
Abstract
Objectives:
Evaluate the quality of life (QoL) in patients diagnosed with achalasia who performed Heller's myotomy.
Methods:
Between January 1, 2000 and March 27, 2019, 99 patients were submitted to esophagomyotomy at the São João Hospital in Oporto, Portugal. The exclusion criteria were other diagnoses, age <18 years at the date of surgery, and death. Seventy-five patients were contacted. Pre- and postoperative evaluations were performed using the achalasia disease-specific QoL questionnaire and by the Eckardt score. QoL was assessed by the Medical Outcomes Study SF-36.
Results:
Forty-nine patients (65%) answered the questionnaires. The median difference in the achalasia-DSQoL questionnaire between the pre- and postoperative period was −9.0 (interquartile range [IQR]: 5–12), whereas in the Eckardt score was −5.0 (IQR: 3.25–7). Lower postoperative scores correlated with higher scores on the SF-36's mental and physical summary measures (Spearman's rho [ρ] = −0.651 and ρ = −0.577 for the achalasia-DSQoL questionnaire and ρ = −0.552 and ρ = −0.515 for the Eckardt score, P < .001). Physical and mental summary measures were correlated with each other (ρ = 0.788, P < .001).
Conclusions:
Heller's myotomy allows a decrease in symptoms and an increase in QoL. Patients with severe symptoms before surgery had higher postoperative scores and patients with fewer symptoms had lower postoperative scores.
Introduction
Achalasia is a rare disease of esophageal motility of unknown etiology 1 with an estimated incidence of 1.59 cases/100,000 per year, 2 having a bimodal distribution, with peaks at 30 and 60 years 3 and an estimated prevalence of 10/100,000. 4 Achalasia occurs equally often in both men and women. 3 It is characterized by insufficient relaxation of the lower esophageal sphincter and loss of esophageal peristalsis, 5 caused by degeneration of the myenteric plexus. 1 The classic presentation is dysphagia for solids and liquids, associated with regurgitation of undigested food or saliva. 4 Symptoms such as retrosternal chest pain during meals, weight loss, and heartburn are also common. 4
High-resolution manometry is recommended as the test of choice for the diagnosis of achalasia, and an upper gastrointestinal endoscopy should also be performed to exclude neoplastic diseases that may cause pseudoachalasia. 6
Laparoscopic Heller's myotomy is one of the treatment options for achalasia, whose objective is to split the fibers of the esophageal muscle layer through a longitudinal cut, thus correcting insufficient relaxation of the lower esophageal sphincter. 7 However, with this technique, there is an increased risk of the patient developing gastroesophageal reflux, so it is important to include an antireflux procedure. 7
Patients and Methods
Patients
This is a retrospective study including all patients submitted to an esophagomyotomy plus fundoplication at the esophagogastric unit of the São João Hospital between January 1, 2000 and March 27, 2019. Exclusion criteria were other diagnoses, age <18 years at the date of surgery, and death. Seventy-five patients met the criteria to enter the study and were contacted by letter and telephone call. Forty-nine patients answered the questionnaires, leading to a response rate of 69%.
This study was approved by the Ethics Committee of the Hospital of São João. Confidentiality and privacy of information were guaranteed in accordance with the Declaration of Helsinki.
Social and clinical characteristics
The demographic data (age and gender) were collected from the database of the Hospital of São João. Pre- and postoperative evaluations were performed using a translated version of the achalasia disease-specific quality of life questionnaire (achalasia-DSQoL) developed by Urbach et al., 8 and by the Eckardt score. 9
Achalasia-DSQoL questionnaire includes 10 questions that assess food tolerance (questions 1–4), dysphagia-related behavior changes (question 5), pain (question 6), heartburn (question 7), distress (question 8), lifestyle limitations (question 9), and satisfaction (question 10). 8 The minimum score is 10 points and the maximum is 31 points; a lower score represents a better QoL. 8
The Eckardt score evaluates dysphagia, regurgitation, weight loss, and chest pain. 9 Dysphagia, regurgitation, and chest pain are rated from 0 to 3, depending on whether they are absent, occasional, daily, or occur several times a day. 9 Weight loss is also rated from 0 to 3, depending on the absence of weight loss, weight loss <5 kg, weight loss between 5 and 10 kg, and weight loss >10 kg. 9 Treatment is considered successful if the Eckardt score is 3 or less. 3
QoL assessment
QoL assessment was performed using the Portuguese version of the Medical Outcomes Study.10–12 The SF-36 Health Survey consists of 36 questions, allowing to measure eight health dimensions on a scale from 0 to 100, with 0 corresponding to the worst possible QoL and 100 to the best possible QoL. 11 The dimensions evaluated are physical functioning (PF), role limitations due to physical health problems (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role limitations due to emotional problems (RE), and mental health (MH).11,12 These dimensions can be grouped into two: physical and mental summary measures (PSM and MSM).11,12 The PSM is calculated from the PF, RP, BP, and GH, whereas the MSM consists of the SF, RE, MH, and VT.11,12 The SF-36 allows us to assess one additional dimension through question 2, which is health change, 12 which aims to assess the patient's perspective regarding their current health in relation to the past. However, in this study, this question was changed to assess the patient's perspective on current health relative to the period before the operation.
