
Abstract
Background:
The diagnosis of occult penetrating diaphragmatic trauma remains challenging, with conventional imaging offering inadequate accuracy for diagnosis. Minimally invasive surgical options for evaluating the diaphragm conventionally require general anesthesia. We propose a technique for evaluating the diaphragm via awake thoracoscopy in the emergency department.
Methods:
A prospective interventional study was conducted to investigate the safety and accuracy of emergency department awake thoracoscopy for diagnosing diaphragmatic injuries in penetrating thoracoabdominal trauma. All adult patients who presented to the trauma unit with penetrating thoracoabdominal trauma who were hemodynamically stable were enrolled. The patients underwent emergency department awake thoracoscopy with a rigid endoscope through a previously inserted intercostal drain. Only local anesthesia and conscious sedation were provided.
Results:
Forty patients were enrolled. All 40 (100%) were men, and the median age was 34 years. Thirty-four had stab wounds (85%), 5 had gunshot wounds (12.5%), and 1 had a suspected iatrogenic diaphragm injury during intercostal drain insertion (2.5%). In 32 (80%), the diaphragm was well visualized, of whom 7 (17.5%) had diaphragm injuries. In the remaining 8 patients in whom the diaphragm was not well visualized, only 1 (2.5%) had a diaphragmatic injury. The diaphragmatic injuries that were identified were confirmed and repaired during a subsequent explorative laparoscopy. There were no procedure-related complications in any of the patients during short-term follow-up.
Conclusions:
Awake thoracoscopy is safe, feasible, and accurate for the diagnosis of occult diaphragm injuries and may offer a modality for assessment that does not require general anesthesia.
Introduction
Diaphragmatic injuries present a diagnostic challenge after penetrating thoracoabdominal trauma. Imaging has not been proven to be very accurate, and patients often require invasive assessment under general anaesthesia. 1 However, the majority of patients will not have a diaphragmatic injury, rendering such an approach excessively invasive and not cost effective. 2
The risk of missed occult diaphragmatic injury is unclear in the long term, as patients may only complicate months or years after the initial injury. However, it is clear that if the patients do develop complications such as herniation and strangulation, this carries a high morbidity and mortality. 3 No ideal modality exists for investigating these injuries and there are little compelling data assessing whether awake thoracoscopy has a role in solving this problem.
This study aimed at evaluating the use of emergency department awake thoracoscopy for assessment of the diaphragm as a novel method of diagnosing these injuries, observing its success, accuracy of its findings, and safety.
Materials and Methods
A prospective interventional study of penetrative thoracoabdominal trauma was conducted at Dr George Mukhari Academic Hospital, Pretoria, South Africa from November 2017 to November 2018. This institution is a 1650-bed tertiary level hospital and trauma center not only serving a catchment area of 1,200,000 people, primarily from the surrounding communities in Northern Gauteng, but also serving as a referral center for selected hospitals in Northern Gauteng, North West Province, and Limpopo Province, South Africa. This institution is affiliated with Sefako Makgatho Health Sciences University.
For the purposes of this study, awake thoracoscopy was defined as video-assisted thoracoscopy performed in the emergency department without the use of general anesthesia. Thoracoabdominal trauma was defined as injuries between the superior border of the fourth intercostal space (ICS) anteriorly and the inferior border of the scapula posteriorly and the costal margin inferiorly.
Our inclusion criteria for this study were: all patients older than the age of 18 years presenting with penetrative thoracoabdominal trauma, with an indication for an intercostal drain. Exclusion criteria were: hemodynamic instability, any immediate indication for surgical exploration (e.g., generalized peritonitis), or inability/unwillingness to provide consent.
Demographic and clinical characteristics of the patients were summarized descriptively by mean, standard deviation, median, interquartile range, and minimum and maximum values for continuous variables (e.g., age), and by frequency counts and percentage calculations for categorical variables (e.g., gender or mechanism of injury). Data recorded included demographic data, mechanism of injury, external location of injury, findings of chest X-ray, findings of thoracoscopy, success rate of thoracoscopy, and complication rates including mortality.
Complications were summarized by type and incidence. Analysis of subgroups was done where of clinical interest.
All statistical procedures were performed on Statistical Analysis Software (SAS Institute, Inc., Carey, NC, USA), release 9.4 or higher.
Before initiation of the study, ethics approval was attained from the local research and ethics committee in accordance with the Declaration of Helsinki. Research ethics committee certificate reference number SMUREC/M/278/2017: PG. Informed consent was obtained from all participants before enrollment into the study.
