
Abstract
Purpose:
To compare the effects of retrograde intrarenal surgery (RIRS) and percutaneous nephrolithotomy (PNL) on postoperative pain and their differences in terms of the postoperative need for analgesics in the treatment of 2–4 cm kidney stones.
Methods:
A total of 132 patients who suffered from renal stones 2–4 cm in size and had surgery at our urology clinic between April 2015 and April 2017 were enrolled in this prospective study (NCT02430168). Patients were randomized into either the RIRS group (Group 1) or PNL group (Group 2) in a ratio of 1:1. Postoperative visual analog scale (VAS) values at 8 and 24 hours postoperatively and analgesic treatments of patients were recorded.
Results:
Patients from both groups had similar demographic characteristics. Stone-free states were achieved in 37 (74%) patients in the RIRS group and 45 (90%) patients in the PNL group. Postoperative complication rates were similar in two groups. Moreover, there was no statistically significant difference between the groups in terms of the postoperative need for analgesics (P = .309). However, the PNL group had higher VAS values (P < .001).
Conclusion:
Although the early postoperative pain scales were high in the PNL group, there was no significant difference between the groups in terms of the standard analgesic treatments for achieving patient's comfort. PNL, which has similar complications, but with higher success rates, compared with RIRS, did not require additional analgesic treatment during postoperative pain management. Thus, in our opinion, PNL should still remain as a first choice in treatment of 2–4 cm renal stones.
Introduction
The prevalence of renal stone disease, which shows variability based on factors such as age, sex, and race, is ∼10%–15%. It most commonly occurs in the age range of 30–60 years. 1 Due to improvements in endoscopic approaches, minimally invasive treatments are commonly being used today in the treatment of renal stones, and only 1%–2% of cases require open surgery. 2 Although currently the primary recommended treatment for renal stones larger than 2 cm is percutaneous nephrolithotomy (PNL), retrograde intrarenal surgery (RIRS) has also started to gain ground based on arguments that it is minimally invasive and more comfortable for patients. The use of RIRS is increasing day by day in a wide variety of locations. This technique, which is described as the more minimally invasive technique, may replace PNL in removal of larger sized stones.
However, the most common postoperative complaint regarding both procedures is pain. No universal pain management strategy has been developed for the procedure yet. Keeping patients pain free during the postoperative period is crucial in getting the maximum possible success rates. We thought to clarify this issue, which was not handled carefully before in the literature. Therefore, we aimed to compare whether these procedures had different needs for postoperative analgesics and to select the first-choice treatment for pain management in this study.
Materials and Methods
The participants were evaluated after obtaining approval from the local ethics committee of our hospital. The national clinical trial number of our study is NCT02430168 and Institutional Review Board number is IRB18-14. Target population size was calculated with the G-Power software by reviewing studies that used similar parameters, with a confidence interval of 0.80. A total of 132 patients who suffered from renal stones, 2–4 cm in size, and had surgery at our urology clinic between April 2015 and April 2017 were enrolled in this prospective study.
After receiving patients' written informed consent, the patients were randomized into either the RIRS group (Group 1) or PNL group (Group 2) in a ratio of 1:1 by using an online research randomizer (Fig. 1). Patients who had a ureteral obstruction, history of stone surgery, infection before operation, and were below the age of 18 years were excluded from the study. The operations were performed by a team of four experienced surgeons with at least 5 years of RIRS and PNL experience each.