Evaluation of the patients' satisfaction and perspective in relation to the surgical procedure
Patients' satisfaction regarding the surgical procedure was accessed by the question “Would you be submitted to surgery again?” with only two possible answers (“yes” or “no”) and by the level of agreement with the statement “I am satisfied with my surgical treatment of achalasia.” A 5-point Likert scale allowed evaluating the degree of patients' satisfaction with surgery.
Statistical analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences Software (IBM SPSS 26.0®). Spearman correlations were performed to compare the results of the different questionnaires. Wilcoxon signed-rank test was performed to compare the pre- and postsurgical periods regarding the achalasia-DSQoL questionnaire and in the Eckardt score.
Results
Demographic and social characterization
Forty-nine patients answered the questionnaires, yielding a response rate of 65%. Forty-seven questionnaires were completed and two were partially completed. The median age of participants at the time of surgery was 38 years (range 18–77 years). All patients had a minimum follow-up of 6 months and median follow-up was 105 months (interquartile range [IQR]: 53.50–132.50 months). Figure 1 shows the distribution of patients' follow-up at each year interval. Twenty-one participants were men (42.9%).
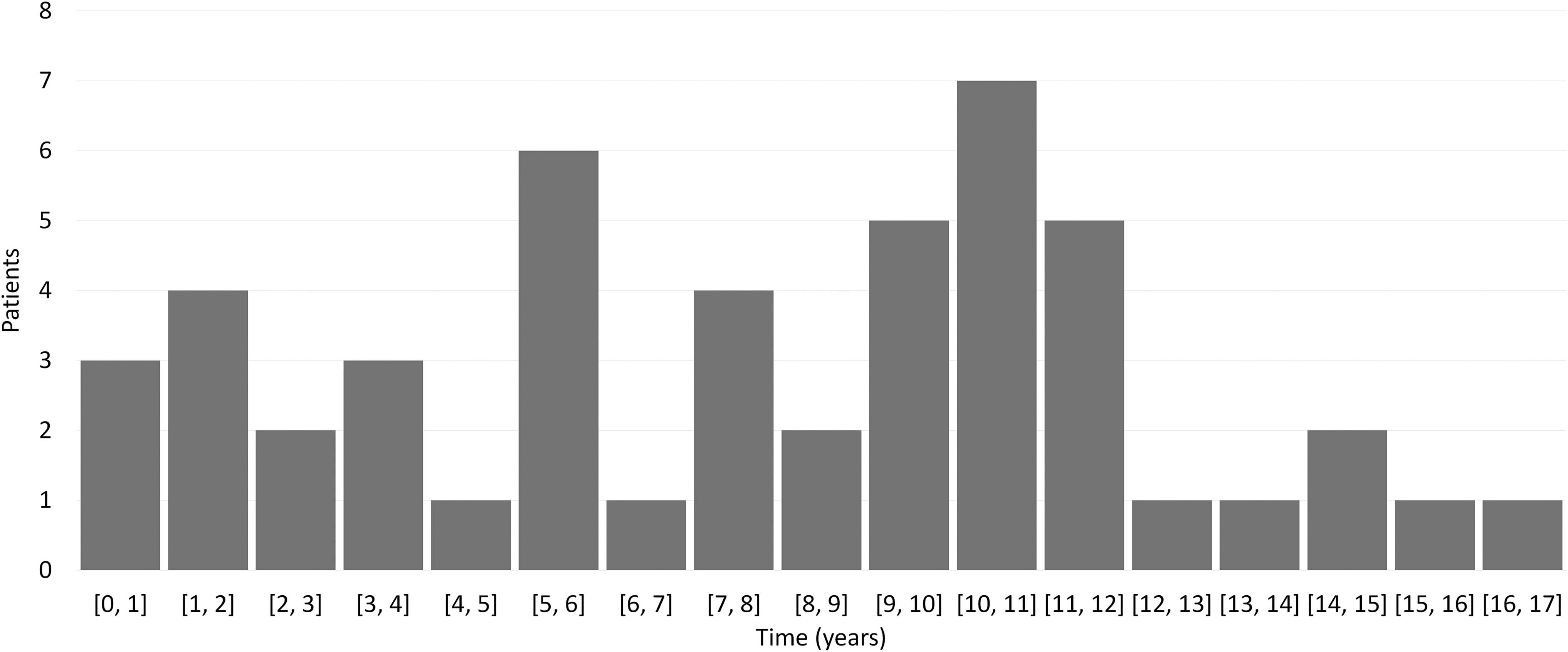
Distribution of patient population according to follow-up time.
