
Abstract
Background:
Gastric bypass is one of the most widely performed bariatric procedures worldwide and continues to be the gold standard in obese patients with metabolic disorders.1 Regarding the complications, these can appear early or late, the most frequent of the latter being anastomosis stenosis, especially the gastrojejunal (G-J) stenosis. The first treatment option in stenosis is the endoscopic approach, but in cases wherein it fails or the diagnosis is kinking, revisional surgery should be performed.
Methods:
We describe the technique, step by step, we use to perform a very complex revisional surgery in a patient with aphagia after gastric bypass.
Results:
This is the case of a 38-year-old female patient who underwent laparoscopic adjustable gastric band in 2011; due to her poor tolerance, a laparoscopic gastric bypass was done. She began with vomiting and gastroesophageal reflux with remarkable symptoms. Diagnosis of stenosis of the jejunojejunal anastomosis of the Roux-en-Y was made and two surgeries were done to treat it. Later the patient referred aphagia and a kink of the gastrojejunal (G-J) anastomosis were observed in the gastrointestinal series. We decided to do a revisional surgery and we describe it step by step in this article.
Conclusion:
The G-J anastomosis stenosis is the most frequent late complication. Also kinking has to be considered strongly when aphagia or symptoms of obstruction are present. If endoscopic treatment for stenosis or cases of kinking is unsuccessful and fails, then revisional surgery should be considered.
Introduction and Background
Gastric bypass is one of the most widely performed bariatric procedures worldwide and continues to be the gold standard in obese patients with metabolic disorders. 1 Among the complications, these can appear early or late, the most frequent of the latter being anastomosis stenosis, especially the (G-J) stenosis.1,2 Postprandial vomiting accompanied or not by pain is the most common symptoms. Given these symptoms, if the endoscopy is not conclusive of stenosis, intestinal obstruction due to kinking should be suspected. The first treatment option in stenosis is the endoscopic approach, but in cases wherein it fails or the diagnosis is kinking, revisional surgery should be performed.3,4
Management of stenosis and kinking
Despite being a safe procedure, gastric bypass can have different complications. These can be early or late complications.1,5 Within the early complications, we can find leaks of the staple lines or anastomoses, gastrointestinal (GI) bleeding, and intestinal obstruction. Within the late stenosis of the anastomosis, marginal ulcer, gastrogastric fistula, and looping of the loop or kinking can be observed.1,6 Among the latter, the most frequent is stenosis and more precisely that of the G-J anastomosis. It has been reported between 5% and 27% of cases, generally appearing after 90 days after surgery. 4 The classic symptoms are postprandial vomiting accompanied by different levels of dysphagia, which can lead to aphagia in severe cases.4,7 The causes of stenosis can be varied, including excessive ischemic and nonischemic scar formation, recurrent marginal ulcers, malrotation or tension of the anastomosis, and surgical technique. Regarding the latter, there are many factors to consider such as the type of suture to be used (linear vs. circular), size of the suture, manual suture, and experience of the surgeon.
The first choice treatment should be the endoscopic approach.4,8 Between 17% and 67% of cases respond satisfactorily to the first attempt at endoscopic pneumatic dilation, although up to 8% of cases require three or more attempts. 4 In cases wherein it fails, surgical treatment should be performed. Laparoscopic revisional surgery is a highly demanding procedure that must be performed by teams trained in laparoscopic bariatric surgery and also in revisional surgeries. The main difficulty remains in the formation of adhesions that make anatomical identification of the different structures difficult by changing the anatomy of the abdomen and stomach.4,9,10
Methods
We describe the technique, step by step, we use to perform a very complex revisional surgery in a patient with aphagia after gastric bypass.
Results
Surgical technique and clinical case presentation
As previously mentioned, revisional surgeries can be highly demanding procedures even in the most trained hands in bariatric surgery, much more if we add to this that patients often have multiple surgeries both laparoscopically and openly, which generates a large amount adhesions that distort the anatomy and hinder the resolution of the case.1,4
This is the case of a 38-year-old female patient who underwent a laparoscopic adjustable gastric band in 2011 in another institution, followed by a laparoscopic gastric bypass in July 2012 due to bad tolerance to the band. In July 2013, an abdominal dermolipectomy was performed and 4 months later in November, a new abdominal and lower limb dermolipectomy was performed.
