
Abstract
Although the results of a laparoscopic repair of a paraesophageal hernia are convincing and accepted, controversies still persist regarding indications for elective repair, the need for a concurrent fundoplication, the use of mesh, and the need for a Collis gastroplasty. This article is a description of our surgical approach to the patient with a paraesophageal hernia in need of a repair.
Introduction
Although the results of a laparoscopic repair of a paraesophageal hernia are convincing and accepted, controversies still persist regarding indications for elective repair, the need for a concurrent fundoplication, the use of mesh, and the need for a Collis gastroplasty.
Historically, the diagnosis of paraesophageal hernia mandated operative management. The risk of incarceration was thought to outweigh the operative morbidity, and patients were offered surgical management regardless of their presentation. This treatment paradigm shifted in the early 2000s with a landmark study by Stylopoulos et al., 1 where the authors demonstrated that the risk of emergency surgery and mortality following urgent operations for minimally symptomatic patients managed nonoperatively were significantly overestimated. In fact, watchful waiting for asymptomatic elderly patients resulted in a significant improvement in quality-adjusted life-years compared to those offered operative management using the proposed Markov decision model. Following this report, watchful waiting became the new standard of care for patients presenting with incidentally found or minimally symptomatic paraesophageal hernias. Newer studies suggest that the incidence of truly asymptomatic paraesophageal hernias is likely overestimated, with most patients, particularly in the setting of chronic hernias, subscribing to mild but tolerable symptoms when probed more carefully. 2 Furthermore, some patients may present with atypical symptoms, not generally ascribed to symptomatic hernias, including asthma, respiratory symptoms, and anemia. 3
While the need for antireflux surgery in addition to paraesophageal hernia repair has been debated, most surgeons perform a 360° fundoplication as it is both therapeutic and preventative for the development of gastroesophageal reflux. The extensive dissection and destruction of some of the continence mechanisms of the gastroesophageal junction accounts for this phenomenon and is properly restored by the total fundoplication. Casabella et al. reported that over 65% of patients who did not undergo a fundoplication developed reflux symptoms following their hernia repair. 4 The utility of partial fundoplications is mostly relevant in the setting of known esophageal dysmotility, or in emergencies. In this case, both a posterior 270° Toupet fundoplication and a Dor 180° fundoplication are considered acceptable as an antireflux procedure. 5
The use of mesh in hiatal hernia surgery is controversial. While there are currently inconclusive data regarding the need for mesh during these repairs, the majority of studies favor its use to prevent recurrences and provide tension-free repairs over primary repairs. This is particularly true in the setting of large, chronic hernias in older patients, where the integrity of the diaphragm is questionable. The longevity of this benefit is debatable, as most of these studies have shown only short-term reduction in recurrence rates without any long-term difference when compared to primary repair. However, a meta-analysis by Huddy et al. demonstrated a clear reduction in recurrence rates in mesh versus nonmesh groups (15% versus 25%). 6 Whether synthetic or biologic mesh is superior has not been unequivocally demonstrated in this field is likely variable depending on the presentation of the patient (elective versus emergent). The biggest concern regarding the use of synthetic meshes is the risk of esophageal erosion and perforation, although most studies comparing the two have reported comparable results.
A key component of a paraesophageal hernia repair is mobilizing sufficient length of the distal esophagus to allow for a floppy 360° Nissen fundoplication. This is typically accomplished by adequate mediastinal dissection through a transabdominal approach. The use of Collis gastroplasty, as such, is reserved in the setting of insufficient esophageal length during the mediastinal and transabdominal portion of the dissection. This is typically encountered during redo operations and is therefore not usually a component of a primary hernia repair.
Below is a detailed description of our surgical approach to the patient with a paraesophageal hernia in need of a repair.
Preoperative Assessment
The essential investigations are barium swallow and esophageal manometry, when the patient presents with smoldering symptoms and on an elective basis. The barium swallow shows the presence and size of the hernia, while the manometry excludes the presence of achalasia, which would contraindicate a total fundoplication. During an emergency, when the patient usually experiences an excruciating epigastric pain that moves to the chest, associated with nausea and retching, a computed tomography scan demonstrates an organ-axial volvulus with most of the stomach within the chest. In these cases, the patient should undergo emergent repair that leaves no time for other studies.
