
Abstract
More than 350,000 ventral hernias are repaired annually in the United States. Currently, there is significant variation in all aspects of ventral hernia management, from preoperative patient selection to postoperative care. Herein, we detail our perioperative evaluation and management of patients selected for laparoscopic ventral hernia and our surgical technique for the performance of laparoscopic ventral hernia repair.
Introduction
Ventral hernia repair (VHR) is one of the most commonly performed general surgery operations.1–4 Nevertheless, VHR lacks standardization in all phases of perioperative care.1–4 The laparoscopic approach to VHR was introduced in 1993. Since that time, several studies have shown that laparoscopic VHR is both safe and effective.1,5–9 More recently, laparoscopic VHR has been shown to have a decreased rate of postoperative wound events and hospital length of stay compared to open VHR.10–13 Cumulatively, these studies emphasize that patient selection and a tailored approach is the most important factor in predicting outcomes following VHR. Herein, we detail our approach to patient selection, surgical technique, and postoperative management of patients undergoing laparoscopic VHR.
Preoperative Evaluation and Patient Selection
There are surgeon, patient, and hernia-specific factors that must be considered when deciding the type of VHR technique that is most appropriate for a specific patient. In a recent article by Kockerling et al., they note that the complexity of abdominal wall hernia surgery continues to increase. 14 In response to the increased complexity of this disease process, they recommend additional specialty training in order for general surgeons to feel comfortable with the specific challenges associated with abdominal wall hernia surgery. This recommendation is consistent with the current value-based health care market landscape in the United States.14–16 Unfortunately, while the learning curve for proficiency with laparoscopic inguinal hernia repair has been well studied, there are currently no studies that have investigated the learning curve for laparoscopic VHR. 14 Therefore, our recommendation is that surgeons who choose to perform laparoscopic VHR have received training in this surgical technique and they feel as confident in producing a durable hernia repair using laparoscopy as they do performing an open VHR.
Patient factors, including patient medical comorbidities, must be thoroughly reviewed. Most commonly, laparoscopic VHR is performed under general anesthesia. Therefore, patients who cannot tolerate general anesthesia due to their associated medical comorbidities are not candidates for laparoscopic VHR. In terms of additional patient factors that may contribute to increased morbidity and mortality following laparoscopic VHR, we use the risk factors previously identified by the Ventral Hernia Working Group to aid in our preoperative discussions. 17 Specifically, a patient's weight, smoking status, nutritional status, and severity of any disease that may lead to increased intra-abdominal pressure (i.e., chronic obstructive pulmonary disease) as well as have a negative effect on postoperative wound healing (i.e., diabetes mellitus) are discussed with the patient before surgical repair of their ventral hernia. To facilitate this discussion and to encourage preoperative patient optimization, we use the Outcomes Reporting App for Clinician and Patient Engagement (ORACLE) tool, which is available at www.ahsqc.org. 18 If a patient does not require emergent and/or urgent surgery, we encourage patients to lose weight, abstain from smoking for at least 6 weeks before surgical intervention, and optimize their medical comorbidities. While we recognize that improvement in medical comorbidities is quite vague, there are currently no specific studies that have identified threshold cut-points for many of the medical comorbidities that impact VHR outcomes.
The hernia-specific factors that are considered before laparoscopic VHR include emergent versus elective repair, size and location of the hernia, the number and type of previous VHRs, any previous component separation repairs, the type and location of previous mesh placement, and number of previous abdominal surgeries. For these hernia-specific factors, we consider patients appropriate for laparoscopic VHR if
Size of the hernia defect is <7 cm on cross-sectional imaging.19,20
Location of the hernia along the anterior abdominal wall that facilitates at least 3 cm of mesh overlap of the hernia defect. 19 For ventral hernias that are in unique locations, including the subxiphoid and suprapubic region, mesh fixation and overlap will often necessitate a preperitoneal open or robotic surgical approach.
Previous hernia mesh placement will not affect the ensuing repair, i.e., the mesh is either not in the intraperitoneal position or if intra-abdominal, was either an absorbable mesh or can easily be removed laparoscopically.