In 2014, she began with vomiting and gastroesophageal reflux with remarkable symptoms. The diagnosis of stenosis of the jejunojejunal anastomosis of the Roux-en-Y was made. Surgery was decided and in December of that year, intestinal resection and redo jejunojejunal anastomosis with hiatoplasty were performed laparoscopically. In February 2015, he underwent a new resection and jejunojejunal anastomosis for continuing similar symptoms. This time the surgery was open. That year the patient begins with a certain degree of dysphagia. An endoscopic diagnosis of stenosis of the G-J anastomosis was made. A failed attempt at endoscopic dilation occurs, so it was decided to reoperate it. A redo gastrectomy and redo G-J anastomosis were performed by an open approach. All these procedures were done in another center.
The patient was referred to us in 2018, she reported >2 years of postprandial incoercible vomiting associated with dysphagia, tolerating only the intake of liquids and highly processed foods. During 2017, she underwent multiple failed endoscopic treatments. A new endoscopy was requested, which reports congestive gastric stump, G-J stenosis, and anastomosis with endoscope passage (Fig. 1).
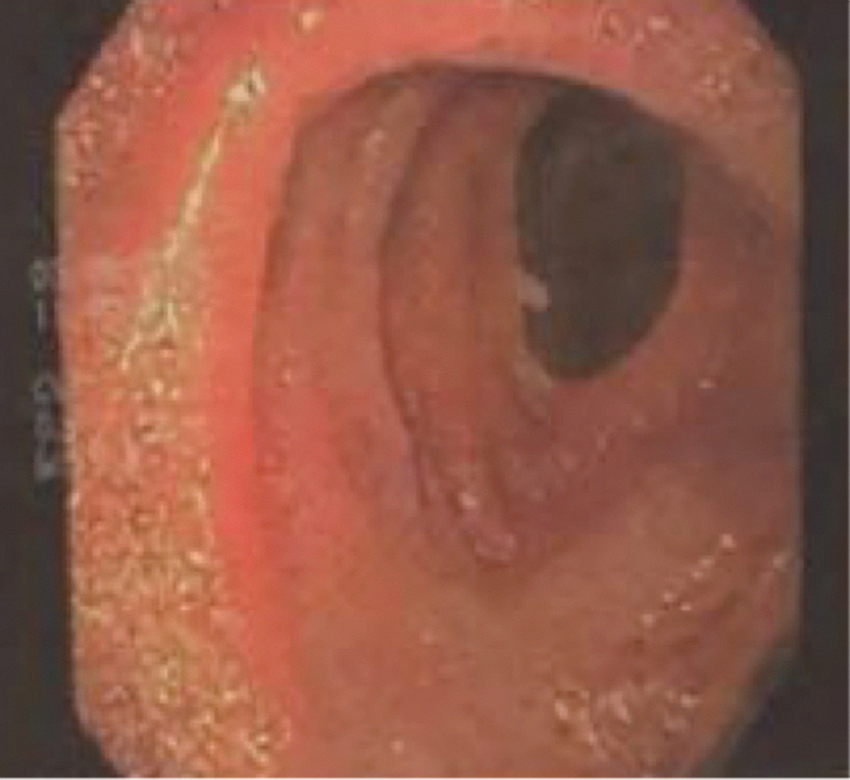
Endoscopic view of anastomosis.
An upper GI series was performed. (Fig. 2), demonstrating an increased gastric stump, without motility and with severe delay in emptying. G-J anastomosis in the anterior superior region of good caliber (2.5 cm). Contract progresses to the left iliac fossa.

An upper GI series was performed demonstrating a kink in the gastrojujunal anastomosis.
With this new diagnosis of intestinal obstruction due to kinking of G-J anastomosis, it was decided to do a revisional surgery.