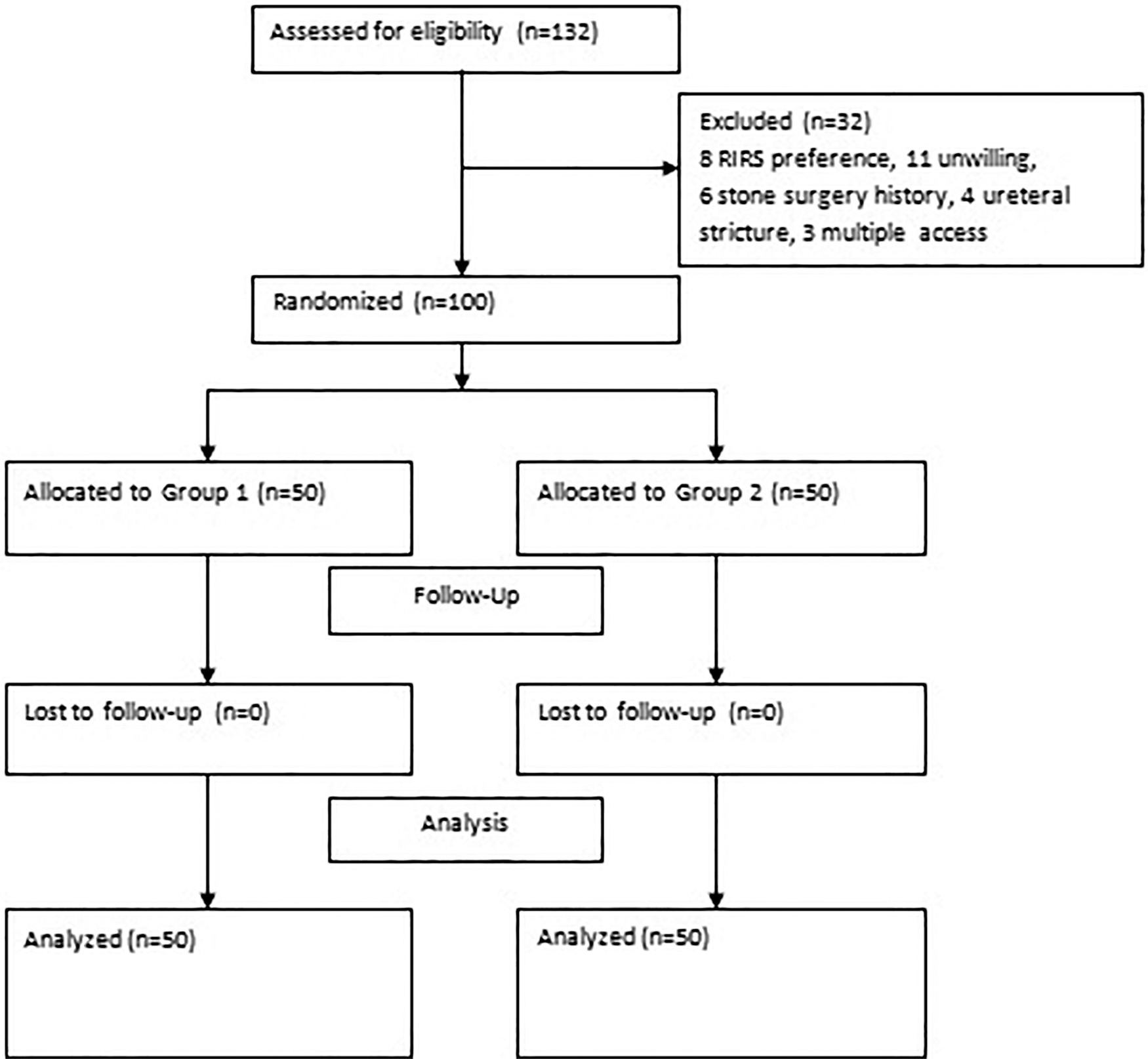
Study flow diagram. RIRS, retrograde intrarenal surgery.
All the patients who underwent surgery had preoperative sterile urine cultures. When calculating stone sizes, the longest diameter of the stone in the computed tomography (CT) scan was recorded in mm. In the case of multiple stones, the longest diameter of each stone was individually measured and all of the measurements were then added together. The Seoul National University Renal Stone Complexity (S-ReSC) score and its modified form were used to evaluate stone distribution.3,4
All patients who underwent renal stone surgery were treated with intravenous dexketoprofen trometamol, 50 mg twice daily, for the purpose of postoperative analgesic and anti-inflammatory treatment. Intravenous tramadol hydrochloride, 100 mg, was added to the treatment for patients who did not have their pain resolved after the initial treatment. In postoperative pain control studies conducted with these agents, the dose of tramadol in combined drugs is 75 mg.5–7 Therefore, when tramadol was used alone and not in combination, we preferred the dose of 100 mg. The patients who were included in the study were asked to fill out a visual analog scale (VAS) questionnaire at 8 and 24 hours postoperatively. Stone clearance after the procedure was evaluated with an X-ray taken on the postoperative first day and low-dose abdominal CT performed at 3 months postoperatively. The outcomes of patients who manifested residues of 2 mm or smaller or who were completely stone free in the follow-up controls were designated as successful.