Procedure technique
The procedure was performed by residents of the department of general surgery of Dr George Mukhari Academic Hospital after having the procedure demonstrated and initially performing it under supervision, until they were familiar with the technique.
The procedure was performed with a 5 mm 30° telescope (Karl Storz, Tuttlingen, Germany) that had been sterilized in Cidex ortho-phthalaldehyde solution. This was attached to a Telepack X LED endoscope with a Telecam camera and a 4.8 mm light cable (Karl Storz).
The recommended position for the patient during the procedure was in the lateral side away from the injured side; for example, if left thoracoscopy was performed, the patient was placed in the right lateral position. Continuous hemodynamic monitoring was used throughout the procedure until the patient was fully recovered.
The patients received a combination of local anesthetic around the intercostal drain insertion site as well as intravenous ketamine at a dosage of 1 mg/kg before initiation of the procedure unless the use of ketamine was contraindicated.
Under aseptic conditions, the underwater bottle was disconnected from the drain. The patient was allowed to draw air into his thorax via the intercostal drain through spontaneous respiration; however, no insufflation was used. The drain may have been shortened for ease of operation as needed, and the tip was cut off to allow passage of the telescope. The lens was then passed through the drain into the pneumothorax that had been created, and the diaphragm was inspected.
If any injuries were identified or there remained diagnostic doubt, patients underwent further investigation, preferably through explorative laparoscopy. If no injury to the diaphragm was identified and the diaphragm was adequately visualized, the patients were managed conservatively.
The patients were all followed up at least 1 week after discharge to assess for any complications and recovery.
Results
There were 40 patients who met the inclusion criteria for the study and were enrolled. The demographic data and patient characteristics are summarized in Table 1.
Demographic Data and Patient Characteristics
IQR, interquartile range; SD, standard deviation.
In keeping with the general trends of trauma, particularly trauma from interpersonal violence, the primary patients who met the inclusion criteria for the study were young males.
Stab wounds were the mechanism of injury in 34 patients (85%) included in the study, with 26 (65%) of the patients having a single stab wound and 8 (20%) of the patients having multiple stab wounds. Of the remaining patients, 5 (12.5%) were victims of gunshot wounds and 1 patient (2.5%) was referred from a peripheral hospital with a suspected diaphragm injury after an intercostal drain insertion during which the drain was placed too low.
As is common in stab wounds, there seems to be a slight predilection for stab wounds to the left hemithorax rather than the right. Stab wounds occurred 20 (61%) times on the left and 13 (39%) times on the right. There were no significant differences in the laterality of gunshot wounds.
If multiple thoracic injuries were present, only injuries that were in the predefined thoracoabdominal area were recorded. If multiple injuries within the thoracoabdominal area were present, the injury in the lowest ICS was recorded.
Thirty (75%) patients sustained injuries between the fifth ICS and eighth ICS. Only 4 of these patients (13.3%) had diaphragmatic injuries. However, of the 9 patients who had injuries in the 9th ICS to 11th ICS, 4 patients had diaphragmatic injuries (44.4%). The ICS was not recorded in 1 case. The location of the external wound and rate of injury is summarized in Table 2.
Location of External Injury and Frequency of Diaphragm Injury
ICS, intercostal space.
In 35 (87.5%) of the patients, the sedation provided to the patients was a combination of local anesthetic and intravenous ketamine. In the cases that this combination was not used, it was due to concerns regarding head injuries, ocular injuries, or previous history of psychiatric illness.
The most frequent finding on chest X-ray was a pneumothorax, in 19 patients (47.5%), with hemothorax occurring in 13 patients (32.5%) and hemopneumothorax in 8 patients (20%). The presence of only hemothorax is associated with lower rates of adequate diaphragm visualization, with only 6 of the 13 patients having adequate visualization (46.2%). This compares unfavorably to cases in which a pneumothorax or hemopneumothorax was recorded. In these cases, the diaphragm was well visualized more frequently, with 25 of the 27 patients having adequate vision (92.6%). The chest X-ray findings as well as the reasons for inadequate visualization of the diaphragm are summarized in Table 3.
Findings of Chest X-ray and Reasons for Inadequate Vision
CXR, chest X-ray.
In total, 8 (20%) of all the patients were shown to have a diaphragm injury (Fig. 1). In 32 (80%) of 40 cases, the diaphragm could be well visualized (Fig. 2). In the patients where the diaphragm could be well visualized, 7 had an injury to the diaphragm (17.5% of total participants, 21.8% of the subgroup in whom the diaphragm could be well visualized). In the cases where the diaphragm could not be well visualized, only 1 patient was subsequently shown to have an injury to the diaphragm (2.5% of total participants, 12.5% of the subgroup in which the diaphragm could not be well visualized). Figure 3 demonstrates the results of the thoracoscopy.
