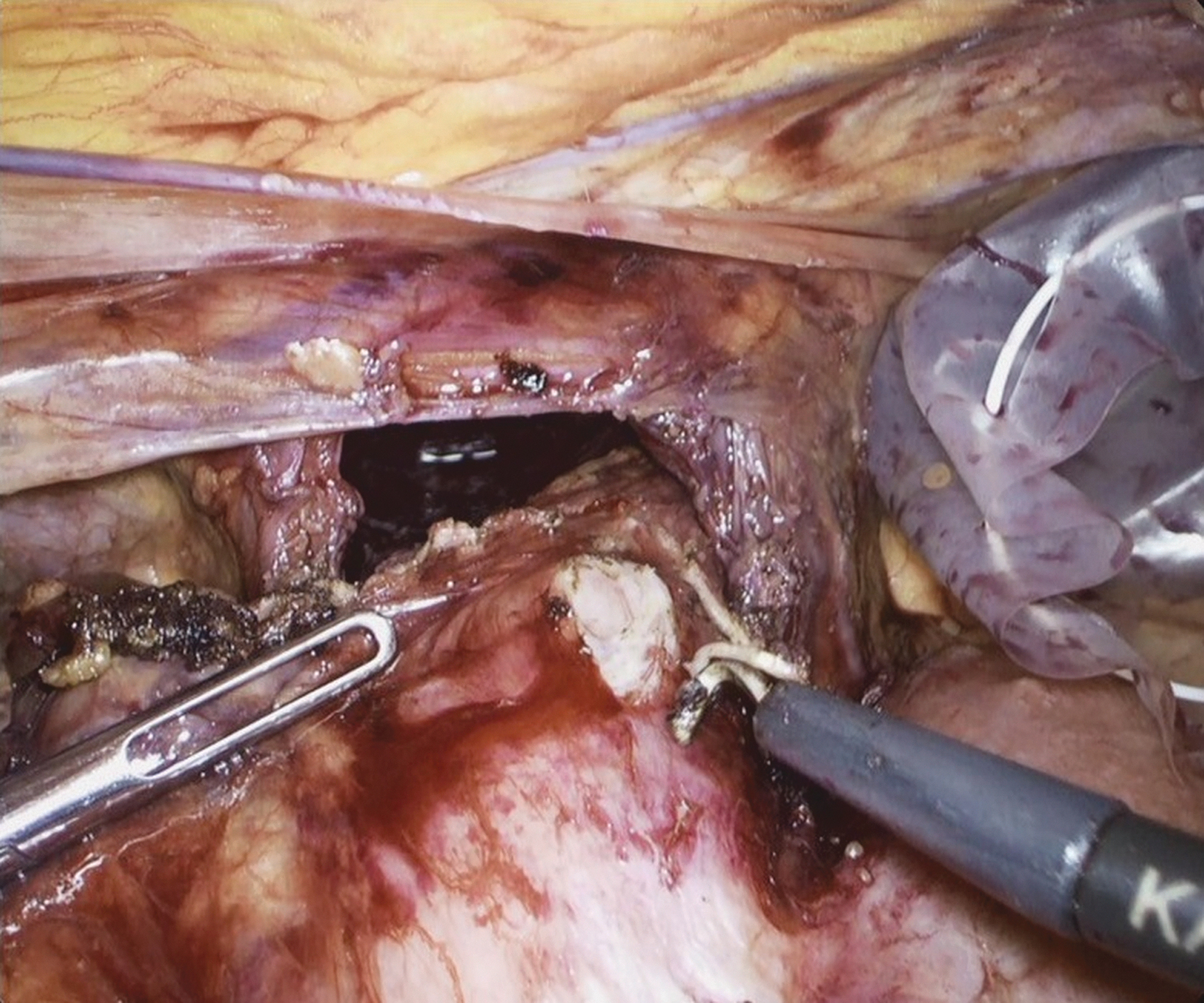
Based on the dimension of the diverticulum, symptoms severity, and presence of hiatus hernia, three different interventions were performed: laparoscopic transhiatal diverticulectomy with Heller myotomy and an anterior Dor fundoplication (34 patients) or posterior Toupet fundoplication (11 patients with concurrent hiatal hernia); in 3 patients with a small symptomatic diverticulum and Heller's myotomy with a Dor wrap was done alone. When specified, the dimensions of the diverticula were classified as small, (<4 cm) 6 patients, medium (from 4 to 6 cm) in 19 patients, and large (>6 cm) in 6 patients. Median length of myotomy was 9 cm (5–13). One patient had two large diverticula, one right-sided and the other on the opposite side, resembling Mickey Mouse ears at barium swallow; in this particular case a double diverticulectomy was carried on with the myotomy in the middle of the two, in central position, together with a Toupet fundoplication.
