
Abstract
Aim:
The aim of this prospective, nonrandomized, observational study was to present our results in operative treatment of complex anal fistulas using video-assisted anal fistula treatment (VAAFT) procedure with a curative intent in 2 years follow-up period.
Materials and Methods:
Between March 2016 and March 2018, 73 patients underwent the VAAFT procedure. Postoperative follow-up was 2 years, up to March 2020. Only patients with complex cryptoglandular anal fistulas were included. All patients were referred for magnetic resonance imaging of the pelvis. Fecal incontinence severity index score was used to assess any continence disturbance prior operation and postoperatively.
Result:
Primary healing occurred in 52 cases (71.23%) after first operation. From 21 patients who had recurrence or who had persisting disease, 16 patients accepted reoperation with second VAAFT procedure and additionally 10 patients achieved healing. From a total number of 73 patients who were included in study healing ultimately occurred in 62 cases (84.93%). In the first operation internal opening was identified in 47 cases (64.38%) and was closed with mattress suture, rectal advancement flap or ligation of intersphincteric fistula tract technique depending on its extent and type of fistula. Median primary healing rate was 6 weeks. There were no serious intra- or postoperative complications. None of the patients reported any type of continence disturbance.
Discussion:
VAAFT has been shown to offer good rates of healing, low morbidities, possibilities of multiple attempts in case of first failure and this series adds to the literature.
Introduction
Anal fistula is a chronic abnormal connection between the anal canal and the perianal skin. It is a tract lined with granulation tissue that supports chronic inflammation. Incidence of the disease is about 10 cases per 100,000 individuals with male to female ratio of 2:1. It mostly develops after an abscess of cryptoglandular origin although it can be associated with inflammatory bowel disease (IBD), trauma, and carcinomas.1,2
Various classifications are proposed, but most widely used is the Parks classification. It relates to the course of fistula in relation to the sphincter mechanism. 3
Nowadays fistulas can also be classified as simple and complex according to the relation of the proportion of the anal sphincter mechanism they pass through. Simple anal fistulas have one tract that crosses <30% of the external anal sphincter. They are treated best by fistulotomy or fistulectomy with very low incidence of continence disturbance. Other fistulas are classified as complex. These tracts cross external anal sphincter at a point that involves more than 30% of the external anal sphincter, and they can be associated with multiple tracts. In case they are treated by fistulotomy, fistulectomy, there is a high risk of postoperative continence disturbance. Complex fistulas also include those anteriorly positioned in a female, recurrent fistulas and those related to IBD. 4
The average rate of continence disturbance after treatment with a cutting set on is up to 12%, which increased when the internal opening of fistula tract was positioned more proximally. 5 After lay open techniques, the incidence of flatus incontinence or liquid stool leakage was observed in 20%–25% of the patients. 6 This resultant effect on continence has resulted in these techniques being less favorable for complex anal fistulas and the appetite for the use of minimally invasive techniques is increasing. Many minimally invasive techniques have been shown to be associated with higher recurrence rates with even less long-term sustainability. This may be a result of missed tracts or failure to identify the true internal opening.7–16
Video-assisted anal fistula treatment (VAAFT) is a novel sphincter preserving procedure that was developed by Italian surgeon P. Meinero. He and others have described long- and short-term healing rates of this technique that has the potential to identify secondary tracts with relative ease. 7
The aim of this prospective, nonrandomized, observational study was to present our results in operative treatment of anal fistulas using VAAFT with or without other sphincter preserving procedures in 2 years follow-up period.
Materials and Methods
This article is a prospective, nonrandomized, observational study of 73 patients treated for complex anal fistulas during the 2 years period (March 2016 and March 2018) with 2 years follow-up period up to March 2020. This study has been approved by the Institutional Ethics Committee. All patients preoperatively signed the informed consent and Helsinki Declaration Principles were implemented. We included patients aged between 18 and 65 years with complex cryptoglandular anal fistulas. All patients were managed with VAAFT technique. Patients with simple fistulas and those with IBD were excluded.
Patients had clinical examination in the office, which included digital rectal examination and examination with linear metal probe. All patients were referred for magnetic resonance imaging (MRI) of the pelvis for preoperative planning. After preoperative assessment, patients were scheduled for the VAAFT procedure based on the MRI findings and the inclusion criteria (complex fistulas of cryptoglandular origin).
On the morning of the surgery all patients received an enema, and antibiotic prophylaxis cefazoline in combination with metronidazole was given 30 minutes before procedure.
The operation was performed in litothomy position under spinal or general anesthesia using Karl Storz® (Karl Storz GmbH, Tuttlingen, Germany) fistuloscope and special designed equipment.
The VAAFT procedure has two phases; diagnostic and therapeutic.
The aim of the diagnostic phase is to visualize the entire fistula tract and the internal opening and to identify any possible secondary tracts and abscess cavities (Fig. 1). Where the internal opening was covered by healthy mucosa no further action was taken to avoid forming a false tract.