Prior surgical history does not suggest the need for substantial adhesiolysis. Caution should be taken for patients with previous intra-abdominal catastrophes, open abdomens, or multiple previous abdominal operations where the operative reports document extensive adhesions.
Patients factors, as highlighted above, are optimized.
Surgical Technique
This section will highlight the key steps to performing laparoscopic VHR, as performed at our institution. For the purposes of this article, we will discuss the laparoscopic VHR with intraperitoneal mesh placement, also known as the intraperitoneal onlay mesh (IPOM) technique. We recognize that there may be variation in the technical aspects of this procedure and we recommend that variations to the steps below be adopted by surgeons as needed in an effort to maximize both patient safety and surgeon comfort.
Routine preoperative interventions are performed, including the administration of preoperative antibiotics and the administration of chemical deep venous thrombosis prophylaxis, as recommended by the Surgical Care Improvement Project Guidelines. All patients receive universal decolonization against methicillin-resistant Staph aureus (MRSA) with 5 days of nasal mupirocin preoperatively. Patients are not routinely instructed to perform preoperative chlorhexidine scrub or to undergo mechanical bowel preparation, as both of these interventions have been associated with an increased risk of postoperative wound events.21,22 Finally, patients with a known history of MRSA wound infection receive preoperative antibiotics that cover MRSA.
Patients are placed supine on the operating room table.
General anesthesia is induced and all hair from xiphoid to pubis is removed with surgical clippers. For patients with a hernia at or below the umbilicus, a Foley catheter is placed to decompress the bladder and to minimize the risk of bladder injury during mesh fixation.
Both arms are tucked, taking care to adequately pad the elbow and other pressure points.
Access to the abdominal cavity is achieved based on surgeon preference, either through an open cut-down technique or Veress needle with subsequent optical entry in the left upper quadrant. For periumbilical ventral hernias, we prefer to insufflate with a Veress needle and then gain access using an optical entry 5 mm trocar in the left subcostal area along the rectus abdominis muscle as this area is least likely to have intra-abdominal adhesions and is far enough away from the hernia to facilitate adequate mesh overlap and fixation.
The patient is slightly flexed to maximize the space between the subcostal margin and the anterior superior iliac spine.
We place two additional ports: one 12 mm slightly more lateral to the 5 mm optical entry trocar on the left side of the mid-abdomen and 5 mm port in the left lower quadrant below the umbilicus within the same plane as optical entry trocar (Fig. 1). Two additional 5 mm ports can be placed on the lateral aspect of the contralateral side of abdomen if necessary, such as when extensive adhesiolysis is required or when a larger piece of mesh is better secured from the contralateral side.
A 30° laparoscope is used to adequately asses the abdominal wall. The anterior abdominal wall is then cleared of any omental and/or intestinal adhesions and the hernia defect and its contents are isolated. Any previous intra-abdominal mesh is removed if possible. The falciform ligament and the median/medial umbilical ligaments are also often taken down in order a flat-lying mesh with adequate overlap of the ventral hernia defect (Figs. 2 and 3).
The ventral hernia is evaluated. If the hernia contains omentum only, a combination of blunt dissection and electrocautery is used to reduce the hernia. If the hernia contains bowel, sharp dissection only is used to reduce the hernia. Exterior downward pressure on the anterior abdominal wall can be applied to help reduce the hernia (Fig. 4).
The hernia defect is then evaluated and the peritoneum cleared from the fascial edges.
