
Abstract
Inguinal hernia repair (IHR) is one of the most commonly performed general surgery operations. Currently, an inguinal hernia can be repaired through an open, laparoscopic, or robot-assisted approach. Herein, we detail our perioperative evaluation and management of patients with a groin hernia as well as our surgical technique for the performance of the laparoscopic transabdominal preperitoneal IHR.
Introduction
Inguinal hernia repair (IHR) is one of the most commonly performed general surgery operations in the United States. In fact, more than 700,000 inguinal hernias are repaired annually in the United States.1–5 While laparoscopic IHR has been shown to be a safe and effective approach to the treatment of inguinal hernias, open IHR remains the gold standard.6,7 In the 2004 VA Cooperative Study, patients undergoing open IHR experienced better outcomes with respect to postoperative morbidity and inguinal hernia recurrence. 6 These differences in outcomes between the open and laparoscopic IHR groups, however, became insignificant as surgeon volume increased. 6 This finding reinforces the idea that surgeons performing laparoscopic IHR should do so on a regular basis. 2 Herein, we detail our approach to the evaluation of patients with a groin hernia, the important technical steps to laparoscopic transabdominal preperitoneal (TAPP) IHR, as well as the postoperative care and follow-up of patients who have undergone laparoscopic IHR.
Preoperative Evaluation and Patient Selection
There are surgeon, patient, and groin hernia factors that should be considered when evaluating and deciding the surgical approach to IHR. Often, a patient with a groin hernia will be referred to a general surgeon after imaging confirmation, such as with an abdominal or scrotal ultrasound or computed tomography (CT) scan of the pelvis. However, if a patient is referred without imaging confirmation of a groin hernia, a focused history of inguinal hernia-related symptoms should be performed, focusing on groin pain, presence of a groin bulge, bowel obstructive symptoms, and any overlying skin changes. A physical examination of the groin should also be performed. To do this, the patient should be standing. Visual evaluation comparing both groins can often times reveal a visible groin bulge and confirm the presence of an inguinal hernia. If not, external pressure over the inguinal canal while asking the patient to cough and/or perform a Valsalva maneuver should facilitate diagnosis of a groin hernia. If groin hernia diagnosis is still allusive following physical examination, but the patient's history and symptoms are consistent with a possible inguinal hernia, imaging of the patient's groin should be performed.
Once a groin hernia has been diagnosed by examination and/or imaging, the surgeon must decide if the patient requires surgical intervention. In the early 2000s, most patients with groin hernias were undergoing IHR despite small hernia defects and only mild-to-moderate discomfort due to the presumed risk of hernia incarceration and strangulation.2,8,9 Nevertheless, in two studies published in 2006, one by Fitzgibbons et al. and the other by O'Dwyer et al., they found that the annual risk for inguinal hernia incarceration or strangulation was less than 1%.8,9 With these findings, it has been recognized that a “watchful waiting” approach to inguinal hernia management is an acceptable option. Additional studies since 2006 have subsequently found that upward of 30% of patients with asymptomatic or mildly symptomatic inguinal hernias crossover to surgical repair within 1 year of the diagnosis of an inguinal hernia and that the rate of crossover after the first year following diagnosis of an inguinal hernia is close to 5% annually.2,8,10–12 To assist in identifying patients who may not be successfully watched, specific patient and inguinal hernia risk factors have been proposed to help identify patients who may benefit from surgical repair at the time of evaluation of their groin hernia, including patients with a known femoral hernia, patients with an inguinal hernia who experience groin pain with activity, patients whose daily activities are limited by their inguinal hernia, and those patients with a chronically incarcerated inguinal hernia.5,12,13
If the decision is made to proceed with IHR, next the surgeon must decide if laparoscopic repair is beneficial and feasible. Prior pelvic surgery and/or radiation are often relative contraindications for laparoscopic IHR due to the potential difficulties in dissection of the preperitoneal space posed by scar tissue. 14 Patients with an inguinal hernia recurrence following open IHR, patients suspected of having bilateral inguinal hernias, and female patients are more likely to benefit from a laparoscopic IHR.5,13,14
Once a patient has been identified as a potential candidate for laparoscopic IHR based on the specific groin hernia risk factors, it is imperative that a thorough review of the medical history is performed. Most commonly, laparoscopic IHR is performed under general anesthesia. 5 Therefore, patients who cannot tolerate general anesthesia due to their associated medical comorbidities are not candidates for laparoscopic IHR. In terms of patient-specific risk factors that may contribute to increased morbidity and mortality following laparoscopic IHR, we use the risk factors previously identified by the Ventral Hernia Working Group to aid in our preoperative discussions. 15 While the associated morbidity and mortality following IHR are much less than that following ventral hernia repair, we do feel that optimization of patient-specific risk factors can further improve postoperative outcomes and hernia repair durability following laparoscopic IHR. The natural history of groin hernias affords a period of time with minimal associated symptoms, in most cases.8,9 Therefore, preoperative optimization of this patient population is often easily facilitated without a significant increase in the rate of groin hernia events, such as inguinal hernia incarceration with associated bowel obstruction or strangulation. The specific patient factors that we address before laparoscopic IHR include a patient's weight, smoking status, nutritional status, and severity of any disease that may lead to increased intra-abdominal pressure (i.e., chronic obstructive pulmonary disease) as well as have a negative effect on postoperative wound healing (i.e., diabetes mellitus). Specifically, before laparoscopic IHR, we require all overweight and obese patients with a body mass index greater than or equal to 30 kg/m2 to attempt to lose weight, we require all actively smoking patients to quit smoking for at least 6 weeks before surgery, and we engage in preoperative optimization with respect to each patient's nutritional status and control of their associated medical comorbidities.