RIRS implementation technique
After general anesthesia was administered to the patient, a guidewire was placed in the ureter. Then, the ureter was accessed with a semirigid 9.5F ureterorenoscope and diagnostic ureteroscopy was performed. Under fluoroscopic control, a ureteral access sheath of 9.5–11.5F thickness was inserted into the ureteropelvic junction over the guidewire placed in the ureter. After observation of the stone by entering through the sheath with a flexible ureterorenoscope (Flex-X2S; Karl Storz, Tuttlingen, Germany) with 7.5F outer diameter, lithotripsy was applied with a 272 μm holmium laser probe (Ho:YAG Laser; Dornier MedTech; Munich, Germany) at a frequency of 8–15 Hz and power within the 1.2–3.0 J range. At the end of the procedure, a Double-J stent was placed into the collecting system.
PNL implementation technique
Once a 5 or 6F open-ended ureteral catheter was retrogradely placed in the kidney, the patient was placed in the prone position. After reaching the specified calix with a percutaneous entry needle of 18 G thickness along with fluoroscopy, a 0.035-inch J-tip guidewire was inserted into the collecting duct system through the needle. The working sheath was placed into the collecting duct system by dilating the renal parenchyma up to 30F with Amplatz or metal dilators. By entering through the working sheath with a 26F nephroscope (Karl Storz®), lithotripsy was applied to the stones within the pelvicaliceal system with a pneumatic lithotripter (LithoClast; EMS, Nyon, Switzerland). Stone fragments were moved out of the working sheath by using forceps. An 18F reentry Malecot catheter was inserted as a nephrostomy tube by ensuring through and through access.
Statistical analyses
The statistical evaluation of data was performed using the SPSS for Windows 16.0 software package (SPSS, Chicago, IL). The one-sample Kolmogorov–Smirnov test was applied to quantitative variables. Differences between the groups in terms of age, body–mass index (BMI), number of stones, duration of operation, fluoroscopy duration, stone burden, and VAS score were analyzed using Student's t-test. Meanwhile, Pearson's chi-square test was used to determine whether there were any differences between the groups in terms of sex, stone orientation, location, Double-J use, rates of postoperative complications, and analgesic use. The Mann–Whitney U test was used to determine the significance of differences between the groups in terms of American Society of Anesthesiologists (ASA) scores and duration of hospitalization. The results were considered statistically significant for a value of P < .05.
Results
When the patient groups were compared in terms of demographic attributes, no statistically significant differences were observed between the groups in terms of age, sex, BMI, and ASA scores. The PNL group had significantly higher number of stones, greater stone burden, and longer duration of operation, fluoroscopy, and hospitalization. However, there was no significant difference between the groups in terms of the S-ReSC scores (Table 1).
Demographic and Clinical Data of Cases According to Groups
Modified S-ReSC score
P < .05: statistically significant.
ASA, American Society of Anesthesiologists; BMI, body–mass index; M/F, male/female; PNL, percutaneous nephrolithotomy; RIRS, retrograde intrarenal surgery; S-ReSC, Seoul National University Renal Stone Complexity.
The stone-free state following the first session was achieved in 37 (74%) patients in Group 1 and 45 (90%) patients in Group 2. Statistically, the PNL group was determined to be more successful (P = .037). No grade III, IV, or V complications were encountered in Group I. When the grades of complications were compared separately according to the Clavien–Dindo classification, the results were similar for both groups (Table 2). 8
Complications According to Clavien–Dindo Classification
P < .05: statistically significant.
PNL, percutaneous nephrolithotomy; RIRS, retrograde intrarenal surgery.
The mean VAS score at the eighth postoperative hour was significantly higher in Group 2 (4.74 [±2.1]) compared with Group 1 (3.34 [±2.0]). The VAS values at the 24th postoperative hour were similar in both groups (Group 1 0.58 [±0.79] and Group 2 0.62 [±0.73]). Thirty-two patients in Group 1 and 27 patients in Group 2 were treated with dexketoprofen trometamol alone as the means of pain management. The number of patients who required dexketoprofen trometamol + tramadol hydrochloride was 18 in Group 1 and 23 in Group 2 (Fig. 2). There was no significant difference between the groups in terms of the postoperative need for analgesics (Table 3).