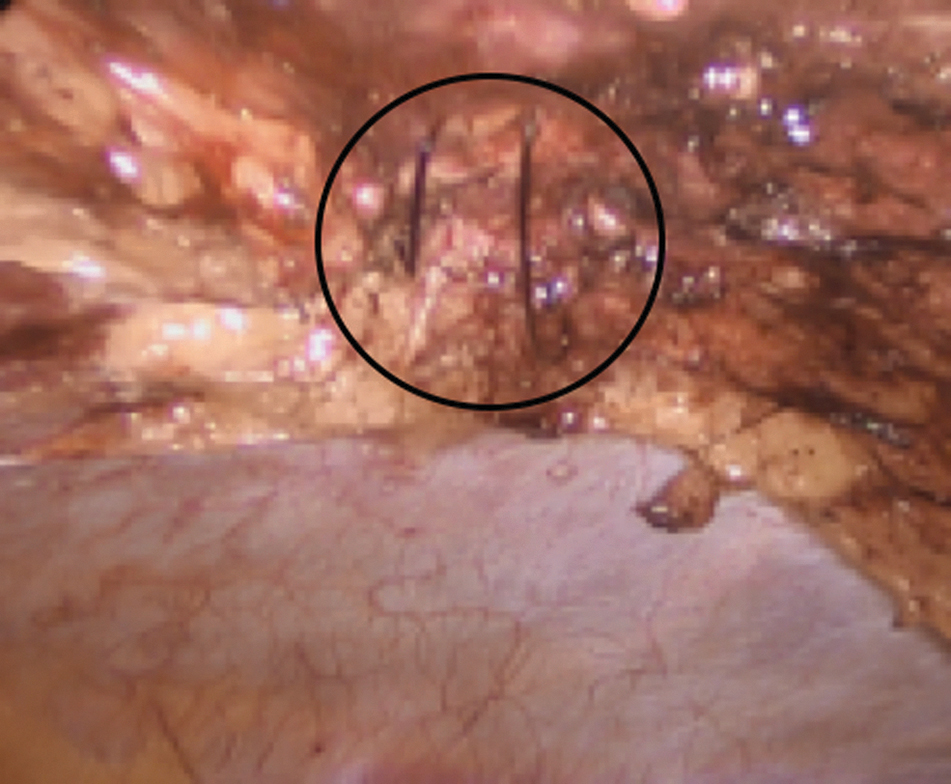
The size of the hernia defect is measured. We perform this by using transabdominal spinal needles to outline the edges of the fascia intra-abdominally. The defect is then measured intra-abdominally using a ruler (Figs. 5 and 6).
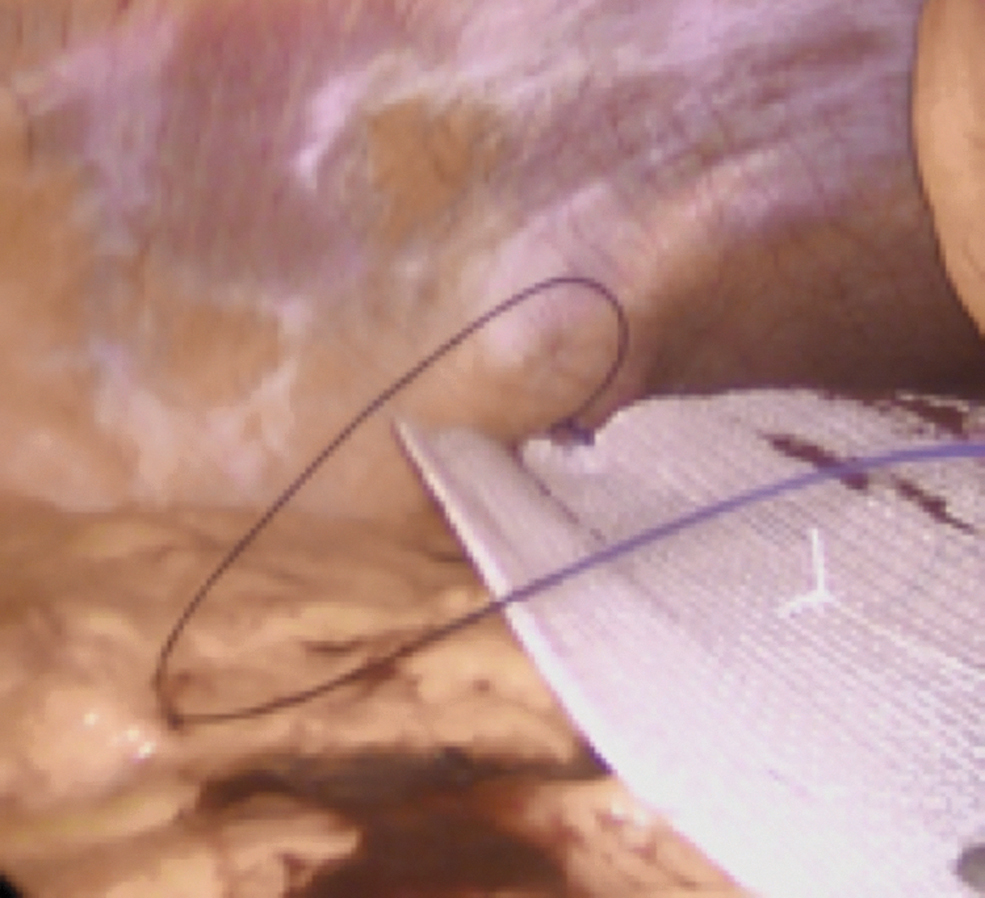
The hernia defect is then closed with a slowly absorbable suture using a “shoelacing” technique as first described by Orenstein et al., by placing sequential figure-of-eight sutures with a laparoscopic suture passer through stab incisions in the skin. 23 The pneumoperitoneum is decreased to 10–12 mmHg before closing the ventral hernia defect (Figs. 7 and 8).