Trocar Placement and Instrumentation
The patient lies supine on the operating table in low lithotomy position with the lower extremities extended on stirrups with knees flexed 20°–30°; a bean bag is inflated to avoid sliding of the patient; an orogastric tube is placed to decompress the stomach, when possible; the surgeon stands between the patient's legs, while first and second assistant stand on the right and left side, respectively. A five trocar technique is used for this procedure (Fig. 1); the first trocar is placed 14 cm inferior to the xiphoid process, in the midline, and accommodates a 30° scope; a second trocar is placed in the left midclavicular line, at the same level with the first trocar, to introduce a Babcock clamp used for traction of the distal esophagus and stomach; a third trocar is placed in the right midclavicular line, at the same level of the other two trocars, and it is used for the insertion of a self-retaining retractor to lift the left lobe of the liver; a fourth and a fifth trocar are placed under the right and left costal margins and they are used for the dissecting (bipolar or ultrasonic, per surgeon's preference) and suturing instruments.

Operative setup and trocar placement.
Surgical Technique and Operative Steps
Excluding placement and removal of trocars, we can consider the following very specific steps for this operation:
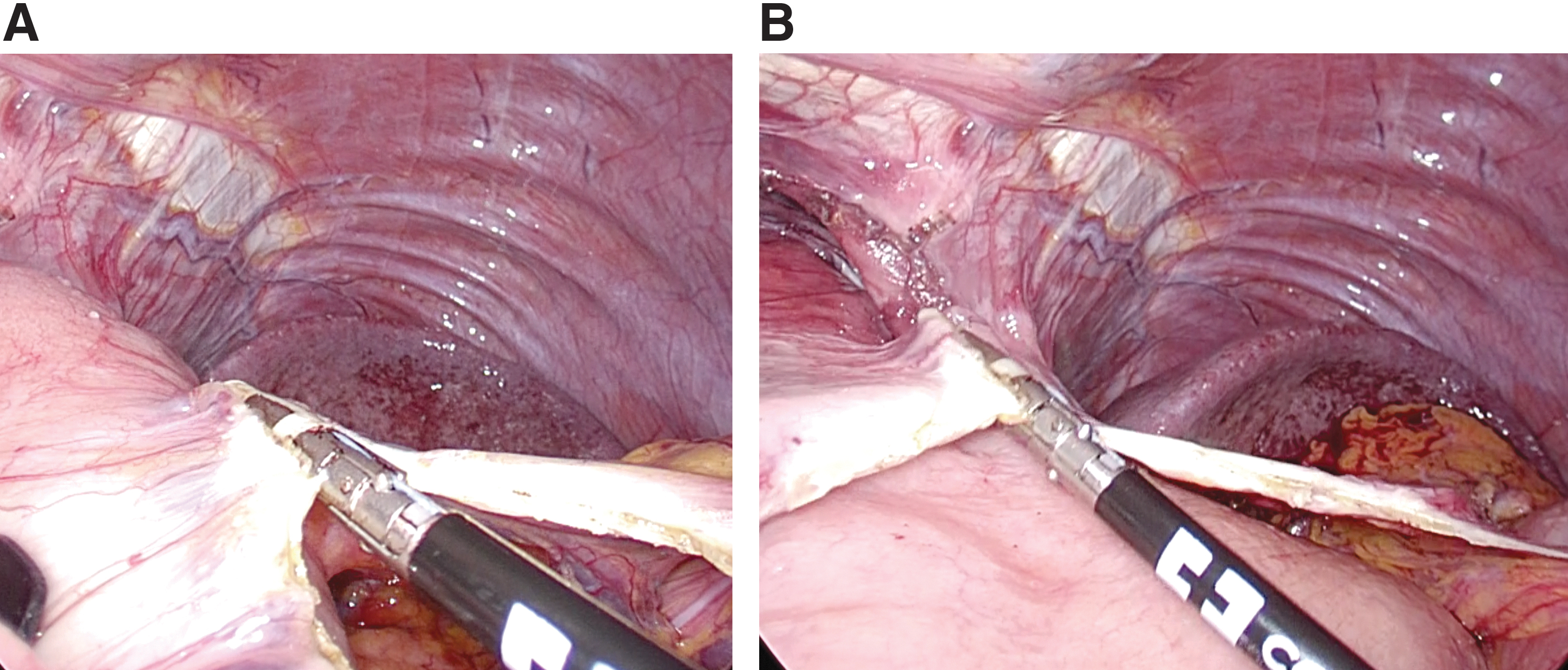
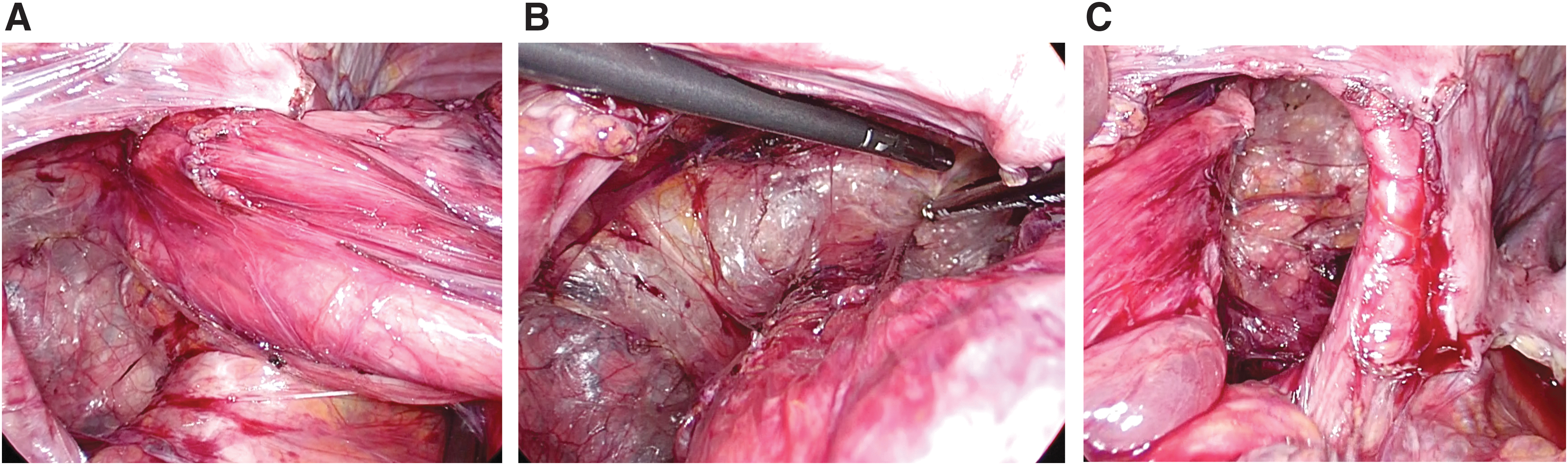
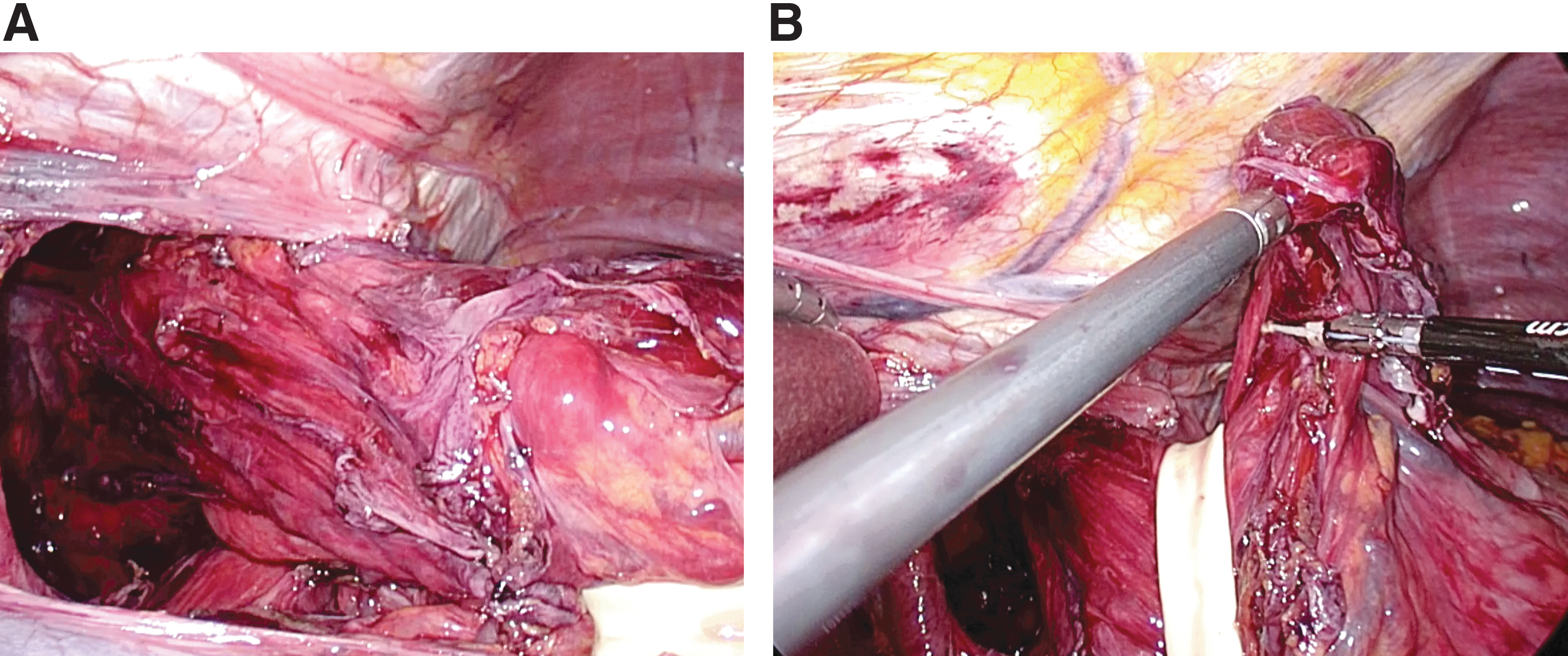
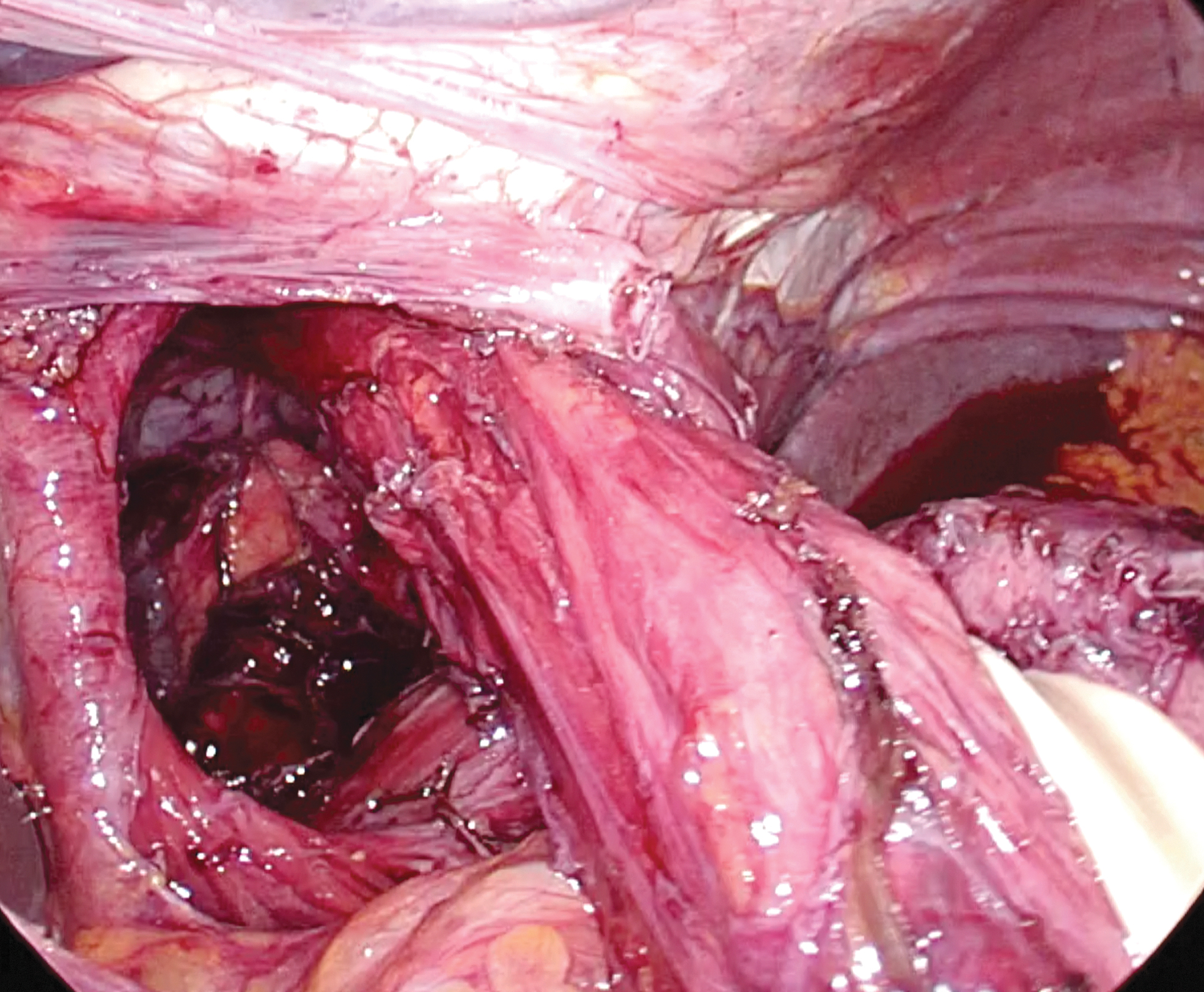
Reduction of the hernia (Fig. 2A, B). Transection of the phrenoesophageal membrane starting from the right pillar of the crus. This allows to grasp the hernia sac, pull it down, and peeling or dissecting it from the posterior mediastinum bluntly or with the help of a dissecting instrument (Fig. 3). The transection of the phrenoesophageal membrane is carried onto the pillar of the left crus (Fig. 4). Transection of the short gastric vessels. This step completes the transection of the sac onto the pillar of the left crus and facilitates the access to the posterior portion of the sac and its mobilization (Fig. 5A, B). Dissection of the posterior mediastinum alongside the esophagus and anteriorly (Fig. 6A–C). At this point, care is taken to further visualize the anterior vagus nerve along its course from the left side of the esophagus. Hernia sac dissection, posterior to the esophagus. This facilitates the creation of the retroesophageal