All surgical interventions were carried out laparoscopically, with no need of conversion with a median operative time of 145 minutes (58–340). Intraoperative complications occurred in 10 patients (21%): 10 pneumothorax treated with a pleural drain, and 3 cases of gastric or esophageal perforation, immediately detected and repaired with interrupted stitches.
Preoperative symptoms, divided by severity are shown in Table 1. The most common symptoms were dysphagia and regurgitation. Other indications for surgery were disabling chest pain and recurrent airways infections (Table 1).
Preoperative Symptoms
Operative Technique with Figures
Before surgery is mandatory for the patient to have a clear-liquid diet for 24 hours, and fasting for at least 12 hours. Depending on the size of the diverticulum, the insertion of a double-lumen nasogastric tube 12 hours before surgery to wash and clean the esophageal lumen from food debris is advisable.
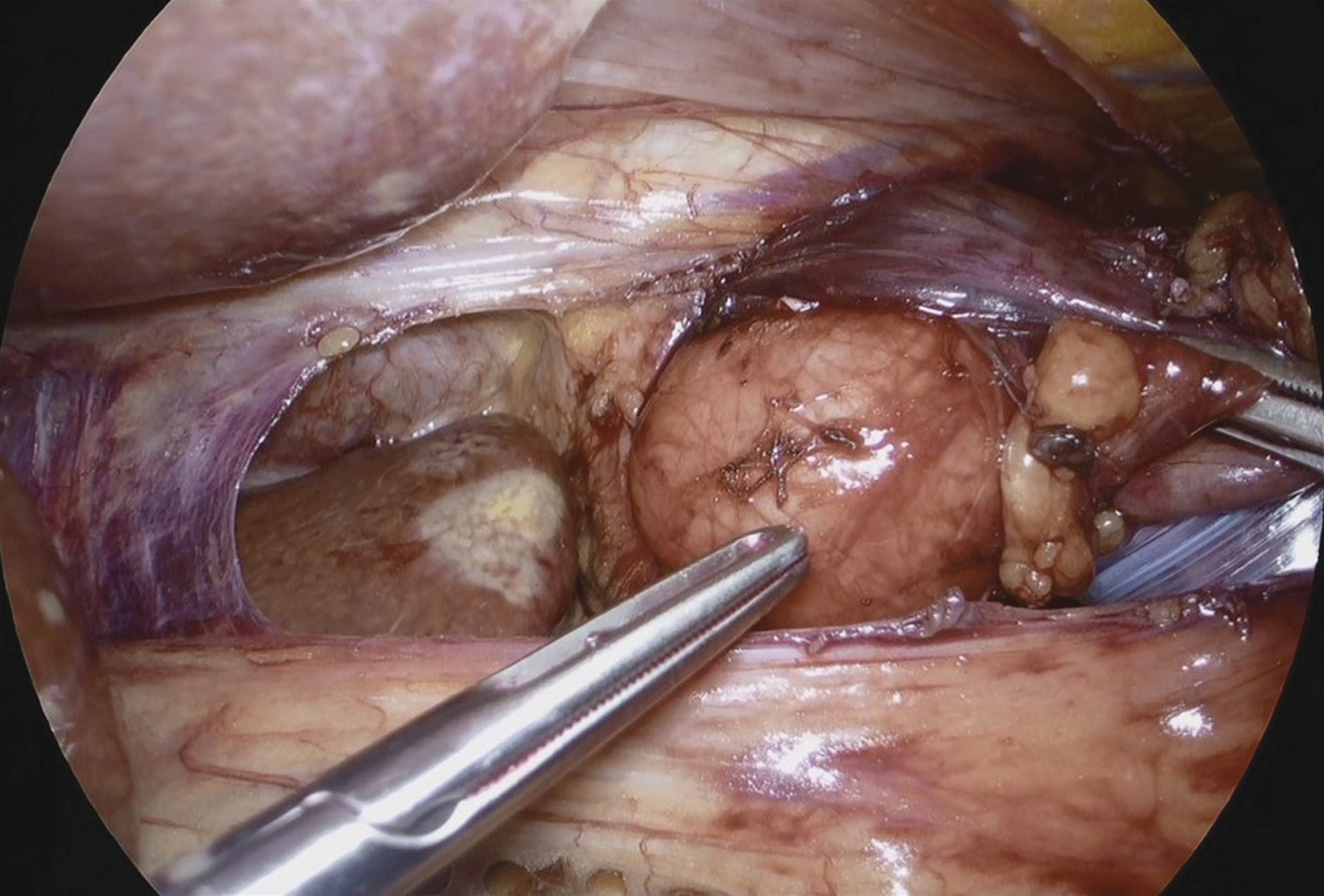
As for other foregut operations, the patient is placed in the lithotomy position with the surgeon standing between the patient's legs. After induction of the pneumoperitoneum with a Veress needle, trocars are in placed as in Figure 2. First step of the operation is the incision of the phreno-esophageal membrane (Fig. 3), sparing the branches of the hepatic division of the anterior trunk of the vagus nerve. The cardia and the abdominal esophagus are completely mobilized, an adequate retroesophageal window is created, and the esophagus is encircled to obtain a good traction, taking care not to damage the anterior and posterior vagus nerves. A good exposure of the mediastinal esophagus must be achieved, by means