An appropriately sized mesh is chosen. Although 3 cm of mesh overlap is recommended, we prefer a mesh overlap of 4–5 cm in all directions. We use a coated synthetic mesh for laparoscopic IPOM VHR. While the type of mesh used will ultimately depend on surgeon preference and what is available at a particular institution, it is important that no uncoated synthetic meshes are placed in an IPOM location due to the increased risk of enterocutaneous fistula formation.
The mesh is prepared on the backtable. To minimize the risk of mesh infection, we do not open the mesh until this part of the operation. We also ensure that the mesh is prepared on a clean towel. A previously unused marker is used to draw lines across the vertical and horizontal midlines along the coated side of the mesh. A 3-0 vicryl suture is then placed in the center of the mesh. A #1 polydioxanone (PDS) suture is secured to the superior and inferior aspects of the mesh. The sutures are placed on the uncoated side of the mesh.
The mesh is introduced into the abdominal cavity and centered over the hernia defect by introducing the laparoscopic suture passer through the middle of the now closed hernia defect. The vicryl suture is grasped and the mesh raised toward the anterior abdominal wall (Figs. 9 and 10).
The mesh is aligned in a vertical direction along the previous markings on the coated side of the mesh. The PDS sutures are pulled through the anterior abdominal wall using a laparoscopic suture passer and secured on the anterior abdominal wall (Fig. 11). During this step of the procedure, it should be ensured that the mesh is taut and the intra-abdominal insufflation pressure is again decreased to 10–12 mmHg.
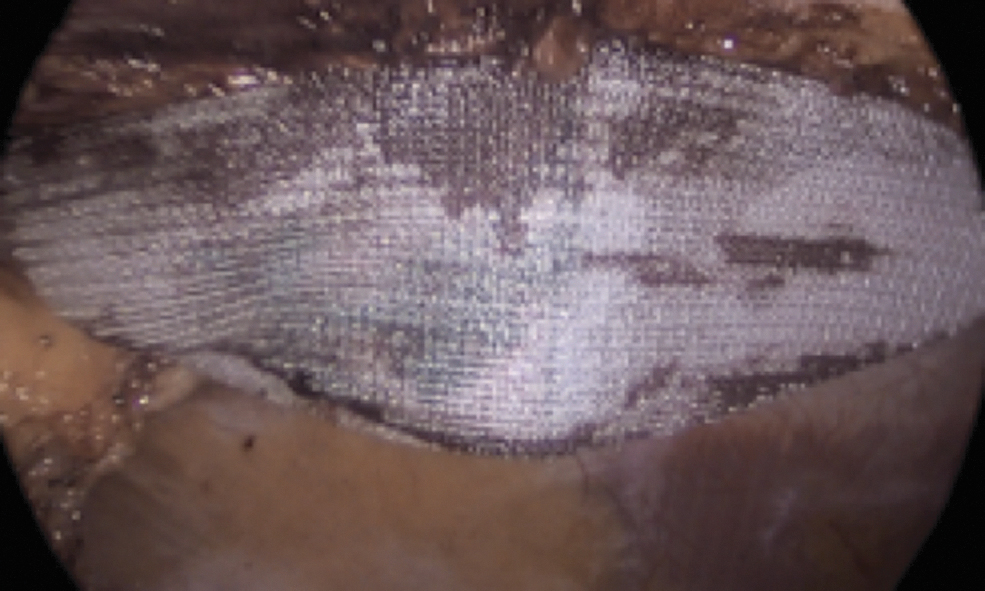
Additional fixation of the mesh is then performed using a permanent tacking device (Fig. 12). By placing the initial tacks at the previously marked lateral midlines, wrinkling of the mesh can be reduced. Two rows of fixation are placed (Fig. 13). During this step of the procedure, the intra-abdominal insufflation pressure is kept at 10–12 mmHg and adequate external counterpressure is ensured to reduce any mesh wrinkling.