window from which a Penrose drain can be inserted to apply atraumatic traction to the distal esophagus for its mobilization from the mediastinum (Fig. 7A). Care should be taken to identify the posterior vagus nerve and incorporate it within the Penrose drain. The sac is then excised (Fig. 7B). Complete dissection of the posterior mediastinum and esophageal mobilization until the gastroesophageal junction lies 2–3 cm into the abdomen. At this point, care is taken to further visualize the posterior vagus nerve from the left side of the esophagus (Fig. 8). Crural repair with a braided nonabsorbable suture. A “V,” which shows the convergence of both crura, should be clearly defined by a proper dissection before suturing (Fig. 8). This would facilitate the approximation of the crura by the stitches (Fig. 9). Should a mesh be used at this stage, this is usually biologic and placed to buttress the repair, never to bridge it. We favor the use of a mesh in reoperations where the crura are thin because of the dissection of the scar tissue around them. Fundoplication: Although a total fundoplication is the procedure of choice, a partial posterior or anterior fundoplication may be considered during emergencies, when an esophageal manometry cannot be performed. A braided nonabsorbable suture is usually used for suturing. A total fundoplication should be short, 2–3 cm, and constructed with three stitches spaced 1 cm apart using the stumps of the short gastric vessels as markers for the proper orientation (Fig. 10). A bougie (54F–56F) is usually recommended to size the fundoplication. Apical stitches and a posterior gastropexy, both between the crura and the fundoplication, are optional, as they would not replace a proper and complete esophageal mobilization with a thorough mediastinal dissection. After the nasogastric tube is removed, should one could be inserted before the operation, an upper endoscopy is always performed to ensure than the fundoplication has been performed without tension or twisting, or in difficult cases where a perforation is suspected. No drains are placed intrabdominally or in the mediastinum, unless a perforation is suspected. No percutaneous endoscopic or laparoscopic gastrostomy tubes are added, as these adjuncts do not reliably keep the stomach in the abdomen, and they cannot replace a well-executed esophageal mobilization. No nasogastric tube is left in the postoperative period. The Foley catheter is removed in the operating room.