We decided to perform it laparoscopically. The position of the trocars to perform this surgery, we used the same that we used for all our bariatric procedures. We placed a supraumbilical 10 mm trocar in the midline for the endocamera, a 5 mm trocar in the epigastrium for liver retraction, two 13 mm trocars in each hypochondrium for the surgeon, and a 5 mm trocar on the left flank for the assistant. (Fig. 3)
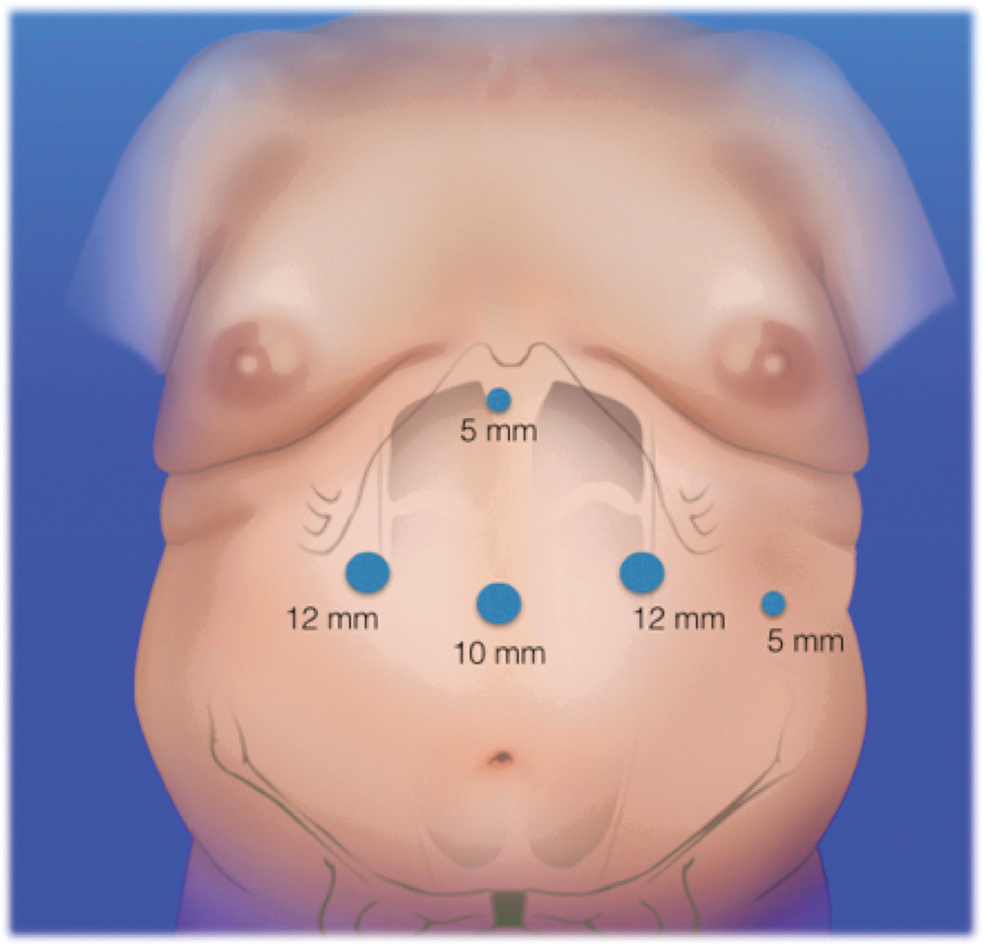
Position of the trocars for revisional surgery.
We started to free the adhesions with ultrasonic scalpel and scissors (Figs. 4 and 5).
