
Abstract
Background:
We wish to describe a novel technique of transdiaphragmatic excision of hepatic hydatid in patients with synchronous ipsilateral lung hydatid.
Patients and Methods:
Two patients, aged 11 and 6 years, presented with large synchronous hydatid cyst in right lung and liver. Second patient had two large cysts in right lobe of liver in posterior-superior segment of VII and VIII. The patients underwent thoracoscopic excision of lung cyst, and in same sitting the liver hydatid was seen bulging through the diaphragm. The diaphragm was incised to expose the cyst beneath, with excision of hydatid. Port-in-cyst technique was used to excise the membranes.
Results:
Both lung and liver cyst were successfully removed through thoracoscopic approach and a laparotomy was altogether avoided. Both patients did well in follow-up (3 years and 6 months). There are no respiratory issues in these patients.
Conclusions:
This is a novel approach for multiple synchronous hepatic and pulmonary hydatid. This can be applied in specific scenario as described. It gives a significant advantage of avoiding a laparotomy and thoracotomy in patients and thus reducing morbidity.
Introduction
Echinococcus infection is very common in endemic regions of the world and often manifests with hydatid cyst in lungs and abdominal viscera. Lung being the most common organ of involvement followed by liver. 1 Quite often when the infection is overwhelming there can be multiple organ involvement. 2 Common patterns with multiple synchronous infection involve liver plus lung, both lungs, and various other combinations that may or may not involve other solid viscera of abdomen or chest. Surgical excision of multiple synchronous hydatid on either side of diaphragm is challenging and is morbid requiring laparotomy and thoracotomy in same or different sittings. To reduce this morbidity, minimal invasive surgery has offered abdominal laparoscopy and thoracoscopy, thus reducing the morbidity of two fairly large-sized incisions and multiple surgeries.
We present a novel approach of excising the hepatic hydatid through the diaphragm while dealing with ipsilateral lung hydatid through thoracoscopy. The patients underwent thoracoscopy for excision of pulmonary hydatid and same approach was utilized to remove the ipsilateral bulging hepatic hydatid. We discuss the scenarios where this approach can be applied. Feasibility, technique, and results are also presented.
Patients and Operative Technique
Two patients, aged 11 and 6 years, presented with large synchronous hydatid cyst in right lung and liver. Second patient had two large cysts in right lobe of liver in posterior-superior hepatic segment of VII and VIII. Preoperative X-ray and computed tomography findings are shown in Figure 1. Both patients underwent initial thoracoscopy for excision of lung hydatid. Three ports were placed in thorax as per the triangularization principles. One additional 10-mm port is required, which is placed just above the cyst. During thoracoscopy the hepatic hydatid was seen bulging through the diaphragm (Fig. 2A). After removal of lung hydatid, a vertical linear incision was made on the bulging part of diaphragm to expose the underlying cyst in liver (Fig. 2B–D). There were minimal adhesions between the undersurface of diaphragm and dome of the cyst. Two lips of incised diaphragm were hitched laterally to widen and stabilize the opening. The cyst was aspirated with a 5-mm aspiration needle and reinjected with scolicidal agent. Once the cyst was decompressed, it was lifted with the help of a hitch stitch. The dome of the cyst was opened and port-in-cyst technique was used to remove the membranes. 3 In this method a 10 mm port is placed on top of the cyst area and is made to enter the cyst cavity. The port acts as a sheath and multiple passes of 10 mm suction are done to remove the fluid and hydatid membranes. This avoids any kind of spillage and also avoids loss of positive pressure inside thorax due to repeated suctioning. The port is transparent and the movement of membranes is seen on screen. The camera can also be inserted into this port to have a look inside the cyst cavity and inspection can be done for residual membranes and biliary communications. A drain is placed by passing a grasper through the abdominal wall and pulling in a Penrose drain. For second patient there were two cysts that required two separate incisions in diaphragm for excision with similar steps. Procedure ended with a chest drain. Second patient had major air leak from the lung hydatid and unfortunately required a second look surgery on third postoperative day to close the air leak. He recovered well after that. Both the liver and lung hydatid were removed by thoracoscopic approach and an abdominal approach was altogether avoided in both patients. Follow-up with 1st patient is 3 years and 6 months with 2nd patient. Both are doing well with no recurrence or any respiratory issues.