Bilateral transabdominal preperitoneal (TAP) blocks are performed for postoperative pain control.
The 12 mm port site is closed, the abdomen is desufflated, and all trocars are removed under direct vision.
All incision sites are closed with subcutaneous sutures and skin glue is placed. If a periumbilical hernia is fixed, a pressure dressing using gauze and a clear adhesive bandage are used. An abdominal binder is placed for external compression.
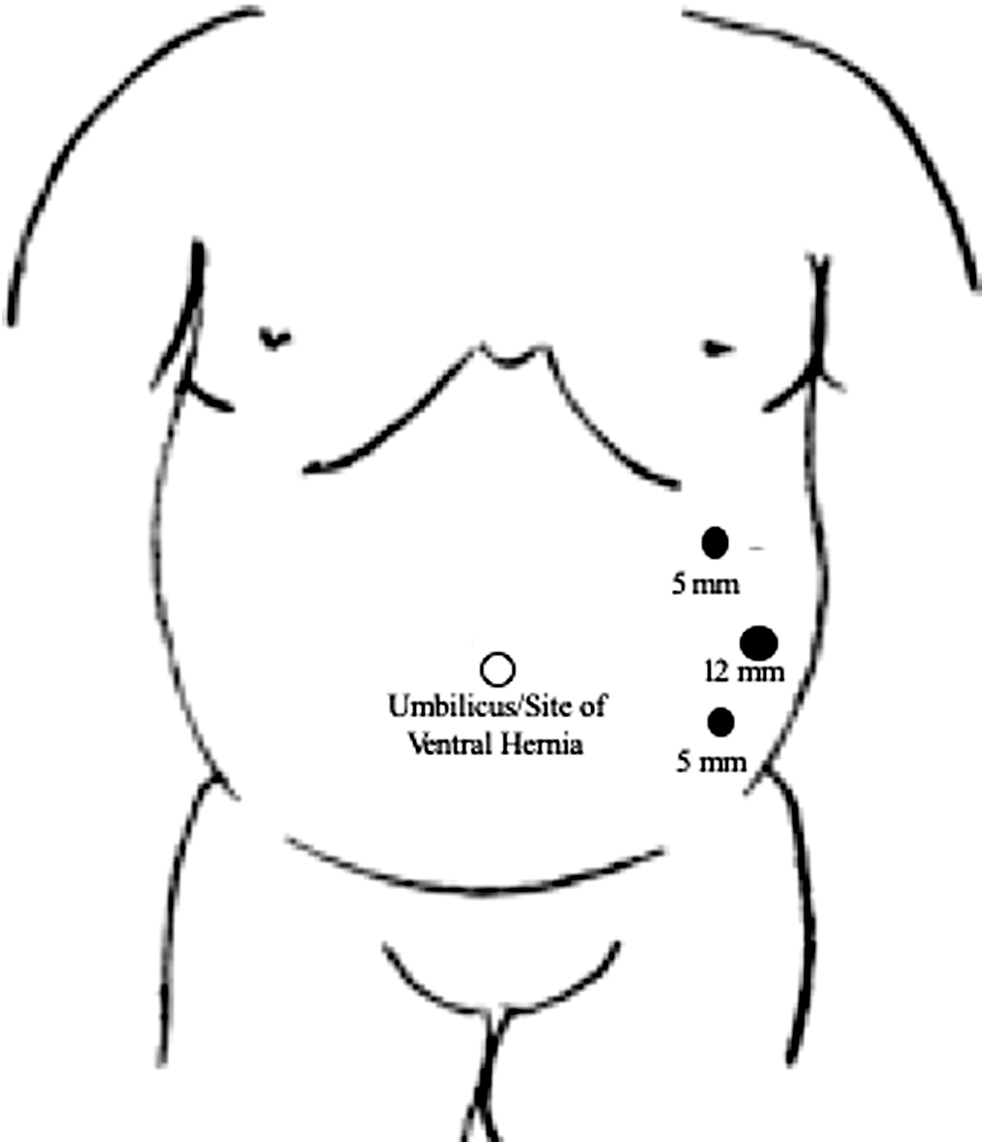
Location and sizes of port used. All of the ports can serve as working ports and locations for camera placement. The 12 mm port can be used for removal of the hernia sac (when performed) and for introduction of the mesh. If needed, two additional 5 mm ports can be placed on the right side of the abdomen lateral to the rectus abdominis muscle.