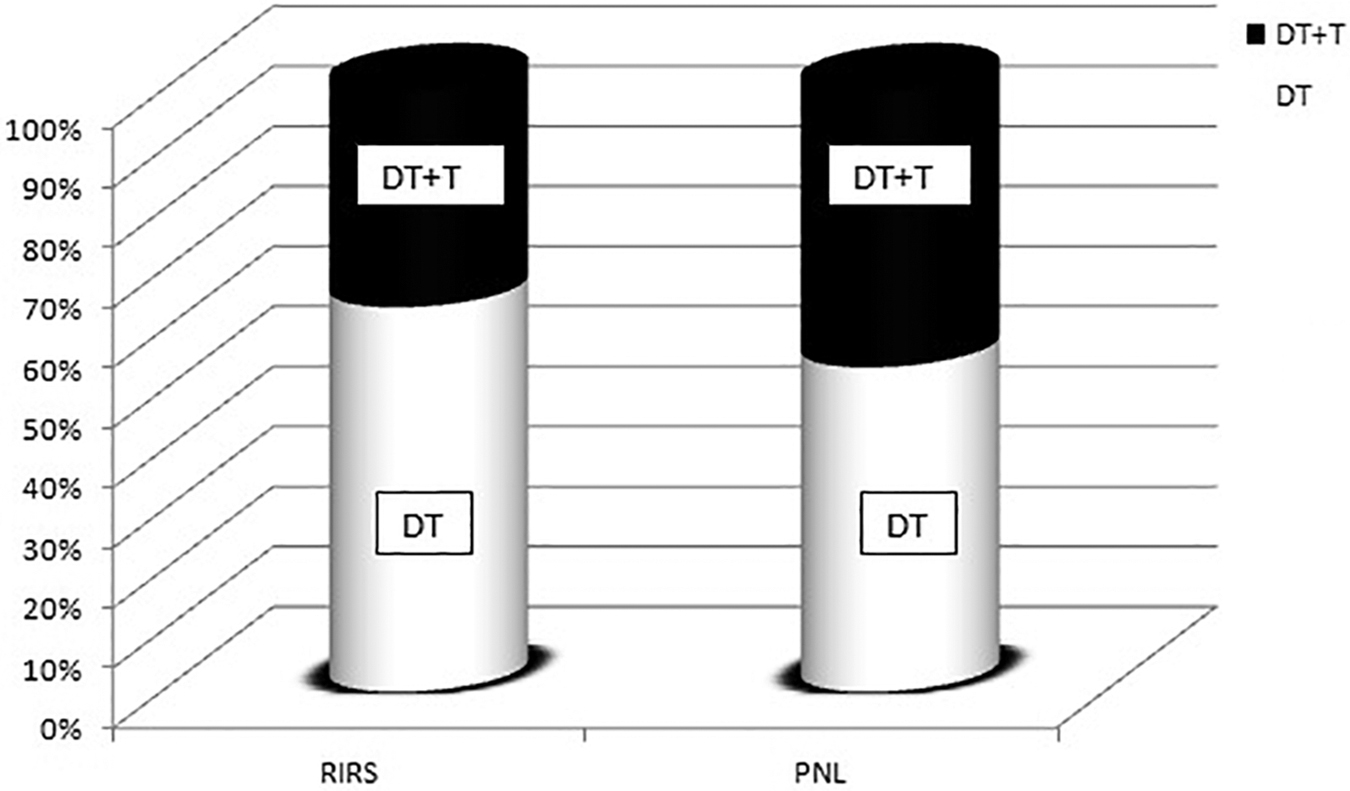
Drugs used in pain management according to procedures. DT, dexketoprofen trometamol; DT + T, dexketoprofen trometamol + tramadol hydrochloride; PNL, percutaneous nephrolithotomy; RIRS, retrograde intrarenal surgery.
Postoperative Pain Scale and Analgesic Requirement
PNL, percutaneous nephrolithotomy; RIRS, retrograde intrarenal surgery; VAS 8th, visual analog scale at eight hours postoperatively; VAS 24th, visual analog scale at 24 hours postoperatively.
P < .05: statistically significant.
Discussion
Postoperative patient comfort and pain management have not been standardized in terms of efficacy and complications in stones larger than 2 cm. To the best of our knowledge, there are no randomized prospective studies that compare the postoperative pain management and analgesic needs of patients who underwent RIRS and PNL for the treatment of 2–4 cm renal stones. Recent technological advances allowed for smaller sized equipment to be used for procedures such as extracorporeal shock wave lithotripsy, RIRS, PNL, and laparoscopic methods frequently used in renal stone treatment have been improving in ways to emphasize patient comfort at a greater rate. The European Association of Urology recommends PNL as the primary choice for the treatment of renal stones larger than 2 cm. 9 However, certain comparative studies that found a relatively high major complication rate associated with PNL have recommended RIRS for treatment of renal stones larger than 2 cm.10,11
It has been reported in the literature that stone-free status is one of the most important factors affecting postoperative pain. 12 In our study, although the stone number and stone size differed between the two groups after randomization, the two groups were similar in terms of the S-ReSC score that predicts stone-free rates. In addition, as expected, the fluoroscopy and operation times were longer in PNL.12–14 However, there are no studies in the literature that investigate these factors' effects on pain.