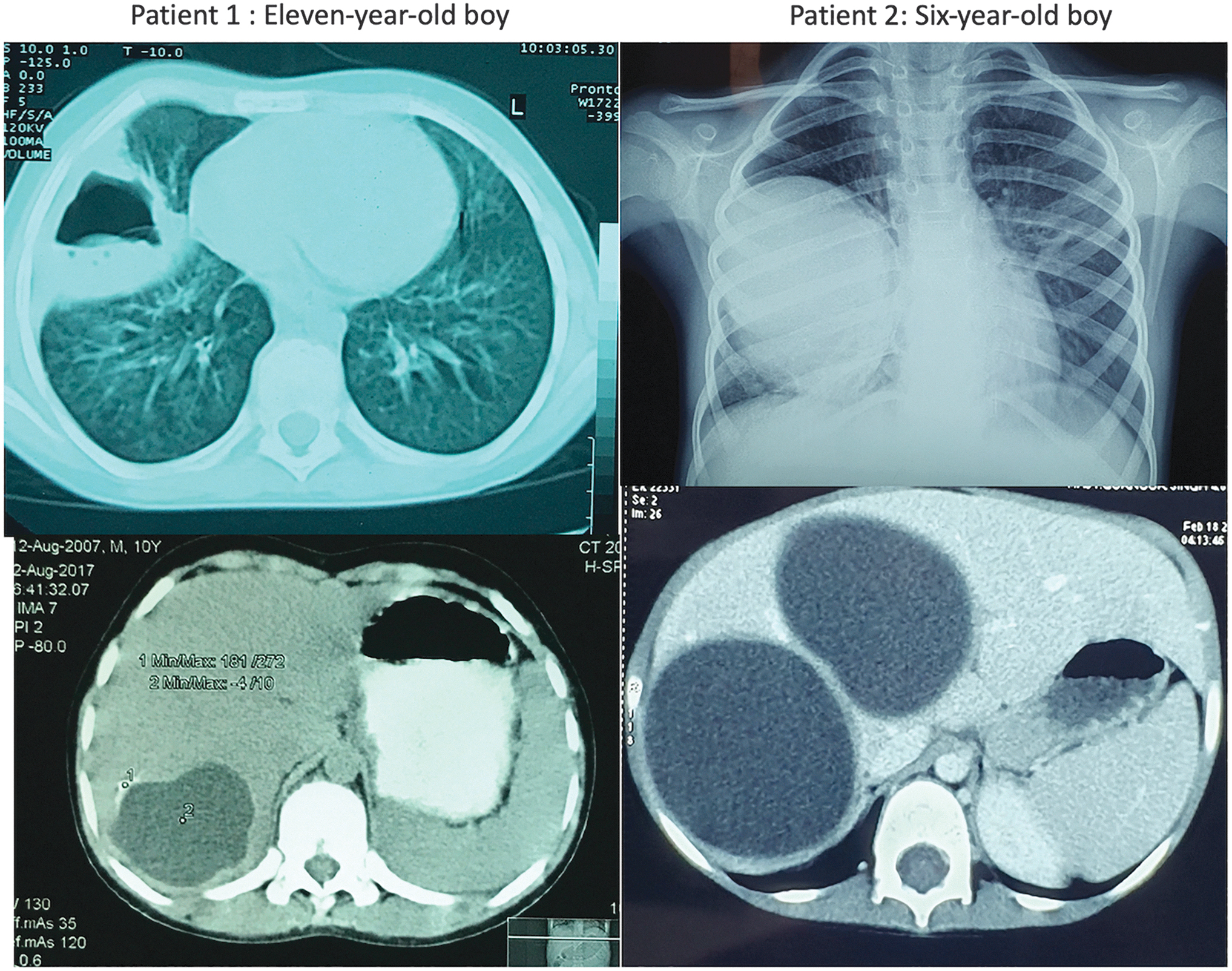
Imaging seen in the 2 patients. Note the 2nd patient had two cysts in right lobe of liver just beneath the large lung cyst.