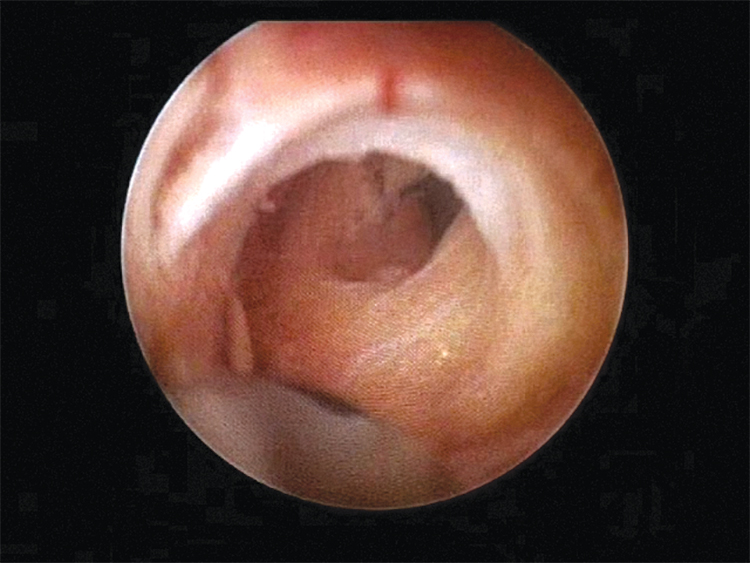
Exploration of the fistula tract using fistuloscope.
In the therapeutic phase, complete destruction of the main and secondary fistula tracts and closure of internal opening are performed (Fig. 2). We used different internal opening closure methods depending on the fistula type and extent of the internal opening. We used mattress suture, rectal advancement flap (RAF), or the ligation of intersphincteric fistula tract (LIFT) technique to close the internal opening if one was identified.

Fulguration of the fistula tract using monopolar electrode advanced through the working channel of the fistuloscope.
We used RAF for fistulas that had an internal opening larger than 5 mm, whereas the LIFT technique was used only in cases of transsphincteric fistulas with smaller internal openings. In all other cases when the internal opening was identified mattress suture was used to close one.
Primary outcome was defined as healing of the fistula. Secondary outcomes were defined as operative time, postoperative pain, fecal continence disturbances, and postoperative complications. Healing was defined as absence of discharge and closure of the external opening until 6 months postoperatively. After that period, if there were signs of persisting fistula, we offered the patient reoperation with the same technique. Along that as well, if the fistula tract healed but reappeared within 6 months period postoperatively, we considered it as a recurrence of disease. Postoperative follow-up period was 2 years.
Visual Analog Scale was used for determining pain intensity in early postoperative period. The fecal incontinence severity index (FISI) score was used to assess continence disturbances.
We used Microsoft Excel® (Microsoft, Seattle, WA) spreadsheet for data collection and Statistica® (TIBCO Software, Inc., Palo Alto, CA) for statistical analysis of our results. To test significance we used Student's t-test for independent samples. P-value that was <0.05 was considered significant.
Results
Out of 73 patients who were included in study, 48 (65.75%) were male and 25 (34.25%) female, with a median age of 45 years (range, 18–65 years). For 54 patients (73.97%) this VAAFT procedure was the first treatment and 19 patients (26.03%) had recurrent disease and had prior operation of anal fistula disease in their medical history (not including VAAFT).
Mean operative time for all operations was 39 minutes (range 15–90 minutes) and it was much shorter in the group when the internal fistula opening was not identified during operation (mean time 27 minutes, range 15–40 minutes), than in the group when there was internal fistula opening (mean time 44 minutes, range 20–90 minutes). There were no intraoperative complications. In postoperative period no major complications were reported, only 1 patient needed emergency reoperation because of postoperative bleeding on the place where RAF was made.
The internal opening was identified in 47 (64.38%) cases. Based on the criteria for treatment of internal opening, as mentioned earlier the LIFT technique was used in 14 cases (29.79%), RAF in 17 cases (36.17%), and mattress suture in 16 cases (34.04%) (Table 1).
Primary Healing and Recurrence Rate, Techniques Used for Closing the Internal Opening, Mean Operation Time After First Operation
LIFT, ligation of intersphincteric fistula tract; RAF, rectal advancement flap.
After the first VAAFT operation primary healing occurred in 52 cases (71.23%) and 21 patients had recurrent or persisting disease (28.77%). From the mentioned 21 patients, there were 11 patients from the group where internal opening was not identified during VAAFT procedure (total number of patients with unidentified internal opening during operation was 26) and 10 patients with identified internal opening during VAAFT procedure (total number of patients with identified internal opening during operation was 47), (recurrence—42.31% versus 22.28%). The difference between healing results in patients with identified and unidentified internal opening was proved to be insignificant after using Student's t-test with P = .058.
As for postoperative pain intensity measured on a VAS (0–10), the mean score was 2.6 and the patients were administered oral analgesics.