Surgical Technique
This section highlights the key steps to performing laparoscopic IHR, as performed at our institution. While both TAPP repair and total extraperitoneal repair (TEP) are considered laparoscopic forms of IHR, we focus on laparoscopic TAPP repair only. It is important for any surgeon performing laparoscopic TAPP IHR to recognize that the learning curve for either laparoscopic TAPP or TEP IHR is longer compared with the learning curve for open IHR. 3 In fact, in a recent study by Merola et al., they noted that proficiency in open IHR was achieved after ∼40 open IHRs, which is in stark contrast to the 250 repairs referenced in the VA Cooperative Study for laparoscopic IHR.6,16 We recognize that there may be variation in the technical aspects of this procedure and we recommend that variations to the steps below be adopted by surgeons as needed in an effort to maximize both patient safety and surgeon comfort. 17
Routine preoperative interventions are performed, including the administration of preoperative antibiotics and the placement of sequential compression devices as recommended by the Surgical Care Improvement Project (SCIP) guidelines. The administration of chemical deep venous thrombosis (DVT) prophylaxis should be determined based on patient-specific risk factors for DVT formation. We do not routinely administer chemical DVT prophylaxis due to proximity of the surgical dissection to the iliac, femoral, and epigastric vessels. However, if chemical DVT prophylaxis is not administered, it is important that pneumatic compression devices are placed on the patient's legs before induction of general anesthesia.
Patients are placed supine on the operating room table.
General anesthesia is induced and all groin hair is removed with surgical clippers. We selectively perform Foley catheterization of the bladder in patients who were unable to successfully void before being brought back to the operating room.
Both arms are tucked, taking care to adequately pad the elbow and other pressure points.
Access to the abdominal cavity is achieved in an open manner at the umbilicus through a Hasson technique.
We place three ports: one 12 mm Hasson port at the umbilicus, one 5 mm port along the lateral aspect of the ipsilateral rectus abdominis muscle at least 10 cm lateral and 2–3 cm above the umbilical port, and one 5 mm port along the lateral aspect of the contralateral rectus abdominis muscle at least 10 cm lateral and in line with the umbilical port (Fig. 1). If a bilateral inguinal hernia is planned for repair, both 5 mm ports are placed in line with the umbilical port (Fig. 2).
Once access to the abdominal cavity is obtained, both groins are thoroughly inspected to confirm the presence of the groin hernia intended to fix as well as any additional inguinal hernia defects (Fig. 3).
A 30° 5 mm laparoscope is used and placed at the ipsilateral 5 mm port. The role of the assistant is vital in helping to create a proper view of the pelvis. A “hot” scissor is used at the umbilical port and a Maryland grasper is introduced through the 5 mm port on the contralateral side of the inguinal hernia.
The ipsilateral anterior superior iliac spine (ASIS) is palpated externally and visualized on the screen. A mental note or actual peritoneal cautery mark can be placed to a site superior and lateral to the ASIS. A high peritoneal flap is then created by grabbing the peritoneum with the Maryland grasper just lateral to the ipsilateral medial umbilical ligament. The peritoneum is scored transversely from medial to lateral to the previously noted site just superior and lateral to the ASIS. For a unilateral IHR, the peritoneal flap is created on the side of the hernia defect only. For bilateral IHRs, the peritoneal flap is created on both the left and right side (Fig. 4).