of combined blunt and sharp dissection. This part can be challenging as the diverticulum can be up to 10 cm from the cardia (Fig. 4). An intraoperative endoscopy guides the exposure of the diverticulum, avoiding mucosal injuries and helping to reach safely the diverticular neck that must be cleaned from adherences, especially on its upper limit. During this step, it is very important to avoid pleural tears. Once the diverticular neck is exposed and the pouch fully dissected, the diverticular neck is sectioned with either a vascular or parenchima cartridge of linear stapler introduced from the left quadrant trocar, and thus reaching the esophagus with a proper angle (Fig. 5). It is important to maintain the suture line parallel to the esophageal axis. Afterward, two or three nonabsorbable stitches or a nonabsorbable barbed continuous suture can help close the muscular layer, thus buttressing the mucosal mechanical suture. Before sectioning the diverticular neck and after the muscular closure, an endoscopic control sizes the diameter of the remaining esophagus to avoid narrowing of the lumen. The second part of the operation adds the myotomy of the esophagus, starting from the cardia up to at least the inferior margin of the diverticular neck to aid the bolus transit and avoid overpressure at the level of the staple line (Figs. 6–8). As most diverticula are on the right side of the esophagus, the myotomy should be performed anteriorly or slightly on the left side. In presence of more than one diverticulum, as for our case of two large diverticula resembling Mickey Mouse ears, they must be dissected and resected separately, with myotomy in the middle (Fig. 9).

Trocar positioning.