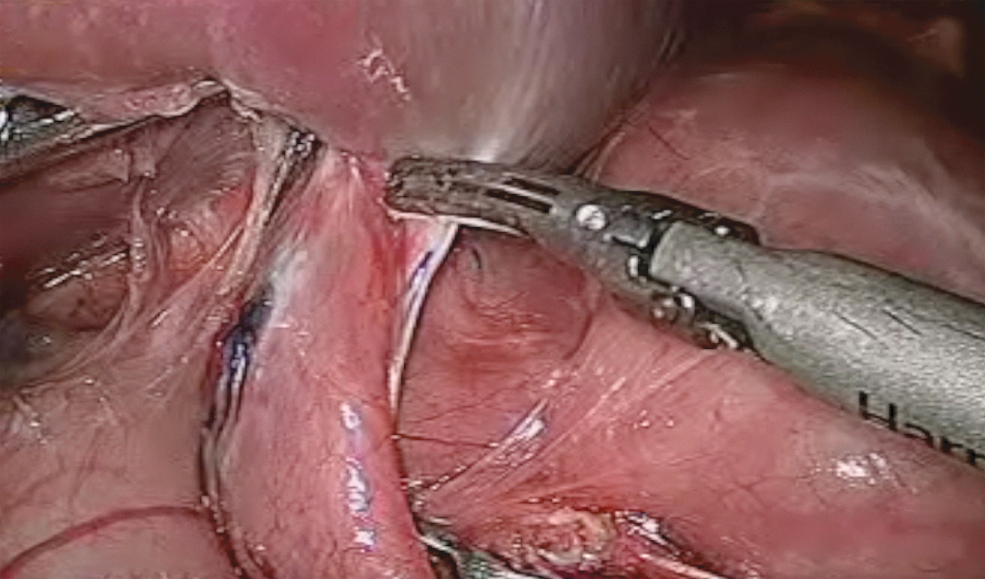
We started releasing the adhesions with ultrasonic scalpel.
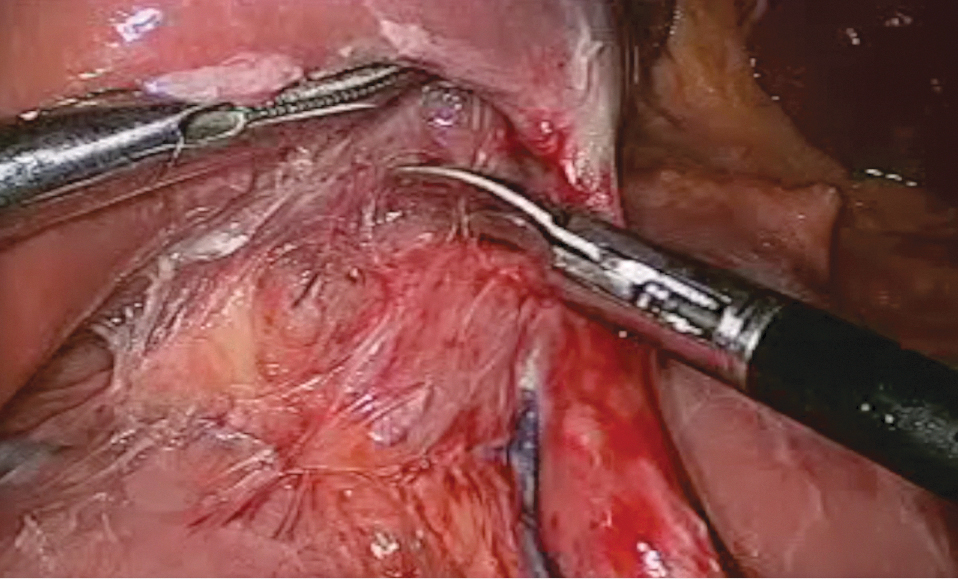
We then continue releasing the adhesions with scissors.
The inferior aspect of the dilated gastric stump is individualized and released. Part of the alimentary loop was identified and released as close as possible to the G-J anatomosis.
Two stitches of 2-0 resorbable material were done to align the lower face of the gastric stump with the jejunal loop where the new G-J anastomosis will be placed.
The jejunal loop was now opened and the underside of the gastric stump was opened.
G-J anastomosis was then performed with a blue load suture, a 2.5 cm anastomosis was performed. (Fig. 6).