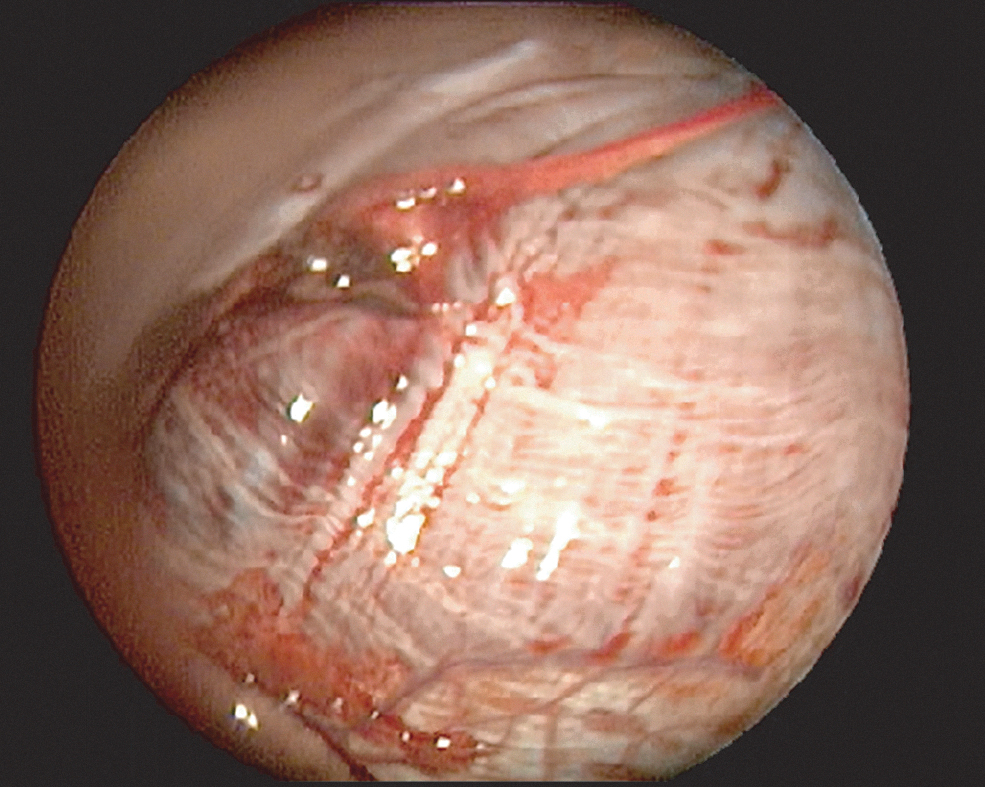
Thoracoscopy demonstrating laceration of the dome of the diaphragm.

Thoracoscopy demonstrating well-visualized diaphragm with laceration of chest wall and intact diaphragm.

Flow diagram of results of thoracoscopy.
The most common reason for poor visualization of the diaphragm was intrathoracic blood. In 6 (75%) of the 8 patients with poor visualization of the diaphragm, vision was impaired by a retained hemothorax that could not be evacuated with suction. In 1 (12.5%) of the 8, poor vision was due to active bleeding from the lung. One (12.5%) of the 8 patients had unexpected intrathoracic adhesions that prevented adequate visualization of the diaphragm.
Of the 8 patients who did not have adequate visualization of the diaphragm, 3 (37.5%) had an explorative laparoscopy performed, none of which revealed a diaphragmatic injury. One patient (12.5%) had a video-assisted thoracoscopic surgery performed for a retained hemothorax, during which a diaphragm injury had been identified and repaired thoracoscopically. One patient (12.5%) had a posterolateral thoracotomy performed for retained hemothorax, during which no diaphragm injury was identified.
Three patients (37.5%) refused explorative laparoscopy or any other surgical exploration, 2 of whom consented to a contrasted CT of the abdomen and lower chest. No features of diaphragm injury were present, and the patients refused further investigation. The other patient refused any further investigation, including imaging.
No procedure or sedation-related complications were recorded during the patients' initial hospital stay or at the follow-up at least 1 week after discharge from the hospital. There were no mortalities in the study group.