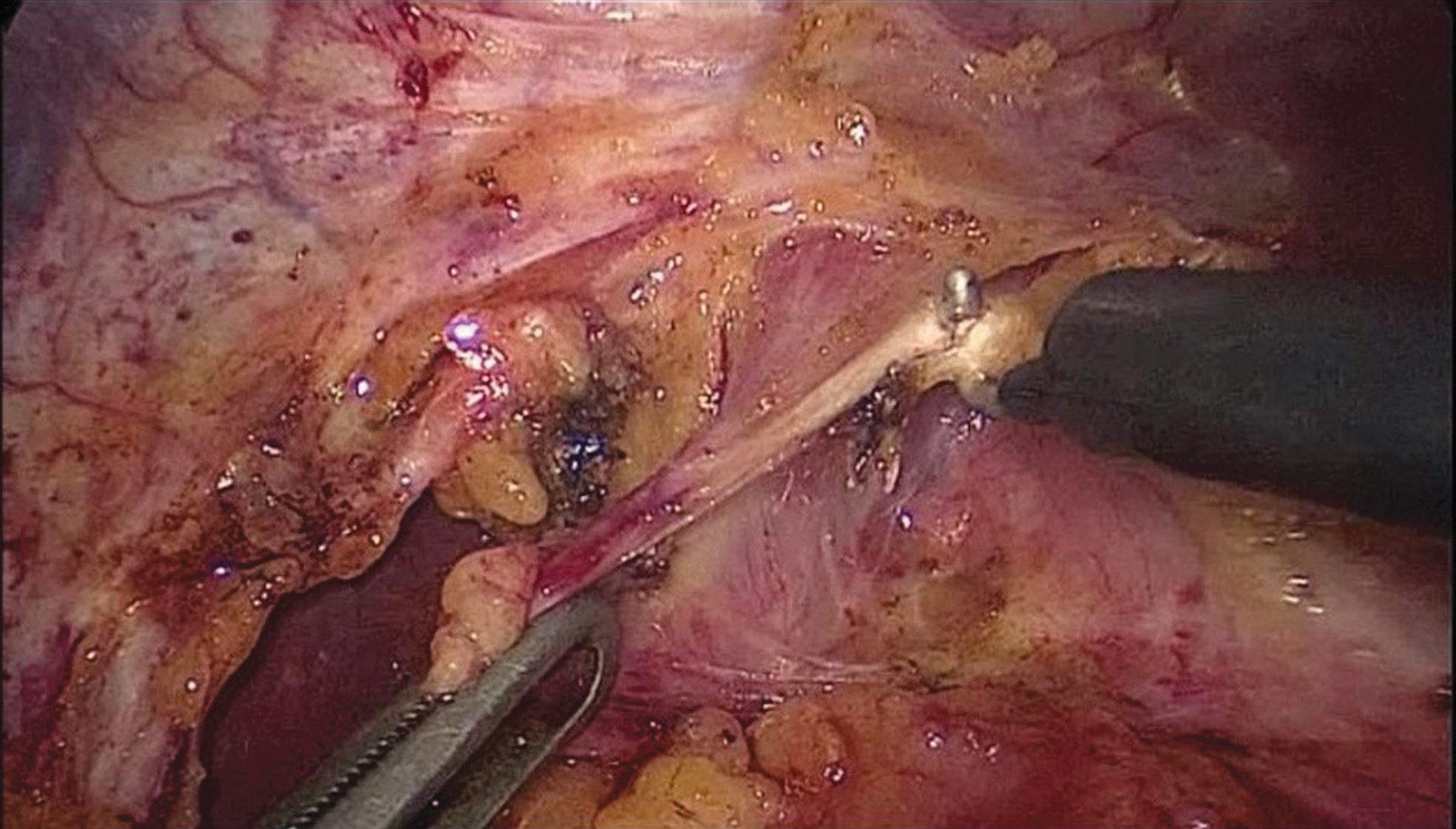
Dissection of the crura. The right crus is separated from the right side of the esophagus by blunt dissection and coagulation hook. Afterward, the right crus is dissected inferiorly toward the junction with the left crus.
After having encircled the esophagus to aid traction, the diverticulum (rightsided, in this figure) is carefully dissected from the pleura and from adherence in the mediastinum.

A linear stapler is positioned at the level of the diverticular neck parallel to the esophageal axis.
Esophageal myotomy starts at the level of the esophagogastric junction, on the anterior part of the esophagus and extended upward.

Myotomy is then completed also on the gastric side.

After the myotomy is completed an endoscopy checks for mucosal tearing.