The large series published early on indicated that success rates for PNL varied between 72% and 98%.15,16 The first comprehensive series that included 1000 cases was reported by Segura et al. in 1985. 16 In recent studies, Sari et al. 14 compared 254 PNL and 185 RIRS procedures used for treatment of renal stones larger than 2 cm and reported rates of success at the first session as 93.3% and 73.5% and total success rates as 94.9% and 85.4%, respectively. Similar rates were reported by Bryniarski et al. 17 in their prospective study with 64 cases that involved treatment of stones larger than 2 cm and included only renal pelvis stones. When evaluated with a success-based approach, the superiority of PNL in terms of the results obtained at the first session is undeniable. Especially in renal stones larger than 2 cm, the superior success of PNL is remarkable.13,14,18
Ozturk et al. 19 reported that the success rate of PNL was higher in the lower pole renal stones with a size of 10–20 mm (94% versus 73%). However, there are also studies showing that high success rates obtained with PNL may be matched with staged RIRS sessions. 11 Palmero et al. 20 reported post-RIRS and PNL success rates of 73.6% and 80.6%, respectively, but stated that this difference was not statistically significant. Success rates at the end of the total procedure were declared as 93.5% and 94.3% in the same study. In another study, in which renal upper pole stones were examined, success rates were similar. In this study published by Selmi et al., 21 we thought that inclusion of upper pole renal stones <2 cm increased the RIRS success. In addition, the success rates of these two methods were similar in another retrospective study involving patients with horseshoe kidney anomalies. 22 Several scoring systems have been developed to predict a wide range of stone-free rates.3,4,23 In our study, no difference was observed between the S-ReSC scores for the PNL group and the modified S-ReSC scores for the RIRS group.
Evaluation of the duration of operations showed that they were significantly longer in the PNL group. We believe that one of the important factors regarding this was the urethral catheter placement procedure done before placing the patient in the prone position. Bryniarski et al. 17 have also reported significantly longer operation times with PNL. However, some studies report a longer duration for RIRS than for PNL in the treatment of renal stones larger than 2 cm.9,13,24,25 We think that the results on this subject may be affected by the relatively high experience of PNL in the years when the studies were published. Karakoyunlu et al. 18 stated that PNL is a method with shorter operation time and higher success rate in renal stones larger than 4 cm. In this retrospective study, RIRS had fewer complications and shorter hospitalization times. Several comparative studies that evaluated renal stones larger than 2 cm have also reported significantly longer fluoroscopy times in the PNL group.13,14,25 Since it is not yet possible to access the collecting duct system under direct vision in PNL, it is crucial to have greater mastery of anatomy and longer fluoroscopy duration to prevent potential complications.
In our study, the postoperative hospitalization duration was significantly longer in the PNL group, paralleling most published studies.13,14,21,25,26 In a meta-analysis of treatments of renal stones larger than 2 cm involving 590 patients, Zheng et al. 27 reported that since RIRS causes less trauma to the patient, patients healed faster in the postoperative period in comparison with the PNL group and therefore the duration of hospitalization was shorter. However, it must be taken into consideration that in the treatment of large stones, as in in our study, the repetitive RIRS sessions performed to obtain the PNL-like stone-free rates will prolong the duration of hospitalization in total and hence would also increase the cost. 10 Accordingly, during the treatment of large renal stones, physicians should remember that applying repetitive sessions of RIRS, instead of keeping the patients in the hospital for a few more days following PNL, might increase associated anesthesia risks and result in comparable duration of hospitalization in total.
The rates of complications associated with RIRS and PNL vary greatly in the literature. While, some publications mention similar complication rates,13,14,21,26 other studies state that RIRS-associated complications are at a more minor level and conservatively treatable, whereas major complications are encountered more frequently following PNL.9,25,26 Although grade II and grade III complication rates appeared quantitatively higher when compared based on the standardized classification, no statistically significant differences were observed between the two groups in our study. Similarly, in a retrospective study of renal stones larger than 2 cm, although more complications were observed in the PNL group, they were not statistically significant. 14 In another retrospective study in our clinic in patients with horseshoe kidney anomalies, these two methods were similar in terms of complications. However, more serious complications were observed in PNL. 22
Postoperative pain assessment is usually not addressed under the title of complications since it is a subjective symptom. However, pain that appears after the procedure prolongs hospitalization is a very important problem for patients. In fact, this subject has always been neglected in studies comparing these two methods13,14,18,19,22 because these studies have a retrospective design. In the current prospective study, we aimed to standardize this subjective symptom with the use of a VAS that measures postoperative pain and compare the differences of this scale's values in patients who underwent RIRS and PNL.