Discussion
Explorative laparoscopy has been established as the gold standard for diagnosis of occult diaphragmatic injuries. This is supported by studies such as the one published by Murray et al., who showed that in patients without hemodynamic instability and peritonitis, 26% of the patients undergoing laparoscopy were found to have diaphragmatic injuries that were not detected on imaging or clinically. 4 This finding has been reiterated by a local study done at our institution demonstrating the clinical utility of laparoscopy in 83 patients. 5
All the data earlier cited are supported by the 2018 Eastern Association for the Surgery of Trauma (EAST) guidelines in which they conditionally recommend laparoscopy as the investigative modality of choice, rather than CT scan or laparotomy. 6
Diagnostic thoracoscopy has been extensively evaluated to investigate patients for occult diaphragmatic injuries secondary to penetrating trauma. Although the technique has comparable accuracy to laparoscopy, it has not gained popularity as it also requires general anesthesia, cannot assess the abdominal contents for co-existing injury, and conventionally requires single-lung ventilation.7–9
The next step in the evolution of diagnosing diaphragm injuries in our institution was a study published by Koto et al. In this study, they demonstrated the safety and accuracy of thoracoscopy under general anesthesia with single lumen endotracheal intubation. In all but 1 case, the findings of the thoracoscopy correlated with the findings during laparoscopy. The limiting factor in this case was dense intrapleural adhesions. This indicated that single-lung ventilation may not be required to adequately visualize the diaphragm and diagnose these injuries. 10
It is with this background in mind that the technique employed in this study was developed. Having shown thoracoscopy without single-lung ventilation to be effective, the next step in the evolution of the technique was to assess whether this could be performed without general anesthesia. The frequency of diaphragm injury in this study was 20%. This is in keeping with what is found in the literature of patients who were investigated with other modalities. In these studies, the frequency of injuries with such trauma ranges from 16.7% to 32%.9,11
The high proportion of stab wounds as opposed to gunshot wounds likely appears due to the selection bias introduced by only enrolling hemodynamically stable patients with no immediate indication for laparotomy. As gunshots are of a higher velocity, the majority of these patients were likely excluded on these grounds. This trend was also observed in the previous study conducted at our institution. 5
The craniocaudal position of the external wounds, which were reported as the ICS where the wound was located, seems to influence the rate of diaphragm injury. The lower ICSs had a significantly higher rate of diaphragm injury when compared with the upper thoracoabdominal area in this study—13.3% of patients with injuries in the 5th to 8th ICS versus 44.4% of patients with injuries in the 9th to 11th ICS.
This seems intuitive, as the central dome of the diaphragm may extend as high as the fifth ICS only during full expiration and be susceptible to injury, but the peripheral attachment of the diaphragm to the lower costal margin means that it is at risk of injury during either phase of respiration.
The results of this study support the feasibility of awake thoracoscopy in diagnosing occult penetrating diaphragmatic injury. Awake thoracoscopy as employed in this study allowed assessment of a large portion of the patient group without the need for general anesthesia, with 32 (80%) of the patients undergoing adequate inspection of the diaphragm. Twenty-five of the 32 patients (78.1%) who had adequate visualization required no further management as no injury was identified.
The avoidance of general anesthesia may be particularly relevant in resource-constrained environments where theater time is at a premium, and any alleviation of the congested emergency lists in South African state hospitals is worth considering. Delays in patients receiving surgery have been widely reported in the South African media, with Dr George Mukhari Academic Hospital singled out as having an exhaustive waiting list of more than 4000 patients, 12 exacerbated by emergency surgery sometimes delaying elective procedures.
Interestingly, in 3 of the patients who had diaphragm injuries visualized, the injury could not be accessed during laparoscopy (two right, one left). These patients all had explorative laparoscopy with the intent to repair the injury; however, these injuries were located very posteriorly, rendering them inaccessible. Accessing these posterior injuries is a known shortcoming of laparoscopy, particularly on the right where the liver limits accessibility of the diaphragm. 6 The clinical importance of these posteriorly located injuries is yet to be determined.
Limitations/shortcomings
The data support the idea that the primary limiting factor to adequate visualization of the diaphragm was blood within the pleural space. Therefore, use of this technique is most valuable in patients with only pneumothoraces or limited hemothorax present. The failure of adequate visualization of the diaphragm in 3 patients who refused exploration does introduce a small group of patients in whom the ultimate state of the diaphragm was unknown. The short follow-up period of these patients also does not allow an analysis of what the long-term outcomes of the procedure were. The small sample size limits the strength of the conclusions that can be drawn from this study.
Conclusion
In conclusion, the technique used within this study for emergency department awake thoracoscopic assessment of diaphragm injuries appears safe, feasible, and accurate. This offers a new modality with which to address this challenging clinical problem.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.