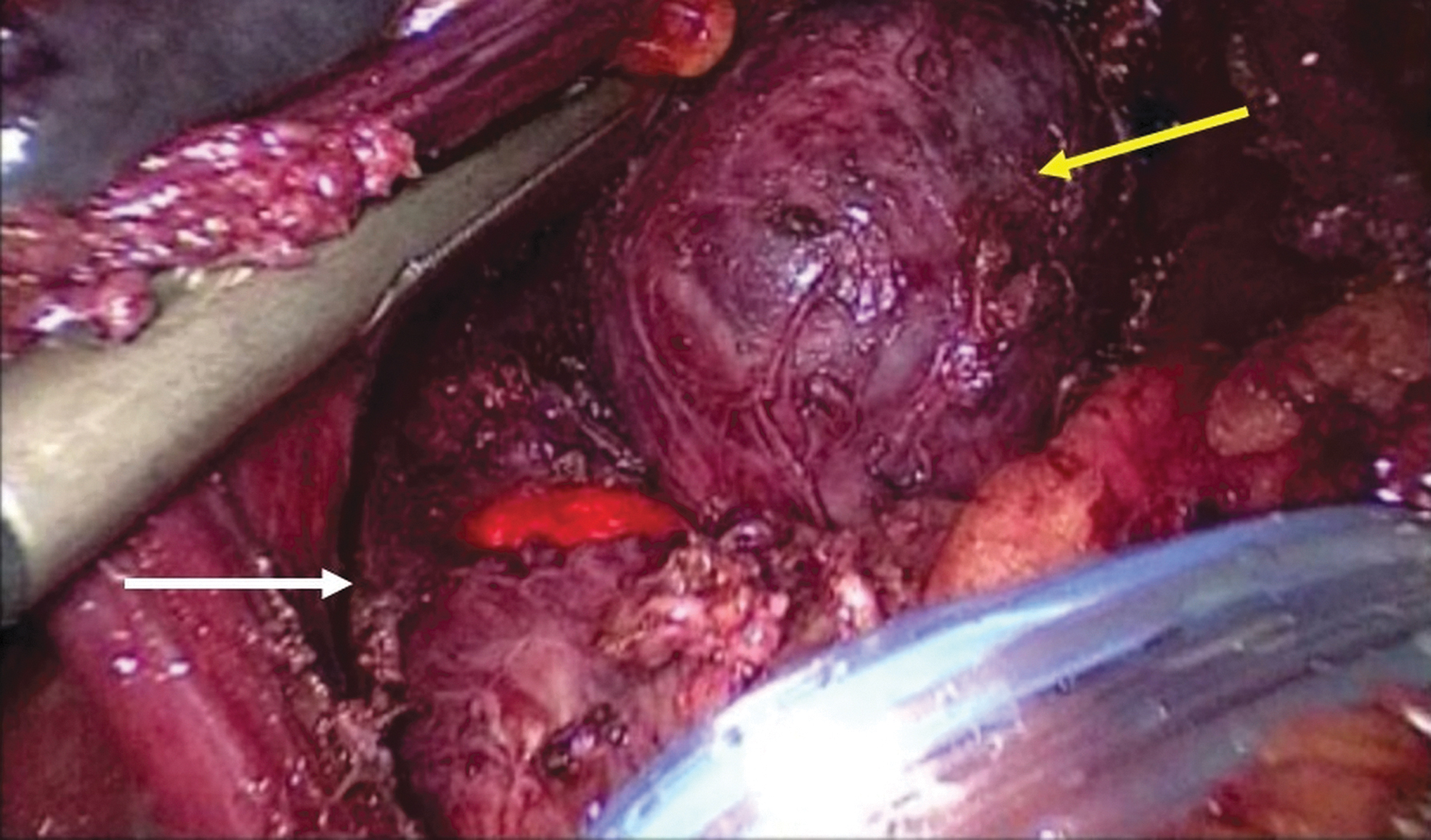
Particular case of treatment of double diverticulum. White arrow showing staple line of right-sided diverticulectomy. Yellow arrow showing the left-sided diverticulum fully dissected from mediastinal adherence. In the middle is visible the light from endoscopic control. (Data presented at 97th Congress of American College of Surgeons, San Francisco, October 2011)
After the myotomy is completed, the hiatus is closed with a few braided nonabsorbable stitches. Attention must be paid not to narrow the hiatus resulting in outflow obstruction and, therefore, causing hyper-pressure on the staple line resulting in possible leakage.