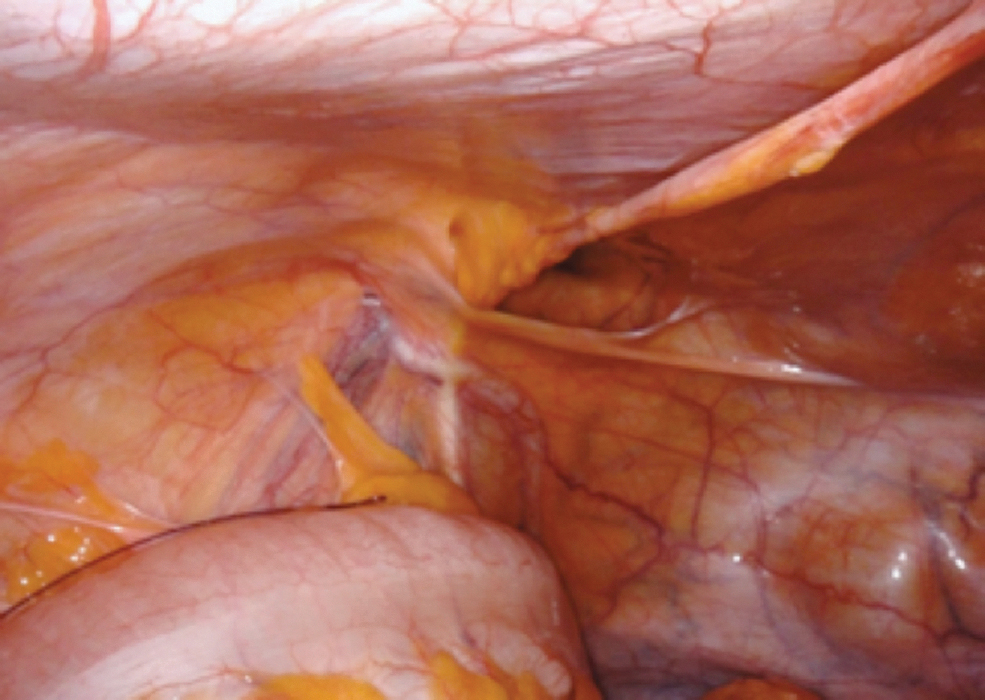
Once the high peritoneal flap is opened, a combination of blunt dissection and electrocautery are used to open the peritoneal flap in the midline from the umbilicus distally to Cooper's ligament (Figs. 5 and 6). The white of Cooper's ligament should be visualized and serves as the landmark for the most distal extent of the preperitoneal dissection.
The peritoneal flap is opened up inferiorly, at least 2 cm below Cooper's ligament into the space of Retzius (Fig. 6). When opening up the peritoneal flap, it is important to ensure that the inferior epigastric vessels remain along the anterior abdominal wall to minimize damage to these vessels or unnecessary hemorrhage (Fig. 7).
Next, the remainder of the peritoneal flap is created laterally. It may occur that the flap dissection is initially started in the retrorectus plane medially and then carried out laterally into the preperitoneal plane. If this occurs, the two planes must be connected by dividing the lateral extent of the posterior rectus sheath until it disappears at the arcuate line (Fig. 8).
The scissors are exchanged for a second Maryland grasper and the preperitoneal space is opened laterally. The peritoneum is grasped with the most lateral grasper and pulled to the lower contralateral corner while the Maryland grasper in the periumbilical port is used to clear off fat and tissue fibers from the peritoneum, working from the most cephalad part of the peritoneal flap toward the internal ring. During this portion of the dissection, it is essential to monitor for and use caution around the gonadal vessels and vas deferens. In addition, care is taken to avoid extensive dissection along the psoas muscle to avoid injury to the nerves.
As the internal ring is approached, the spermatic cord (male patient) or round ligament (female patient) is identified. The peritoneum is carefully dissected away from these structures and any cord lipoma is reduced (Fig. 9).
Additional dissection of the peritoneal flap is performed inferior to the internal ring to ensure adequate mesh overlap and to reduce any future clam-shelling of the mesh. In females, the round ligament is ligated with an energy device at this time, close to the peritoneum, to avoid injury to the overlying nerves. Ligation of the round ligament helps to facilitate future mesh placement.