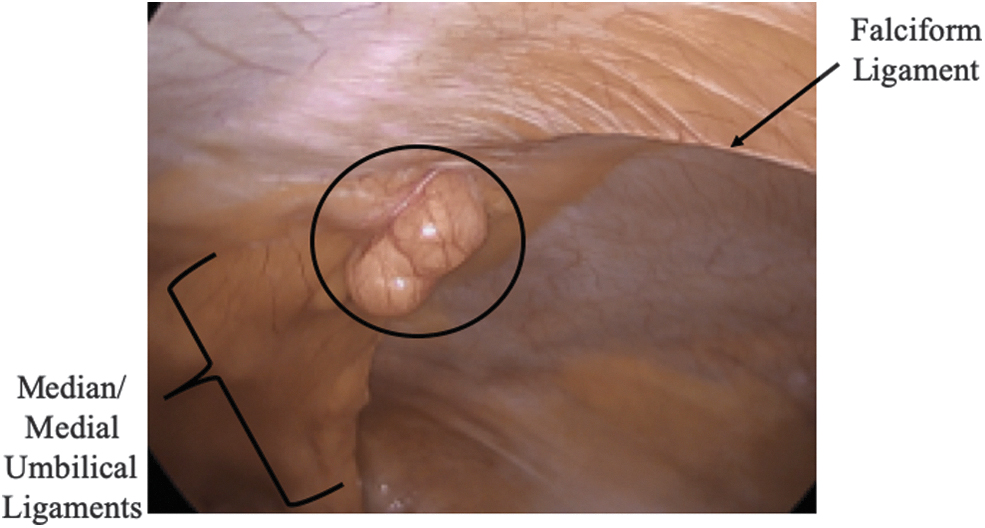
After entrance into the abdominal cavity, the ventral hernia is identified. The location of the ventral hernia relative to the falciform ligament and the median and medial umbilical ligaments is noted. Furthermore, an intra-abdominal adhesion or previous intra-abdominal mesh placement and location is also noted at this time.

To facilitate adequate mesh overlap of the ventral hernia defect, the falciform ligament is taken down with a “hot” scissors.

Gentle external downward pressure is placed on the hernia defect to facilitate complete reduction of the hernia contents. Notice that the falciform ligament and the median/medial umbilical ligaments have also been partially taken down to ensure that the mesh lays flat along the anterior abdominal wall.

Two 20-gauge spinal needles are used to outline the width of the ventral hernia defect.

A ruler is placed into the abdomen and the insufflation pressure is dropped to 10–12 mmHg to accurately measure the width of the ventral hernia. Here, the ventral hernia measures ∼2.5 cm.

Closure of the ventral hernia defect is performed using a “shoelacing” technique, with the assistance of a laparoscopic suture passer. Slowly, absorbable suture is used for closure of the ventral hernia defect.
Demonstration of the “shoelacing” technique, which results in a figure-of-eight stitch to aid in closure of the ventral hernia defect.