The last step of the operation involves the prevention of gastroesophageal reflux, usually with an anterior Dor fundoplication or a posterior Toupet (if a hiatus hernia is present) (Fig. 10). Depending on the fundoplication chosen to prevent reflux the short gastric vessels might be transected.
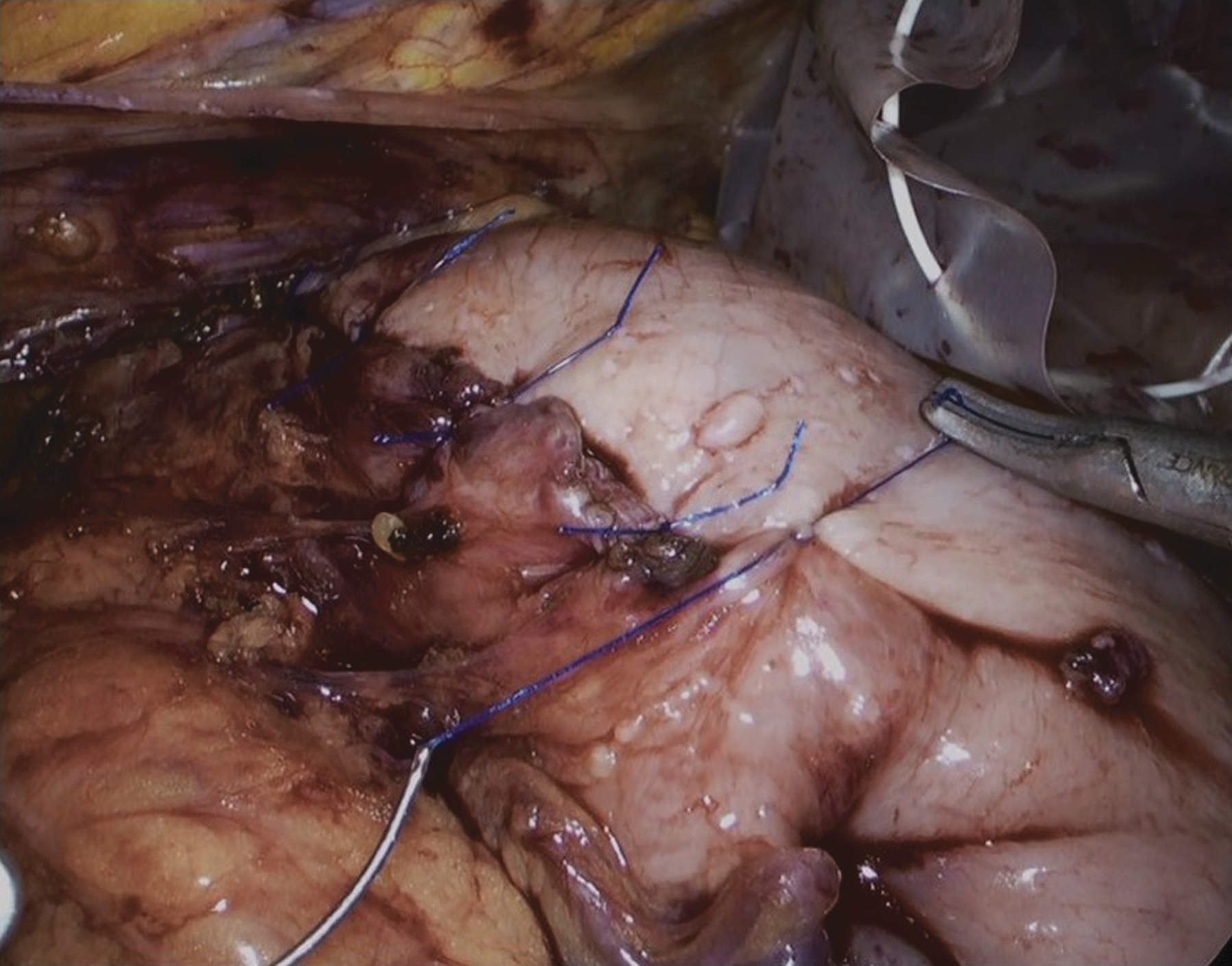
Anterior Dor fundoplication. The fundus of the stomach is then folded anteriorly to achieve an antireflux wrap.