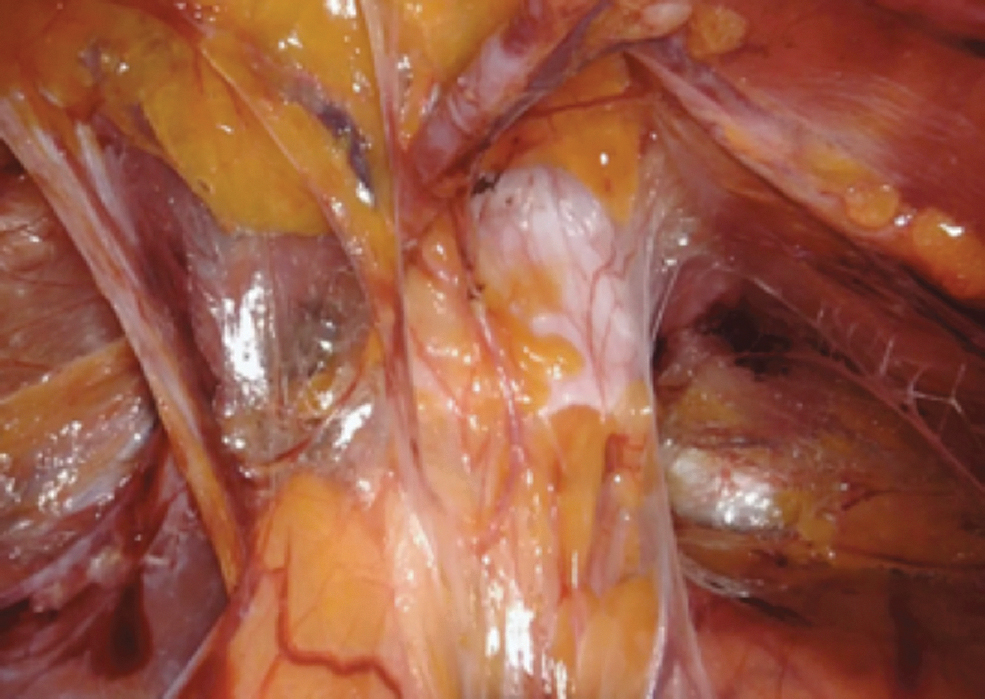
The direct, indirect, femoral, and obturator hernia spaces are identified and inspected. Any hernia is reduced (Figs. 9 and 10).
The preperitoneal space is reinspected to ensure hemostasis and that the flap is large enough to accommodate an ∼10 × 15 cm piece of medium-weight, synthetic mesh. The peritoneal flap is inspected from the abdomen to ensure that there is no tethering of the peritoneal flap to intra-abdominal adhesions or structures, such as the sigmoid colon.
The mesh is introduced through the periumbilical port. The mesh is placed over all hernia spaces with at least 3 cm of overlap superior to the direct hernia space and 3 cm inferior to Cooper's ligament (Fig. 11).
The mesh is secured with a permanent tacking device. Two tacks are placed on Cooper's ligament medially, one tack is placed medially and superior on the anterior abdominal wall, taking care not to injure the inferior epigastric vessels and the other tack is placed lateral and superior on the anterior abdominal wall, taking care not to injure any nerves (Fig. 12).
The peritoneal flap is closed over the mesh, using the same permanent tacking device as was used to secure the mesh. Any holes in the peritoneum should be closed before closing the peritoneal flap to prevent a preperitoneal hernia (Fig. 13).

Location and sizes of ports used for a unilateral laparoscopic TAPP IHR. This image demonstrates a left TAPP IHR. A 12 mm port and two 5 mm ports are used. The 5 mm port placed on the side of the inguinal hernia is placed 2–3 cm above the umbilical port, while the contralateral 5 mm port is placed in line with the umbilical port. All of the ports can serve as working ports. The periumbilical port can also be used for camera placement if a 10 mm camera is used and is the site where the mesh is introduced into the abdominal cavity. IHR, inguinal hernia repair; TAPP, transabdominal preperitoneal.

Location and sizes of ports used for a bilateral laparoscopic TAPP IHR. This image demonstrates a bilateral TAPP IHR. A 12 mm port and two 5 mm ports are used. The 5 mm ports are placed in line with the umbilical port. All ports can serve as working ports. The periumbilical port can also be used for camera placement if a 10 mm camera is used and is the site where the mesh is introduced into the abdominal cavity. IHR, inguinal hernia repair; TAPP, transabdominal preperitoneal.
Thorough inspection of the groin reveals a left direct inguinal hernia.

Development of the peritoneal flap from the periumbilical port site at the median umbilical ligament. This is performed with bipolar cautery attached to laparoscopic scissors through the contralateral 5 mm port with downward traction on the peritoneum by a Maryland grasper through the periumbilical 12 mm port. For the purposes of this picture, a left inguinal hernia repair is being performed.