In the retrospective study reported by Atis et al. 25 on the treatment of renal stones 2–4 cm in size, where pain levels on postoperative day one following 146 RIRS and 146 PNL procedures were evaluated, VAS values of patients who underwent PNL were significantly higher. Bryniarsky et al. 17 reported higher postoperative VAS values and higher rates of narcotic analgesic use in patients who underwent PNL due to renal pelvis stones. On the other hand, Ozayar et al. 28 reported similar early postoperative VAS values and levels of the need for analgesics in their prospective study of 56 patients who underwent RIRS or PNL for treatment of lower pole renal stones smaller than 2 cm. In a randomized study by Hanna et al., 29 twice daily parenteral dexketoprofen trometamol, 50 mg, was reported to have good analgesic efficacy.
Poor analgesia adversely affects patient comfort in the postoperative period. It was also reported that pain was the main reason that led patients who had been discharged after ureteroscopy to return to the hospital. 30 While a 30F working sheath was used at our clinic, Monga and Oglevie 31 reported less perioperative pain and bleeding with the use of a 20F working sheath. Oğuz et al. 12 prospectively investigated the factors that affected pain in the early postoperative period in 250 patients who underwent RIRS. In their study, where they separately investigated the factors associated with the patients' demographics, stone, and operation, the significant factors that were found to affect pain were reported as female gender, stone size, and the duration that the access sheath remained in the ureter. Among women included in the study, 27.9% were determined to experience severe postoperative pain, while for men, this rate was 11.6%. Again, in this particular study, it was reported that the pain levels of patients who had residual stones were higher.
Different analgesics, including opioids, nonsteroidal anti-inflammatory drugs (NSAIDs), local analgesia, and different combinations, are used through different routes. Opioids are the most commonly used strong analgesics for pain control, but are associated with adverse conditions such as respiratory depression, bradycardia, hypotension, nausea, vomiting, and a long follow-up period. 32 Initially, NSAIDs were used to complement the opioids and to reduce their dose and side effects. With time, however, certain centers replaced opioids and NSAIDs started being used as sole agents for pain relief during the perioperative period. 11 Nowadays, combination therapies are used to provide the highest comfort in pain control.5–7,33
In our study, we investigated the pain control efficacy of a standard NSAID between RIRS and PNL. We found that the necessity for additional opioids after these two—patient-controlled analgesia or operation site nerve block—is becoming increasingly available after PNL especially if surgeons favor inserting nephrostomy tubes. Administering bupivacaine around the nephrostomy tract immediately after surgery was demonstrated to be more effective for early postoperative pain control. 34 This technique may also increase early patient satisfaction. Intercostal blockade with bupivacaine significantly improves pain control in the early postoperative period. The effectiveness of bupivacaine clears away within 6 hours of surgery, after which narcotic use becomes indistinguishable. Intercostal nerve blockade is an easy, safe, and inexpensive method that can be used to control postoperative pain after PNL. 35
In our study, high VAS scores at the postoperative eighth hour after PNL can be reduced with such recommendations. In addition, PNL is frequently terminated with a Malecot catheter in our clinic. As shown in some studies, tubeless operation reduces the need for analgesics after PNL.31,36 The absence of tubeless PNL cases may be one of the limitations of this study. Future studies in high-volume centers with tubeless PNL may offer important insights. In addition, a minor limitation of our study was the lack of stratification of the groups according to stone sizes of 2–3 cm and those of 3–4 cm. However, our study is the first randomized prospective study comparing these two methods in terms of postoperative pain and analgesia management. In addition, unlike many studies comparing these two methods, it is a study that focuses on patient comfort, which can sometimes be ignored.
Conclusion
We reached the conclusion that although early postoperative pain scales are higher after PNL, patient comfort can be ensured with the standard use of anti-inflammatory and analgesic treatments following both RIRS and PNL. In addition, PNL did not cause additional analgesic need in postoperative pain management. Based on our results, after a single session, PNL should continue to be the primary choice of treatment due to its superiority in postoperative stone-free rates and similar outcomes in terms of complication rates and need for additional analgesics.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.