Postoperative Course
On postoperative day 1, a gastrographin swallow is performed to rule out a possible leak from the staple line or from the myotomy. Afterward the patient is free to drink and eat a soft diet. After discharge, the patient continues the same dietary regimen for 2 weeks; after an outpatient clinic control that will allow an unrestricted diet.
Incidence of a leak from the staple line is well reported, ranging between 4% and 23%.4,12,13
In our cohort of patients, the overall complication rate was 13% (Table 2): a leak occurred in 3 patients (6%), managed endoscopically with the over-the-scope-clip system (Ovesco Endoscopy, GmbH, Tuebingen, Germany) in 1 patient. The other 2 patients required a reintervention through a left thoracotomy: the tearing was sutured and reinforced with an intercostal muscle flap. Readmission was necessary in 1 patient, in which an esophageal stent was positioned for a persistent esophageal leak (Table 2).
Postoperative Course
Median follow-up was 70 months (7–247). Symptoms of gastroesophageal reflux were reported by 5 patients (10%), 4 treated with proton-pump inhibitor with benefit, and 1 requiring a redo fundoplication; postoperative occasional dysphagia was reported in 2 patients (4%). An asymptomatic recurrence of diverticulum was detected in 1 patient by barium swallow.
Discussion
Selection of the patient is the mainstay for the treatment of epiphrenic diverticula. Considering the difficulty of the operation and the possibility of serious complications, the mere presence of a diverticulum, found incidentally or causing mild symptoms, is not an indication for a surgical treatment. Some authors offered a diverticulectomy for all patients with diverticula for the higher risk of respiratory symptoms and aspiration, 14 but mortality is not insignificant even in high-experienced centers. 15
Since 1960s, by Belsey 16 and later on by Orringer, in 1993, a “masterful inactivity” was advocated as the best approach in case of asymptomatic diverticula. 17 Not even the risk of cancerization can tilt the balance in favor of surgery, because the risk is very low, reported as 0.6%, 18 thus suggesting just routine endoscopic follow-up.
In patients with incapacitating symptoms, an esophagomyotomy was also advised, but the extension is questionable. We strongly agree with this opinion as an underlying motility disorder is probably the cause of diverticulum and expansion even if not properly identified by preoperative testing, thus justifying the extension of myotomy beyond the lower esophageal sphincter. If this step of the operation is not done, the risk of leak from the staple line or of recurrence of the diverticulum is more frequent; This part is so important that even in cases of mid-esophageal diverticula treated with transthoracic approach, a laparoscopic myotomy is recommended.
As for Heller myotomy, to avoid or limit the incidence of postoperative gastroesophageal reflux, an antireflux fundoplication is mandatory: the decision on which kind depends on the presence of hiatus hernia. Besides the presence of motility disorders, a total fundoplication is not recommended because it increases the pressure at the lower esophageal sphincter and thus of potential postoperative leaks: in case of concomitant hiatus hernia (11 patients in our series) a posterior partial fundoplication is sufficient to prevent gastroesophageal reflux.
Conclusions
Transhiatal approach to treat epiphrenic diverticulum is safe and effective in the large majority of the patients. As this operation is technically challenging and can result in potentially life-threatening sequelae and mortality, it must be done in a specific setting by a well-trained surgical team capable of dealing with intra- and postoperative complications. This means that surgery for epiphrenic diverticula should be centralized in high-volume centers for foregut surgery. A careful and complete evaluation of the patients' symptoms and preoperative workup should be done before considering surgery. Remember the “masterful inactivity” suggested by Sir Ronald Belsey for asymptomatic patients.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.