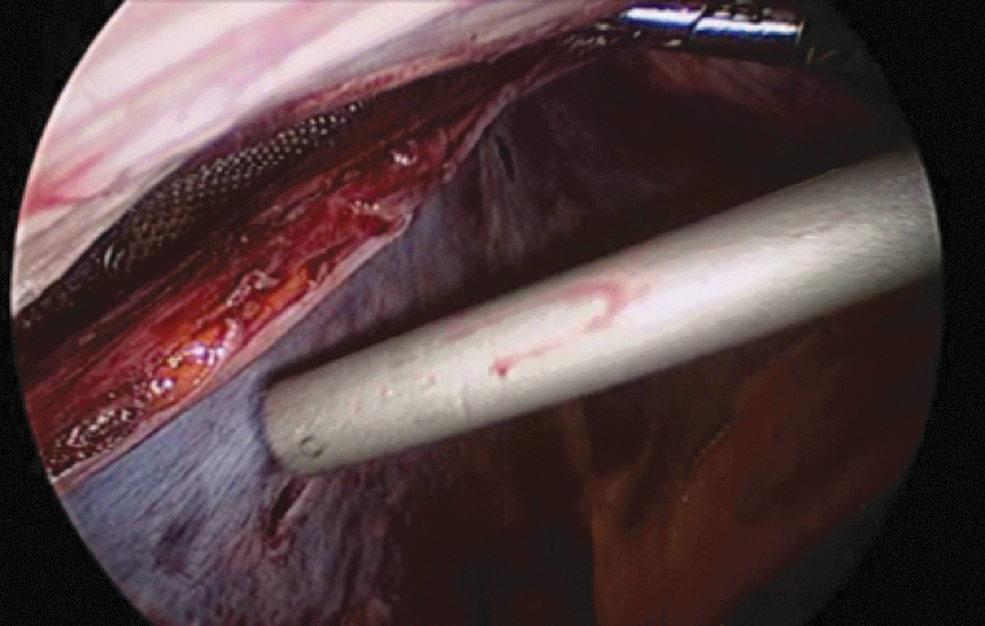
Once the peritoneal flap is started, it must be further opened. To do this, the laparoscopic scissors are placed within the flap and gentle downward pressure toward the patient's spine is applied. Care must be taken to ensure that the epigastric vessels are not incorporated into this blunt move to avoid injury to them. For the purposes of this picture, a left inguinal hernia is being repaired.
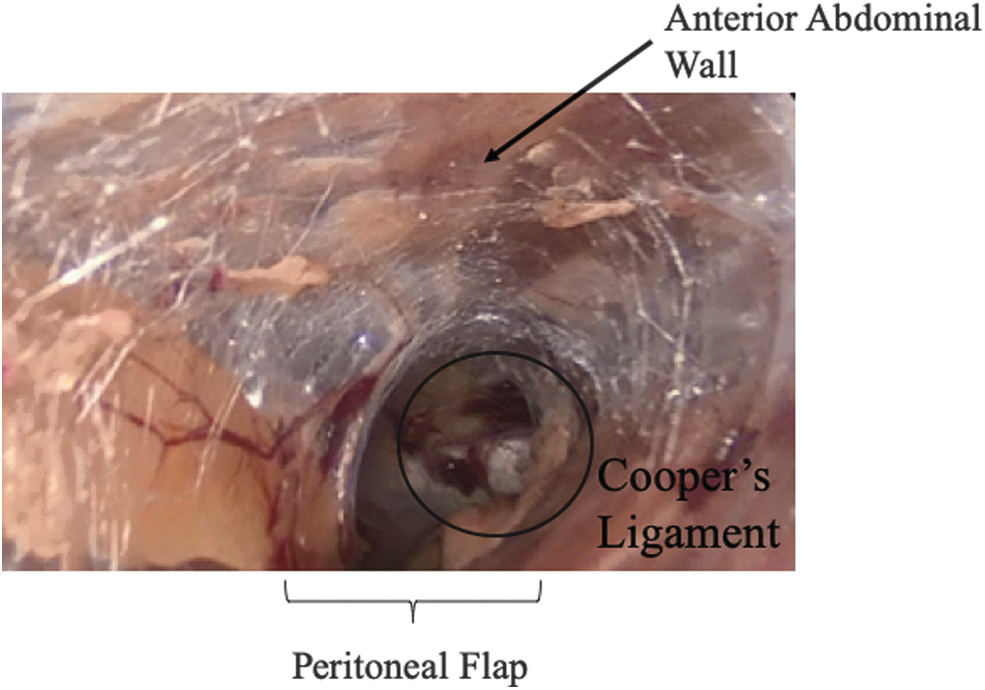
Dissection of the peritoneal flap is carried down medially until Cooper's ligament is identified.