Table 1 summarizes the main demographic and clinical characteristics of the patients.
Demographic and Preoperative Clinical Characteristics
Presurgical characterization
Before surgery, dysphagia was the predominant symptom, presenting in 98% of the patients, and 67.3% reported dysphagia at every meal. Regurgitation, chest pain, and weight loss were also quite common, being present in 93.9%, 83.7%, and 75% of patients, in the order given (Table 2). The presurgery Eckardt score had a median value of 8 (IQR: 7–10). In the achalasia-DSQoL questionnaire, the median of the ratings was 27 (IQR: 22–29).
Comparison of the Symptoms That Form the Eckard Score Between the Pre- and the Postoperative Period
Postsurgical characterization
In the postoperative evaluation, dysphagia remained the most common symptom, being present in 75% of patients. Chest pain became the second most common symptom with 56.2% of patients reporting the presence of this symptom, followed by regurgitation and weight loss, with 50% and 20.4%, in the order given (Table 2).
The median value of the Eckardt score was 2 (IQR: 1–4), whereas in achalasia-DSQoL questionnaire it was 15 (IQR = 13–22).
Comparing the preoperative with the postoperative assessment, there was a median decrease of 9 (IQR: 5–12) in the achalasia-DSQoL and 5 (IQR: 3.25–7) in the Eckardt score. The analysis of both differences, through Spearman correlation, showed a significant correlation between them (Spearman's rho [ρ] = 0.552, P < .001).
We compared the pre- and postsurgery achalasia-DSQoL and Eckardt scores for each patient using Wilcoxon signed-rank test and found that both were significantly lower (P < .001) postsurgery. These findings are illustrated in Table 3.
Wilcoxon Signed-Rank Test
Achalasia-DSQoL, achalasia disease-specific quality of life; IQR, interquartile range.
QoL assessment
The value of each of the eight dimensions of the SF-36 Health Survey are summarized in Table 4. Regarding the PSM, the median value was 93.54 (IQR: 60.83–100) and the median of the MSM was 66.84 (IQR: 41.55–81.15). These significantly correlate with each other (ρ = 0.788 and P < .001). The PSM and MSM are also correlated with both the postoperative achalasia-DSQoL and the Eckardt score (Table 5).
Results of the SF-36 Health Survey
Values are expressed as means.
SF-36, Medical Outcomes Study SF-36.
Spearman Correlations Used on This Study
Achalasia-DSQoL, achalasia disease-specific quality of life; ρ-Spearman's rho.
Using the achalasia-DSQoL questionnaire, the difference found between pre- and postoperative assessment is inversely correlated with the PSM (ρ = −0.645, P < .001) and the MSM (ρ = −0.642, P < .001) at a statistically significant level. The same correlation can be found when comparing the difference in Eckardt score between pre- and postoperative moment with PSM (ρ = −0.291, P = .044) and MSM (ρ = −0.445, P = .002). We also analyzed the results obtained by gender. The results can be found in Supplementary Table S1.
Perspective and satisfaction in relation to the surgical procedure
Regarding the question “Would you undergo to surgery again?” 38 patients (80.9%) answered “Yes.” Concerning the statement “I am satisfied with my surgical treatment of achalasia,” 24 patients (50%) answered “Strongly agree,” 14 (29.2%) “Agree,” 6 (12.5%) “Neither agree nor disagree,” 2 (4.2%) “Disagree,” and 2 (4.2%) “Strongly disagree.”