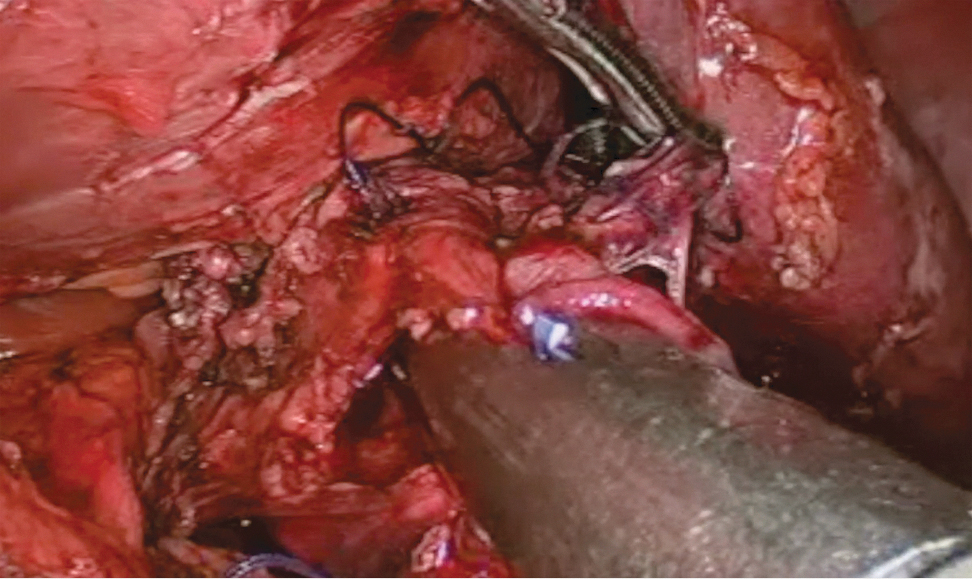
A 2.5 cms gastrojejuno anastomosis is then performed with blue load linear stapler.
The anastomotic defect was then closed manually with 2-0 reabsorbable material. (Fig. 7). A second suture reinforcement layer was finally performed.
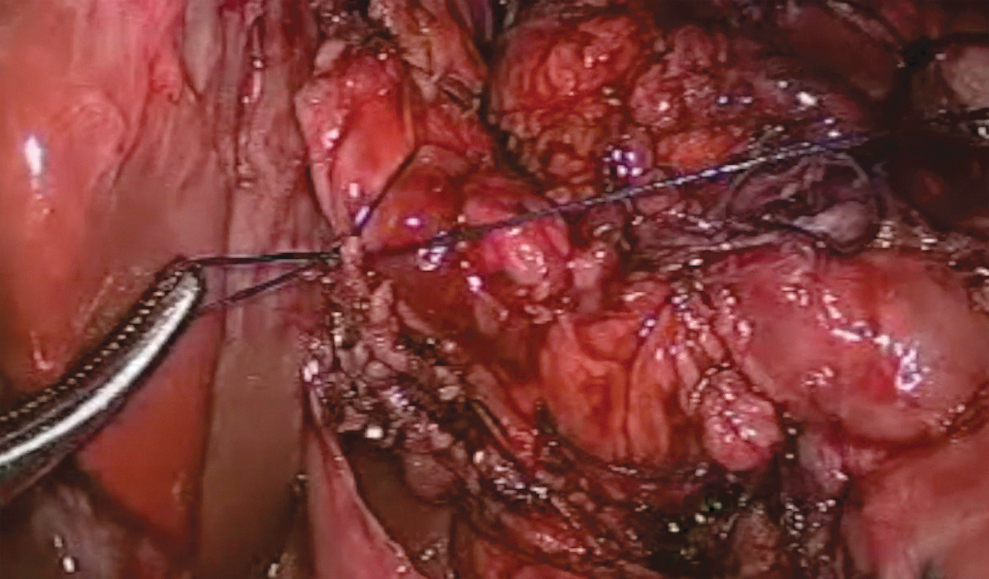
The anastomotic defect is finally closed manually.
A drain was placed toward the anastomosis.
The follow-up was uneventful, with the patient tolerating fluids 24 hours after the surgery and being discharged home in the postoperative day 2.
Conclusions
Regarding the late complications of gastric bypass, the G-J anastomosis stenosis is the most frequent. The predominant symptoms are postprandial vomiting accompanied by different degrees of dysphagia. Resolution is mainly endoscopic. If the endoscopy is inconclusive for stenosis with these symptoms, we have to take into account the possibility of intestinal obstruction due to kinking and it should be considered strongly. If endoscopic treatment for stenosis or cases of kinking are unsuccessful and fail, then revisional surgery should be considered. They are demanding and must be performed by experienced bariatric surgeons.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.