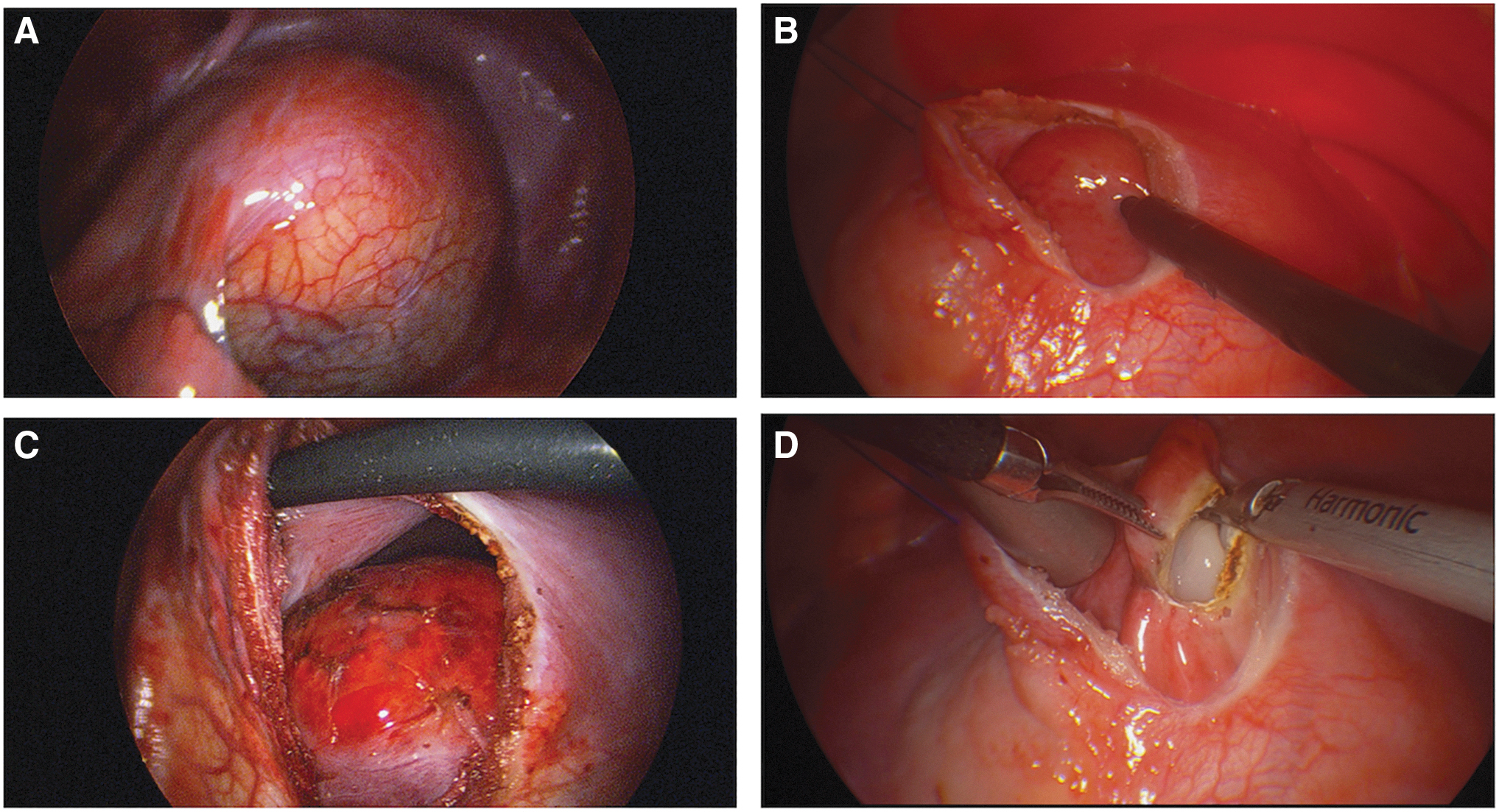
Intraoperative views in 2 patients.