Median primary healing rate after first operation was 6 weeks (range 3–14 weeks). None of the patients had recurrence 6 months after first VAAFT operation. Patients who had recurrent or persisting disease were offered another operation using VAAFT technique. Out of 21 patients with recurrent or persisting disease, 16 accepted and underwent second operation. In this group 10 patients have achieved primary healing. That brings up the number of healed patients to 62 (84.93%) from a total of 73 who were included in this study.
None of the patients who underwent VAAFT reported any type of continence disturbance based on a FISI score. Some of the patients who underwent some other type of anal fistula treatment, before initial VAAFT procedure, had mild continence disturbance that did not worsen after VAAFT procedure (Table 2).
Fecal Incontinence Severity Index Score After Video-Assisted Anal Fistula Treatment Procedure
Discussion
In the last decade several new sphincter preserving techniques including VAAFT have been developed to reduce the risk of continence disturbances.7–16 Compared with other minimally invasive techniques, VAAFT is the only procedure that allows intraoperative visualization of the entire fistula tract, possible secondary tracts and the internal fistula opening from within the tract. The main indication for VAAFT is operative treatment of complex anal fistulas, where there is a high possibility of continence disturbance if the sphincter were to be divided, and complex anal fistulas with multiple tracts.5,17 The VAAFT technique is comparable with other sphincter preserving techniques in relation to healing and patient satisfaction. 18 Diminished postoperative pain, earlier recovery after surgery, and smaller postoperative perianal wounds allow for earlier return to normal activities.
The VAAFT technique allows multiple attempts in case the procedure is not successful in the first instance as shown in our results. We could argue that if even more reoperations were done on the persisting or recurrent fistulas we would have had even higher percentage of healed patients, but this was not the focus of this study. The proposed mechanism whereby repeated procedures have an incremental effect is converting a complex fistula with multiple tracts into a more manageable fistula with perhaps one tract and also by de-epithelializing the tracts. The epithelialization is very clearly seen through the fistuloscope and the epithelial tissue can be destroyed by cauterization.
Meinero and Mori initially proposed closing the internal opening with a stapler. We did not use this technique as it was economically unjustifiable and the results have not been replicated. Many techniques with similar results have been employed to close the internal opening and this justifies our rationale for not using the stapler.7,17,19 The subject of the best method to close the internal opening causes much debate and no one technique has been proven to be superior and same was also in our study with similar recurrence rate.
To date, the VAAFT has been shown to be safe and associated with good functional outcomes and very low incidence of complications.7,15,17,19–23 We have also shown that the VAAFT does not alter continence further adding to the available evidence.
In our study, primary healing after first treatment was obtained in 52 cases (71.23%) with median primary healing rate of 6 weeks. After we have reoperated 16 patients who had persisting symptoms or recurrent disease, additional healing occurred in 10 cases, so total healing rate in all 73 patients who were included in this study was 84.93% (62 cases). We compared our results with other studies, especially with a currently available meta-analysis and long term follow-ups on the subject.22–24 The meta-analysis describes a recurrence rate of 14.2%, which is smaller than in our study (after first treatment).
We believe this to be because other studies and meta-analysis also included simple fistulas, which contributed to higher success rate. We believe the VAAFT procedure has limited value in treatment of intersphincteric and very low transsphincteric fistulas (i.e., simple fistulas), because they can be adequately treated with simple lay open techniques with excellent results and without risk of continence disturbances.
The success of VAAFT may depend on a few important operative steps. First, during the diagnostic phase of VAAFT identifying all tracts is essential. In fistulas with multiple branches, MRI correlation may be useful. Second, during the operative phase it is necessary to destroy all granulation tissue by cauterization and to evacuate necrotic tissue from fistula tract. After this, it is important to close the internal opening and if one does not exist, or if it is covered with mucosa, iatrogenic perforation should be avoided. Depending on the extent of internal opening and the type of fistula, we have used different techniques (LIFT, RAF, and mattress suture). 25 It is also of great importance to secure adequate drainage of fistula tract and to clean it with the use of Volkmann spoon and antiseptic liquid.
Our study has shown that VAAFT technique is useful when performing fistula surgery in patients with recurrent disease, with results comparable to those of patients with first presentation. Although this was not quantified in this study, patients who had previous conventional treatment were much more satisfied with this technique as far as postoperative pain and general discomfort of the healing period is concerned. Patient satisfaction with the procedure has also been demonstrated elsewhere.26,27 Despite promising results, multicenter studies on a larger group of patients with longer-term follow-up is necessary.
VAAFT is a sphincter preserving, minimally invasive technique for treatment of anal fistulas. Its value lies particularly in the treatment of complex fistulas without risk of continence disturbances and with low rate of morbidities. This technique can be used in combination with other sphincter preserving techniques with also high primary healing rate. Its main value is in the sphincter saving nature of the procedure and possibility of multiple attempts in case of first failure. Also, it is a technique that allows treatment of deep parts of fistula tracts or multiple tracts simultaneously without making huge perianal wounds. Recurrence after VAAFT procedure may be related to identification of internal opening or missed secondary tracts. The long-term durability needs to be assessed.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no specific funding for this article.