In the SF-36's question 2, which is altered in this study to assess health change from the patient's perspective regarding current health in relation to the period before the operation, 34 patients (69.4%) answered “Much better,” 10 (20.4%) “Somewhat better,” 4 (8.2%) “About the same,” and 1 (2%) “Somewhat worse.”
Discussion
Heller's myotomy with a fundoplication has been described as an effective therapy in the treatment of achalasia, 13 with several studies reporting an efficacy of around 90%. 3 If we consider an Eckardt score of 3 or less as the cutoff point for an effective treatment, we have in this study 34 patients with such a value—an efficacy of 70.8%. This differs from what has been reported in recent studies, in a population that in the preoperative evaluation 94.9% scored 4 or more in the Eckardt score, Asti et al. 14 reported that only 13% maintained this score after Heller myotomy with fundoplication. However, in our study, only 5 patients did not show differences in the Eckardt score between pre- and postoperative evaluation, meaning that 89.6% of patients saw their symptoms improve after surgery. Regarding the achalasia-DSQoL questionnaire, only 1 patient did not show a decrease in the total result in the postoperative evaluation. Luketich et al. 15 also obtained similar results; they reported that only one of the patients showed no improvement in dysphagia and 92.5% of patients were satisfied with the outcome of the surgery. In addition, they pointed that all SF-36 domains were equal to or better than normal U.S. population value. In Figure 2, a comparison is shown between the SF-36 results that we obtained with other similar study that used the SF-36 Health Survey as well as with the Portuguese Normal Values.11,15–17 Our results differ from those obtained in other studies, but are similar to the normal values of the Portuguese population.

SF-36 domains comparison. SF-36, Medical Outcomes Study SF-36.
Achalasia has a profound effect on the patient's ability to eat and maintain a good nutritional status. Also, changing eating habits in response to symptoms has a negative impact on patients' QoL. Ben-Meir et al. 17 showed that domains such as physical function and social function are the most altered between the pre- and postoperative period. Thus, it was demonstrated that domains that were not supposed to be affected by achalasia did not stray far from normal population values. This is in line with other studies where the SF-36 values in postoperative patients are similar to population values. Thus, differences between populations may explain the difference found between this and the other studies.
We found that better results on the achalasia-DSQoL questionnaire had a significant correlation with better results on the SF-36 Health Survey (Table 5). In his study, Frankhuisen et al. 18 compared the achalasia-DSQoL questionnaire with the RAND-36, which is an SF-36-like QoL assessment tool, showing only a slight correlation between the two tools, implying that a DSQoL measure exhibits a weaker correlation with a measured generic QoL. This can be explained by the generic characteristics of both RAND-36 and SF-36.
Patients with severe symptoms before surgery had higher postoperative scores and patients with fewer symptoms had lower postoperative scores, suggesting that early intervention might provide better outcomes in QoL. Different results were presented by Decker et al. 19 ; at 3 years of follow-up, patients with severe symptoms registered significant improvements in QoL Questionnaires and in patients with mild symptoms, although there was a slight increase in QoL, this was not statistically significant. However, in the same study, it is noted that there is a slight decrease in the QoL between the evaluation of the first year and the third year after surgery. 18 This decrease can be explained by a euphoric state of the patients to the fact that the operation restores their ability to eat, thus causing an overestimation of the assessments, which decreases as they get used to their new normal state. Or, because Heller Myotomy plus fundoplication is a palliative surgery and this is a result of the progression of the disease.
One of the limitations of our study is related to the follow-up time, as this is quite heterogeneous among patients and the postsurgical evaluation was performed only once and the time at which it was performed differs from patient to patient. Maybe this can explain why our results differ from the rest of the literature. More long-term studies with regular evaluations will be needed to clarify which of the reason mentioned earlier may have influenced the differences found in the effectiveness of the treatment and in the QoL outcomes.
Footnotes
Authors' Contributions
This study was designed by D.M.P.P. and J.B. J.P.B. performed statistical analysis. D.M.P.P. and J.P.B. contributed to the interpretation of the results. J.B. and E.B. supervised the study. D.M.P.P. wrote the article in consultation with J.P.B., J.B., and E.B.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was not financially supported.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.