The mesh is introduced into the abdomen, taking care to place the coated side toward the abdomen and the uncoated side toward the anterior abdominal wall.

The middle vicryl suture is grasped using a laparoscopic suture passed through the middle of the hernia defect and the mesh is raised toward the anterior abdominal wall.
The transfascial sutures are placed at the superior and inferior aspects of the mesh to ensure that the mesh is taut against the anterior abdominal wall.

The first row of permanent tacks is placed. This picture demonstrates the use of external perpendicular pressure to ensure that the tacks are secured to the abdominal wall and to help keep the mesh flat.

A second row of permanent tacks is used to secure the intraperitoneal onlay mesh. Of note, less tacks are used in the second row than in the first (outside) row of tacks.
Postoperative Management and Follow-up
Postoperatively, if a Foley catheter was placed preoperatively, it is removed before the patient emerges from general anesthesia. Patients are transferred to the postanesthesia care unit (PACU). The decision to discharge the patient from the PACU or to admit the patient for overnight observation depends on the size of the hernia defect and the extent of adhesiolysis performed. Patients with smaller hernia defects (<4 cm) with minimal adhesiolysis are routinely discharged from the PACU. These patients must void before discharge and must meet all other PACU discharge criteria.
At the patient's preoperative appointment as well as in the preoperative area before surgery, a thorough discussion is had with patients in regard to pain control. Patients are also provided with written instructions to review at their preoperative appointment and at the time of discharge from either the PACU or the hospital floor. In addition to the bilateral TAP blocks, patients are encouraged to place intermittent cold packs directly over the surgical site the night of surgery. Patients are encouraged to take acetaminophen and ibuprofen, as medically able, every 6 hours in an alternating manner, while awake for the first 3 days postoperatively. It is stressed to patients that narcotic medications are a rescue medication and should only be used when necessary. At the time of discharge, patients are provided with a prescription for no more than 10 pills of narcotic medication. Our practices are consistent with those recommended by the Americas Hernia Society Quality Collaborative. 24
Patients' activities are limited postoperatively to walking and stairs for the first 2 weeks with lifting restrictions of no more than 10 pounds. The use of an abdominal binder is encouraged for the first 2–6 weeks after surgery, depending on the size of the repair. Patients are asked to return to clinic for a routine postoperative visit at 2–4 weeks postoperatively. At that time, patients are asked about how they are doing in general and specific questions related to their postoperative recovery are asked. A thorough physical examination of the surgical sites and site of the previous hernia is performed, evaluating for wound healing issues, hematomas, seromas, or ventral hernia recurrence. If patients are without evidence of any of these issues, they are instructed that they may resume more strenuous physical activity, but to continue to limit their lifting to no more than 20 pounds until 6 weeks postoperatively. For patients who have either a large/symptomatic hematoma or seroma, patients are instructed to return to clinic on a weekly basis until the hematoma/seroma is almost fully resolved. We prefer not to perform percutaneous aspiration or drain placement into a postoperative hematoma or seroma to minimize the risk for mesh infection. For patients in whom a ventral hernia recurrence is suspected, either a groin ultrasound or pelvic CT scan is obtained for further evaluation.
At our institution, we participate in the Americas Hernia Society Quality Collaborative (AHSQC) and our postoperative follow-up is consistent with the timeline outlined by the AHSQC. Specifically, patients are seen within 30 days of surgery. We encourage patients to return at 6 months postoperatively, at 1 year postoperatively, and annually thereafter, but this rarely occurs for asymptomatic patients. Postoperative wound events are defined as recommended by Haskins et al. 2 Ventral hernia recurrence is determined either by physical examination or by the ventral hernia recurrence inventory. 25
Conclusions
Laparoscopic VHR is a safe and effective approach to the management of many abdominal wall hernias. It is our intention that this article will serve as a guide to the perioperative management of patients undergoing laparoscopic VHR. While we recognize that there will be some variation in the surgical technique that we have described, rigorous patient selection, preoperative optimization, and the key steps to performing laparoscopic VHR as detailed in this article are essential to producing sound 30-day outcomes and long-term hernia repair durability.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.