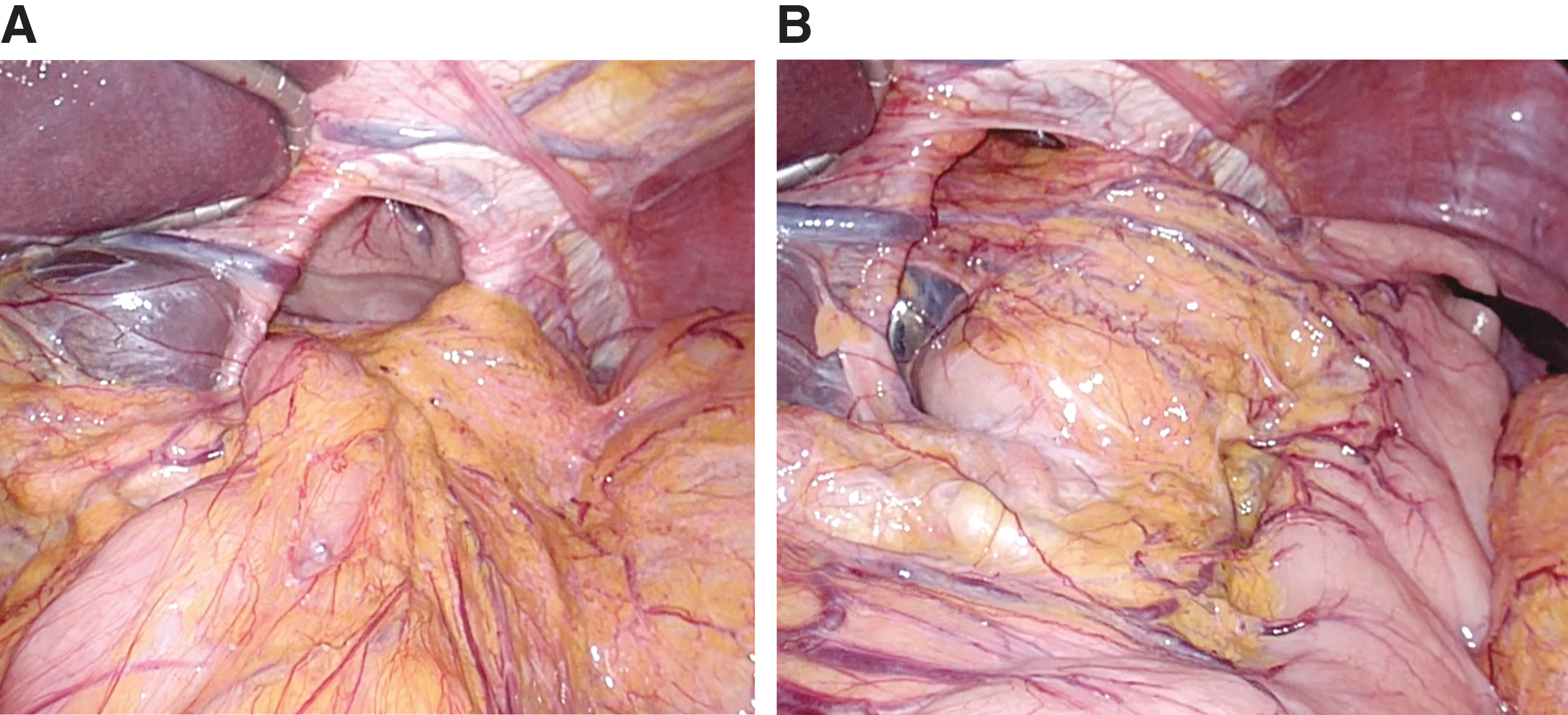
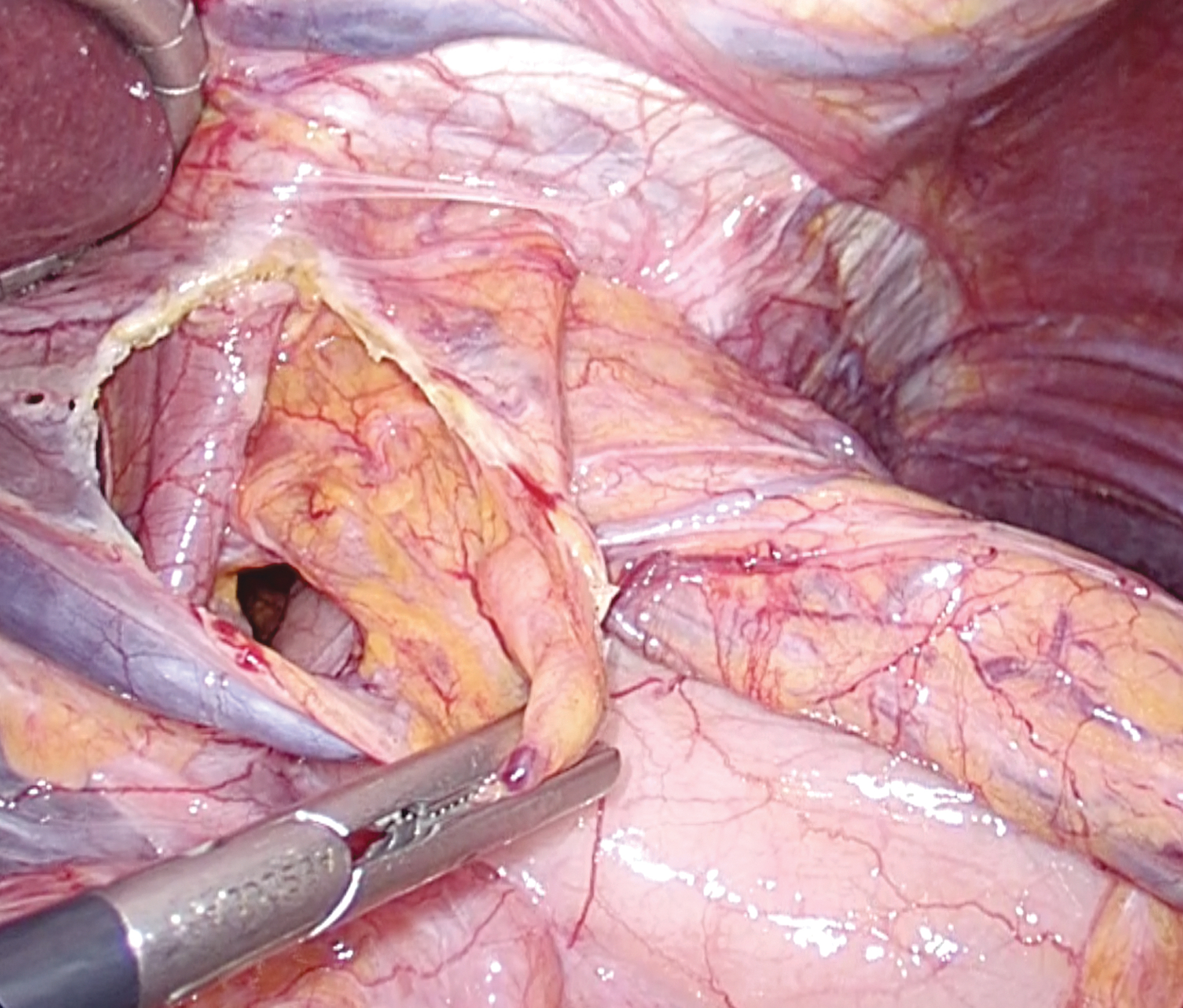
Transection of the phrenoesophageal membrane. This allows to grasp the hernia sac, pull it down, and peeling or dissecting it from the posterior mediastinum bluntly or with the help of a dissecting instrument.

The transection of the phrenoesophageal membrane is carried onto the pillar of the left crus.
Complete dissection of the posterior mediastinum and esophageal mobilization until the gastroesophageal junction lies 2–3 cm into the abdomen. At this point, care is taken to further visualize the posterior vagus nerve from the left side of the esophagus.

Crural repair with a braided nonabsorbable suture. A “V” showing the convergence of both crura, should be clearly defined by a proper dissection prior to suturing.
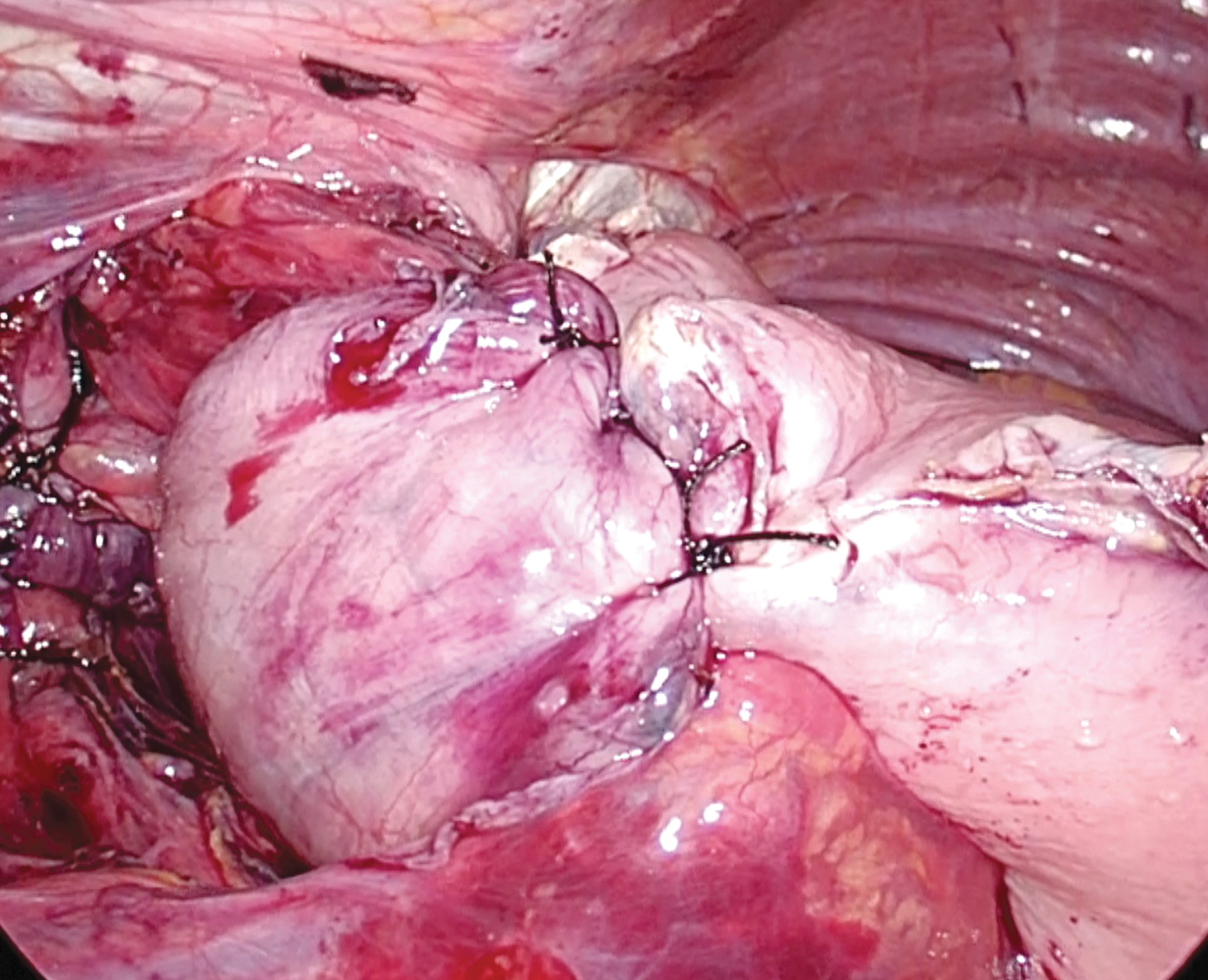
Total fundoplication, short, 2–3 cm, and constructed with three stitches spaced 1 cm apart using the stumps of the short gastric vessels as markers for the proper orientation. A braided nonabsorbable suture is usually used for suturing. A bougie (54F–56F) is usually recommended to size the fundoplication.
Postoperative Management