Discussion
Asia, Middle East, and African countries have a very high rate of echinococcus infestation and are endemic regions. 4 With high infection load, multiple synchronous visceral involvement on both sides of diaphragm are very common. Management of hydatid cyst through minimal access surgery can avoid the morbidity of large abdominal incisions and thoracotomy for pulmonary hydatid. Several authors have reported successful outcomes with laparoscopic and thoracoscopic excision of hydatid with results comparable with open surgery.5,6 For patients presenting with multiple location hydatid, as liver and lungs, the conventional norm is of laparotomy and thoracotomy in single or different sittings and is morbid because of the approach. The operative technique described in 2 patients deals with the lung and liver hydatid in the same anesthesia through thoracoscopy. There is a specific subset of hydatid patients where this can be applied. The liver hydatid should be on the same side as the lung hydatid and should be large enough to surface on the liver and bulge through the diaphragm. It is seen as a lump beneath the diaphragm during thoracoscopy (Fig. 2). This will happen if the cyst is in the posterior segments of liver (segment 7 and 8). The cyst can thus be approached through the diaphragm following all the principles of hydatid excision.
Port-in-cyst technique as previously described by the same author 3 is an effective way of removing cyst contents laparoscopically without the fear of spillage. The 10 mm port provides an outer sheath or working channel for the wide bore 10 mm suction canula to make multiple passes and remove the membranes or daughter cyst.
Transdiaphragmatic approach for lung and liver lesions in either direction has been reported previously in adult literature in relation to liver tumors. 7 Authors have reported resection of ipsilateral metastatic lung lesions for patients with hepatic tumor and resection of liver tumors in posterior-superior segments through thoracotomy. 8 Similar approach has been used for heart and pericardium from abdominal side. 9
Minimally invasive approach with the concept of transdiaphragmatic approach has also been described for similar posterior-superior liver lesions. 10 We have utilized the same concept for hydatid lesions. This has not been applied before in pediatric patients. The posterior-superior lesions in segment VII and VIII are difficult to approach laparoscopically and even after extensive hepatic mobilization a good view of the cyst with a stable approach is difficult to achieve. This is conveniently accessible from thoracic side as the cyst is seen bulging through the diaphragm.
Argument can be made for possibility of diaphragm dysfunction, resulting out of opening of otherwise normal diaphragm. The cases reported in adult literature have utilized this approach by opening large portions of diaphragm and have not reported any dysfunction in follow-up. In presented cases the opening in diaphragm was 5 cm approximately and was repaired to satisfaction. Diaphragm being a well-vascularized structure heals well without much of scarring. These patients have not shown any evidence of respiratory issues. Fluoroscopy was done in the first patient after 6 months of surgery showed normal dynamics. Diaphragmatic outline as seen on chest X-rays in follow-up of both patients was normal.
This approach provides a major advantage of tackling two organs in single sitting with one access through thorax, thus avoiding additional incisions or approaches. For centers not practicing laparoscopy for hydatid excision can use the same concept for eligible patients even if they are doing open thoracotomy for lung hydatid and avoid a laparotomy.
There are certain disadvantages of this technique. It cannot be applied if the liver lesions are not bulging through the diaphragm and are involving more of the anterior segments of diaphragm. Similarly, small lesions deep seated in liver can also be difficult to get to and are not advisable by this approach. Other than this other possible complications are generic to the laparoscopy/open procedure with risk of spillage and seeding of thoracic and abdominal cavity. This can be avoided with meticulous handling of the cyst and using the port-in-cyst technique.
To conclude, this is a novel approach for multiple synchronous hepatic and pulmonary hydatid; can be applied in specific scenario as described in this study; gives a significant advantage of avoiding a laparotomy and thoracotomy in patients and thus reducing morbidity. A larger set of patients is needed to further prove the success/failures that can be associated with this approach.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.