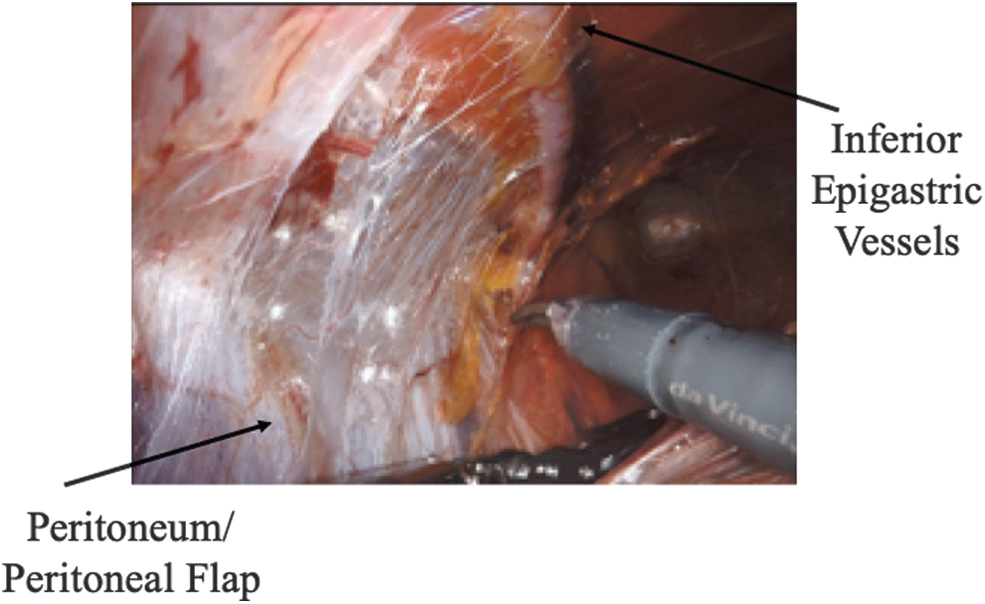
When performing the peritoneal dissection, it is important to ensure that the inferior epigastric vessels remain up on the anterior abdominal wall to minimize the risk of damage to these vessels and serious hemorrhage.
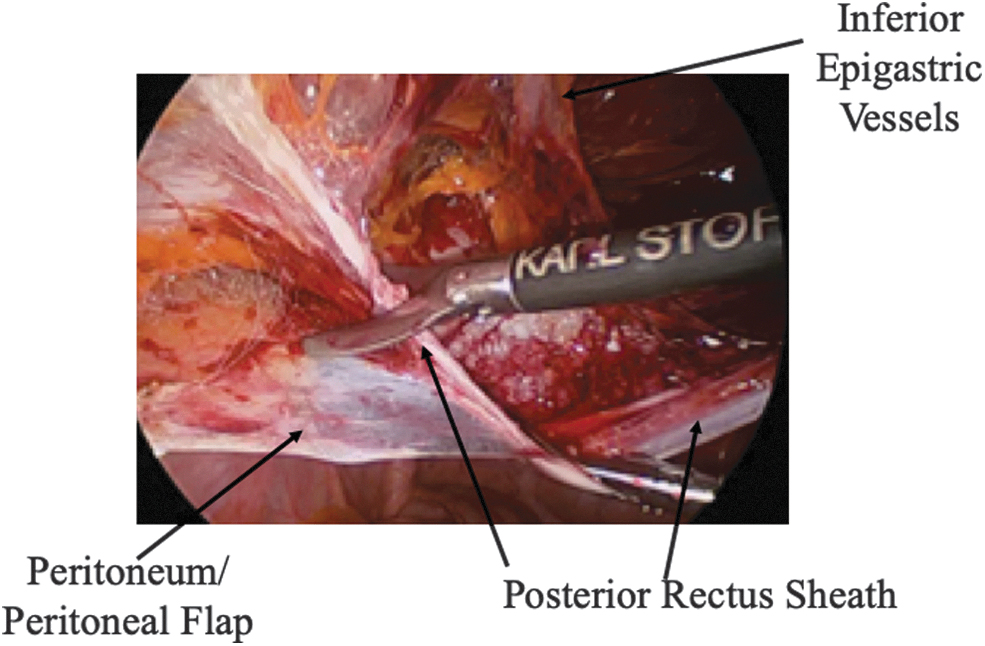
Creation of the peritoneal flap medially can sometimes occur in the retrorectus space rather than in the preperitoneal space. When this occurs, the two spaces must be connected at the arcuate line.
Demonstration of the direct hernia sac, medial to the inferior epigastric vessels.