Antiemetics are routinely prescribed to avoid nausea postoperatively. A complete blood count is ordered in selected cases, when blood loss or a perforation is of a concern. The patient starts a soft diet the morning of the first postoperative day; it is important to avoid meat, bread, and carbonate beverages for 2 weeks, and instructed that a mild degree of dysphagia will be normal, yet, self-limited; the patient is usually discharged within the day after the operation, after breakfast. A barium swallow is obtained postoperatively to assess for any recurrence only if symptoms persist or recur.
Complications
Intraoperative complications are pneumothorax, esophageal or gastric perforation, splenic injury, and vagal nerve injury. Postoperative complications are dysphagia and persistent or recurrent reflux and symptoms. In these cases, a complete diagnostic workup should be performed de novo.
Results
The current standard of care for a paraesophageal hernia repair remains a laparoscopic approach. Compared to the open technique, minimally invasive approaches provide significant reductions in hospital length of stay, postoperative pain, and overall perioperative complications. Many large-volume foregut centers average a hospital length-of-stay of 1–2 days for elective cases following a laparoscopic approach, with minimal postoperative morbidity. The associated morbidity and mortality rise precipitously with emergent cases, which is why vigilant outpatient monitoring of known paraesophageal hernias is a key component of the management. Laparoscopic management is generally preferred for both emergent and elective cases, if possible, due to the associated reduction in postoperative morbidity. Operative planning and patient selection should be approached carefully in elderly patients, as they have higher rates of morbidity and mortality following elective repairs compared to their younger counterparts.7–10 The impact of frailty on operative morbidity has gained significant interest recently, as frailty scores are a sensitive predictive measure of postoperative complications. Assessing frailty in patients presenting with minimally symptomatic paraesophageal hernias should become an important part of preoperative assessment when weighing the risks and benefits of elective repairs. Recurrence rates following repairs range widely in the literature, anywhere from 15% to 40%, with most quoting reductions in repair following mesh utilization.11–20
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.