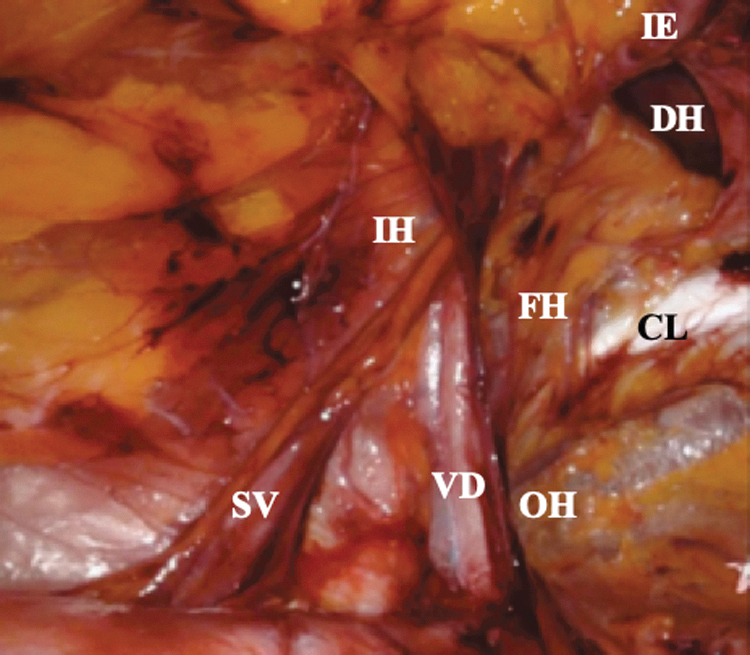
Following reduction of the direct hernia defect, the remainder of the potential groin hernia spaces are evaluated. Here, you can see the direct hernia (DH) along the anterior abdominal wall medial to the inferior epigastric (IE) vessels. Also demonstrated in this picture are Cooper's ligament (CL), the spermatic vessels (SV), and the vas deferens (VS). While not present, the sites of indirect (IH), femoral (FH), and obturator (OH) hernias are also noted.
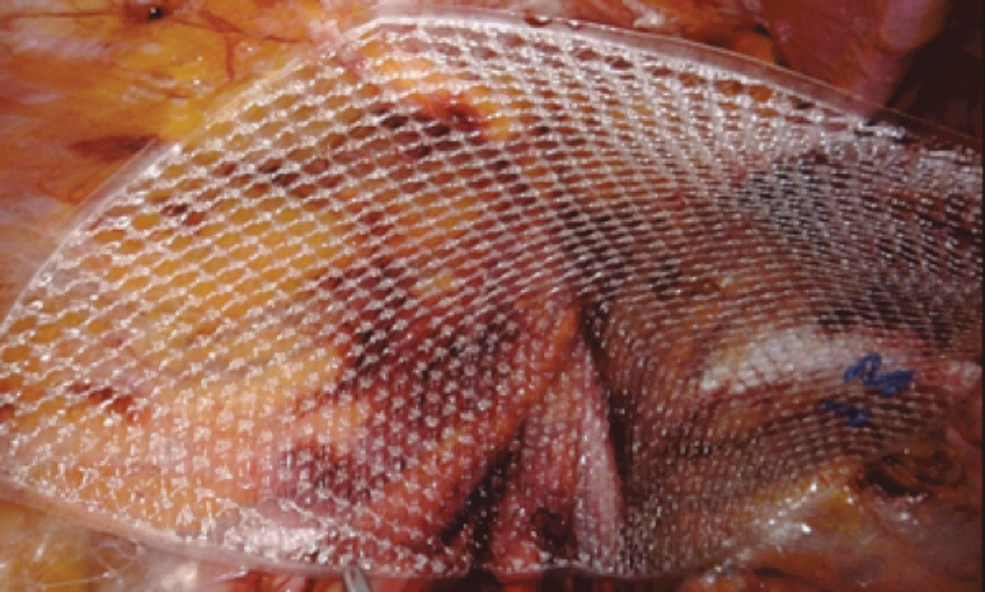
A 10 × 15 cm piece of medium-weight, synthetic mesh has been placed within the preperitoneal space, ensuring adequate coverage of all groin hernia spaces.
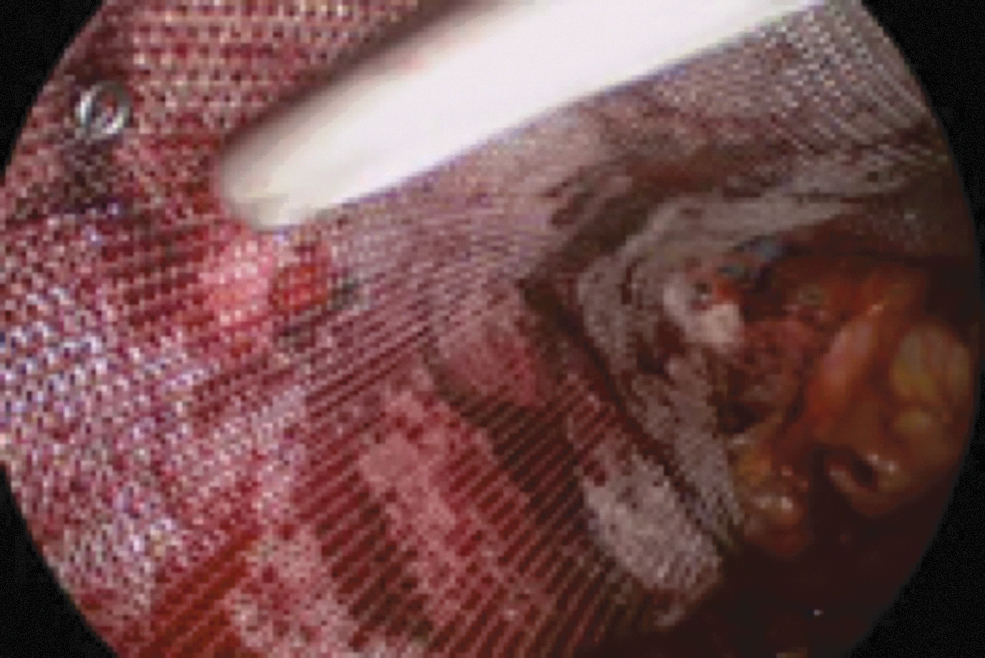
Fixation of the mesh at the superior and lateral site of the preperitoneal flap. Care must be taken not to perform fixation too laterally on the anterior abdominal wall to avoid injury to the nerves.
Closure of the peritoneal flap over the mesh using the same permanent tacking device that was used for mesh fixation.
Postoperative Management and Follow-Up
Postoperatively, the Foley catheter, if present, is removed before the patient emerges from general anesthesia. Patients are transferred to the postanesthesia care unit (PACU) and are routinely discharged to home once they have voided and have met all PACU discharge criteria. Additional details regarding the postoperative management of our patients are as follows:
Postoperative pain management. We follow the recommendations provided by the Americas Hernia Society Quality Collaborative (AHSQC) regarding the management of postoperative pain following IHR.
18
Specifically, patients are instructed to place a cold compress at the site of their surgery for the first 24 hours postoperatively. Patients are also instructed to take acetaminophen and ibuprofen around the clock for the first 3 days postoperatively. Patients are provided with six tablets of oxycodone 5 mg with instructions to take every 4–6 hours if they have persistent pain that is not relieved by the other interventions described above. With the exceptions of patients with chronic pain, none of our patients has had issues with the above postoperative pain management regimen. We believe that the key to successful postoperative pain management with minimization of narcotic pain management is based on thorough patient counseling as to pain expectations and management postoperatively during the preoperative visit. Postoperative follow-up. Patients are instructed to return to clinic for a routine postoperative appointment within 2 weeks of their inguinal hernia surgery. At that time, if patients are without evidence of wound healing issues or other concerns, such a large/symptomatic hematoma or seroma or concern for an inguinal hernia recurrence, patients are instructed to follow-up on an as-needed basis. For patients who have either a large/symptomatic hematoma or seroma, they are instructed to return to clinic on a weekly basis until the hematoma/seroma is almost fully resolved. We prefer not to perform percutaneous aspiration or drain placement into a postoperative hematoma or seroma to minimize the risk for mesh infection. For patients in whom an inguinal hernia recurrence is suspected, either a groin ultrasound or pelvic CT scan is obtained for further evaluation. Postoperative physical activity. Patients are instructed to perform activities of daily living and limiting lifting to five to 10 pounds until their postoperative clinic appointment. At that time, if a patient is without postoperative issues, they are cleared for light activity, including walking on the treadmill and lifting up to twenty pounds. Patients are asked to refrain from heavy lifting or aerobic exercise until 6 weeks postoperatively.
Conclusions
IHR is one of the most commonly performed general surgery operations. There are many surgical approaches to the repair of a groin hernia, including the laparoscopic TAPP approach, as described in this article. It is our intention that this article serves as a guide to the perioperative management of patients undergoing laparoscopic TAPP IHR. While we recognize that there will be some variation in the surgical technique, the key steps described in this article are essential to producing long-term and durable outcomes following laparoscopic TAPP IHR.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.